
Abstract
The aim of the study was to determine statin drug association with patency, limb salvage rates and survival after revascularization in patients with chronic limb ischemia. We retrospectively reviewed all patients who underwent revascularization for intermittent claudication or critical limb ischemia between 05/2001 and 12/2009. Patients were grouped based on statin therapy at the time of revascularization. Early postoperative outcomes as well as patency, limb salvage, and survival rates were compared between groups. Of 717 patients, 397 (55.4%) were on statins. The incidence of major adverse cardiac events (MACE) was significantly lower in the statin group. Patency and limb salvage rates were similar; however, survival was significantly better in the statin group. Non-statin use, coronary artery disease, chronic pulmonary obstructive disease, renal insufficiency, critical limb ischemia, and age >70 years were found to be independently associated with decreased survival. Statin use was associated with improved survival, but not with long-term patency and limb salvage.
Introduction
The use of statins (3-hydroxy-3-methylglutaryl-coenzyme A reductase inhibitors) has been associated with atheroprotective and anti-inflammatory effects, independent of their lipid-lowering effects.1–3 These effects have been attributed to improvements in endothelial function, a reduction in smooth muscle cell proliferation and migration, and a reduction in the number of smooth muscle cells and collagen content in plaques.4,5 Statins have been reported to reduce coronary events, 6 stroke rates 7 and to increase claudication distance in patients with peripheral artery disease (PAD). 8 In the Heart Protection Study, the largest randomized study on the effects of statins on major morbidity and mortality, the authors reported all-cause mortality was reduced in patients who received statins, primarily due to the reduction in death from vascular causes. 9 In a subgroup analysis of 6748 patients with documented PAD, the authors also reported a 22% reduction in the rate of a first major vascular event in the statin treated patients. 10
The statin drugs have also been associated with improved patency rates11,12 and limb salvage rates 12 in patients who undergo infrainguinal bypass procedures. However, a reanalysis of a randomized trial in which patients with critical limb ischemia (CLI) underwent infrainguinal bypass procedures, showed no differences in patency or limb salvage rates, but survival was noted to be significantly better in patients taking statins. 13 A more recent study by Aiello et al. 14 showed statin use to be associated with improved patency, limb salvage and survival rates in patients with CLI who underwent endovascular revascularization. Another study by Westin et al. 15 showed that statin use was associated with lower mortality, major adverse cardiovascular and cerebrovascular events and increased amputation-free survival in patients with CLI who underwent endovascular interventions. There have also been reports on the effects of statins reducing postoperative morbidity and mortality following various non-cardiac vascular procedures.16–18
The goal of this study was to determine if the use of statins was associated with a decrease in postoperative vascular events, graft patency, limb salvage and survival in patients undergoing endovascular and open revascularization for disabling claudication and CLI. Our primary outcome of interest was all-cause mortality and our secondary endpoints were primary patency and limb salvage.
Methods
The study protocol was reviewed and approved by the Institutional Review Board at the VA Western New York Healthcare System.
Patient population
All patients who underwent open or endovascular revascularization in the VA Western New York Healthcare System for symptomatic chronic limb ischemia (Rutherford categories 3–6) between May 2001 and December 2009 were retrospectively analyzed from our prospectively maintained database. Patients who had endovascular revascularization received local anesthesia with moderate sedation and those who had open surgery received either general or regional anesthesia at the discretion of the treating anesthesiologist. Patients were categorized as ‘statin group’ or ‘no statin group’ depending on whether they were receiving statins at the time of the revascularization procedure. Patients were prescribed statins by the primary providers but the duration of treatment prior to the procedure was unknown.
Patients presenting with acute limb ischemia and those who had undergone primary amputation for non-salvageable limbs were excluded. In the patients who underwent bilateral revascularization, only the first limb procedure was included. Demographics, comorbidities, clinical presentation, preoperative medications (i.e. statins, angiotensin-converting enzyme inhibitors (ACEIs), antiplatelet agents, beta-blockers), laboratory values, functional status, non-invasive arterial studies, details of the procedures performed, postoperative course, follow-up arterial studies, and status of limbs on last follow-up were recorded.
Coronary artery disease (CAD) was defined as documented angina pectoris, myocardial infarction, congestive heart failure or history of coronary artery revascularization. Renal insufficiency was defined as having an estimated glomerular filtration rate of <60 mL/min, or a patient on dialysis. Hyperlipidemia was defined as a fasting cholesterol level >200 mg/dL, a low-density lipoprotein (LDL) level >130 mg/dL, or triglycerides >200 mg/dL.
