
Abstract
The purpose of this study was to examine trends in racial and gender disparities in the severity of lower extremity amputation among individuals with peripheral artery disease (PAD) over the period of a decade (2002–2011). This is a longitudinal secondary analysis of data from the Healthcare Utilization Project Nationwide Inpatient Survey (HCUP-NIS) for the years 2002–2011. Level of amputation was determined from ICD-9-CM procedure and coded as either transfemoral (TF) or transtibial (TT). The main predictors were gender and race; covariates including age, race, income, insurance status and presence of vascular disease were incorporated as control variables in regression analysis. A total 121,587 cases of non-traumatic dysvascular amputations were identified. Female gender (odds ratio (OR) 1.35; 95% confidence interval (CI) 1.32, 1.39) and black race (OR 1.17; 95% CI 1.12, 1.23) are both significantly associated with increased odds for receiving TF amputation with no change in these odds over the decade of study. Other covariates with significant associations with TF amputation level include increased age (OR 1.03; 95% CI 0.99, 1.09), low income (OR 1.21; 95% CI 1.15, 1.27), Medicaid insurance (OR 1.36; 95% CI 1.29, 1.44), Medicare insurance (OR 1.27; 95% CI 1.21, 1.32), and cerebrovascular disease (OR 2.12; 95% CI 2.03, 2.23). In conclusion, although overall rates of amputation have decreased, disparities in level of amputation related to female gender and black race have not significantly changed over time. Higher-level amputation has significant consequences from a quality-of-life, medical and economic perspective.
Introduction
The elimination of health disparities is a primary goal of the Federal government, health care agencies, medical providers and medical stakeholders. The Department of Health and Human Service’s goals and objectives for the nation’s health, Healthy People 2000, 2010 and now 2020, consistently places the elimination of health disparities as a primary health care goal. 1 Even with increased resources and attention directed at achieving this goal, health disparities in the areas of health care access, quality and outcome remain unacceptably high. 2
Health disparities related to the treatment and outcomes of peripheral artery disease (PAD) are an ongoing problem that need attention.3,4 Amputation, as one possible outcome of PAD, has been observed to occur in a manner that is differential in terms of both race and gender.5,6 In the past decade, the overall amputation rate for patients with PAD declined slightly: one study computes the change from 7258 per 100,000 (2000) to 5790 per 100,000 (2008).7,8 However, even with this decline in amputation and the improvements in endovascular interventions, there are studies supporting the presence of health disparities related to the treatment and outcome of PAD.3,4
A recent ‘call to action’ statement by the American Heart Association highlights the disparity in treatment and diagnosis of PAD in women. 4 Cross-sectional research shows women to be at risk for a higher level of transfemoral (TF) over transtibial (TT) amputation when compared to men.5,9 Women have been found to be more likely to receive endovascular intervention for limb ischemia, when compared to surgical intervention, even though they are on average older and present with more severe disease when compared to men. 10 Women also demonstrate higher in-hospital mortality regardless of disease severity or procedure performed, even after adjusting for age and comorbidities. 10
Race also continues to be related to amputation rate, level, screening and use of endovascular interventions. Individuals of Black race have been found to be 1.77 times as likely as individuals of White race to receive lower extremity amputation, with the greatest disparity being found among those in a wealthier zip code. 4 Black race has not only been associated with the overall odds of receiving amputation in the presence of PAD, but also with an increased risk of TF or more severe amputation, when amputation occurs. 4 Black patients have also been found to experience fewer revascularization procedures when compared with white patients. 11
Higher-level or TF amputation is a medical decision that should be based solely on clinical presentation, and one that has significant consequences. Energy expenditure, balance confidence, and overall mobility are all impacted as the level of lower extremity amputation moves more proximally.12–14 In addition, the loss of the knee joint, which occurs with TF amputation, has a more significant impact on return to functional activities, such as the performance of activities of daily living, than amputees who maintain a knee joint.15,16 Many of the variables that contribute to the presence of health disparities, such as socio-economic status, employment, psychosocial stability and educational attainment, are also impacted as the level of amputation moves proximally. TF amputation has also been associated with higher rates of overall mortality, longer hospital stays and less frequent discharges to home. 9
This study builds on our previous work that was a cross-sectional analysis of a single year of 2007 Healthcare Utilization Project (HCUP) Nationwide Inpatient Survey (NIS) data. In that study we observed higher odds of a TF than a TT level of amputation for female gender and black race when compared to male gender and white race. 5 This is the first study to evaluate whether the disparity in severity or level of amputation is changing over time. A longitudinal trend study provides evidence to support or refute the premise that increased government attention and funding toward the elimination of health disparities has positively affected the population presenting with PAD. With improvements in pre-amputation screening and advancements in treating PAD, it is hypothesized that the health disparities found in previous studies would be reduced over the study period of 2002–2011, with fewer women and fewer black individuals experiencing the higher level and more severe TF amputations over time when compared to men and white individuals.
