
Abstract
We sought to quantify whether health-related quality of life (HRQoL) is improved through exercise training in people with peripheral artery disease (PAD) and to clarify which prescriptions were optimal for improving HRQoL when compared to usual care. We conducted a systematic search (PubMed, CINAHL, Cochrane Central Register of Controlled Trials; 1966 – 31 August 2014). We only included randomized controlled trials (RCTs) of exercise training versus usual medical care in persons with PAD that included the Walking Impairment Questionnaire (WIQ) and Short-Form Health Survey component summary scores as outcomes. Of 15 RCTs, 1257 participants were studied: 543 participated in supervised exercise, with only 61 undertaking resistance training and 316 unsupervised exercise. When compared to controls, participants who completed any form of exercise training significantly improved their WIQ speed [mean difference (MD) 9.60 (95% CI 6.98 to 12.23, p<0.00001)]; WIQ distance [MD 7.41 (95% CI 4.49 to 10.33, p<0.00001)] and WIQ stair-climbing [MD 5.07 (95% CI 3.16 to 6.99, p<0.00001)]. Walking also significantly improved the Short-Form Physical Component Summary (SF-PCS) score when compared to controls [MD 1.24 (95% CI 0.48 to 2.01, p=0.001)], but not the Mental Component Summary (SF-MCS) score [MD –0.55 (95% CI –1.27 to 0.18, p=0.14)]. Exercise training improves the SF-PCS dimension, as well as perceived walking distance, speed and stair-climbing as measured by the WIQ, but not the SF-MCS score. Future studies should aim to blind assessors of such subjective measures, and study alternative modes and prescriptions of exercise alternative to walking.
Introduction
The health-related quality of life (HRQoL) burden in persons with peripheral artery disease (PAD) is as great in magnitude as in patients with other forms of cardiovascular disease. 1 In addition, HRQoL has been shown to predict long-term survival in persons with PAD, 2 and outcomes from the Walking Impairment Questionnaire (WIQ) have been shown to predict mortality in PAD. 3 In addition, persons with PAD have limited exercise capacity, reduced functional performance, and poor cardiorespiratory and musculoskeletal fitness, 4 which have also been linked to higher all-cause and cardiovascular mortality. 5 Previous systematic reviews and meta-analyses have shown exercise improves walking ability, fitness and functional performance4,6–8; however, these reviews have not shown whether exercise training programs within randomized controlled trials (RCTs) also improve HRQoL and perceived walking ability. Although there was a review completed in 2010, 9 the search was current until 2008 and data from non-RCTs was considered. Moreover, at that time of publication only five RCT’s were available, so meta-analysis was not justified.
There has also been no meta-analysis on RCTs for exercise and PAD that has quantified the magnitude of change in HRQoL and WIQ outcomes attributable to exercise training. We therefore sought to conduct an updated systematic review, while also undertaking appropriate meta-analyses, with a particular focus on quality of life and perceived walking ability outcomes. The aims were to quantify the magnitude of change in exercise training participants versus sedentary controls for improvements in HRQoL and the WIQ, and to identify whether specific prescriptive elements improve HRQoL and WIQ more so than others.
Methods
Search strategy
Potential studies were identified by conducting a systematic search using PubMed, www.ncbi.nlm.nih.gov/pubmed (1966 to 31 August 2014). CINAHL and the Cochrane Central Register of Controlled Trials were also searched (1966 to 31 August 2014). The search strategy included key terms such as peripheral arterial disease, intermittent claudication, peripheral vascular disease, lifestyle therapy, physical training and exercise training. These were combined with a sensitive search strategy to identify RCTs. Reference lists of papers found were scrutinized for new references. All identified papers were assessed independently by two reviewers (BP and GP); a third reviewer (NS) was consulted to resolve disputes. Searches of published papers were also conducted until 31 August 2014. Study quality was assessed using a modified Physiotherapy Evidence Database (PEDro) score. 10 As supervision has previously been deemed an important component of an exercise program for this population,11,12 supervision was added to the quality criteria score for a maximum score out of 11.
Inclusions
RCTs of exercise training of greater than 4 weeks’ program duration in persons diagnosed with PAD were included. There were no language restrictions. Studies were included if they had a control group that had been placed on usual medical care, with or without exercise advice, and if they measured quality of life outcomes including the WIQ or component scores from the Short-Form (SF) 12, 20 or 36 Health Surveys. HRQoL, as measured via the SF surveys, and perceived walking ability, as measured via WIQ, are both validated questionnaires for measuring aspects of quality of life in PAD.13,14 The Physical and Mental Component Summary scores from the SF-36, SF-20 and SF-12 have been shown to correlate highly 15 and therefore were merged into one analysis. The WIQ is a PAD-specific measure of self-reported walking limitations that has been validated for use within PAD cohorts. 14 The questionnaire consists of four sub-categories: claudication severity, distance, walking speed and stair-climbing. Owing to only two studies measuring the claudication severity score, it was not suitable for inclusion in this meta-analysis.
Exclusions
Animal studies, review papers and non-RCTs were excluded. Studies that did not have any of the desired outcome measures or used participants without diagnosed PAD in either exercise or control groups were excluded. Several authors were contacted to provide missing data or to clarify if data was duplicated in multiple publications. If authors did not respond, or were unable to provide data, the study was excluded. If a partial data set was deemed to have been previously published, and this was confirmed by the corresponding author, the more complete data set was used in these analyses. Studies using interventions other than exercise, or in addition to exercise (e.g. electro-acupuncture, ultrasound, surgery), were excluded.