The decision between an endovascular or open procedure was made by the vascular surgeon. Patients who underwent endovascular interventions received clopidogrel bisulfate in the recovery room (300 mg) and 75 mg daily for at least 30 days. Lifelong enteric-coated acetyl salicylic acid (ECASA, 81 mg) was also given. Patients who underwent bypass with vein graft or above-knee bypass with prosthetic grafts received ECASA 81 mg daily and those who underwent below-knee bypass with prosthetic grafts received Coumadin. All patients were followed postoperatively, and at 3 and 6 months and then every 6 months thereafter for ankle–brachial index (ABI) measurements, graft or stent velocities, and Duplex imaging for patency. A total of 56 patients (7.3%) were lost to follow-up within 36 months: 12 patients (1.6%) did not have a follow-up exam after 3 months, 18 (2.4%) after 12 months, 17 (2.2%) after 24 months, and nine (1.1%) after 36 months – although survival data were available for all these patients. In these patients, the last examination was used for determining patency. The loss of patency was defined as occlusion, restenosis >50%, an elevated ratio of velocity to the proximal segment being >300% by duplex examination, loss of a previously palpable pulse, or a decrease in ABI of >0.2. In patients who had multiple levels of revascularization, restenosis in each segment was considered as loss of patency, even with a normal ABI. A major adverse limb event (MALE) was defined as above-ankle amputation of the index limb or major reintervention (new bypass graft, jump/interposition graft revision, or thrombectomy/thrombolysis). A major adverse cardiovascular event (MACE) was defined as myocardial infarction, stroke or death (any cause).
Statistical analyses and data management
Data analysis was performed using SPSS 17.0 software (SPSS Inc., Chicago, IL, USA) and NCSS (Kaysville, UT, USA). Kaplan-Meier analysis and log rank test were used to compare groups for primary patency, assisted-primary patency, secondary patency, limb salvage and overall survival. Patency and limb salvage rates were calculated based on the first limb when bilateral surgery were performed, and survival was calculated based on patients. Only patients who presented with CLI were included for limb salvage analysis. Demographic comparisons were made using the chi-squared test or two-tailed Fisher’s exact test for categorical variables, and by t-test for continuous variables. Univariate analysis was performed using the log-rank test for identifying factors predicting patency, limb loss, and survival. Multivariate analyses were