
Abstract
Supervised walking exercise is an effective treatment to improve walking ability of patients with peripheral artery disease (PAD), but few exercise programs in community settings have been effective. The aim of this study was to determine the efficacy of a community-based walking exercise program with training, monitoring and coaching (TMC) components to improve exercise performance and patient-reported outcomes in PAD patients. This was a randomized, controlled trial including PAD patients (n=25) who previously received peripheral endovascular therapy or presented with stable claudication. Patients randomized to the intervention group received a comprehensive community-based walking exercise program with elements of TMC over 14 weeks. Patients in the control group did not receive treatment beyond standard advice to walk. The primary outcome in the intent-to-treat (ITT) analyses was peak walking time (PWT) on a graded treadmill. Secondary outcomes included claudication onset time (COT) and patient-reported outcomes assessed via the Walking Impairment Questionnaire (WIQ). Intervention group patients (n=10) did not significantly improve PWT when compared with the control group patients (n=10) (mean±standard error: +2.1±0.7 versus 0.0±0.7 min, p=0.052). Changes in COT and WIQ scores were greater for intervention patients compared with control patients (COT: +1.6±0.8 versus −0.6±0.7 min, p=0.045; WIQ: +18.3±4.2 versus −4.6±4.2%, p=0.001). This pilot using a walking program with TMC and an ITT analysis did not improve the primary outcome in PAD patients. Other walking performance and patient self-reported outcomes were improved following exercise in community settings. Further study is needed to determine whether this intervention improves outcomes in a trial employing a larger sample size.
Introduction
Peripheral artery disease (PAD) is associated with increased cardiovascular complications,1,2 with over eight million adults presenting with the disease in the United States. 3 Intermittent claudication (IC), defined as pain, aching and/or cramping in the muscles of the legs during walking which resolves with rest, is estimated to occur in 35% of all patients with PAD.4,5 Thus, PAD patients have significantly impaired walking and functional ability as well as poor patient-reported outcomes. 6
Supervised walking exercise programs in hospital settings typically improve exercise outcomes and improve symptoms that impair walking ability in PAD and IC.7,8 However, factors such as lack of reimbursement have prevented adoption of these programs. In contrast, many community-based walking exercise programs for PAD patients have not been successful. Generally, these programs have consisted of general instructions for patients to exercise at home.9–11 The absence of benefit observed in many studies may be due to lack of supervision, lack of training in how to exercise and failure to address barriers to exercise in the community. Recent community-based walking programs have improved outcomes in PAD patients,12–14 providing evidence that walking programs outside of hospital settings may be beneficial. These previous trials have employed structured training, monitoring and coaching (TMC) components commonly used in supervised exercise programs, but implemented in community settings for PAD patients.
Thus, a community-based walking exercise program that builds on previous successful trials by including structured TMC components used in supervised walking exercise programs, in addition to novel methods used in public health programs, should increase the chances that PAD patients adopt and sustain exercise in the community setting. The aim of this pilot study was to develop a feasible yet effective community-based walking exercise program for PAD patients. We tested the hypothesis that PAD patients randomized to a community-based walking exercise program with TMC, would improve peak walking time (PWT) on a graded treadmill compared to patients who only received usual care advice.
Methods
Study design
The pilot study utilized a randomized, controlled treatment design. Patients were randomized to the exercise treatment or usual care control group using a computer-generated random allocation scheme following baseline outcomes assessment. Investigators and patients were blinded to study arm allocation during patient recruitment, screenings, the consenting process and during baseline testing, but not during follow-up testing.
Patients
Male and female PAD patients were recruited from the vascular and internal medicine clinics at the University of Colorado Hospital, the Denver Veterans Affairs Medical Center and through Hospital/University-wide email and newsletter recruitment announcements. Patients were included if they were ⩾40 years of age, had received peripheral endovascular therapy four to six weeks prior to baseline testing or presented with stable IC symptoms and had not previously received revascularization within the four to six week window. For those with IC, patients were included if their ankle-brachial index (ABI) was ⩽0.90. For patients recruited post peripheral endovascular therapy, an ABI >0.90 was not exclusionary. Patients who had previously received peripheral revascularization but did not fall within the four to six week window were allowed into the trial following a one-year washout period from the previous endovascular procedure if they continued to present with IC symptoms. Assessments of ABI were performed according to published methods 15 using a standard Doppler device (CareFusion Nicolet, Golden, CO). Patients were excluded if they: 1) had lower extremity amputation(s) that interfered with walking on a treadmill, 2) had critical limb ischemia, 3) had PAD of non-atherosclerotic nature, 4) were primarily limited in walking by comorbidities other than IC, 5) exhibited severe cardiac ischemia as documented on noninvasive testing, 6) had a previous myocardial infarction, transient ischemic attack or stroke three months prior to screening, and 7) were treated with pentoxifylline or cilostazol for the treatment of IC (one-month washout period allowed). The Colorado Multiple Institutional Review Board and Denver Veterans Affairs Medical Center Institutional Review Board approved all procedures for the study. Patients provided written informed consent prior to testing.
