
Abstract
Background:
The presence of plaque in the external carotid artery (ECA) detected on carotid duplex ultrasound (CDU) is of unknown clinical significance and may not be reported in routine clinical practice. We hypothesize that ECA plaque in the absence of plaque in the other cervical vessels is a risk factor for increased all-cause mortality.
Objectives:
To determine the significance of ECA plaque on all-cause mortality in the absence of internal carotid artery (ICA) or common carotid artery (CCA) plaque.
Methods:
We queried the Non-Invasive Vascular Laboratory database for all CDUs performed between 1 January 2005 and 31 December 2005. All images were reviewed for the presence of plaque. Studies were included if plaque was absent in both the CCA and the ICA. Chart review was performed to obtain demographic and clinical information. All-cause mortality was determined using the Social Security Death Index.
Results:
A total of 500 patient studies met the inclusion criteria; 64 patients (12.8%) had plaque in one or both ECAs. There was no significant difference in age (mean 58.1 ± 14.8 years), race (82.5% white), or sex (64.4% male) between those with and without ECA plaque. There was a significant difference in all-cause mortality between patients with and without isolated ECA plaque after adjustment for age, sex, low-density lipoprotein cholesterol, smoking, hypertension, body mass index, and surgery within 30 days of CDU (adjusted hazard ratio 2.60, 95% CI 1.46–4.66, p<0.001).
Conclusions:
The presence of plaque isolated to the ECA is an independent predictor of all-cause mortality and may impart important prognostic information for patients referred for CDU.
Introduction
Carotid duplex ultrasonography (CDU) is commonly used to evaluate patients suspected of significant carotid artery stenosis or as a screening modality in patients at risk for atherosclerotic vascular disease. 1 While it is well accepted that internal carotid artery (ICA) stenosis is a risk factor for increased cardiovascular morbidity and mortality,2–4 the presence of plaque alone without hemodynamically significant narrowing is also a marker for increased events and adds incremental value for predicting cardiovascular events when added to carotid intima–media thickness (CIMT) and traditional risk factors.5,6 The association between the presence of plaque in the peripheral vasculature (internal carotid,5–7 common carotid,5–8 aorta9,10 and femoral artery8,11,12) and increased morbidity and mortality when compared to patients with normal or minimal arteriosclerosis has been reported, but the prognostic importance of the presence of plaque isolated to the external carotid artery (ECA) has not been extensively studied.
Methods
We queried our institutional Non-Invasive Vascular Laboratory database for all CDUs performed between 1 January 2005 and 31 December 2005. For patients with multiple CDUs performed during that timeframe, only the first study was included in the analysis. Ultrasound examinations reporting no significant stenosis or plaque in both the common carotid artery (CCA) and ICA (0–19% in our institution) bilaterally were eligible for re-review of all study images for the presence of plaque. Any studies with plaque identified on re-review in either the CCA or ICA were excluded such that only studies with isolated ECA plaque were included in the analysis. The laboratory is accredited by the Intersocietal Accreditation Commission – Vascular Testing Division.
Demographic, clinical, laboratory and medication information within 1 year before or after the date of CDU were obtained through review of the electronic medical record. Demographic information included age, race, sex and body mass index (BMI). Charts were reviewed for history of smoking, diabetes, and hypertension, and laboratory values were obtained for total cholesterol, low-density lipoprotein (LDL), high-density lipoprotein (HDL), total triglycerides, serum creatinine and hemoglobin A1C (HbA1c). The use of aspirin, statins, antihypertensive medications and other cholesterol-lowering medications were also included to assess for any statistical significance between those with isolated ECA plaque versus those without. Query of the Social Security Death Index was used to assess for all-cause mortality. This study was approved by the Institutional Review Board prior to investigation.
Ultrasound
In compliance with IAC (Intersocietal Accreditation Commission – formerly the Intersocietal Commission for the Accreditation of Vascular Laboratories (ICAVL)) standards, 13 the CDU protocol in our laboratory includes spectral Doppler waveforms taken from the proximal, mid, and distal portions of bilateral common and internal carotid arteries. Limited Doppler assessment of the ECA is also performed of at least one site in the origin or proximal segment of the vessel, and transverse and longitudinal B-mode imaging is routinely performed to assess for the presence of plaque at the distal CCA and at the level of the bifurcation of the ICA and ECA. Digitally archived images of studies meeting all criteria by initial database query (no reported stenosis or plaque in the ICA and CCA bilaterally) were re-reviewed de novo to assess for the presence of plaque within the CCA, ICA, and ECA. Reviewers were blinded to the original ultrasound reports. Plaque was defined as the presence of focal wall thickening at least 50% greater than adjacent vessel walls or a protruding focal CIMT >1.5 mm 14 (Figure 1). The origin of the ECA was considered to start at the flow divider, and plaque which extended from the carotid bulb into the ECA were considered CCA plaque and excluded from final analysis.