done by the Cox-Mantel hazard log-rank test for time-dependent events (primary patency, limb salvage, and survival). All factors that showed a trend of significance as identified by p-values <0.1 in univariate analyses were included in multivariate analyses. Propensity scores were calculated using basic demographic predictors, as well as CAD, diabetes, hypertension, chronic obstructive pulmonary disease (COPD) and chronic kidney disease, preoperative use of beta-blockers, ACEI, and ECASA, and the presence of CLI, which were elected due to their known association with decreased survival, and were noted to be significantly different in the two groups (Table 1). After identifying the propensity score, data were matched (1:1) and Cox regression was performed to examine the role of statin on survival. Non-parametric survival analysis (Kaplan-Meier) was performed and treatment groups were compared. Odds ratios (ORs) were reported for 2 × 2 tests and hazard ratios (HRs) were reported with 95% confidence intervals (CIs) for time-to-event endpoints analyses. Null hypotheses were rejected if p-values <0.05.
Baseline characteristics and demographics before and after propensity score matching.
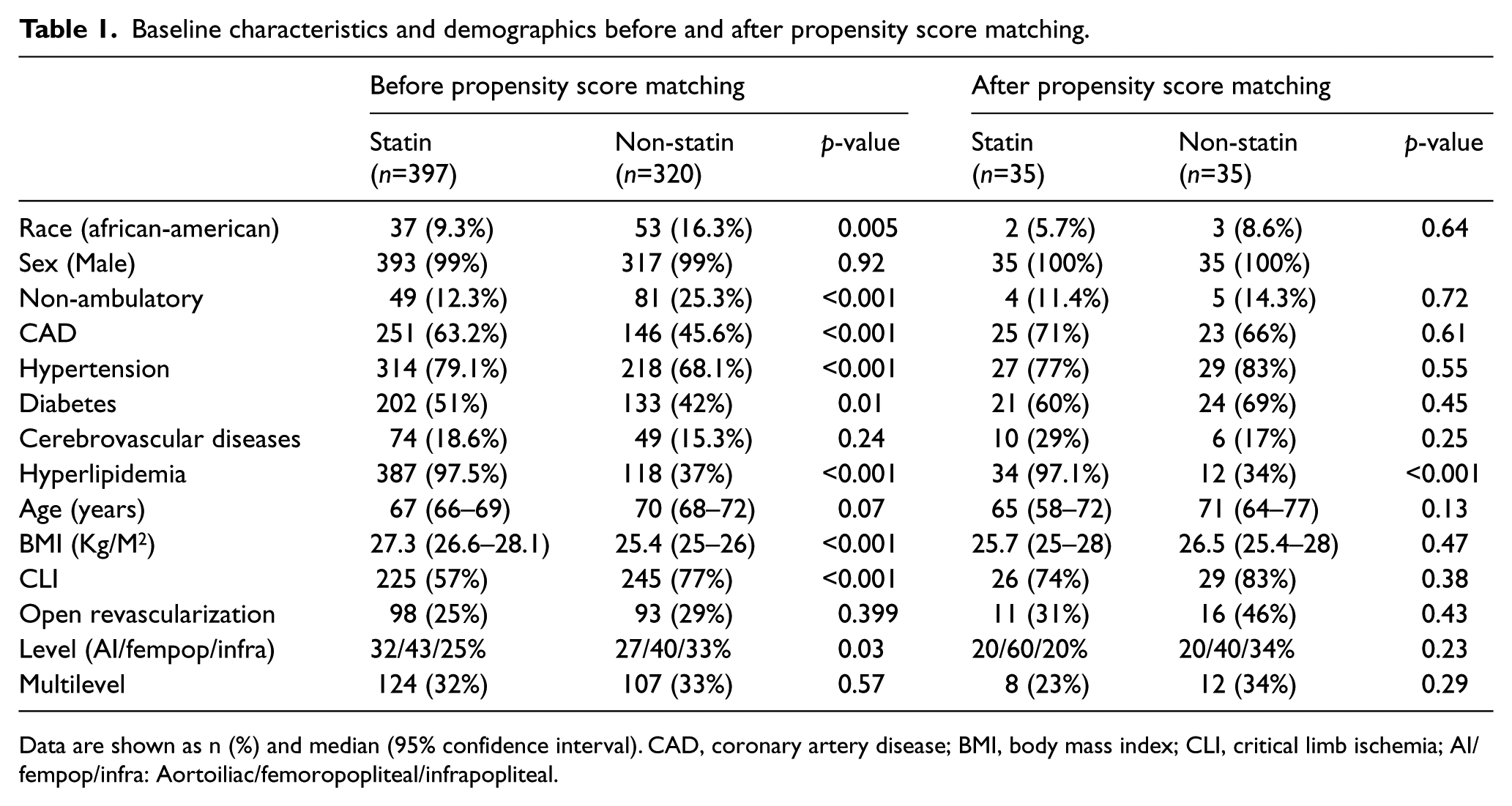
Data are shown as n (%) and median (95% confidence interval). CAD, coronary artery disease; BMI, body mass index; CLI, critical limb ischemia; AI/fempop/infra: Aortoiliac/femoropopliteal/infrapopliteal.
Results
The study population consisted of 717 patients who underwent revascularization over the study period: 397 were on statins and 320 were not. Open revascularization was performed in 25% of patients on statins versus 29% in the non-statin group (p=0.399). Statin use increased from 49% before 31/12/2005 to 64% (p<0.001) after. The baseline characteristics and comorbidities of patients are presented in Table 1. There was a greater prevalence of caucasian race, CAD, diabetes, hypertension, and hyperlipidemia in the statin group. However, the non-statin group had more patients with CLI (77% vs 57%, p<0.001), non-ambulatory status (25.3% vs 12.3%, p<0.001), and lower body mass index (BMI) (25.4±5.0 vs 27.3±4.6 kg/m2, p<0.001).
Based on the pharmacologic profile, the statin group patients were more likely to be on beta-blockers, ACEIs and aspirin, whereas non-statin users were more likely to be on warfarin (Table 2). Patients in the non-statin group also had lower triglyceride and serum albumin levels and a higher estimated glomerular filtration rate (eGFR) than patients on statins (Table 3).
Pharmacologic interventions before and after propensity score matching.