Methods
Data source
This study was approved via expedited review by the Institutional Review Boards of both Springfield College and Widener University. This study did not have an informed consent procedure as secondary retrospective data initially collected by the Agency for Health Care Research and Quality (AHRQ) were used for data analysis. This study used data from the HCUP-NIS from the years 2002–2011. HCUP is a family of databases containing longitudinal hospital care data that has been sponsored by AHRQ since 1988. The NIS is the database in HCUP that encompasses hospital inpatient stays from a national sample of more than 1000 hospitals representing 8 million stays on an annual basis. The NIS data approximate a 20% sample of community hospitals in the United States. The data include patient demographics, primary and secondary diagnoses, primary and secondary procedures and other variables that describe payment and hospital characteristics. AHRQ has made NIS data available yearly dating back to 1988. HCUP-NIS data have been used previously in cross-sectional analysis of both gender and race disparities in the level of amputation; the HCUP-NIS dataset is constructed to facilitate trend over time analysis.5,9
Study sample
From 2002 to 2011 a total of 121,587 unweighted cases of non-traumatic dysvascular amputations were identified in the NIS. To be included in the study sample, a discharged participant needed to be over 30 years of age and have a non-traumatic dysvascular amputation (84.15 and 84.17 in the ICD-9-CM codes). Discharges were identified as having a TT amputation by the ICD-9-CM procedure code 84.15, and as having a TF amputation by code 84.17. Amputation due to trauma was identified by the ICD-9-CM procedure codes 895–897 and these discharges were excluded from the data analysis.
Additional covariates were included in the sample development for analysis. The socio-demographic variables gender, age, race, income and insurance status were extracted directly from the NIS dataset. The category ‘other’ for insurance status encompasses worker’s compensation, CHAMPUS (Civilian Health and Medical Program of the Uniformed Services), CHAMPVA (Civilian Health and Medical Program of Veterans Affairs) and other government programs.
Discharged participants were identified as having a comorbid vascular disease by one of the following ICD-9-CM diagnosis codes for vascular diseases: hypertension (401.00–405.11), diabetes (250.00–250.90), peripheral vascular disease (440.00–441.00), ischemic heart disease/myocardial infarction (410.00–414.9), congestive heart failure (428.00–428.90), ulcers (707.00–707.90), gangrene (785.40) or cerebrovascular disease (430.00–438.90).
One limit of the NIS data was the amount of missing data on the variable that identified race in the discharged participants (25,443 cases). The distribution of this missing data results in a greater proportion of missing values in the first 5 years of our analysis (2002–2006). We undertook an analysis of the differences between those discharges in which there were missing data on the independent variables and those with complete data. As in our previous studies, we mitigated this loss of data by adding in a ‘missing’ category for the variable race. 5
Statistical analyses
Descriptive statistics for the sample were generated using the sample weights. We created a weighted ratio of the TT to TF amputations for each year of the survey and also for gender and race classifications. To analyze these trend data we used linear regression to assess the ratios: linear regression in this case provides an estimate equivalent to the chi-squared test for trend in proportions. Additional analysis consisted of chi-squared tests and multivariable logistic regression. All analyses used Stata/SE 12.0 survey commands employing Taylor series linearization methods as well as the appropriate longitudinal weight and strata variables as provided directly in the HCUP-NIS dataset for both computation of descriptive statistics and subsequent hypothesis-based analyses. The main analysis was the logistic regression to assess the effect of year along with the covariates and confounding variables on the likelihood of receiving a TF amputation (as opposed to a TT amputation).