Data synthesis
Information on outcome measures was archived in a database. The outcome measures were changes in three items of the WIQ (speed, distance and stair-climbing) and SF-36 Physical and Mental Component Summary scores. The mean difference (MD) was calculated for the outcome measures by subtracting the baseline from post-intervention values (e.g. using the formula MD = post-mean – pre-mean). The standardized mean difference (SMD) calculated as percentage change from baseline was used when different methods to establish the same outcomes were used. If studies reported median and standard error, range or inter-quartile range, then the median was substituted for the mean when the sample size exceeded 25 and their measures of variability were converted to standard deviation as per Hozo et al. 16
Statistical analysis
Meta-analyses were completed for continuous data by using the change in the mean and standard deviation of outcome measures. It is an accepted practice to only use post-intervention data for meta-analysis but this method assumes that random allocation of participants always creates intervention groups matched at baseline for age, disease severity, etc. Change in post-intervention mean was calculated by subtracting the baseline from post-intervention values. Change in the standard deviation of post-intervention outcomes was calculated by using RevMan 5.0 (Nordic Cochrane Centre, Copenhagen, Denmark). Data required were (1) 95% confidence interval data for pre–post intervention change for each group or, when this was unavailable, (2) actual p-values for pre–post intervention change for each group or, if only the level of statistical significance was available, (3) we used default p-values (e.g. p<0.05 becomes p=0.049, p<0.01 becomes p=0.0099, and p = not significant becomes p=0.05). A random effects inverse variance was used with the effects measure of mean difference. Heterogeneity was quantified using the Cochrane’s Q test. 17 Egger plots were provided to assess the risk of publication bias (supplementary files). We used a 5% level of significance and 95% confidence intervals; figures were produced using RevMan 5.0.
Results
Studies included in the review
Our initial search identified 16,606 manuscripts; examination of the latest editions of relevant journals yielded a further 63 manuscripts. Out of 16,669 studies, 62 were excluded at first inspection as duplicates; 16,473 were removed after reading titles or abstracts; 46 studies were not studies of exercise therapy in PAD patients. Out of the remaining 88 studies, 73 studies did not meet the inclusion criteria, leaving 15 studies for inclusion in this analysis (Figure 1).
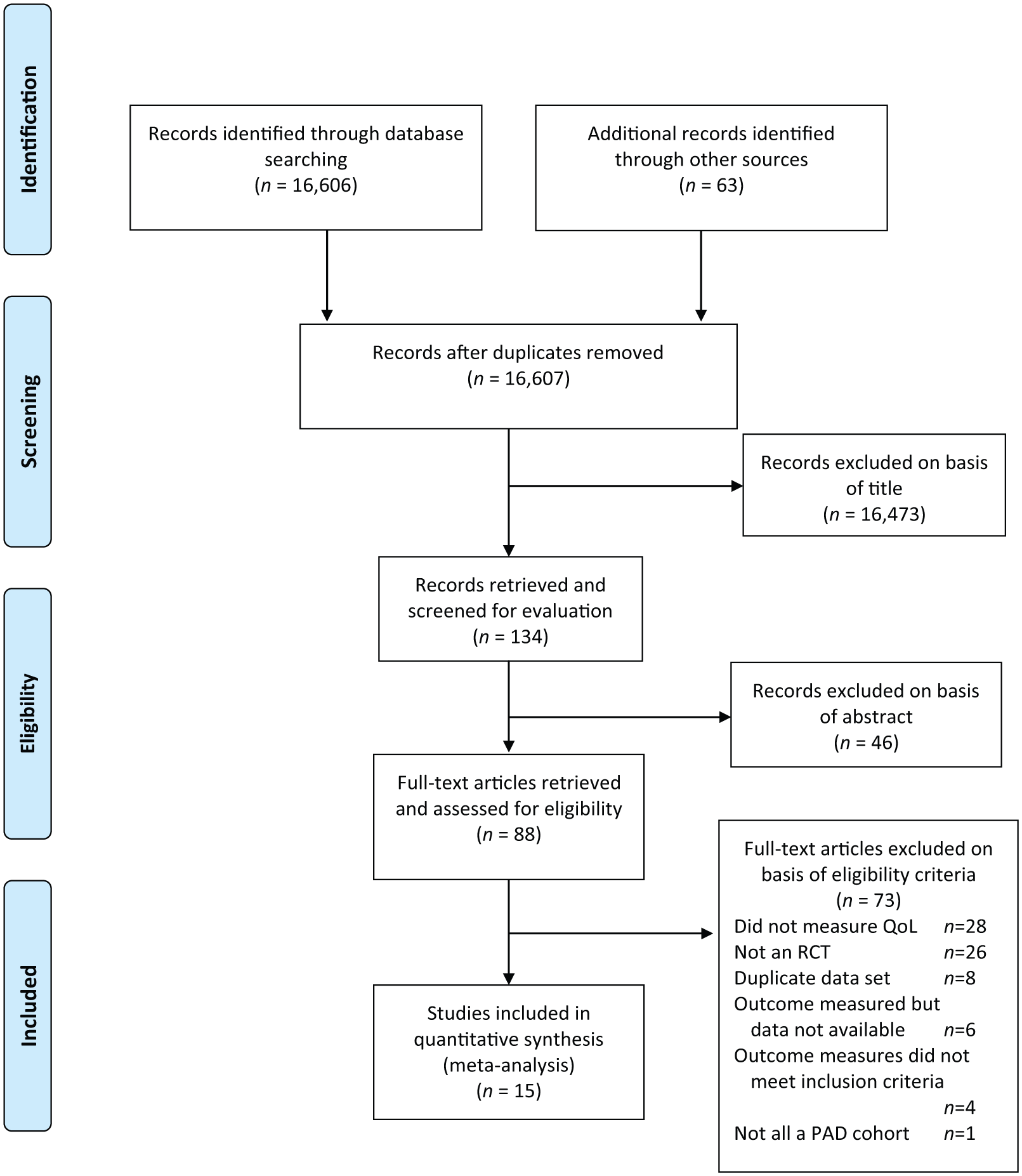
Literature search flow chart.