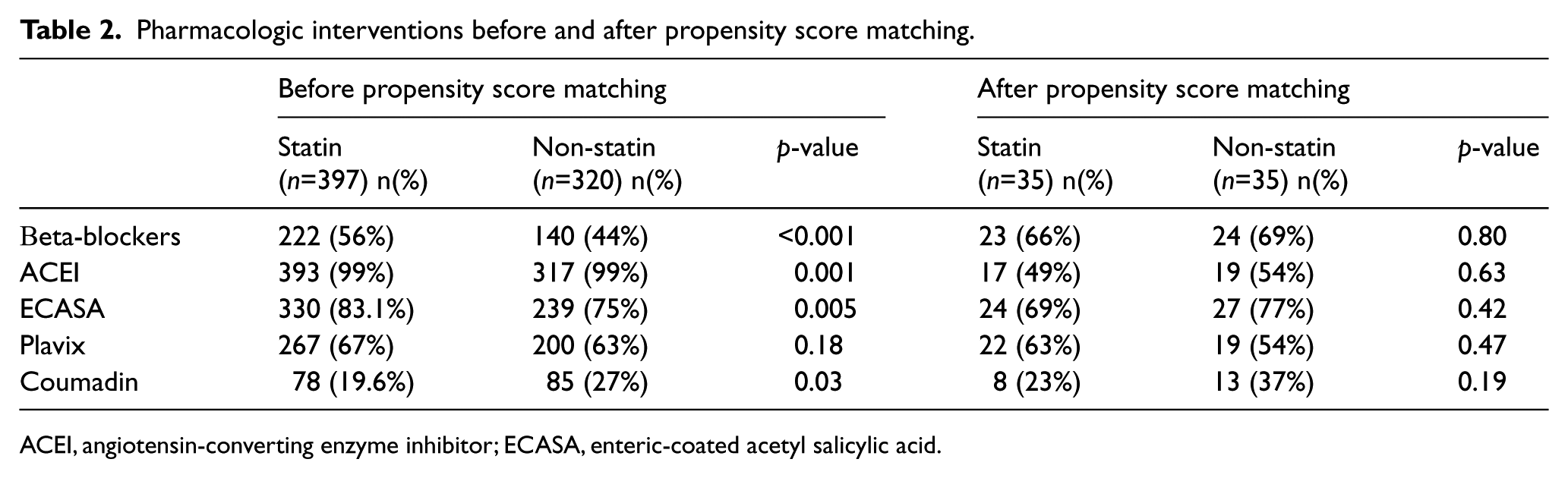
ACEI, angiotensin-converting enzyme inhibitor; ECASA, enteric-coated acetyl salicylic acid.
Preoperative laboratory findings before and after propensity score matching.
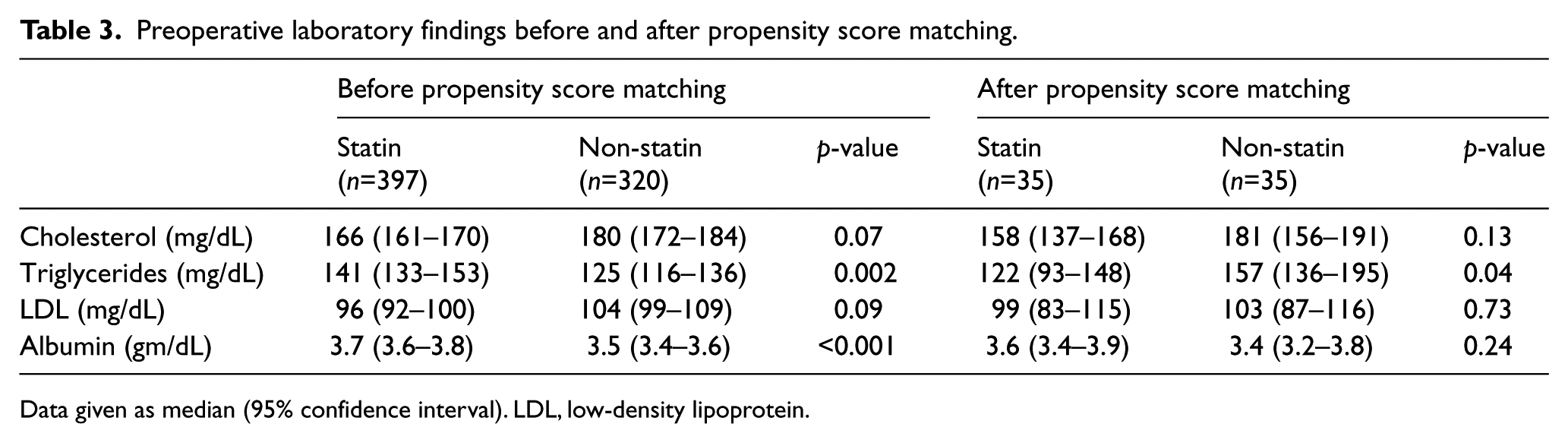
Data given as median (95% confidence interval). LDL, low-density lipoprotein.
After propensity score matching, based on the significant differences in demographic and comorbid conditions, and pharmacologic and laboratory profiles, we had a total of 124 patients: 62 patients on statins and 62 patients in the non-statin group. The only significant difference that remained between the two groups after matching was hyperlipidemia (97% in the statin group and 40% in the non-statin group, p<0.001). Mean follow-up for limb salvage and survival was 50.5±35.2 months.
Major adverse cardiac events (MACE)
The incidence of MACE was significantly lower in patients in the statin group: HR 0.71 (0.60–0.85), p<0.001; but after propensity score matching this difference was no longer significant: HR=0.66 (0.42–1.04), p=0.6.