Results
During the 10-year period between 2002 and 2011 there were 592,812 discharges with vascular amputation in US hospitals, of which 53.9% (95% confidence interval (CI) 53.3, 54.6) were TT and 46.1% (95% CI 45.4, 46.7) were TF. The number of amputations performed did decrease during the 10-year period (p for trend = 0.007) though visually the proportions of TT and TF amputations (Figure 1) and subsequently the ratio of TT to TF amputations show only small changes over time. Table 1 provides descriptive statistics and the bivariable analysis for the demographic characteristics for the sample. Highlights include a greater proportion of TT amputations among males (58.8%; 95% CI 58.2, 59.4), white individuals (54.3%; 95% CI 53.6, 55.1) or Hispanic ethnicity (61.4%; 95% CI 59.8, 62.9) and a greater proportion of TF amputations among females (53.1%; 95% CI 52.3, 53.8) and individuals who were identified as black (50.7%).
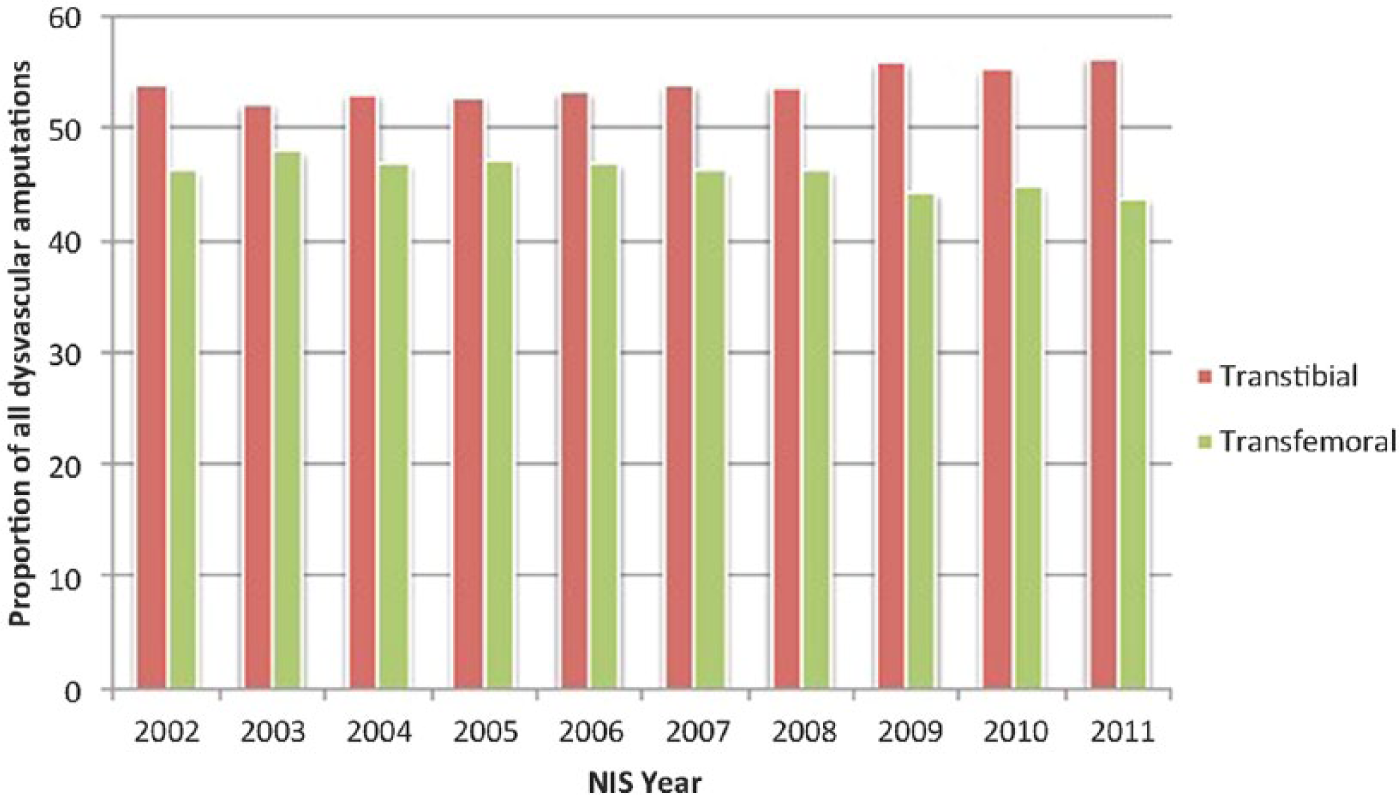
Proportion of total dysvascular amputations for HCUP data (2002–2011).