Exercise performance endpoints
Graded exercise tests were conducted on a treadmill with continuous electrocardiogram monitoring (Q-Stress TM55, Quinton Cardiology Systems Inc, Bothell, WA) using a modified Gardner protocol as previously described with patients walking until maximal claudication pain or other exercise-induced factor.16,17 An open circuit respiratory-metabolic system (Ultima Series, Medical Graphics Corp, St Paul, MN) was used to measure peak oxygen consumption (VO2peak) (ml∙kgˉ1∙minˉ1). PWT (minutes) was recorded as the maximal time the patient could walk on the treadmill before having to stop. IC was measured with the Claudication Symptom Rating Scale (ranges from 1 to 5 with 1=no pain, 2=claudication onset, 3=mild, 4=moderate and 5=maximal claudication). 18 Claudication onset time (COT) (minutes) was obtained by the patient pointing to the Rating Scale at the onset of symptoms, if any. Outcomes were assessed at baseline and 14 weeks later. If patients had previously received peripheral endovascular therapy, the baseline graded exercise test was conducted after the follow-up exam with the cardiologist (four to six weeks post revascularization).
Functional ability and patient-reported outcomes
Functional ability was assessed at each outcome assessment time point with the Short Physical Performance Battery (SPPB). 19 The SPPB has been studied previously in PAD populations with and without previous peripheral endovascular therapy20–22 and combines data from 4-m walking velocity, repeated chair rises and standing balance. Testing procedures followed the guidelines developed by Guralnik et al. 19 Additionally, patients completed the 4-m walking velocity test at their fastest pace, as has been previously conducted with PAD patients.20,23 The Walking Impairment Questionnaire (WIQ) and Medical Outcomes Study Short-Form 36-item (SF-36) questionnaire were administered prior to treadmill testing at baseline and post 14 weeks as previously described.24–27
Walking exercise intervention
Training (T)
Patients assigned to the control group received verbal advice to exercise but no other formal training. Patients in the intervention group received in-hospital exercise training on a treadmill for an initial two weeks (3 days∙weekˉ1). Patients then completed 12 weeks of community-based walking exercise training. The following training procedures were used for both the in-hospital and community-based walking exercise programs in the intervention group:
Patients were instructed to walk/rest on a treadmill during the in-hospital walking exercise program and in their self-selected community location for 35 minutes progressing to 50 minutes as tolerated.
Intensity was at a level great enough to induce moderate leg pain within 3–5 minutes for patients with IC. For PAD patients who did not experience IC, ratings of perceived exertion were used to regulate exercise intensity at a moderately hard level.28,29
Attempts to increase exercise intensity were made at least weekly, by manually increasing speed and/or grade during the in-hospital exercise and through encouraging patients to increase their walking pace while in the community.
During rest periods, investigators stopped the treadmill belt in the supervised setting and the patient used a portable lightweight collapsible chair (Walkstool, Trangsund, Sweden) for rest periods (also used in the community setting if needed). For patients who experienced IC, exercise resumed upon cessation of leg pain (pattern repeated until the target time was reached). For patients who did not experience IC, other factors that limited walking exercise (e.g. general fatigue) were used to initiate resting periods.
Ambulatory monitoring (M)
Patients in the exercise treatment group were monitored over the duration of the 14 weeks of exercise with a piezoelectric activity monitor (OrthoCare Innovations LLC, Oklahoma City, OK). Additionally, patients were given a spring-levered hip pedometer (Model AE120XL, Accusplit Inc, Livermore, CA). Patients were asked to wear the monitors during walking exercise sessions (3 days∙weekˉ1 for 14 weeks) and were also responsible for recording details about each session in a provided walking exercise log. Investigators called patients weekly with specific prompting to evaluate how much and how often patients were walking.
Coaching (C)
The intervention included an operational coaching model that provided training guidance and help in addressing local barriers to exercise training in the community. This model was also used to promote and reinforce facilitators for each individual patient in the intervention group. This included the following: 1) upfront provision of educational print materials and a video, 2) social and behavioral methods, and 3) environmental auditing of local walking areas for each patient. Campaigns focused on informational outreach and education have been cited as key strategies for promoting physical activity by the Centers for Disease Control and Prevention and the Task Force on Community Preventive Services. 30 Thus, educational materials from the Vascular Disease Foundation and PAD Coalition were given to patients randomized to the intervention group. Additionally, all patients randomized to the intervention group watched an eight-minute video developed by the National Heart, Lung, and Blood Institute and PAD Coalition Stay in Circulation campaign that focuses on PAD and treatment options. Coaching also included identification of specific resources in the community to help facilitate walking exercise for each patient, such as advocating walking exercise at local parks where seating may be readily available. Patients were also encouraged to walk with family, friends and pets as social support has been cited to increase physical activity levels in the elderly.31,32
Before each patient began the community-based walking exercise phase of the intervention, an evaluation of the local walking environment using an audit tool was conducted. 33 The tool examines permanent, transient and social-environmental factors that may influence adoption and compliance of walking exercise in patients. Patients identified an origin or starting point (e.g. home) for walking exercise as well as destinations (e.g. park) close to the origin. The investigator performed the audit using Google Earth®34 as well as by in-person visits, identifying barriers and facilitators to walking exercise in street segments and intersections. Examples of barriers to walking exercise included discontinuous sidewalks or poor lighting in an area. Facilitators to walking exercise could include shade trees along the route or high visibility crosswalk stripes at intersections. Several routes were discussed with patients when possible. Additionally, three patients (12%) chose to use treadmills for part of their walking exercise in community locations rather than walking outside. The investigator then walked with patients in their location of choice to review the most appropriate routes, destinations and exercise prescription in an initial community walking exercise visit. The investigator subsequently met with patients four and eight weeks later to walk in the community setting of their choice.