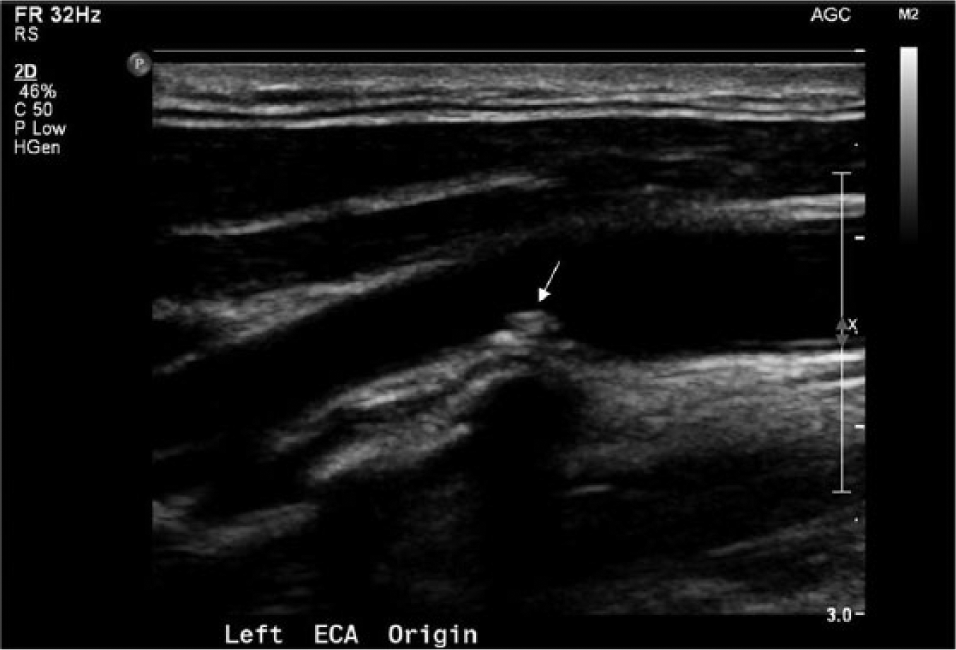
Plaque in the external carotid artery on B-mode ultrasonography. A B-mode ultrasound image of the origin of the external carotid artery showing focal thickening of the far wall (white arrow) at least 50% greater than the adjacent vessel walls with protrusion into the lumen consistent with atherosclerotic plaque.
Statistical analysis
Statistical analysis was performed using STATA. 15 Two-tailed t-tests and chi-squared tests were used in bivariate analysis of baseline variables. Multivariable cox proportional hazards regression modeling was used to estimate survival for those with and without ECA plaque using traditional cardiovascular risk factors as covariates: age, sex, LDL cholesterol, smoking, and hypertension. BMI and having surgery within 30 days of CDU were also included in the multivariable analysis because of a statistically significant difference in BMI between those with ECA plaque and those without plaque in bivariate analysis and the large proportion of CDUs performed for pre-operative evaluation.
Results
The database query resulted in a total of 687 patients with carotid ultrasound studies that met all the inclusion criteria. Of these, 97 were excluded due to the presence of plaque in the CCA or ICA on imaging re-review, 56 were excluded due to inadequate B-mode imaging of the ECA, 33 due to inability to re-review the images, and one due to carotid stent placement. Of the 500 studies meeting all inclusion criteria, 64 had the presence of plaque in one or both ECAs (12.8%). There were 42 of 64 (65.6%) patients with ECA plaque visualized on blinded image re-review that were not reported to have plaque on the original clinical CDU report.
The mean age of all patients studied was 58.1 ± 14.8 years, with 64.4% being male. The indications for CDU referral were as follows: asymptomatic bruit (n=199, 39.8%), TIA (transient ischemic attack)/CVA (cerebrovascular accident) (n=25, 5.0%), surveillance of known cerebrovascular disease (n=21, 4.2%), pre-operative examination (n=215, 43.0%), and other not otherwise listed (n=40, 8.0%). Of the 211 patients who underwent surgery at our institution within 30 days of the CDU, 128 (60.7%) underwent cardiac surgery, 53 (25.1%) underwent vascular surgery, and 30 (14.2%) underwent non-cardiovascular surgery.
