
Abstract
Proximal claudication is secondary to ischemia caused by peripheral artery disease (PAD), whereas proximal pseudo-claudication is secondary to other disease processes such as hip arthritis, spinal stenosis, neuropathy, and so forth. The differentiation between the two can be challenging. Exercise transcutaneous oxygen pressure measurement (exercise-TcPO2) allows noninvasive detection of flow-reducing lesions in the proximal arteries and tributaries of the lower extremity arterial tree. We present the first case report in the United States using an exercise-TcPO2 algorithm. A 71-year-old diabetic patient with proximal left-sided and right-calf claudication with indeterminate ankle-brachial indices underwent an exercise-TcPO2 study before and after endovascular intervention. Four TcPO2 probes were placed: one at chest level (reference probe), one on each buttock, and one on the symptomatic calf. The Delta from Resting Oxygen Pressure (DROP) index was calculated at each probe site using a previously validated protocol. Proximal left- and right-calf ischemia were confirmed by the initial exercise-TcPO2, and, after endovascular treatment of the left iliac artery lesion, improvements in proximal exercise-TcPO2 values were found. These data suggest that exercise-TcPO2 can be useful in PAD evaluation in patients with non-compressible arteries and/or proximal claudication.
Keywords
Introduction
Lower limb pain while walking is a frequent symptom in elderly patients. 1 Pain that is absent at rest, appears during walking, forces the patient to stop, and is relieved by a brief period of rest, suggests a vascular origin and true claudication. Pain that involves the lower back, hip, buttock, or thigh, suggests proximal claudication (often simply referred to as “buttock” claudication, which may inappropriately limit the anatomic region[s] of involvement). It is known, however, that these symptoms may also represent pseudo-claudication resulting from diseases other than peripheral artery disease (PAD), 2 such as lumbar spinal stenosis,3,4 sciatica, or hip osteoarthritis. 5 As noted by Kauppila et al., a combination of these entities is frequent, often making the diagnosis of proximal claudication very challenging,6–8 and recent papers have shown that proximal claudication is underestimated.9,10 The American College of Cardiology/American Heart Association (ACC/AHA) statements suggest measuring ankle-brachial indices (ABIs), pulse volume recordings, segmental pressures, duplex ultrasound and/or exercising testing with ABI to evaluate claudication versus pseudo-claudication. 2 Near Infra-Red Spectroscopy (NIRS) and penile-brachial index have also been proposed by some authors but their accuracy in assessing proximal claudication is debatable.11–13
Since 2003, an exercise transcutaneous oxygen pressure measurement (exercise-TcPO2) protocol has been used in France to diagnose proximal claudication due to PAD. 14 Exercise-TcPO2 has demonstrated good sensitivity (79%) and specificity (86%) to detect significant lesions (stenosis⩾75%) in the arterial tree of the pelvic circulation when compared to angiography as a gold standard. 14 Their algorithm monitors the cutaneous TcPO2 overlying the area of discomfort during treadmill exercise as a marker of local arterial supply. We report below the first case in the United States of a patient with proximal claudication being evaluated by an exercise-TcPO2 protocol both before and after angioplasty.
Case history
A 71-year-old man presented with six months of worsening left buttock discomfort on ambulation. Cardiovascular risk factors included hypertension, current smoking, diabetes, and dyslipidemia. Radiographic imaging of the lumbar spine and hips found mild to moderate degenerative disk disease at L4, moderate to advanced lower lumbar facet arthropathy with spinal canal narrowing, and mild degenerative arthritis of both hips. He also reported a history of right-calf claudication that had been stable for five years. Studies were performed and their results included:
- Ankle-brachial indices measured in both the dorsal pedis and posterior tibial arteries on both limbs were indeterminate (systolic pressures >255 mmHg) due to poorly compressible vessels.
- Continuous wave Doppler waveforms before the treadmill test from the common femoral arteries on both sides were biphasic, and from the ankle arteries were monophasic on both sides related to PAD (Figure 1). The continuous wave Doppler waveforms results indicated that the lesions were distal to the common femoral and proximal to the below-knee arteries.
- After the completion of a treadmill test using a speed of 1.5 mph and a 10% grade, systolic pressures remained elevated (>255 mmHg) at 1 minute for both ankles.