Fifteen studies18–32 (18 intervention groups) met the inclusion criteria for our analyses; three of these studies20,24,30 had more than one intervention group, which are separated in Forest plots. The total number of patients in our analyses was 1257: 543 took part in supervised exercise, 61 in a resistance training program, 316 completed an unsupervised exercise program, and 337 were assigned to usual medical care. The exercise prescriptive elements for each trial are outlined in Table 1. Training was often interval-based due to claudication pain and ranged from 20 to 60 minutes in duration, averaging 46±12 minutes, including rest time. Walking to moderate–maximum claudication pain was the most common prescription (nine of 15 studies). Training frequency ranged from 1 to 7 days weekly, with the most common frequency being 3 days per week. All studies provided complete supervision for the intervention. In the trials that reported it, average compliance to the supervised exercise programs was high: mean 83.1±9.2%18–20,28,29,31 or median 79.1%.22,24 In addition, for those trials that compared supervised exercise to unsupervised exercise, there were no significant differences between the groups for exercise compliance.20,29 The authors note that unsupervised exercise compliance was rigorously quantified with a step activity monitor in Gardner (2011); 20 however, it was self-reported in the earlier trial. 29
Included studies and intervention characteristics.
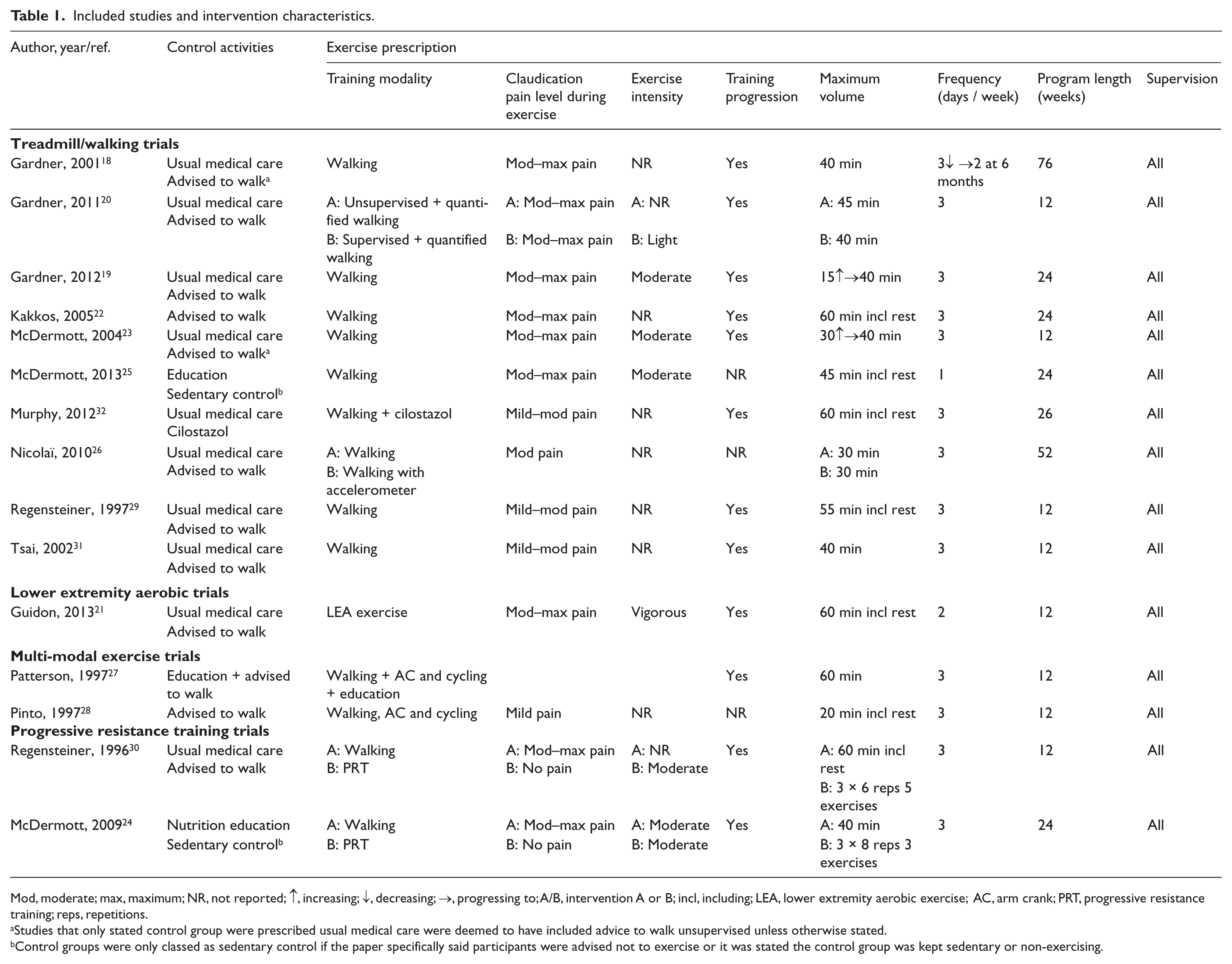
Mod, moderate; max, maximum; NR, not reported; ↑, increasing; ↓, decreasing; →, progressing to; A/B, intervention A or B; incl, including; LEA, lower extremity aerobic exercise; AC, arm crank; PRT, progressive resistance training; reps, repetitions.
