
Abstract
The popliteal artery (PA) is, after aorta, the most common site for aneurysm formation. Why the PA is more susceptible than other peripheral muscular arteries is unknown. We hypothesized that the wall composition, which in turn affects wall properties, as well as the circumferential wall stress (WS) imposed on the arterial wall, might differ compared to other muscular arteries. The aim was to study the WS of the PA in healthy subjects with the adjacent, muscular, common femoral artery (CFA) as a comparison. Ninety-four healthy subjects were included in this study (45 males, aged 10–78 years and 49 females, aged 10–83 years). The diameter and intima-media thickness (IMT) in the PA and CFA were investigated with ultrasound. Together with blood pressure the WS was defined according to the law of Laplace adjusted for IMT. The diameter increased with age in both PA and CFA (p<0.001), with males having a larger diameter than females (p<0.001). IMT increased with age in both PA and CFA (p<0.001), with higher IMT values in males only in PA (p<0.001). The calculated WS was unchanged with age in both arteries, but lower in PA than in CFA in both sexes (p<0.001). In conclusion, this study shows that the PA and CFA WS is maintained during aging, probably due to a compensatory remodelling response with an increase in arterial wall thickness. However, the stress imposed on the PA wall is quite low, indicating that mechanisms other than WS contribute to the process of pathological arterial dilatation in the PA.
Introduction
The popliteal artery (PA), a peripheral muscular artery, is, after aorta, a central elastic artery, the most common site for aneurysm formation. About 30% of patients with popliteal aneurysm will develop abdominal aortic aneurysm (AAA) 1 and 5% of patients with AAA may be affected with a popliteal aneurysm. 2
Arterial distensibility in peripheral muscular arteries shows no or very little age-related changes in contrast to central elastic arteries where a large decrease in distensibility is seen.3–8 However, a paper from our group suggests that the wall function of the PA differs from other peripheral arteries with a marked age-related decrease in distensibility. 9 In this aspect, the PA shows a striking similarity to the abdominal aorta, indicating that the functional arrangements of arterial wall components as well as the age-related changes are similar in the two arterial regions. 9 This may have implications for the similar susceptibility to aneurysm formation, as well as the association of dilating disease between the PA and the abdominal aorta.
The possibility of an imbalance between circumferential wall stress and wall strength, being an underlying factor responsible for arterial dilatation, has been emphasized by the found relation between blood pressure and diameter increase both in healthy arteries and in arteries affected by aneurysmal dilatation.9,10 The aim of this study was to investigate, in healthy subjects, if there is a different regulation of circumferential wall stress in the PA compared to another peripheral muscular artery; the common femoral artery (CFA), not being affected by pathological dilation at the same extent as the PA.
Materials and methods
Materials
Ninety-four healthy subjects participated in this study (45 males, range 10–78 years and 49 females, range 10–83 years). In 44 males and 45 females, ultrasonic examination of the diameter and intima-media thickness (IMT) of the PA was performed successfully, and of the CFA in 36 males and 42 females.
The subjects were all non-smokers, free from medications and did not have any history of hypertension, cardiopulmonary or renal disease, cerebral-vascular events, diabetes or intermittent claudication. The ankle–brachial index (ABI) was greater than 1.0 in all subjects. Pregnancy was an exclusion criterion. All subjects gave informed consent to participate in this study according to the Declaration of Helsinki, and the Ethics Committee at Lund University, Sweden, approved the study.
Examination
The measurements were performed by an experienced ultrasound technician in a darkened and quiet room. At the beginning of the investigation the non-invasive pressure was measured with a cuff in the upper arm bilaterally. Since no significant difference in pressure between the arms was found, the right arm was used due to the location of the ultrasound equipment in the investigation room.
The subjects rested in a supine position for at least 15 minutes before the ultrasound measurements. The right CFA was examined at the site of the inguinal fossa, with the hip joint as a landmark and the right PA was examined at the site of the popliteal fossa, with the patient prone, using the patella as a landmark. The arteries were visualized in the longitudinal section and care was taken to minimize pressure from the transducer to the skin.