Patency rates
The mean follow-up for patency was 36.0±30.9 months. There was no difference in primary patency: HR 1.01 (77–1.33), p=0.92. This was unchanged after matching: HR 0.92 (0.52–1.80), p=0.90. Secondary patency rates were also not significantly different before matching (HR 1.13 (0.78–1.63), p=0.52) and after matching (HR 1.15 (0.48–2.71), p=0.75). Statin use was not associated with improved patency in either endovascular (p=0.52 for primary, p=0.84 for secondary patency) or open treated patients (p=0.17 for primary, p=0.40 for secondary patency). The patency rates were also similar in the open-treated patients who had bypass procedures using autologous vein grafts (p=0.66 for primary, p=0.48 for secondary patency), or prosthetic grafts (p=0.46 for primary, p=0.86 for secondary patency, data not shown). Multivariate analysis showed that statins were not associated with improved patency rates: HR 1.15 (0.85–1.56), p=0.34.
Limb salvage rates
The 5-year limb salvage rates were similar between the statin and non-statin groups (80±3% vs 80±3%, p=0.77), with no difference in endovascular (p=0.52) or open treated patients (p=0.85). However, patients who were on statins and had autologous vein grafts, had better limb salvage rates at 36 months than those who were not on statins (91±4% vs 73±7%, p=0.03). There was also a trend for more patients with tissue loss in the non-statin group (69% vs 50%, p=0.08). The freedom from MALE rates was similar between groups (72±3% vs 74±3% in statin vs non-statin groups, p=0.991).
Survival
Overall, 30% of mortalities were due to cardiovascular causes, 10% were due to respiratory failure, 9% were infection-related, 14% cancer and in 37% the cause of death was either unknown or due to other causes. The survival was significantly better in patients who were on statins than those who were not (Figure 1). Univariate analysis showed that statin use was associated with improved survival regardless of diabetic status, method of revascularization, or use of ACEI medications. Statin use also improved survival in patients with COPD. The impact of statin use in improving survival was more pronounced in patients who had CAD, CLI, and hypertension and in those patients who were taking beta-blockers (Table 4).
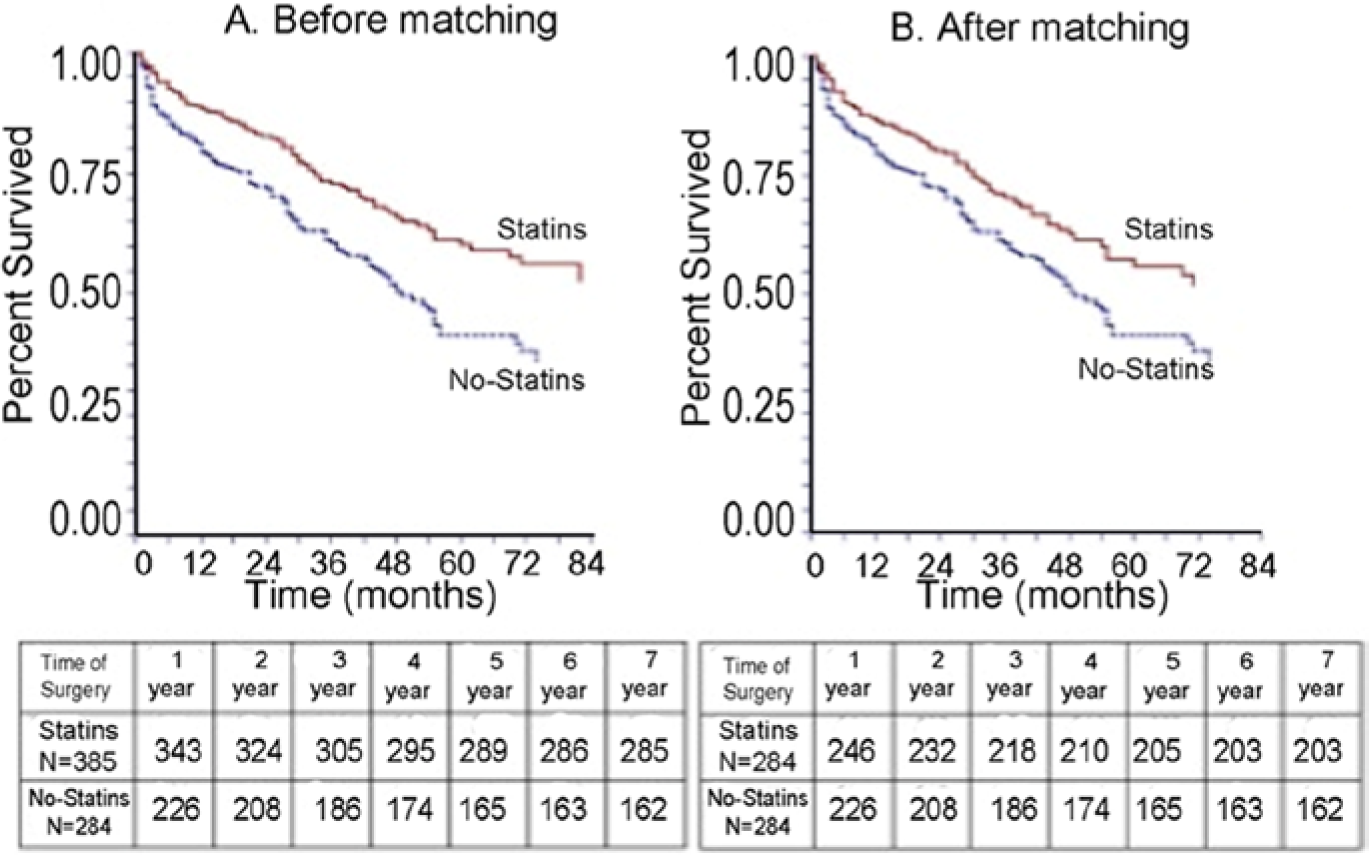
Five-year survival by the Kaplan-Meier method in statin and no statin groups. (A) Unweighted propensity score for survival (p=0.0002). (B) Weighted propensity score for survival (p=0.02).