- The treadmill test was terminated at 1 minute 55 seconds due to left-leg pain from the buttock to the calf, with no symptoms in the right limb. The electrocardiogram was negative for coronary ischemic changes.
In addition to the standard vascular assessment, the patient participated in an exercise O2 study that was approved by the Institutional Review Board. Exercise-TcPO2 was performed according to the published French algorithm as previously described. 14 Briefly, measurement of TcPO2 was performed using calibrated TcPO2 probes (TCOM/TcPO2; PF 5040 TcPO2/CO2 Unit; Perimed®; Jarfalla, Sweden). The temperature of each probe was set to 45°C, which allows maximal vasodilation and decreases the arterial to skin surface oxygen pressure gradient. A reference electrode (chest probe) was placed between the scapulae to measure systemic changes in TcPO2 during exercise. 15 One electrode was positioned on each buttock, 4 to 5 cm behind the bony prominence of the trochanter, and one electrode on the most symptomatic calf, which was the right calf according to the patient. Once the electrodes were in position, a period of 10 minutes in the standing position was required to stabilize the electrodes to obtain baseline values. Exercise was performed on a treadmill at a 10% slope and a speed of up to 2 mph, a different protocol from the routine initial test for post exercise ABI measurement, but one that corresponded to the protocol published in the original validation study. 14 A 12-lead ECG monitored heart rate and rhythm for ischemic changes during the exercise test procedure. The patient was encouraged to walk for the longest time possible to mimic his symptoms of claudication. Exercise was discontinued at the patient’s request (or, by protocol, up to maximum exercise duration of 12 minutes). 16
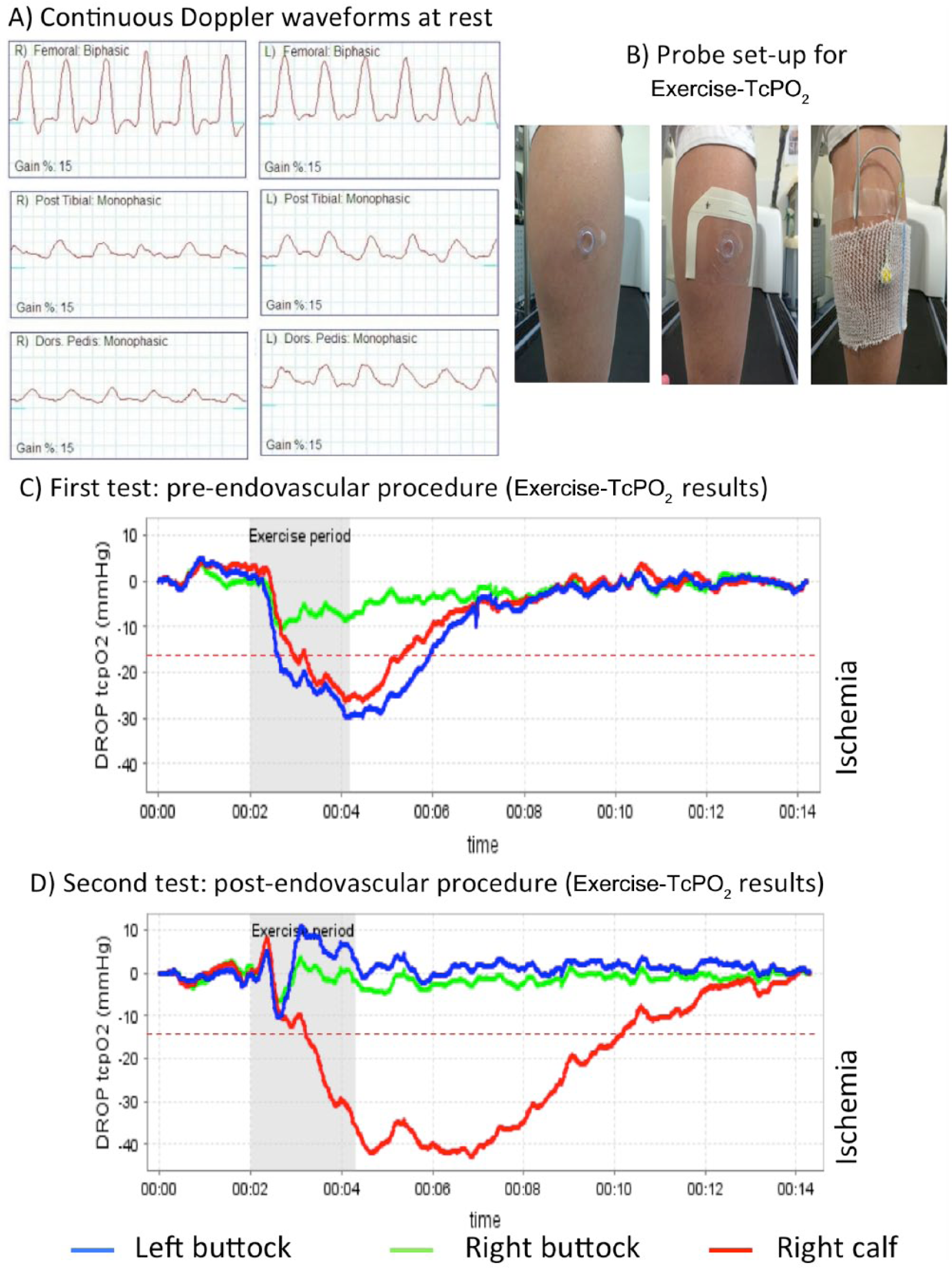
Results of vascular laboratory investigations. A: Continuous wave Doppler waveforms at rest. B: TcPO2 probe fixation using Tegaderm® and Surgifix®. C and D: DROP, Delta from Resting Oxygen Pressure. An endovascular procedure was performed that successfully stented the left common iliac artery; attempted recanalization of the occluded right popliteal artery was unsuccessful.