Measurement of intima-media thickness and lumen diameter
The IMT was measured as a substitute to arterial wall thickness. 11 The adventitial layer was not included, but it is evident that the major part of the wall is studied.12,13 Further, the relation between adventitial thickness and the IMT is unaffected by sex or age. 14 Accordingly, during recent years the IMT has been used as a surrogate to arterial wall thickness in the calculation of wall stress.11,15–18
For measuring the IMT and lumen diameter (LD), a Philips P700 ultrasound device was used (Philips Ultrasound, Santa Ana, CA, USA) with a 7.5 MHz linear transducer to visualize the CFA and a 5 MHz linear transducer to visualize the PA. A longitudinal perpendicular image of the vessel was insonated and recorded on a video monitor, two images of good quality were frozen in end-diastole, according to the prevailing standard of IMT measurements, and the IMT of the far wall as well as the LD were measured manually by tracing a cursor along the echo edges on a section of 10 mm with the aid of the digitizer.11,19,20 This provides approximately 100 boundary points from which the mean value of IMT and LD is automatically calculated (VAP version 2.0, Department of Applied Electronics, Chalmers University of Technology, Gothenburg, Sweden). The accuracy of the technique was studied by Pignoli et al., 20 who showed a good correlation between ultrasound and histology measurement of the arterial wall. The reproducibility in the PA and CFA measurements is acceptable, coefficient of variation 10% and 2% for IMT and LD, respectively. 11 The mean value of IMT and LD was calculated based on two images with good recording quality.
Wall stress
Stress is the force per unit cross-sectional area. In the artery, stresses are present along the circumferential, the radial and the longitudinal axes. Since arteries elongate little during the cardiac cycle and the compression of the vessel wall is considered negligible, we have focused on the circumferential wall stress (dyne/cm2), calculated according to the law of Laplace21,22
where DP = diastolic pressure, LD = the lumen diameter (cm) and IMT = intima-media thickness (cm). Diastolic pressure (dyne/cm2) was used since IMT measurements were performed in diastole: 1 mmHg equals 1333 dyne/cm2. Body surface area (BSA) was estimated according to Du Bois’s formula: 23 BSA (m2) = weight0.425 (kg) × height0.725 (m) × 71.84.
IMT was used in the measurements as arterial wall thickness, even though the adventitia layer is not included in IMT. However, evidence points out that the major part of the total wall thickness is included as shown (e.g. in the abdominal aorta, iliac and coronary arteries). Further, since the relation between adventitial thickness and the IMT does not seem to be affected by age and sex, this approximation is acceptable. Accordingly, during recent years IMT has been used as a surrogate for wall thickness in the calculation of WS.17,18,24–27
When measuring the diastolic blood pressure, it would be favourable to measure it invasively ‘in situ’, since the blood pressure undergoes transformation in the arterial tree. 22 Direct measurement of blood pressure in the PA and CFA may be performed, but seems unethical and difficult to use in larger population studies. Instead, we used the brachial artery for blood pressure measurements. Studies in our laboratory, however, show that blood pressure in the CFA compared with auscultatory blood pressure in the upper arm, has only a slightly lower diastolic blood pressure. 8