Sample characteristics for the full sample of adult NIS discharges 2002–2011 with vascular amputation.

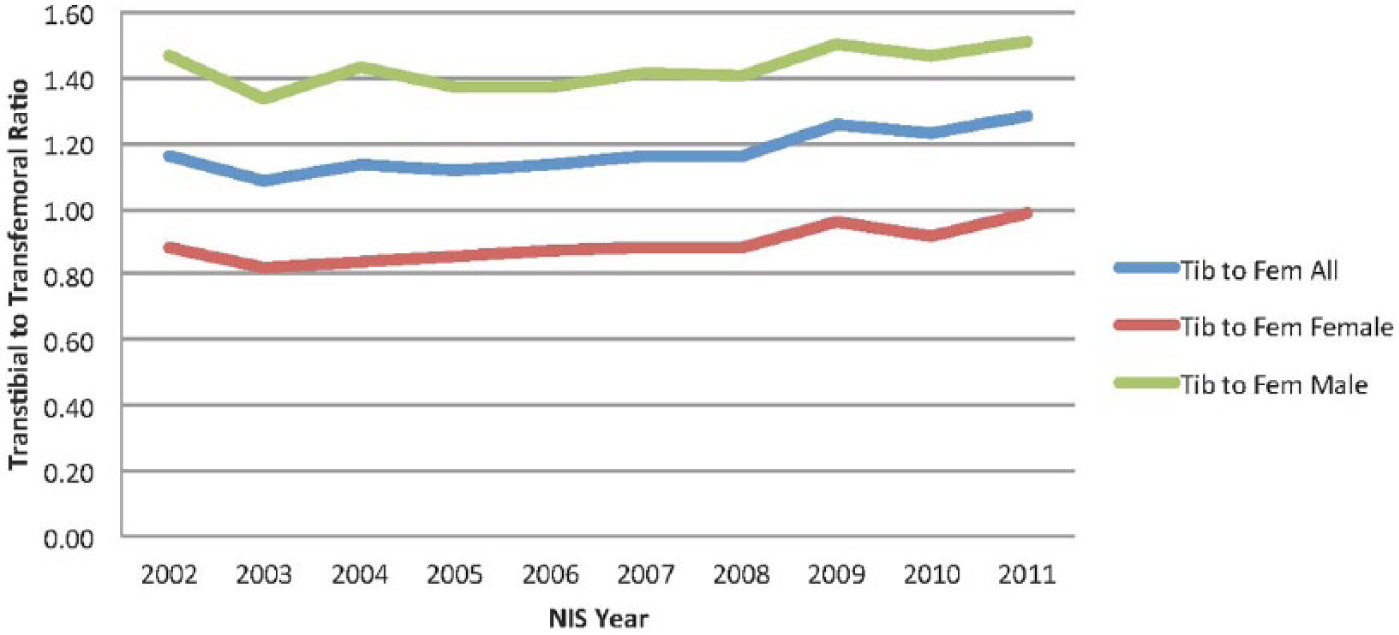
We calculated the ratio of TT to TF (TT/TF) amputations in all of our demographic subgroups and plotted these over time. Figure 2 demonstrates the relationship between TT and TF amputation over time and shows that the female ratio stays below the male ratio throughout the 10-year period and only at the end of the 10-year period begins to approach the 1.0 mark (p for trend <0.000). This indicates that, over time, females are receiving more TF amputations in relationship to TT when compared to men.