The measurements from the TcPO2 electrodes were used to calculate the Delta from Resting Oxygen Pressure (DROP) index (expressed in mmHg), the absolute change in TcPO2 from resting value in each of the three limb probes, corrected for the absolute change in TcPO2 at the chest electrode. The equation for the DROP index is as follows:
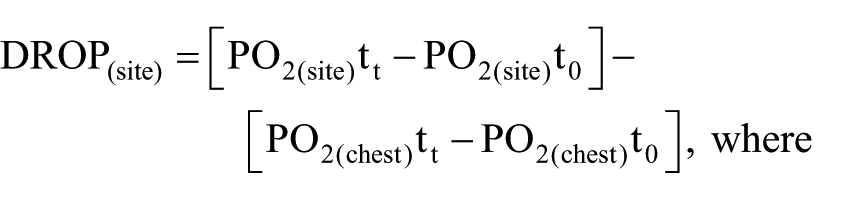
PO2(site)tt is the oxygen pressure at a measurement site at time t, PO2(site)t0 is the mean oxygen pressure at a measurement site over the baseline resting period; PO2(chest)tt is the oxygen pressure at a chest site at time t and PO2(chest)t0 is the mean oxygen pressure at a chest site over the resting period. The DROP index was automatically calculated and displayed graphically by a dedicated software package that allowed real-time monitoring of DROP values at the levels where the probes were placed. 14
The lowest DROP value during exercise has been shown to be accurate and reliable in predicting the presence or absence of severe arterial stenosis, as compared to angiography, at the buttock and ankle levels.14,17 Previous results at the buttock 14 and distal levels 17 have shown that a DROP value lower than −15 mmHg suggests ischemia is present at the TcPO2 probe site (see Video 1: online supplementary data showing the procedure to perform Exercise Transcutaneous Oxygen pressure measurements).
The results of the exercise-TcPO2 study were a walking time of 2 minutes 11 seconds, with left-buttock discomfort that forced the patient to stop. There was an appropriate increase in chest probe TcPO2 value during exercise.15,18 TcPO2 DROP values at the left buttock, right buttock and right calf were −30 mmHg, −11 mmHg and −26 mmHg, respectively (Figure 1), consistent with ischemia at the left buttock and the right calf.
Computed tomography angiography (CTA) confirmed the presence of a severe left common iliac artery stenosis (which could not be quantified as a percentage luminal reduction due to a heavy calcification, as noted by the interpreting radiologist), a moderate stenosis of the left internal iliac artery, a moderate right common iliac stenosis, a moderate right internal iliac artery stenosis and complete occlusion of the right popliteal artery.