There were no statistically significant differences in demographic or clinical variables between those with and without ECA plaque (Table 1). BMI was lower in those with ECA plaque versus those without (26.0 vs 28.6, p=0.001); however, there was no significant relationship between BMI and all-cause mortality in multivariate analysis. During a median follow-up of 4.9 years from the date of the ultrasound study, there were 61 deaths with a statistically significant difference in all-cause mortality between patients with and without isolated ECA plaque (Figure 2), with an adjusted hazard ratio (HR) of 2.60 for all-cause mortality in those with ECA plaque compared to those without ECA plaque (95% CI 1.46 to 4.66). Of the 61 deaths, a cause of death could be determined through the electronic medical record for only 21 (13 died due to a cardiovascular cause, two died postoperatively, and six died from other causes).
Patient characteristics.
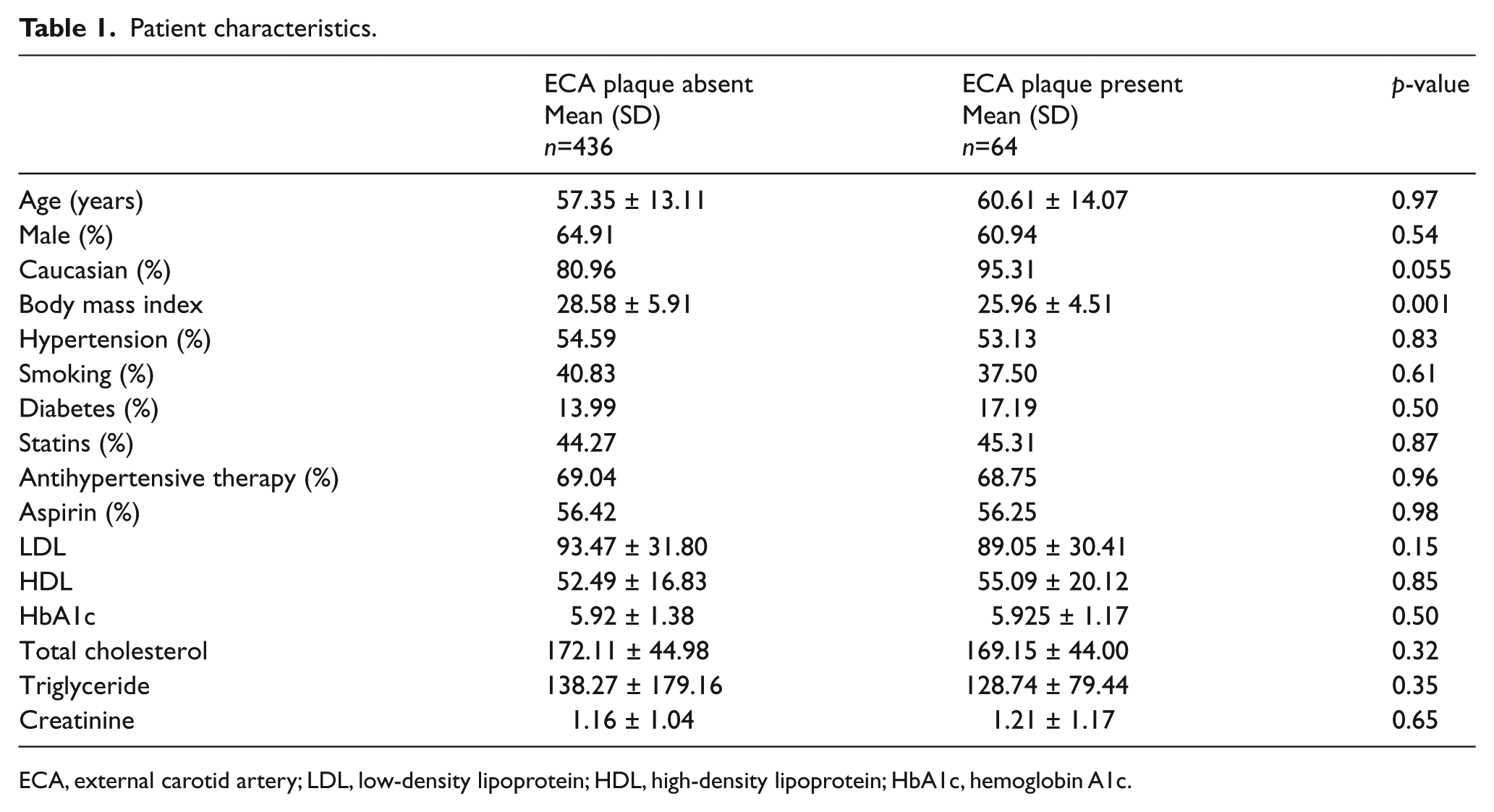
ECA, external carotid artery; LDL, low-density lipoprotein; HDL, high-density lipoprotein; HbA1c, hemoglobin A1c.