Statistics
Pearson’s correlation coefficient was used to assess the relationship between age and LD, IMT and wall stress. Differences between sexes were tested using analysis of covariance. Paired Student’s t-test was used to calculate differences between studied vessels. A multiple regression model was performed on IMT and LD. A p-value <0.05 was considered to be significant. The statistical analyses were performed in IBM SPSS 19.0 and graph illustrations were performed in IBM SPSS 19.0 and Microsoft Excel 2007.
Results
Table 1 presents the demographic data of the studied population.
Demographic data of the studied population.
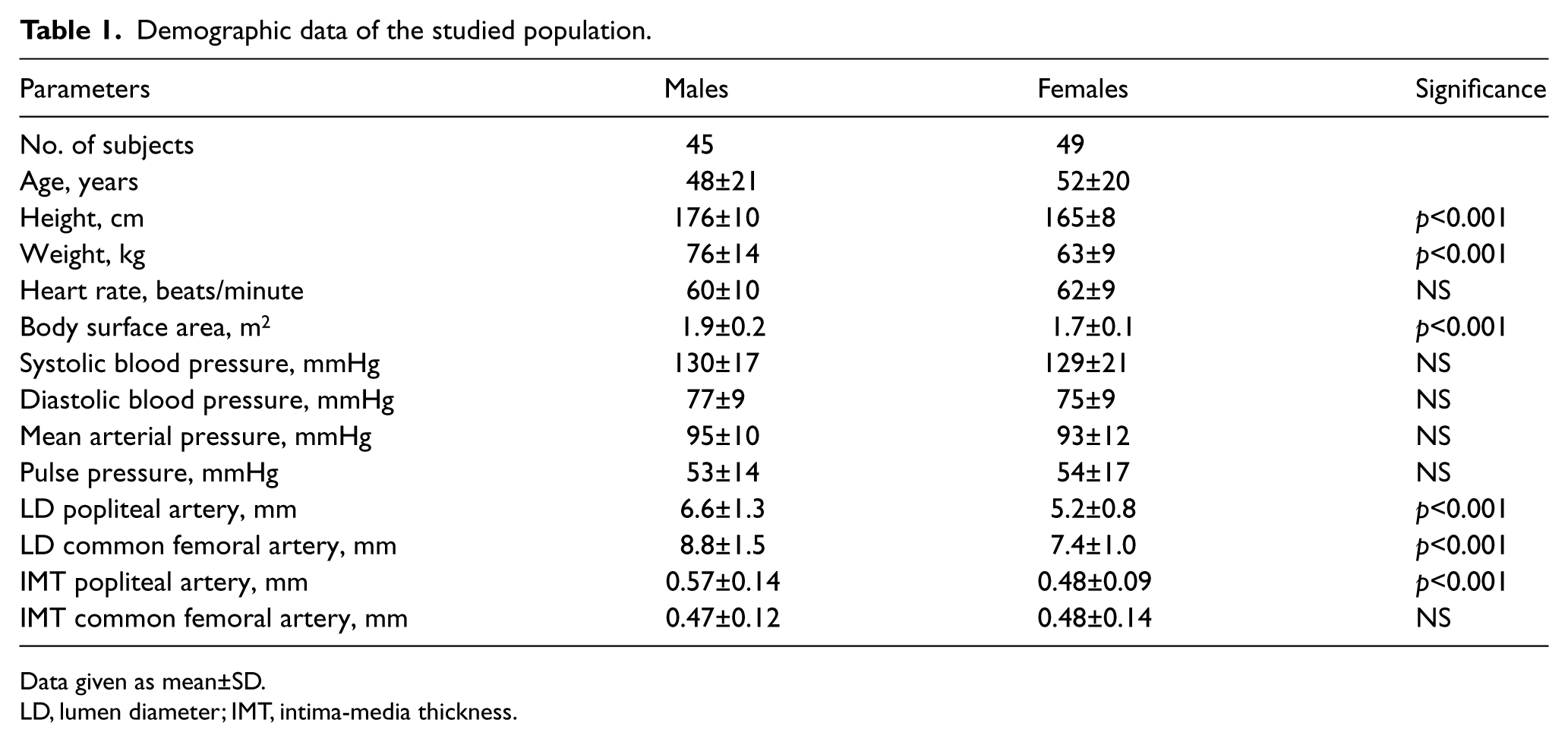
Data given as mean±SD.
LD, lumen diameter; IMT, intima-media thickness.
Lumen diameter of the popliteal artery and common femoral artery
The LD of the PA increased with age in both males (r=0.68, p<0.001) and females (r=0.53, p<0.001), with 23% higher LD values in males than in females (p<0.001). In adults between the ages of 25 and 70 years, the LD increased from 5.42 to 7.43 mm in male subjects (37%) and from 4.74 to 5.67 mm (20%) in females. The LD of the PA was mainly affected by age (46% for males vs 28% for females), while the BSA and systolic blood pressure (SBP) only had a minor influence (BSA 10% for males vs 2% for females; SBP 11% for females).
The LD of the CFA increased exponentially with age in both males (r=0.58, p<0.001) and females (r=0.50, p<0.001), with males having 20% larger LD values than females (p<0.001). In adults between the ages of 25 and 70 years, the LD of the CFA increased from 7.78 to 9.74 mm (25%) and 6.65 to 7.61 mm (14%) in males and females, respectively. The LD of the CFA was mainly affected by age in both males and females (33% vs 25%). Only in males did BSA and diastolic blood pressure (DBP) influence the LD (18% vs 7%). The LD values were higher in the CFA than in the PA in both males (p<0.001) and females (p<0.001).
Intima-media thickness of the popliteal artery and common femoral artery
The IMT values of the PA increased exponentially with age (r=0.82 and r=0.62) in males and females, respectively (p<0.001), with males having IMT values 14% higher than females (p<0.001). In adults between the ages of 25 and 70 years, the IMT of the PA increased from 0.42 to 0.63 mm (50%) in males and from 0.41 to 0.54 mm (32%) in females. The IMT of the PA was mainly influenced by age (68% and 38% in males and females, respectively) and the LD influenced only males in a modest way (6%).
The IMT of the CFA increased exponentially with age in males (r=0.73, p<0.001) and females (r=0.47, p<0.005), but without any sex difference. In adults between the ages of 25 and 70 years, the IMT of the CFA increased from 0.38 to 0.57 mm (50%) and from 0.39 to 0.54 mm (39%) in males and females, respectively. The IMT of the CFA in males was affected by age (53%) and LD (7%). In females, the IMT was only affected by age (22%). In males, the IMT of the CFA was thinner than in the PA (p<0.001), while in females no difference was seen.