Studies that only stated control group were prescribed usual medical care were deemed to have included advice to walk unsupervised unless otherwise stated.
Control groups were only classed as sedentary control if the paper specifically said participants were advised not to exercise or it was stated the control group was kept sedentary or non-exercising.
Walking Impairment Questionnaire (WIQ)
WIQ speed
Eleven studies (14 intervention groups) measured WIQ speed. Overall, a significant improvement was observed in exercise training participants versus controls: MD 9.60 (95% CI 6.98 to12.23, p<0.00001) (Figure 2). Both of the trials24,30 that used progressive resistance training (PRT) as an intervention showed that moderate intensity PRT did not significantly improve perceived WIQ speed. However, walking to some form of claudication pain three times a week for 30–40 minutes was the only other exercise prescription studied.
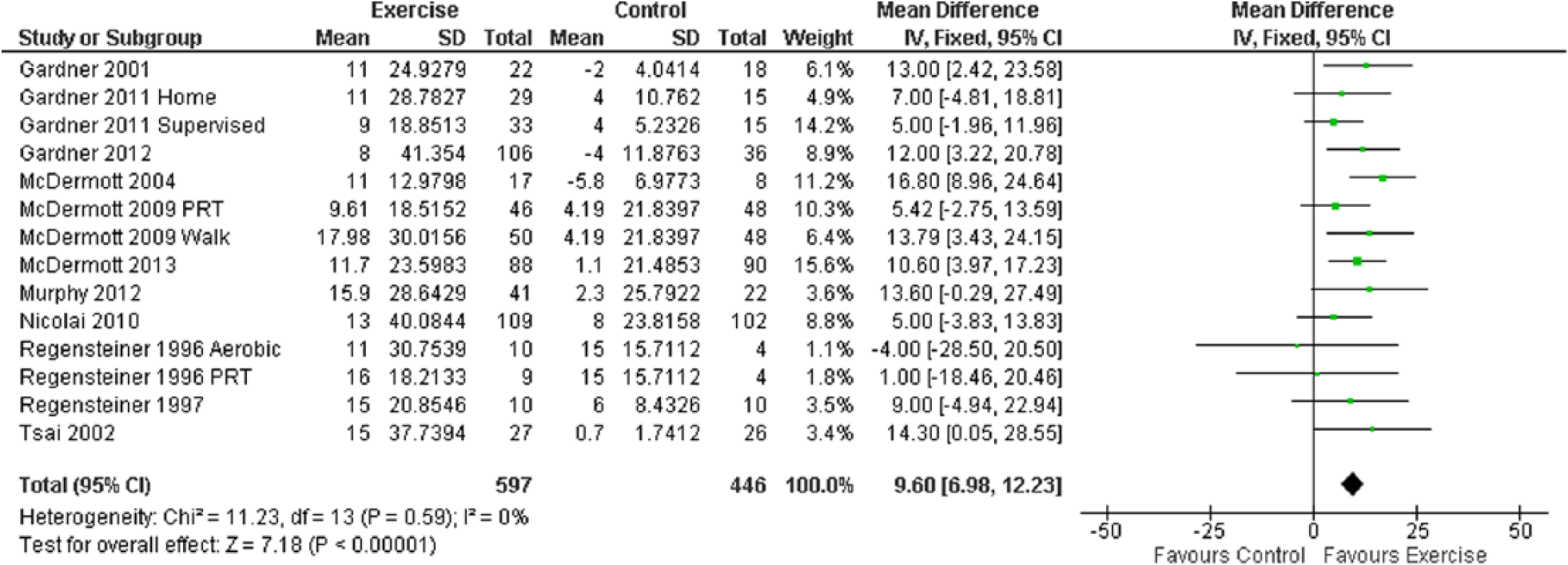
Mean difference in WIQ speed: exercise versus control groups.
WIQ speed sub-analysis
When non-aerobic intervention groups were removed for the purpose of sub-analysis, the MD increased marginally: 10.27 (95% CI 7.47 to 13.07, p<0.00001) (Figure 3).