The association of statin drug use with accumulative hazard ratio in subgroups (6-year survival ± standard error %).
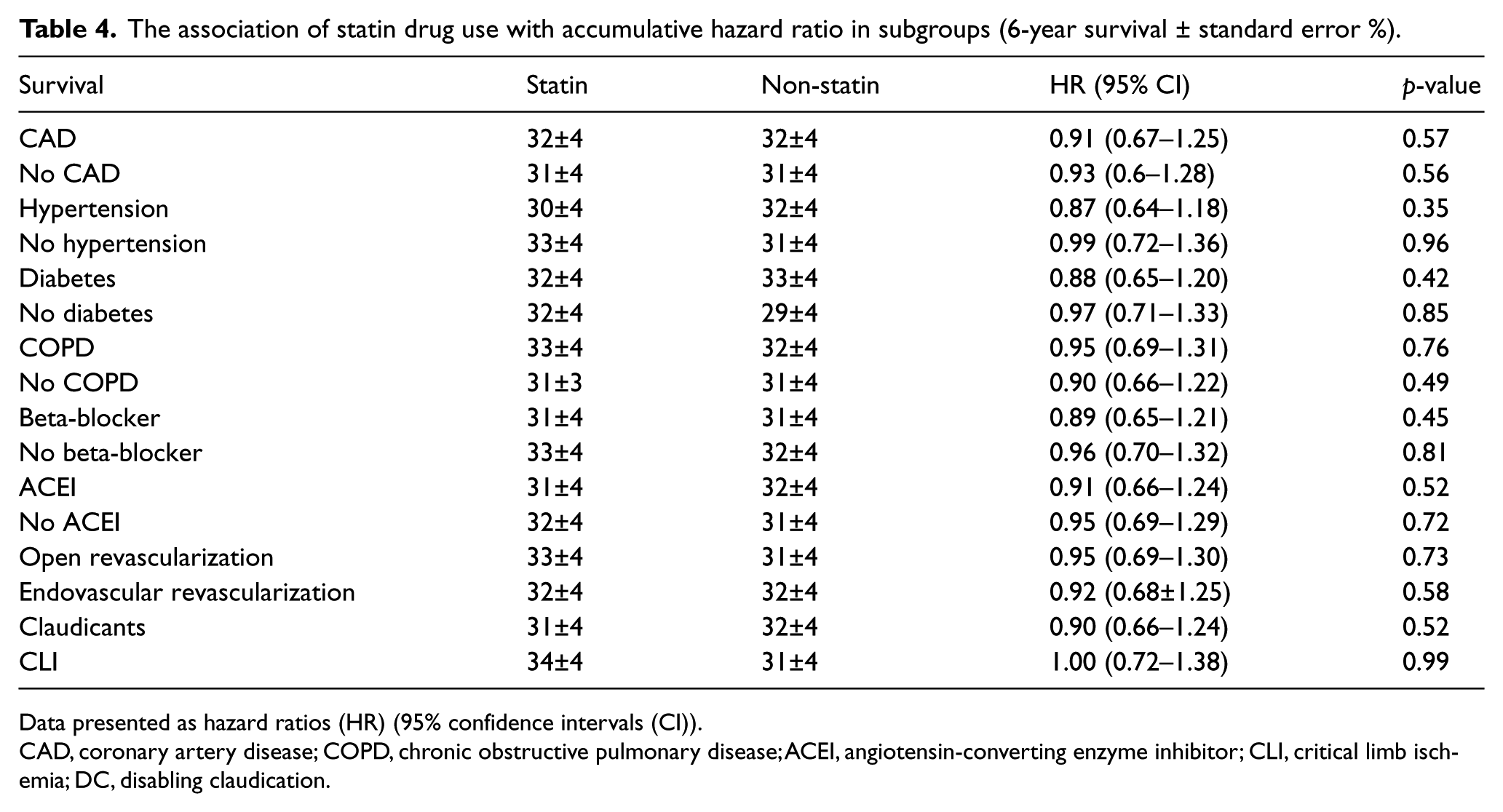
Data presented as hazard ratios (HR) (95% confidence intervals (CI)).
CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; ACEI, angiotensin-converting enzyme inhibitor; CLI, critical limb ischemia; DC, disabling claudication.
Sixty-two patients were matched in each group using propensity scores. Within a 5-year follow-up period, 102 patients (35.9%) died in the statin group while 139 patients (48.9%) died in the control group. At 5 years, using unweighted data, patients taking statins had a HR of death of 0.55 (0.37–0.80), p=0.002. After the data were matched, patients on statins had a HR=0.74 (0.57–0.96), p=0.02, at 5 years (Figure 1B). The pre-operative albumin level was also significantly associated with lower mortality: HR=0.69 (0.51–0.93), p=0.016. Patients with intermittent claudication (IC) had better survival than those with CLI: HR=0.54 (0.32–0.89), p=0.015. CAD, COPD, renal insufficiency, CLI, age > 70, use of beta-blockers and diabetes were independently associated with decreased survival in a multivariate logistic regression model, whereas hypertension, cerebrovascular disease, pre-existing chronic kidney diseases, (CKD), acute kidney injury, (AKI), smoking, type of revascularization (EV vs open), use of ACEI, ECASA, Plavix, and BMI were not.
Amputation-free survival (AFS)
There was a significant difference in AFS in patients who presented with CLI, which were 68±3%, 60±3%, 50±3%, 44±3% and 41±3% in 1, 2, 3, 4, and 5 years postoperatively in the statin group and 62±3%, 51±3%, 42±3%, 31±3% and 25±3% in the non-statin group (p=0.008).
Discussion
The statin drugs are one of the mainstays for medical management of patients with PAD,10,19,20 and their beneficial effects are mediated by both lipid-reducing and plaque stabilization properties. 2 Their use has been associated with early and late survival benefits in patients with various manifestations of arterial disease,16,21,22 but their effects on improving patency and limb salvage rates have been reported with conflicting results,12–15 possibly due to different patient populations with divergent endpoints. There is no defined set-point to start statin drugs in PAD patients; however, the most avidly used guideline is The Adult Treatment Panel III guidelines. 23 Our study included all consecutive patients with intermittent claudication or CLI who underwent endovascular and open revascularization procedures.
One unique feature of our study was that it included all comers with PAD requiring revascularization, including both open and endovascular procedures. The majority, 62% of revascularization procedures, were endovascular. Although there have been numerous studies on the beneficial effects of statins following percutaneous coronary interventions, 24 only two studies14,15 reported on the beneficial effects of statins on peripheral endovascular interventions. The outcomes were similar both in open and endovascular treated patients in our study, with improved survival without any differences in patency and limb salvage rates.
The main finding in this study was that statin use was independently associated with improved survival after revascularization, particularly in patients with CAD and CLI. Although there are a number of studies showing improved survival in patients on statins after vascular surgical procedures14–18,21 or in those with a diagnosis of PAD, 10 there are a few that included only patients with peripheral revascularization procedures.11–15 Only three of these studies showed survival benefit.13–15 Schanzer et al. reported a survival benefit at 1 year (86% vs 81%) with statins in their cohort of patients with CLI who participated in the PREVENT III trial. 13 Aiello et al. 14 reported improved survival at 24 months in patients who had endovascular interventions for CLI (77% vs 62%). Westin et al. 15 reported 21% mortality, 23% MACE in patients without statins compared to 15% mortality, and 18% MACE in patients taking statins and undergoing endovascular interventions for CLI. These differences were significant after adjusting for comorbidities and modes of presentation. The 1-year survival in our group was 84% in statin users and 76% in non-users, and the survival benefit became more pronounced at 5 years (53% vs 36%, p<0.001). Although the survival differences persisted with and without propensity score matching, contrary to the trial by Westin et al. the MACE was not significant after matching in our series, likely due to the small number of eligible patients after matching. Henke et al. reported no survival benefit with statin use, despite the graft patency and decreased amputation rate in their 293 patients after infrainguinal bypass procedures, and found that only ACEI use, along with graft surveillance, was associated with decreased mortality. 12 These authors pointed out that these findings may simply be the consequence of a poor patient compliance rather than the medication itself. Abbruzzese et al. 11 reported no change in 2-year survival in infrainguinal bypass procedures using autologous vein grafts. The survival benefit of statins persisted after multivariate analysis in our patients along with CAD, COPD, renal insufficiency, CLI, and age >75, which was very similar to those reported by Schanzer et al. and Aiello et al.13,14 A study of 2067 patients who underwent infrainguinal bypass for CLI in the Vascular Study Group of New England registry showed improved 5-year survival in patients who presented with CLI (not in claudicants) who were on statin medications perioperatively and, similar to our findings, the 12-month limb salvage and graft occlusion rates were not significantly different in these patients. 25
As in previous reports, we were unable to demonstrate any difference in 30-day morbidity and mortality rates related to the use of statins.11,13 Long-term postoperative morbidity and mortality were decreased by statins in patients following abdominal aortic aneurysm (AAA) repair, carotid endarterectomy and leg revascularization.16–18,22 We also found that the largest difference between the groups occurred at the 60-month postoperative period with a 14% difference for MACE.