Statistical analyses
This study was designed to evaluate the benefits of a community-based walking exercise program. The intent-to-treat (ITT) population included 20 patients who had complete and evaluable data post randomization. An additional, exploratory analysis was also conducted, excluding one patient in the intervention group based on a post randomization decision that the patient was a potential clinical outlier due to significant morbidity from newly diagnosed cancer. The primary comparison was of PWT relative change from baseline to 14 weeks post-treatment between the intervention and control groups. Separate one-way within-subject analyses of covariance (ANCOVA), including previous peripheral endovascular therapy as an a priori defined covariate, were performed on PWT change scores from baseline to week 14 compared between intervention and control groups. Secondary outcomes included COT, VO2peak, functional ability and patient-reported outcomes from the WIQ and SF-36. Normality assumptions of ANCOVA were assessed prior to analyses. Significance was set a priori at α=0.05. Statistical analyses were performed with the IBM SPSS statistics package (Version 21.0, IBM Corp, Armonk, NY). In addition, the response in the two main subgroups of patients (those with previous peripheral endovascular therapy versus those without) was tested for interaction with a two-way between-subjects analysis of variance. No significant interaction was found, thus the results are reported for all patients combined. The study used standard approaches to determine power and for guiding the overall statistical analyses. After evaluation of assumptions of parametric testing (e.g. normality), we noted no considerable deviations and did not perform data transformation prior to statistical analyses.
Walking exercise compliance was calculated as the total number of completed exercise sessions divided by 42 (3 sessions∙weekˉ1 for 14 weeks). 35 A session was counted as complete when evidence of training was demonstrated by both the piezoelectric activity monitor and walking exercise log. Confirmation of exercise from the activity monitor required at least 10 minutes (within a 35–50 minute window) of moderate activity on the activity monitor (10 steps∙minˉ1 or more).
Sample size was calculated for change in PWT from baseline to 14 weeks post exercise treatment. The control group effects and pooled standard deviation estimates were based on data within a clinical trial conducted by our group examining PWT in a similar PAD patient population. 35 A sample of 18 patients per arm (total sample n=36) was estimated to provide 80% power at α=0.05 to detect a net 25% difference in PWT between groups at 14 weeks. A pooled standard deviation on the log ratio of 0.4 was used based on historical data. 36
Results
Sixty-three patients were initially screened from June 2010 to March 2013, of whom 38 were not randomized. Of these 38, 20 failed initial phone screening due to exclusionary criteria and 18 did not meet study inclusion criteria during the screening visit. Thus, 25 patients were randomized to either the intervention or control group. Twenty patients completed both baseline and post-14 week outcomes assessment and were used in the ITT analyses. Change score outcomes were analyzed for a total of 19 patients (intervention: n=9; control: n=10) as additional exploratory analyses due to one patient being diagnosed with advanced metastatic cancer (renal cell carcinoma with metastatic brain lesion) shortly following 14-week outcomes assessment (deemed a clinical outlier). Table 1 provides baseline characteristics for PAD patients included in the ITT (n=20) and exploratory (n=19) analyses as well as those not included in the final analyses due to a lack of evaluable data post randomization (n=5). Patients randomized to the control group had a higher resting heart rate (p=0.009) and weight (p=0.04) at baseline compared to patients in the intervention group for the ITT analysis. There were no other statistical differences noted from the ITT analysis at baseline between intervention and control group patients for demographic characteristics or baseline exercise performance outcomes.
Baseline characteristics for the intent-to-treat and exploratory analyses and patient dropouts.