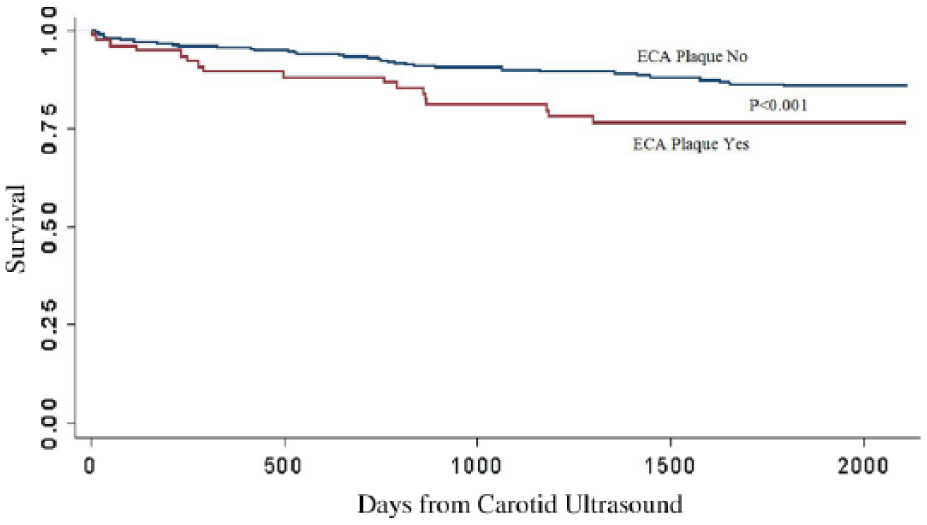
Adjusted survival functions by the presence of ECA plaque. During a median follow-up of 4.9 years, there was a statistically significant difference in mortality between patients with and without isolated ECA plaque with an adjusted hazard ratio of 2.60 for all-cause mortality in those with ECA plaque compared to those without ECA plaque (95% CI 1.46 to 4.66). Survival function was adjusted for age, sex, LDL cholesterol, smoking, hypertension, BMI, and surgery within 30 days of CDU.
Discussion
While simple for use in clinical practice, risk prediction scores such as the Framingham risk score 16 do have limitations in their ability to accurately classify risk. 17 The addition of biomarkers18,19 and imaging techniques such as coronary artery calcium scoring (CACS)20–22 and CIMT 5 may improve risk stratification by direct imaging of the vasculature for early changes of atherosclerosis. Similarly, plaque detection using duplex ultrasonography of the peripheral vasculature can also improve coronary heart disease risk prediction,5,8,9,11 and in this study the presence of isolated ECA plaque was significantly associated with all-cause mortality, independent of age, race, sex, LDL cholesterol, smoking history, diabetes, or hypertension. These findings support that the presence of atherosclerotic plaque, even in arterial beds considered to be of minor clinical significance, such as the ECA, may be an indicator of increased risk for all-cause mortality.
The American College of Cardiology Foundation and the American Heart Association recognize the potential value of imaging for cardiovascular risk assessment. 23 In the 2010 Guideline for Assessment of Cardiovascular Risk in Asymptomatic Adults, 23 carotid IMT and CACS are each given a Class IIa recommendation for risk assessment in asymptomatic adults at intermediate risk. Other groups have also advocated for the use of imaging for the detection of subclinical atherosclerosis: the Screening for Heart Attack Prevention and Education (SHAPE) Task Force 24 guideline recommends that all apparently healthy men aged 45–75 years and women aged 55–75 years without a history of coronary heart disease who have at least one traditional cardiovascular risk factor undergo testing for subclinical atherosclerosis with either CACS or CIMT to more precisely stratify their risk for myocardial infarction. Aggressive secondary prevention is recommended for those with a positive test for subclinical atherosclerosis, which is defined as a CACS ≥1 or CIMT ≥50th percentile or the presence of carotid plaque. 24 While CACS is a non-invasive test with accepted predictive ability and reproducibility, the advantage of CIMT over CACS is the ability to predict risk without radiation exposure. CIMT, however, is a highly technical examination requiring trained and experienced operators and readers. Plaque screening using CDU does not require highly specialized training, and several observational studies have demonstrated that the presence of carotid plaque is similar to, or perhaps even more predictive than, increased CIMT as a marker of risk for cardiovascular events.25–32
The importance of plaque screening during a CIMT examination is well recognized. 14 Additionally, the incremental value of plaque screening, when added to IMT, has been demonstrated using the ARIC cohort 5 and, more recently, the MESA cohort. 6 It is important to note, however, that while plaque screening during CIMT is well accepted to be an integral part of risk stratification, the assessment of plaque usually involves close inspection of the CCA, the carotid bulb, and the ICAs.5,6,14 Few studies have included assessment of the ECA during plaque screening, 32 and, to our knowledge, no prior studies have described the importance of plaque isolated to the ECA as an independent risk factor for increased all-cause mortality.