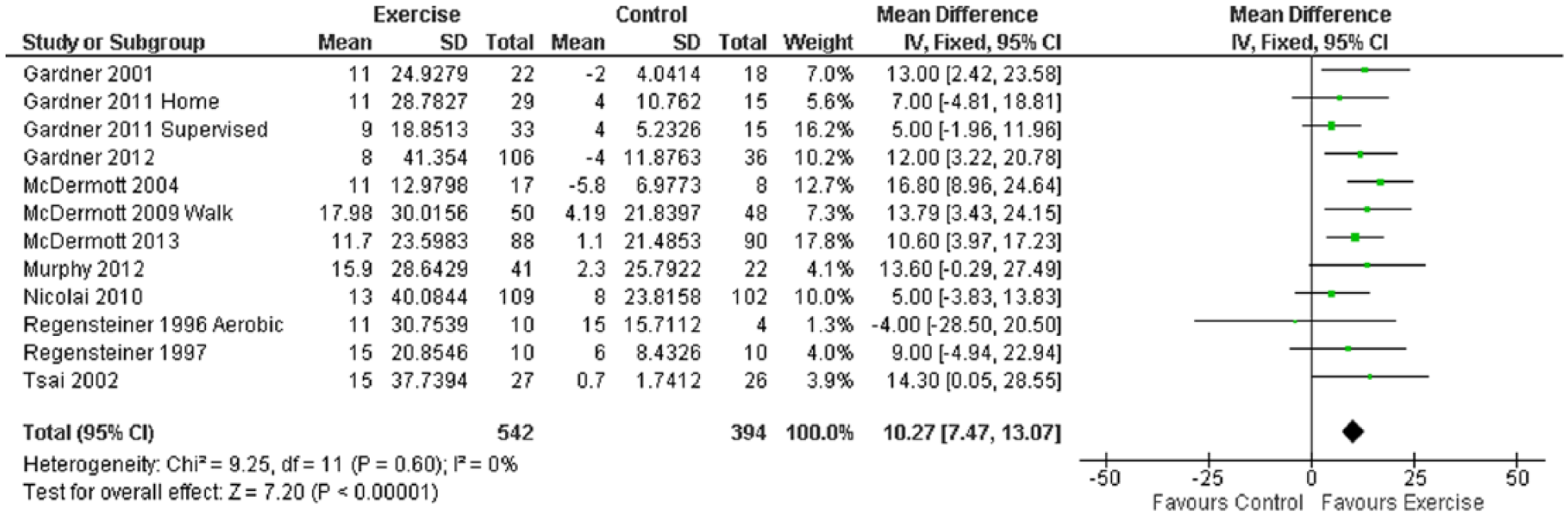
WIQ speed sub-analysis.
WIQ distance
Ten studies (13 intervention groups) measured WIQ distance. Overall, an improvement was observed in exercise training participants versus controls: MD 7.41 (95% CI 4.49 to 10.33, p<0.00001) (Figure 4). The one trial that used PRT as an intervention showed that moderate intensity PRT did not significantly improve perceived WIQ distance. However, again, walking to some level of claudication pain was the only other exercise prescription studied. Sub-analysis was not indicated.
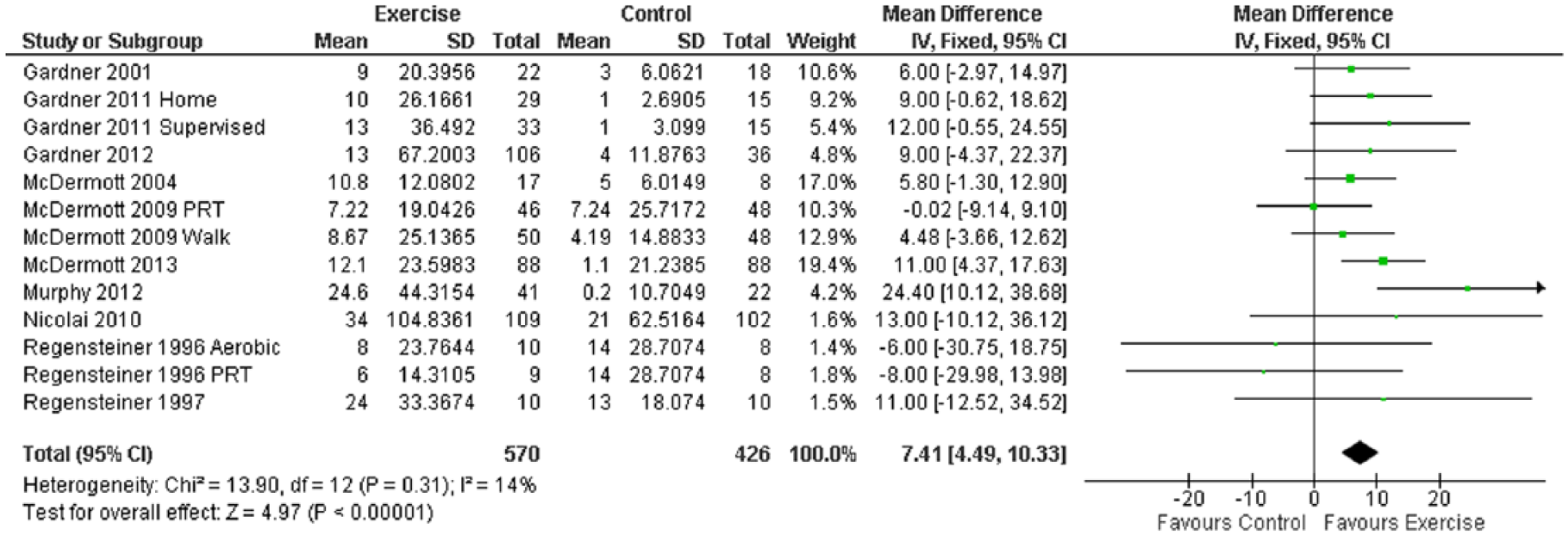
Mean difference in WIQ distance: exercise versus control groups.
WIQ stair-climbing
Ten studies (13 intervention groups) measured WIQ stair-climbing ability. Overall, an improvement was observed in exercise training participants versus controls: MD 5.07 (95% CI 3.16 to 6.99, p<0.00001) (Figure 5). Both of the trials that used PRT as an intervention showed that moderate intensity PRT did not significantly improve perceived WIQ stair-climbing ability. All other trials used a prescription of walking to a level of claudication pain as the prescription and only three of these trials significantly improved the WIQ stair-climbing score. Sub-analysis was not indicated.