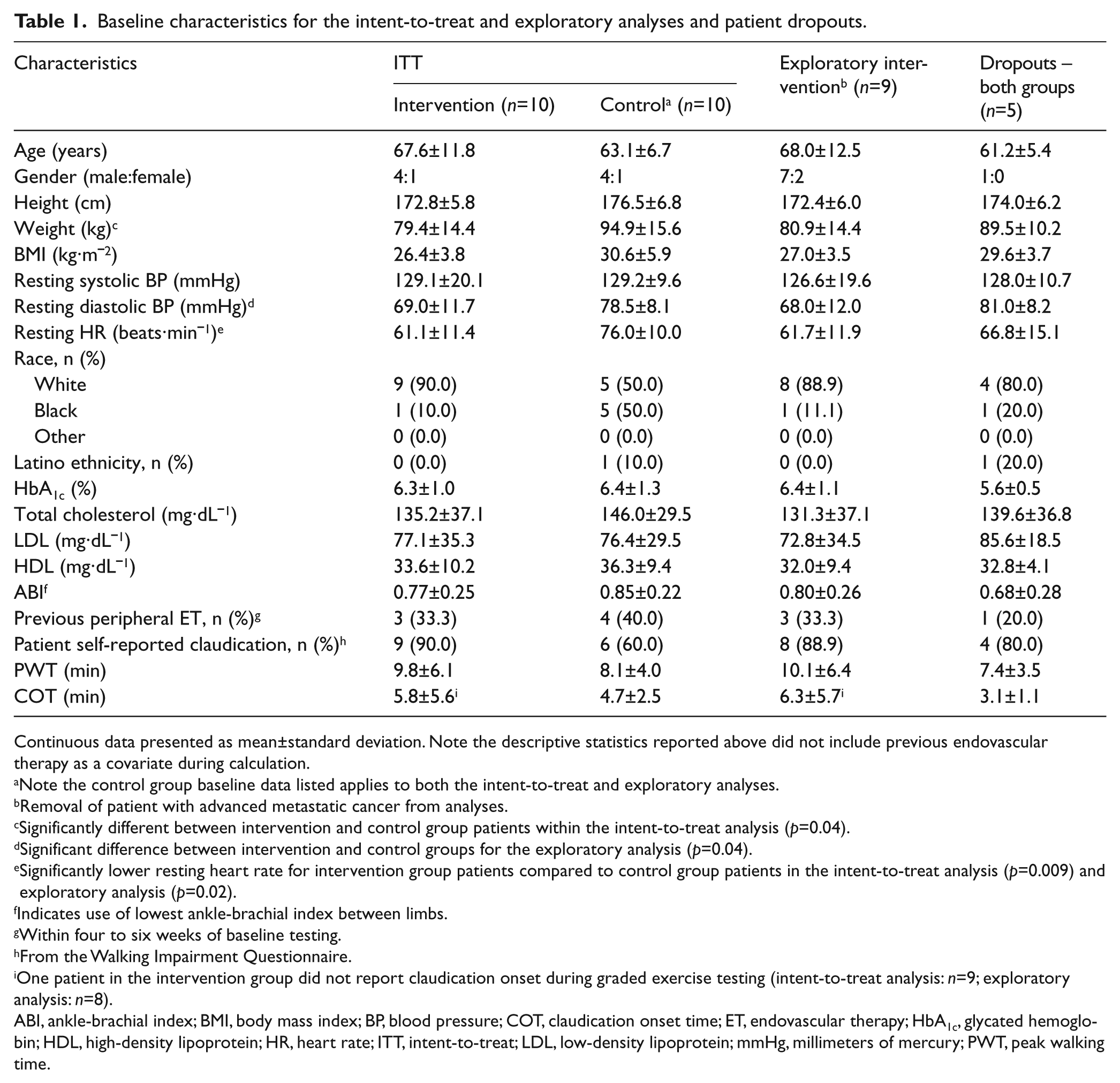
Continuous data presented as mean±standard deviation. Note the descriptive statistics reported above did not include previous endovascular therapy as a covariate during calculation.
Note the control group baseline data listed applies to both the intent-to-treat and exploratory analyses.
Removal of patient with advanced metastatic cancer from analyses.
Significantly different between intervention and control group patients within the intent-to-treat analysis (p=0.04).
Significant difference between intervention and control groups for the exploratory analysis (p=0.04).
Significantly lower resting heart rate for intervention group patients compared to control group patients in the intent-to-treat analysis (p=0.009) and exploratory analysis (p=0.02).
Indicates use of lowest ankle-brachial index between limbs.
Within four to six weeks of baseline testing.
From the Walking Impairment Questionnaire.
One patient in the intervention group did not report claudication onset during graded exercise testing (intent-to-treat analysis: n=9; exploratory analysis: n=8).
ABI, ankle-brachial index; BMI, body mass index; BP, blood pressure; COT, claudication onset time; ET, endovascular therapy; HbA1c, glycated hemoglobin; HDL, high-density lipoprotein; HR, heart rate; ITT, intent-to-treat; LDL, low-density lipoprotein; mmHg, millimeters of mercury; PWT, peak walking time.
Exercise compliance
For patients enrolled into the intervention group, exercise compliance rates were very high, with patients completing 81.9±25.6% (mean±standard deviation) of walking exercise sessions prescribed (dose of exercise equaling 344 of 420 total walking exercise sessions prescribed across all patients).