Endovascular revascularization and stenting was successful on the left common iliac artery, but attempted recanalization of the occluded right proximal popliteal artery was unsuccessful.
Two days after the endovascular procedure the patient underwent a second exercise-TcPO2 study. He walked for 2 minutes and 18 seconds, 7 seconds more than during the pre-procedure test. Walking was stopped due to a general weakness and right-calf claudication, but no left-buttock pain occurred. At the left-buttock, right-buttock and right-calf levels, DROP values were −11 mmHg, −7 mmHg and −43 mmHg respectively (Figure 1), suggesting improved perfusion to the left buttock and persistent ischemia of the right calf.
Discussion
This case is the first report of the exercise-TcPO2 technique in the United States. It shows that exercise-TcPO2 may be done in patients with exercise-induced proximal lower-limb pain. It confirms the presence of a regional buttock blood flow impairment during exercise as a likely significant contributing cause of proximal walking induced pain, even while multiple potential other etiologies are present. Further, it demonstrates improvement in the exercise-TcPO2 after treatment. 14 The present case also illustrates that exercise-TcPO2 is useful in a patient with non-compressible vessels, which make post-exercise ABIs invalid. The toe-brachial index could have been used to show the presence of obstructive disease, but it is not specific for buttock ischemia.19,20
The maximal walking durations for pre- and post-intervention exercise-TcPO2 testing were almost identical. This likely resulted from either (i) the fact that the popliteal artery occlusion was still present and distal perfusion may have been worsened by the procedural occlusion of small collateral vessels, or (ii) the interval between the endovascular procedure and the retest was too short (two days). This study confirms the feasibility of the protocol at an institution distinct from the site where the majority of the reproducibility studies for the proximal level and distal levels (r2=0.82 and r2=0.80, respectively) were initially performed.15,21
Determining the etiology of proximal claudication is often challenging due to both unique and concomitant diseases that may explain symptoms in the patient. Finding the true origin is important in order to avoid performing unnecessary or inappropriate treatments. Resting ABI and Doppler waveforms at rest at the common femoral artery can help to localize a significant stenosis, but only when the stenosis is axial, thus missing information about the internal iliac arterial system. Exercise-TcPO2 allows assessment of the internal iliac system but does not specifically define the location of lesions either. 22 Ideally, with a system of 5 or more channels, both buttocks and calves could be monitored at the same time allowing the simultaneous analysis of proximal and distal ischemia on both sides.23,24
For a patient with intermittent claudication, AHA statements suggest evaluation with duplex ultrasound. 2 Moneta et al. showed that sensitivity and specificity for the diagnosis of stenoses greater than 50% diameter to the iliac or common femoral arteries were 88% and 97%. 25 For the detection of greater than or equal to 50% aortoiliac stenoses, a peak systolic velocity ratio ⩾2.8 provided 86% sensitivity and 84% specificity (positive predictive value, 84%; negative predictive value, 85%; accuracy, 85%). 26 Despite these excellent results, it has also been reported that on a multi-center basis, “routine” ultrasound has a poor sensitivity (41% [34%−47%]) and fair specificity (81% [72%–87%]) to detect a vascular origin in patients complaining of proximal claudication. 27 In “routine” use, many angiologists either do not report results for the internal iliac arteries or report that these arteries were not adequately analyzed due to calcification or gaseous interposition. CTA is expensive, and requires contrast agents with the potential for renal and/or allergic complications, which limit its use as a primary diagnostic tool. A problem common to each of these tests is that they assess blood flow when the patient is at rest, whereas exercise-TcPO2 allows assessment of the blood flow during exercise, which is when symptoms occur.
Conclusion
This case study shows the utility of exercise-TcPO2 in a patient with known spinal stenosis and clinically suspected proximal claudication and with non-compressible tibial and dorsal pedis arteries. Further evaluation and dissemination of the use of this technique should lead to improved management and care of patients with peripheral arterial disease.
Footnotes
Acknowledgements
GM thanks the Société Française de Médecine Vasculaire and the Institut Servier, which gave to him grants for his post-doctoral fellowship at the Mayo Clinic, Rochester, MN, USA. GM received an ARIANES grant from the University of Angers.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.