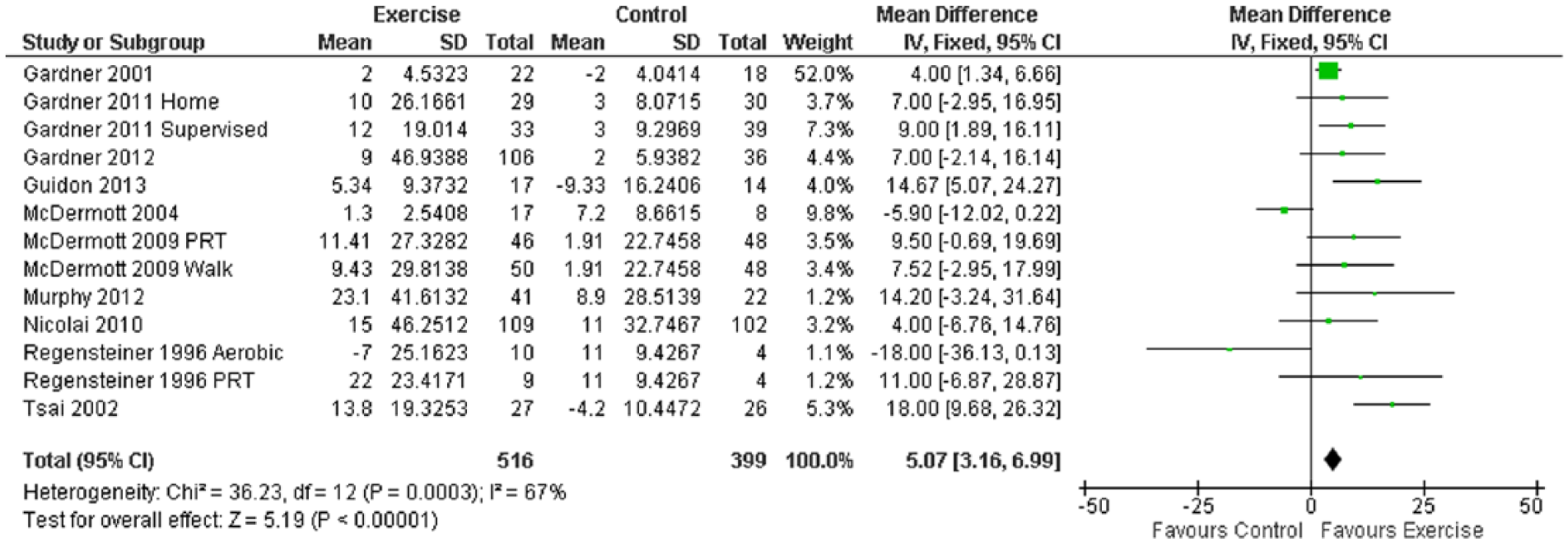
Mean difference in WIQ stair-climbing: exercise versus control groups.
Short-Form Physical Component Summary (SF-PCS) score
Nine studies (11 intervention groups) measured SF-PCS; there were insufficient data reported within the studies to conduct individual SF physical domain analyses. A small improvement was observed in exercise training participants versus controls: MD 1.24 (95% CI 0.48 to 2.01, p=0.001) (Figure 6). The one trial that used PRT as an intervention showed that moderate intensity PRT did not significantly improve perceived SF-PCS. One trial used a variety of modes of aerobic exercise and did not improve SF-PCS. All other trials used walking to various levels of claudication pain, three times a week.
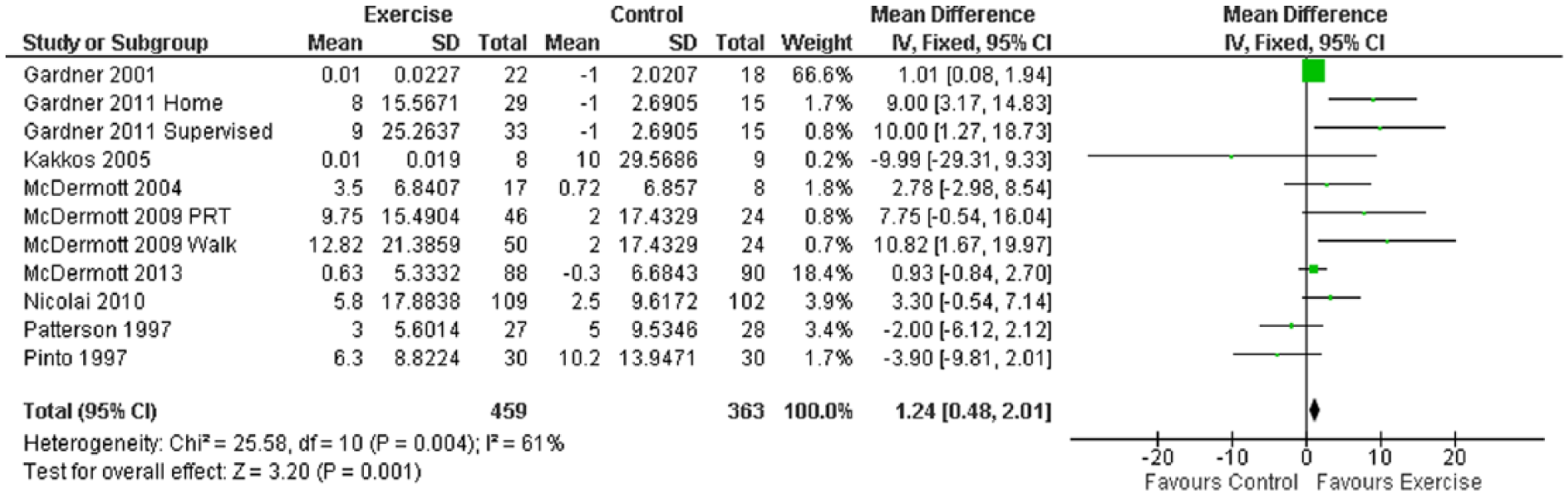
Mean difference in SF-PCS scores: exercise versus control groups.