Exercise performance outcomes
The ITT analyses when controlling for previous peripheral endovascular therapy indicated there were no significant differences for the primary endpoint PWT from baseline to post 14 weeks between intervention PAD and control group PAD patients (mean±standard error: 9.8±1.7 to 11.9±1.8 min versus 8.2±1.7 to 8.2±1.8 min, p=0.052). The exploratory analysis, removing the one patient who developed cancer post randomization, indicated patients enrolled into the intervention group showed significant group mean improvement for PWT change scores (10.1±1.8 to 12.4±1.9 min) from baseline to post 14 weeks assessment compared with control group patients (8.2±1.7 to 8.2±1.8 min, p=0.037). Group mean improvements in COT were demonstrated for patients in the intervention group (n=9) compared with control group patients (n=8) when including previous peripheral endovascular therapy as a covariate in the model for both the ITT (5.8±1.5 to 7.4±1.6 min versus 4.7±1.4 to 4.1±1.5 min, p=0.045) and exploratory (6.3±1.6 to 8.1±1.7 min versus 4.7±1.4 to 4.1±1.5 min, p=0.046) analyses. Figures 1 and 2 depict primary and secondary walking outcomes for intervention and control group patients at baseline and 14 weeks based on group means. Analysis of VO2peak indicated no significant improvements between intervention and control patients from baseline to post 14 weeks for both ITT (17.5±1.3 to 18.7±1.3 ml∙kgˉ1∙minˉ1 versus 15.0±1.3 to 15.7±1.3 ml∙kgˉ1∙minˉ1, p=0.66) and exploratory (17.7±1.4 to 19.1±1.4 ml∙kgˉ1∙minˉ1 versus 15.0±1.3 to 15.8±1.3 ml∙kgˉ1∙minˉ1, p=0.60) analyses.
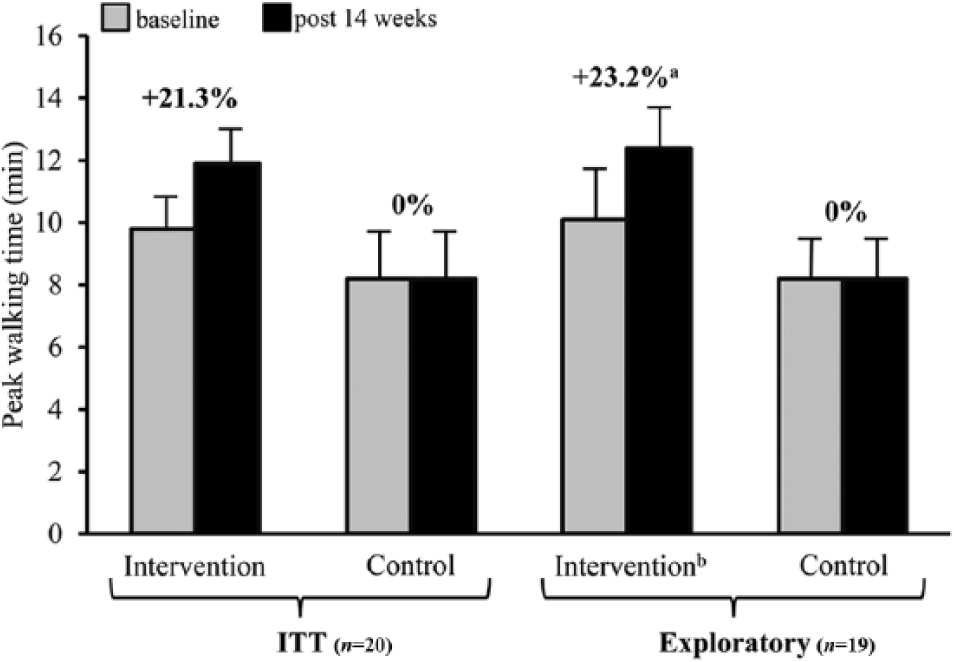
Primary walking performance outcome from the intent-to-treat and exploratory analyses at baseline and 14 weeks for intervention and control group patients.
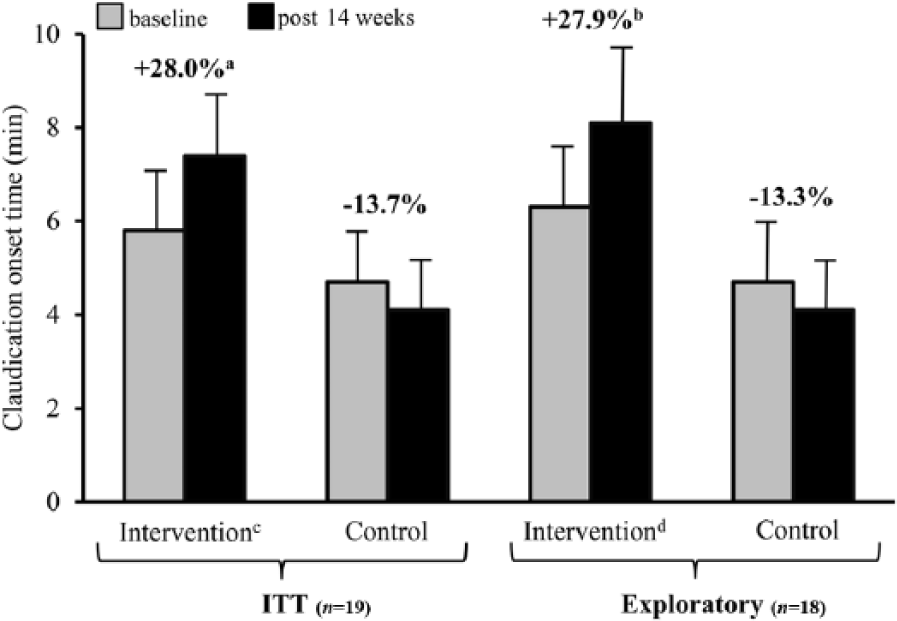
Secondary walking performance outcome from the intent-to-treat and exploratory analyses at baseline and 14 weeks for intervention and control group patients.