In the clinical setting, CDU is most commonly used for the detection of CCA or ICA stenosis, and the presence of plaque within the ECA (particularly in the setting of normal CCA and ICAs) may be regarded as an incidental finding that does not merit further investigation or even clinical reporting. Even in our own laboratory, despite the use of report templates with drop-down box options for plaque reporting, the presence of ECA plaque was reported less than half of the time. Most of the medical literature regarding the significance of ECA atherosclerosis is in the context of its implications for treatment of severe ICA disease,33,34 but there has been a post-mortem study demonstrating that atherosclerosis in the ECA and femoral arteries have a stronger correlation with atherosclerosis in the coronary arteries compared to the ICA and CCA. 35 While we did not study the relative strength of the association between ECA plaque and mortality compared to plaque in the ICA or CCA, our study emphasizes the importance of vascular plaque presence as an important predictor of increased risk for all-cause mortality (even in ‘minor’ vascular beds) and suggests that patients with plaque in any of the extracranial carotid arteries may warrant a comprehensive review of their overall cardiovascular risk.
A potential limitation of this study includes the referral bias inherent to a vascular laboratory at a tertiary medical center. The indication for carotid ultrasound in our study was pre-operative evaluation in 43.0% of patients. The high rate of events over 5 years (61 deaths in a population of 500 patients) may be hypothesized to be due in part to the high number of screening CDU examinations performed prior to open heart surgery or vascular surgery at our institution; however, multivariate survival analysis including having surgery within 30 days of the CDU did not change the statistically significant relationship between ECA plaque and overall mortality. The more likely explanation for the high number of events is that ECA plaque is a marker for atherosclerotic disease elsewhere, including the coronary and peripheral arteries. To this extent, another potential limitation of our study is the unknown proportion of patients with coronary and/or peripheral artery disease in our cohort, entities known to be associated with elevated cardiovascular morbidity and mortality.
Because we are a tertiary referral center, follow-up information is not available for all patients through the electronic medical record. As such, a cause of death was obtainable for only 21 of the 61 total deaths (34.4%). Some would argue that the use of all-cause mortality is a potential limitation for this type of study; however, in contrast to the use of cardiovascular mortality, all-cause mortality is an unbiased and objective end point of great primary interest to both patients and providers. 36 Nonetheless, consideration of the use of cardiovascular mortality, in addition to all-cause mortality, would be of value in future studies.
Another potential limitation of our study may be misclassification of the presence or absence of ECA plaque as the B-mode grayscale interrogation was limited to the bifurcation of the CCA and the origin of the ECA. As atherosclerotic plaque tends to form at the carotid bifurcation and at the origin of the ICA/ECA, however, misclassification bias is less likely to be a significant issue. Given these limitations, further study is necessary to determine the relative incremental value of adding plaque evaluation of the ECA to CIMT and CCA/ICA plaque screening in large, population-based studies and to assess the reproducibility of plaque assessment in the ECA during CDU.
In summary, the presence of atherosclerotic plaque in the external carotid artery is an independent predictor of all-cause mortality and may impart important prognostic information for patients referred for CDU. Conscientious reporting of the presence of ECA plaque, even in the absence of CCA or ICA plaque, should be considered. Further study is required to determine the relative importance of ECA plaque for prognostication when compared to traditional risk scores, biomarkers, and imaging modalities such as CACS, CIMT, and traditional plaque screening of the CCAs and ICAs.
Footnotes
Acknowledgements
We would like to acknowledge Ms Mariam Khan, Mr Neil Poria, Mr David Rausch and Ms Susan Whitelaw for their assistance with database query and data management.
Declaration of conflicting interest
Dr Kim is a consultant for Philips Ultrasound and has received grant support from GE.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.