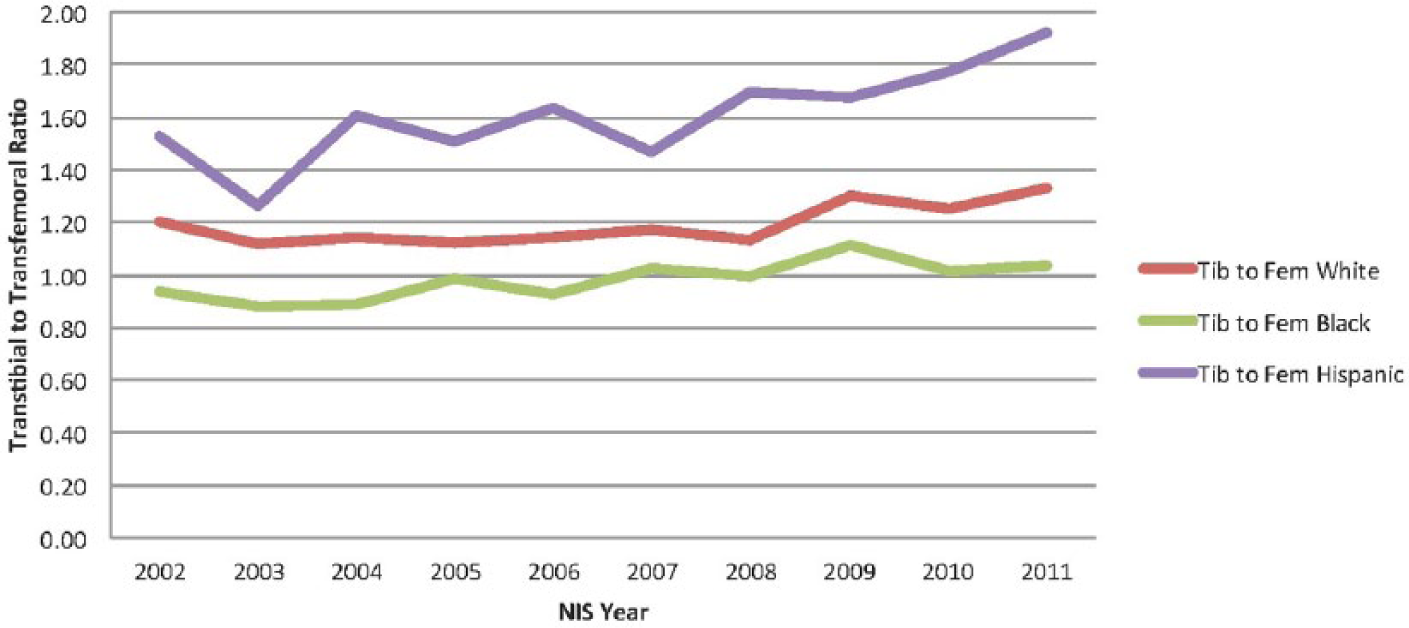
Transtibial to transfemoral ratio for white, black and Hispanic individuals for HCUP data (2002–2011).
When evaluating the TT/TF ratio with regard to race, Figure 3 shows the TT/TF ratio over the designated 10-year timeframe for three categories of the racial coding (black, white and Hispanic). In this sample population, those identified as black individuals do approach the TT/TF ratio 1.0 mark, but remain consistently below the TT/TF ratio of both white individuals and those identified as Hispanic (p for trend <0.000). It should be noted that the rate of TT/TF amputations for Hispanic individuals remains higher than 1.0, indicating that they are receiving TT amputations at much higher rates than TF amputations. In addition, the ratio follows a somewhat different pattern to that seen among those of both black and white individuals in the figure.
Transtibial to transfemoral ratio for white, black and Hispanic individuals for HCUP (2002–2011).