Functional ability and patient-reported outcomes
Functional ability assessed by the 4-m walking velocity at the patient’s fastest pace improved significantly (p<0.001) from baseline to post 14 weeks for intervention group patients (1.3±0.1 to 1.5±0.1 meters·sec-1) compared to control group patients (1.4±0.1 to 1.3±0.1 meters·sec-1) in the ITT analysis as well as for the exploratory analyses (1.3±0.1 to 1.5±0.1 meters·sec-1 versus 1.4±0.1 to 1.3±0.1 meters·sec-1, p<0.001). The usual pace 4-m walking velocity was not different (p=0.062) in the ITT analysis for patients randomized to the intervention group (1.0±0.06 to 1.1±0.0 meters·sec-1) compared to control group patients (1.0±0.06 to 1.0±0.0 meters·sec-1) and the exploratory analyses (1.0±0.1 to 1.1±0.0 meters·sec-1 versus 1.0±0.1 to 1.0±0.0 meters·sec-1, p=0.059). The ITT and exploratory analyses also indicated no differences in change scores from baseline to post 14 weeks between groups for repeated chair rises assessed by the SPPB for intervention or control groups (ITT: 11.7±2.1 to 8.6±0.6 sec versus 10.7±2.1 to 10.7±0.6 sec, p=0.26; exploratory: 11.7±2.2 to 8.2±0.6 sec versus 10.7±2.1 to 10.7±0.6 sec, p=0.23). Additionally, ITT and exploratory analyses results indicated no differences in balance change scores assessed by the SPPB from baseline to post 14 weeks between intervention (ITT: 3.4±0.2 to 3.4±0.3 points; exploratory: 3.3±0.2 to 3.3±0.3 points) and control (ITT: 3.7±0.2 to 3.8±0.3 points, p=0.76; exploratory: 3.7±0.2 to 3.8±0.3 points, p=0.79) group patients. Analysis of change in SPPB total scores in the ITT and exploratory analyses pre and post 14 weeks also resulted in no statistical difference between intervention (ITT: 10.9±0.5 to 11.3±0.3 points; exploratory: 10.9±0.5 to 11.3±0.3 points) and control group patients (ITT: 11.2±0.5 to 11.2±0.3 points, p=0.65; exploratory: 11.2±0.5 to 11.2±0.3 points, p=0.60).
Community-based walking ability measured by the combined WIQ dimensions using the ITT population significantly improved for the intervention group compared to the control group from baseline to post-14 weeks assessment (42.3±7.7 to 60.6±7.2% versus 49.1±7.7 to 44.6±7.2%, p=0.001). The exploratory analysis also resulted in significant change (p=0.001) from baseline to post 14 weeks for PAD patients enrolled in the intervention group (45.1±8.1 to 64.4±7.2%) compared to the control group (49.5±7.7 to 44.8±6.8%). When examining individual dimensions within the WIQ employing ITT and exploratory analyses, patients’ perspectives on their ability to walk specific distances and speeds improved for intervention group patients compared to control group patients (ITT distance: 40.4±10.4 to 60.3±10.5% versus 51.8±10.4 to 44.5±10.5%, p<0.001; exploratory distance: 43.7±11.0 to 65.4±10.7% versus 52.1±10.4 to 44.9±10.1%, p<0.001; ITT speed: 43.1±7.2 to 59.7±6.4% versus 44.7±7.2 to 37.3±6.4%, p=0.004; exploratory speed: 46.1±7.5 to 62.6±6.6% versus 44.9±7.1 to 37.5±6.3%, p=0.006). There was no statistical difference between groups for the WIQ stair climbing dimension at post 14 weeks assessment for either ITT (intervention: 43.2±9.3 to 61.8±9.5%; control: 50.9±9.3 to 52.0±9.5%, p=0.24) or exploratory (intervention: 45.7±10.0 to 65.3±9.9%; control: 51.4±9.4 to 52.1±9.4%, p=0.23) analyses. Analyses of patient-reported outcomes pre and post 14 weeks assessed by the SF-36 indicated no statistical differences between intervention and control groups regardless of analyses employed. Functional ability and patient-reported outcomes at baseline and change scores at post 14 weeks are depicted in Table 2.
Functional ability and patient-reported outcomes at baseline and change after 14 weeks for the intent-to-treat and exploratory peripheral artery disease patient populations.