The patency rates were identical in our patients regardless of the method of revascularization. Other researchers also found a similar primary patency rate between groups; however, the assisted primary patency and secondary patency rates were significantly better in patients on statins.11,13 A better primary and secondary patency rate in the statin group has been reported. 14 The anti-inflammatory properties of statins might have contributed to the improved patency independent of their lipid-reducing effects observed by some other investigators.24,26 It is possible that the role of statins on patency was possibly masked by other important technical and pharmacological factors (i.e. antiplatelets) in our study.
The limb salvage rates in our patients were almost identical with or without statins, irrespective of the method of revascularization. Henke et al. found improved limb salvage and patency rates with the use of statins. 12 In an administrative database of Medicare patients treated as inpatients for chronic limb ischemia, Vogel et al. 27 demonstrated better limb salvage in patients who were on statin drugs; however, this was observed only in claudicants and those with rest pain, and there was no difference in limb salvage in those with tissue loss, which is not dissimilar to our findings. Although improved limb salvage was reported by another study where the majority (66%) of patients had autologous vein bypasses, 12 Abbruzzese et al. did not show any differences in an all-autologous bypass series. 11 It is important to note that there were more patients with tissue loss in the non-statin group, and the reason for improvement in limb salvage without a difference in patency rates by the use of statins remains unclear.
Despite the role of statins in decreasing cardiac morbidity and mortality, these drugs are still under-prescribed in patients with PAD. Although statin usage of 57% seems to be low, it is consistent with other reports.12,14,28,29 Clearly, this is one area that we can improve on with the potential of optimizing medical management of our patients with symptomatic limb ischemia, and potentially improve their survival. The timing of statin administration is still being disputed, but if indeed our observations were true, starting statins prior to an elective procedure would likely precondition the patient at the time of the procedure.
Feringa et al. suggest that intensified lipid-lowering therapy in patients with an ABI of <0.9 is associated with improved outcomes. 19 The American College of Cardiology/American Heart Association recommend targeting a LDL level of 70 mg/dL in high-risk patients with PAD. 28 Since the beneficial effects of statins are multifaceted,1,3,30 all patients undergoing peripheral revascularization with no contraindications should be considered for statin therapy. Assessment of the patients by the anesthesiologists in preoperative clinics may be a good opportunity to discuss therapeutic options, to start the treatment and to notify the primary physicians to continue the treatment postoperatively.
Limitations
Our study limitations include its retrospective nature and having a relatively small sample size in a nearly all-male population. It is also not the intention of this paper to draw any causality conclusion. We also did not investigate the actual duration of treatment, patient compliance, or documentation of other lipid-lowering agents (fibrates), nor did we monitor lipid profiles over the follow-up period. We also have no information on those patients who may have been started on statins by their primary providers after revascularization, which may have impacted the outcomes.
The LDL levels being similar in patients with or without statins also raises the issue of their efficacy, and we cannot rule out that subtherapeutic use of these drugs may account for the lack of effect on patency and limb salvage in our study. Lastly, the issue of compliance and socioeconomic status creating a selection bias in the use of statins cannot be excluded.
Conclusion
In summary, statins seem to be associated with improved survival in patients with symptomatic PAD requiring intervention, and may also have beneficial effects in reducing vascular events in the first 3 months following revascularization. Although statin use was not found to be associated with long-term patency and limb salvage, it was associated with improved overall survival, especially in patients with a history of CAD and CLI.
Footnotes
Declaration of conflicting interest
None of the authors listed reports any conflict of interest for this manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.