Finally, we conducted both bivariable analysis (Table 1) and multivariable logistic regression analysis (Table 2) incorporating year of discharge as a variable. Table 2 summarizes the results of the logistic regression analysis and provides adjusted odds for the likelihood of receiving a TF amputation (as compared to a TT amputation). Even after controlling for confounding variables, female gender (odds ratio (OR) 1.35; 95% CI 1.32, 1.39) and black race (OR 1.17; 95% CI 1.12, 1.23) are both significantly associated with increased odds for receiving TF amputation. Other covariates with significant associations with amputation level include increased age (OR 1.03; 95% CI 0.99, 1.09), low income (OR 1.21; 95% CI 1.15, 1.27), Medicaid insurance (OR 1.36; 95% CI 1.29, 1.44), Medicare insurance (OR 1.27; 95% CI 1.21, 1.32), and cerebrovascular disease (OR 2.12; 95% CI 2.03, 2.23).
Multivariable logistic regression analysis for level of amputation: adult NIS discharges 2002–2011 with vascular amputation.
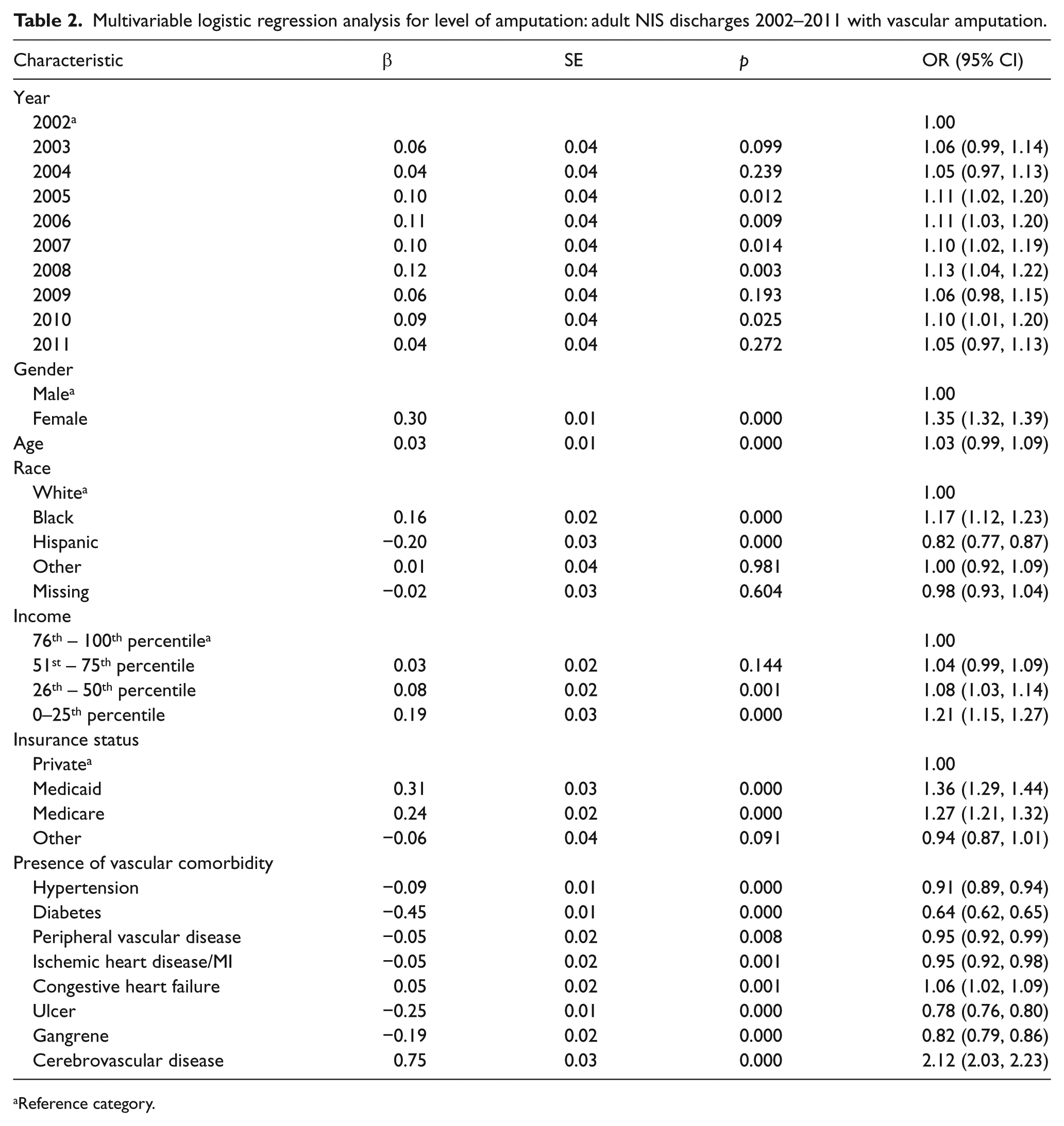
Reference category.