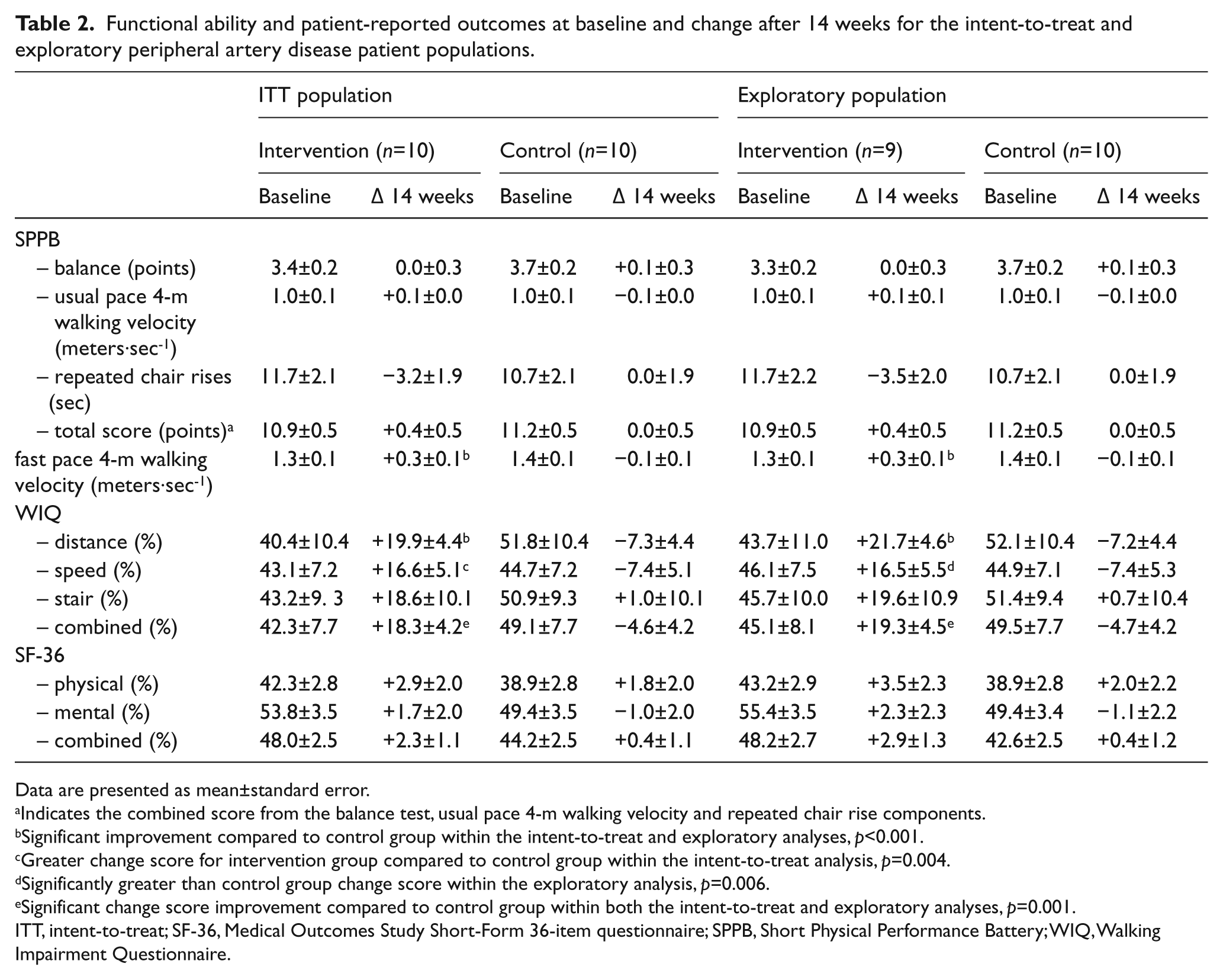
Data are presented as mean±standard error.
Indicates the combined score from the balance test, usual pace 4-m walking velocity and repeated chair rise components.
Significant improvement compared to control group within the intent-to-treat and exploratory analyses, p<0.001.
Greater change score for intervention group compared to control group within the intent-to-treat analysis, p=0.004.
Significantly greater than control group change score within the exploratory analysis, p=0.006.
Significant change score improvement compared to control group within both the intent-to-treat and exploratory analyses, p=0.001.
ITT, intent-to-treat; SF-36, Medical Outcomes Study Short-Form 36-item questionnaire; SPPB, Short Physical Performance Battery; WIQ, Walking Impairment Questionnaire.
Discussion
This pilot study in PAD patients found that a community-based program of walking exercise with elements of TMC did not improve PWT significantly compared to results in a non-exercising control group. Other measures of walking ability (i.e. COT), functional ability (i.e. fast pace 4-m walking velocity) and patient-reported outcomes were improved by this program for both the ITT and exploratory analyses. This pilot provides some evidence that innovative methods may be beneficial for PAD patients walking in community settings. Results should be interpreted as preliminary however, given the limitations in the study design.
Several studies have recently proposed community-based walking exercise programs with novel components.12-14,35 McDermott et al. 12 conducted a six-month walking exercise group-mediated cognitive behavioral intervention in PAD patients (n=194) that used social cognitive theory, principles from group dynamics research, and self-regulation to guide the trial. Patients in the treatment group received instruction on how to improve health followed by 45 minutes of supervised walking exercise (at an indoor track). Patients were also advised to exercise for 5 days∙weekˉ1 up to 50 minutes∙sessionˉ1, which included instructions to walk until they experienced severe leg pain. Control patients participated in weekly health education group sessions as well as health management lectures. Change in six-minute walk distance (primary outcome) was significantly different for treated patients compared to control patients (+42.4 versus −11.4 m, p<0.001). This study highlighted a new approach to community-based programs in PAD by using supervised walking groups. This is important as elements of TMC such as in the McDermott et al. trial may be needed for PAD walking programs. However, we chose to provide individualized instruction and one-on-one support in our study rather than group-based walking exercise. Thus, results from previous successful walking exercise trials12,13 and our trial using exercise supervision at community locations rather than in clinical settings, may be the appropriate approach for developing a comprehensive community-based walking exercise program for PAD patients.