Short-Form Mental Component Summary (SF-MCS) score
Only six studies (six intervention groups) measured SF-MCS, which was not significantly different between exercise training participants versus controls: MD –0.55 (95% CI –1.27 to 0.18, p=0.14) (Figure 7).
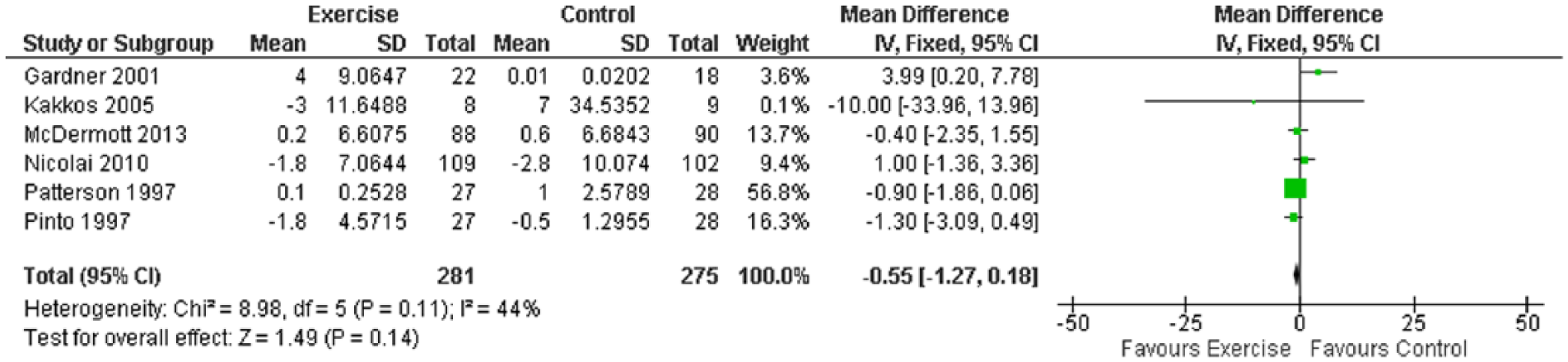
Mean difference in SF-MCS scores: exercise versus control groups.
Study quality assessment
Study quality assessment is presented in Table 2. Overall, the quality of the included trials was modest, with, on average, seven of the 11 quality criteria being present (mean 6.7±1.2, range 5–9/11). Common limitations were concealment of randomization, blinding of subjects, therapists and assessors, and, importantly, measurement of key outcomes in greater than 85% of trial participants. Ten of the 15 studies reported a >15% drop-out rate; however, nine of these studies addressed this concern by implementing an intention-to-treat analysis. Eleven studies (73.3%) in total completed an intention-to-treat analysis. No studies blinded therapists administering exercise interventions or participants. Only four studies (26.7%) blinded assessors who measured at least one key outcome. Thus, the assessor’s belief in intervention efficacy in 11 of the 15 trials (73.3%) may have biased such subjective treatment outcomes. 33 This lack of blinding of the outcome assessors is a serious limitation of the RCTs included in this review, particularly because the outcomes assessed are subjective and present greater opportunities for bias. 34
PEDro quality assessment.
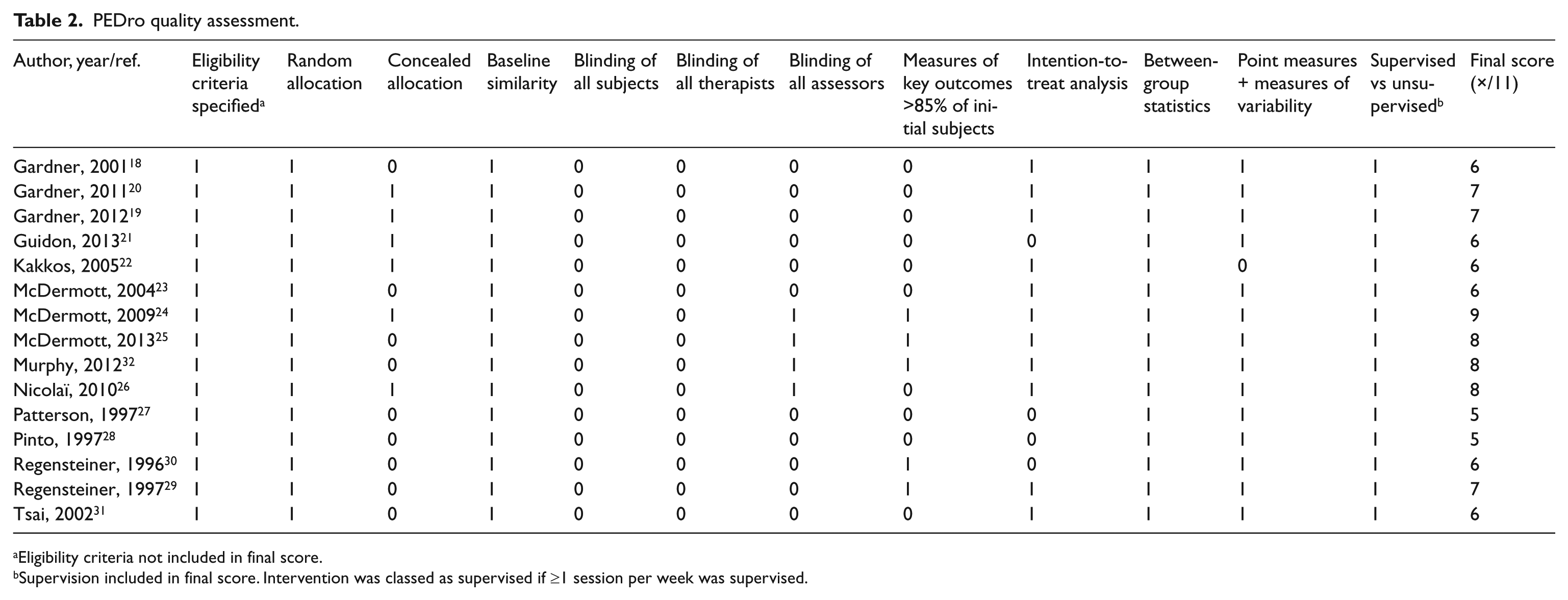
Eligibility criteria not included in final score.