Discussion
The trend in amputation from 2002 to 2011, as demonstrated by this 10-year analysis of HCUP-NIS data, shows that TT amputation constituted 53.8% of amputations for PAD in 2002, while TF accounted for 46.2% of PAD amputations. Although the proportions show slight shifting over the 10-year period (Figure 1), the proportion of TT amputations is always higher than the proportion of TF. These findings are consistent with other studies that have evaluated the rate of amputation over time.7,9
The bivariable and multivariable logistic regression are also consistent with other findings in the literature around health disparities, PAD, and amputation.5,9,17 This analysis of multi-year HCUP-NIS data demonstrates that females and black individuals are at greater odds of receiving a TF amputation, even when controlling for other covariates that could affect these outcomes. These greater odds for TF amputation remain stable over time. Both females and black race populations with PAD may be in need of more specific, focused interventions to specifically address and target health disparities; current pre-amputation screening and use of the ankle–brachial index may not be enough to meaningfully affect this specific issue.
The other covariates found to have increased odds of TF amputation include increased age, low income, Medicaid insurance, Medicare insurance, and cerebrovascular disease. Other studies have found a similar relationship between age and TF amputation.5,9 As age increases, the likelihood for illness, cardiovascular illnesses such as PAD, increases. 18 Therefore, the potential for greater odds of TF amputation with increasing age and Medicare insurance exists. The TF amputation rate associated with age and Medicare could also be a reflection of their status in a high-risk patient subgroup, with age being associated with greater mortality post amputation procedure.19,20 In addition, repeat amputation is a possible explanation for the greater number of TF amputations seen with increasing age.
Other studies of samples with Medicaid insurance and low income have found definitive relationships between disparities in health access, quality and outcomes. Specific to this study on individuals with PAD, socio-economic status has been found to play a significant role in the rate of amputation in individuals with PAD. For example, Eslami et al. found that patients in the lowest median income by zip code bracket were 1.41 times more likely to receive an amputation compared with individuals in the highest median income per zip code bracket. 21 The increased odds for TF amputation found in this study is consistent with these findings. In addition, Lefebvre et al. found lower income to be associated with higher-level amputation. 5
Cerebrovascular disease is a vascular condition that can be related to PAD and, therefore, indirectly to amputation. A study by Miura et al. of 2930 patients with intermittent claudication who underwent an endovascular procedure, found that cause of death was cardiovascular in 42.8% of the cases of mortality, demonstrating the close presence between cardiovascular diseases, such as coronary artery disease, cerebrovascular disease and PAD. 19 However, the findings of such high odds of TF amputation are surprising. This is consistent with our previous findings, and it warrants further exploration. 5 Cerebrovascular disease could be a variable to consider when developing risk assessment strategies for diagnosing or screening for PAD.
When observing the ratio of TT/TF amputations over time for race and gender, a pattern is evident that indicates that a continuing and unchanging disparity exists over time. Not only is the relationship between TT/TF amputations consistent over time when comparing female to male gender and black to white race, the ratio for the reference male and white race groups always remains above 1.0 (indicating a greater number of TT to TF amputations), while the female gender and black race ratio consistently remains below 1.0 (indicating a greater number of TF amputations than TT amputations). This is indicative of two findings. The first finding indicates that female gender and black race are predictive of a greater rate of TF amputations when compared with TT amputations, with the opposite findings for male gender and white race. Second, the trends in this ratio parallel each other. At no point in the analysis do the ratios close the gap. The gap in this trend remains consistent over time.