Our study employed a walking exercise program individually tailored for patients at locations where they could successfully complete the prescribed exercise and where they received three supervisory visits and were monitored over the course of the study. The community walking exercise environment itself may be challenging for PAD patients, as there are numerous individual and disease-specific barriers potentially preventing successful completion of the program.37–39 Evaluations of the local walking environment using audit tools can provide assessments of factors (e.g. quality of sidewalks) that could potentially limit physical activity participation.40,41 Thus, the built environment should be considered when designing walking exercise programs in the community setting; something we were able to address. PAD patients may also experience severe leg pain when they walk which is a major barrier cited by a previous focus group study in PAD. 42 Our intervention improved walking outcomes in PAD patients by circumventing community-based barriers to physical activity (e.g. lack of a place to sit) by facilitating ease of walking (e.g. providing patients with a portable chair for seating). The acknowledgement of problems that may occur in community settings is paramount to the success of any community-based walking exercise program as simple advice to go home and walk has been unsuccessful for improving PAD patients’ walking ability.
There were several limitations of the current study which include: 1) small sample size, 2) inadequate blinding of outcome assessors for patient study group assignment, 3) familiarization effect with the upfront treadmill training at the hospital, 4) lack of a true attention control group, and 5) moderately high dropout rate for post-14 week outcome assessments. The small sample size may have limited interpretation of the oxygen uptake data as well as the SF-36 results due to a smaller effect size on those variables than for PWT and COT. There were potential confounders to our interpretation of the data due to the limited patient sample. This, in addition to the loss to follow-up, warrants caution when interpreting the results of the current pilot trial. Additionally, given adequate resources such as in large-scale, fully-funded trials or having strong preliminary evidence to conduct a larger trial, complete blinding of investigators during outcomes assessment is warranted. At a minimum, we felt it was important to blind investigators and patients until after baseline outcome assessments. The familiarization of patients during the initial two weeks (six total sessions) with the exercise modality (i.e. treadmill) used for walking performance outcome assessments is a concern as patients may have experienced a learning effect. Our intention was to develop and test a generalizable pilot program of exercise in a community setting for PAD patients and the initial two weeks was important for coaching patients on the appropriate exercise prescription needed for improvement of outcomes. Future trials should provide less training in a hospital setting as PAD patients will be walking primarily in community settings. Because this was a pilot study, we restricted our analyses to patients who completed the protocol and had post randomization data available (ITT analyses). An exploratory analysis excluded one patient who developed cancer that limited their exercise performance independent of their PAD. Our analytic approach was chosen to best define both the feasibility of the exercise intervention in patients limited by PAD and also demonstrated the potential optimal responses. Thus, we did not utilize any method to impute for missing data (e.g. centering, algorithmic method) since our intention was to test the methods and feasibility of our design.
This study implemented a new approach building on current successful studies12–14 for encouraging patients to actively participate in a community-based exercise program. Patients set training goals with the investigators, were monitored over the course of the study and were also taught to self-monitor their exercise while learning to problem-solve issues that arose during exercise in the community. This study addressed specific barriers such as lack of adequate places for PAD patients to rest due to IC by providing lightweight, portable walking chairs and also implemented a new approach to getting patients to actively participate in the exercise program by thoroughly reviewing each patient’s local walking area using an environmental audit tool. It is important to incorporate program evaluation, such as patient completion of activity logs and problem-solving discussions, to allow adjustments to program components as necessary. Programs may need to consistently incorporate the strengths of supervised walking exercise programs focused on the PAD patient. This pilot study may serve as the basis for large, randomized controlled trials to establish community-based walking exercise as an effective, adjunct therapy for patients with PAD.
Footnotes
Declaration of conflicting interest
Dr Hiatt is the director of a clinical trials research organization (CPC Clinical Research) that manages trials evaluating new treatments for PAD. Sponsors for relevant projects include Pluristem, AstraZeneca, Bayer, the Cardiovascular Cell Therapy Research Network and Cardiovascular Systems, Inc. Dr Regensteiner is principal investigator of four grants including a NIH K12 HD057022, a Clinical/Translational Research Study from the American Diabetes Association and two Investigator Initiated Research Studies; one from Bristol Myers Squibb and one from Merck, respectively. None of these grants are related to PAD. Dr Ho is a consultant for Anthem, Inc which is unrelated to the current publication. The other authors note no conflicts.
Funding
The study was supported by the National Institutes of Health/National Center for Research Resources Colorado Clinical Translational Science Institute (grant number UL1 RR025780); and the National Institutes of Health/National Heart, Lung, and Blood Institute National Research Service Awards (grant numbers T32HL007822–11A2, F32HL105095–01A1) for Dr Mays.