Supervision included in final score. Intervention was classed as supervised if ≥1 session per week was supervised.
Heterogeneity
The Cochrane I2 scores from analyses in Figures 2 and 3 showed zero heterogeneity. Analyses in Figures 4–7 exhibited low to high evidence of between-study heterogeneity, ranging from 14% to 67%.
Egger plots
Egger plots indicated negligible risk of publication bias for all analyses.
Discussion
Despite several recent systematic reviews4,6,35 and Cochrane meta-analyses,7,12 this is the first meta-analysis limited to RCTs to analyse perceived walking impairment, general health (both Physical and Mental Component Summary) and quality of life outcomes for exercise interventions in PAD. In analysing the findings, it is important to take into account the quality of the trials included in this review and the limited study of exercise modes other than walking. Despite this, our findings suggest that walking training to claudication pain leads to small but significant improvements in perceived walking distance, speed and stair-climbing ability in PAD as measured by the WIQ. In addition, walking to claudication pain also improves the SF-36 Physical, but not Mental Component Summary score. These findings are encouraging, as HRQoL in PAD has been shown to predict long-term survival. 3
Unfortunately, to date, studies that have measured the WIQ and/or the SF-36 have mostly been studies using walking to some level of claudication pain as a prescription. Only two studies28,27 looked at a combination of aerobic modes and only two studies24,30 have examined the effect of resistance training. In the studies that utilized exercise modalities other than walking, the efficacy of exercise training produced mixed results. More studies looking at various modes and elements of exercise prescription are needed to assess the maximum likely treatment effect of exercise training on HRQoL in PAD and to identify which specific prescriptive elements improve HRQoL the most.
Strengths and limitations
Analyses in Figures 2 and 3 showed zero heterogeneity, suggesting the analyses of WIQ speed were appropriate. Analyses in Figures 4–8 exhibited moderate to high evidence of between-study heterogeneity, suggesting results of data pooling of WIQ distance, stair-climbing and the SF Physical and Mental Components must be interpreted with caution. Nevertheless, Egger plots showed minimal evidence of publication bias. This lack of bias may be due to similarity of training modes used in most of the trials examined. It is therefore unlikely that unpublished negative or neutral datasets exist for the outcome measures and significance levels suggest unpublished data would not change presented findings. A serious limitation of the literature analysed in this paper is that most (73%) of the investigators assessing outcome measures were aware of intervention group assignment. Whilst it is difficult to blind participants and trainers in an exercise training study, unless ‘sham’ exercise is used, the importance of blinding outcome assessors cannot be overlooked. The importance of blinding assessors for subjective measures presented in this paper cannot be under-estimated. If the outcomes assessors believe in one treatment more so than another, they could influence more generous responses to that intervention. 36 The outcomes presented in this paper are entirely subjective outcomes, answers which are based on the patient’s perception, which present large opportunities for bias. 34 Future studies must at least blind the outcome assessors to the participants’ intervention to minimise outcome assessment bias, especially with subjective outcomes of interest such as the WIQ and Short-Form Health Surveys. The results from this study should be interpreted keeping the lack of assessor blinding in mind. Only one study with >15% withdrawal failed to conduct an intention-to-treat analysis; this would have had minimal impact on the overall findings. The PEDro scale has no assessment for quantifying compliance to the exercise programs, nor has an optimal compliance to exercise regimes for PAD been established. Therefore, we are unable to objectively comment on how compliance to the exercise program may have affected the overall findings. However, with such a high rate of compliance to the exercise programs, the authors doubt that compliance to programs affected the results of this analysis. Further limitation in this field of study is the lack of trials employing alternative modes of aerobic exercise or resistance training whilst measuring these HRQoL outcomes. More studies employing alternative aerobic and resistance training prescriptions are required in order to make further comment on the maximum likely treatment effect of specific exercise prescriptions on these outcomes. The authors note that the addition of a further nine RCTs since Guidon’s 2010 review 9 has made meta-analysis possible.
Conclusions
Walking training to various levels of claudication pain improves perceived walking speed, distance and stair-climbing performance as measured by the WIQ, and self-reported physical function (SF-36) in people with PAD. Walking to claudication pain was the most common prescription studied and consequently yielded the most improvements in these outcomes. Further studies employing alternative modes and prescriptions of exercise are needed to measure the effect of multiple modes of exercise on HRQoL and walking impairment outcomes.
Footnotes
Acknowledgements
The authors would like to thank included study authors who provided additional information.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.