Even though black individuals have been found to be more likely to receive pre-amputation peripheral arterial testing within 24 months of amputation, when compared to a white race reference group, the results of our study show that a disparity in the level of amputation received exists and has remained relatively stable over time. 22 This disparity exists even in light of an overall decrease in amputations, and efforts in the medical community to increase endovascular intervention and increase pre-amputation screening.7,23,24 This health disparity may be related to the fact that even though black individuals and those with PAD are more likely to be screened, Vemulapalli et al. found that 68.4% of all patients undergoing non-traumatic lower extremity amputation were screened less than 12 months prior to their amputation, including taking a non-invasive ankle–brachial index measurement. In addition, the mean time between pre-amputation arterial testing and amputation was 14 days, indicating that this screening was not performed as a preventive measure, but rather to determine whether or not a suspected need for surgery was clinically indicated. 22
Consistent with the findings of this study, evidence also supports that female gender is associated with increased risks related to PAD. Although women have a lower prevalence of PAD than men, their estimated burden is higher and outcomes are often poorer when compared to men.25,26 These outcomes include higher mortality, increased functional impairment and poorer quality of life.25,27 Asymptomatic lower extremity PAD is common in an aging female population, making diagnosis and treatment more challenging. 28 This again highlights the importance of access to screening for the asymptomatic female patient in order to deter the poorer outcomes, such as the increased risk for TF amputation and related issues associated with that higher level of amputation.
Frieden et al. recommend six key components of effective public health implementation. Considering health disparities to be a public health issue, implementation of programs to address disparities in level or severity of amputation may begin to help with making meaningful improvements over time. Implementation should consider innovation, a technical package based on evidence-based interventions, performance management with feedback mechanisms that allow for performance improvement, partnerships with public and private sector organizations, communication to change public perception and, most importantly, political support in the way of funding, resources and support. 29 In addition, the Community Preventative Services Task Force recommends the use of clinical decision support systems that are intended to address barriers that may be adversely effecting optimal physician diagnosis and treatment planning at the patient, provider and organizational level. These computer-based systems are designed to assist health care providers in providing care supported by clinical guidelines at the point of care by providing evidence-based diagnosis and treatment recommendations.30,31
When interpreting our study it is important to consider the nature of the data source. This is an observational study based on cross-sectional data. Thus, we infer no causal implications in our analysis. Further, there are no variables in this set that shed light on the clinical decision of level of amputation. Even with these limitations the data do provide a unique and longitudinal assessment of the impact of socio-demographics on amputation. Our analysis provides insights into the impact or lack thereof of policy to reduce disparities in this outcome of PAD.
Study limitations
The HCUP-NIS dataset lacks the clinical level variables that would have allowed the researchers to take into account and control for the severity of the PAD. Researchers in this study were unable to control for any patient characteristics, such as the extent of anatomic or hemodynamic disease. The disease severity can only be inferred by the level of the amputation (a higher level may be indicative of a more significant disease presence).
Opportunities for future research
There were some interesting and unexpected findings as a result of this study. First of all, the analysis shows that Hispanic race was somewhat of a protective factor for TF amputation. We cannot draw any conclusions as to why this relationship occurred, but it is an unusual finding and needs to be addressed with more specific research in the future. Second, the data show that a diagnosis of cerebrovascular disease puts an individual at a significantly greater risk of TF amputation (OR 2.12; 95% CI 2.03, 2.23). This is a significant finding that also warrants further investigation.
Conclusion
The disparity in level of amputation between females and males and individuals of black and white race has not been meaningfully affected by increased government and policy attention to the issue of health disparities over the 10-year period of our study. This is concerning as a level of amputation has a significant relationship with an individual’s function and quality of life. These findings should stimulate thought and research around the ideas of clinical decision support and public health initiatives that might allow for more meaningful change over time.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by an internal Provost’s Grant at Widener University and the Springfield College Research Fund.
No commercial party having a direct financial interest in the results of the research supporting this article has or will confer a benefit upon the authors or upon any organization with which the authors are associated.