Wall stress of the popliteal artery and common femoral artery
Figure 1 shows the wall stress in the PA (A) and CFA (B) in relation to age in males and females. There was no increase in wall stress with age either in PA or in CFA. Males had 11% and 20% higher wall stress than females in the PA and the CFA (p<0.01 and p<0.001, respectively). Figure 2 shows the difference in wall stress in PA and CFA in males and females. Wall stress was higher in the CFA than in the PA in both males and females (p<0.001).
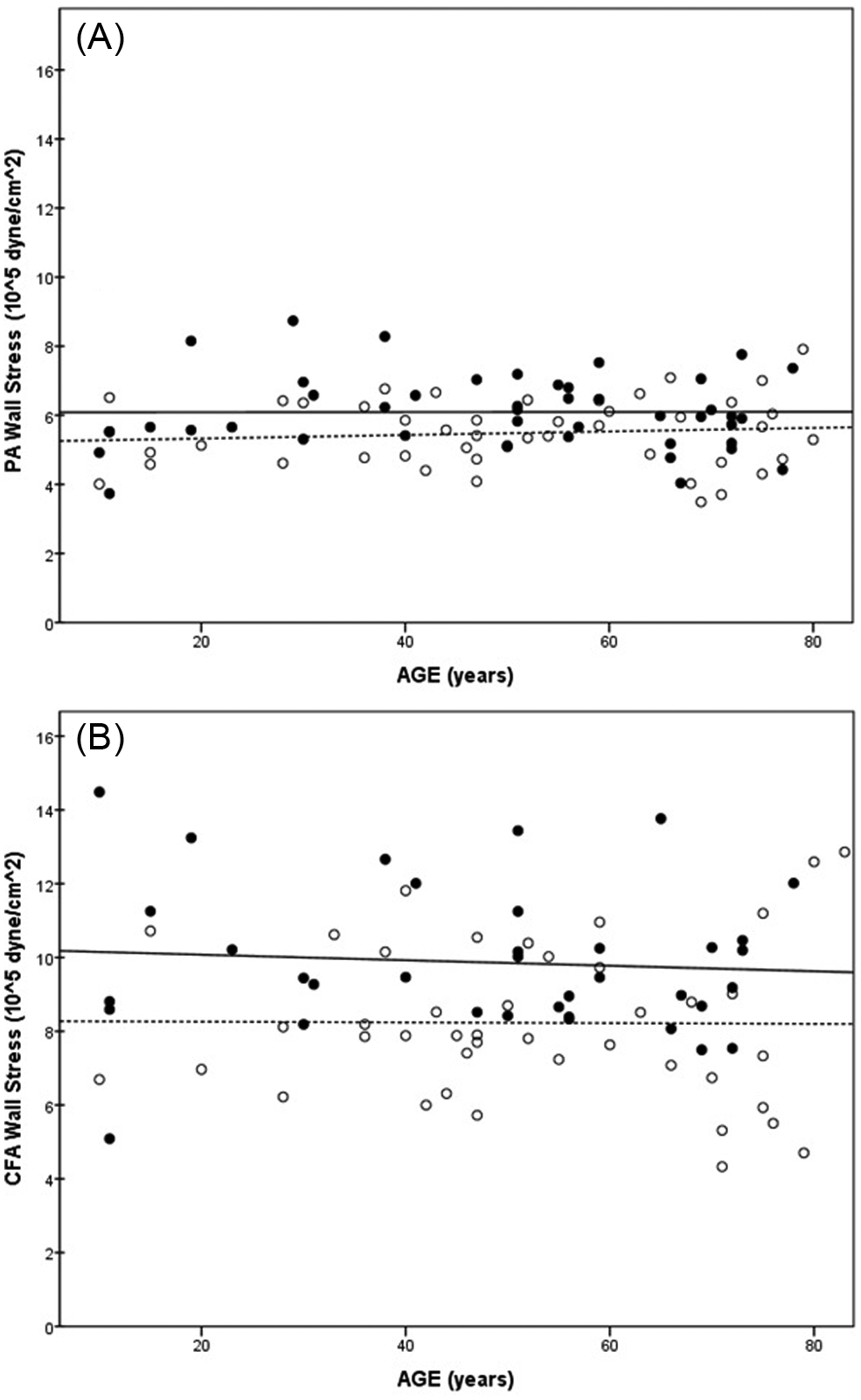
(A) Wall stress of the popliteal artery (PA) in relation to age; (B) wall stress of the common femoral artery (CFA) in relation to age (males: black circles, solid line; females: open circles, dashed line).
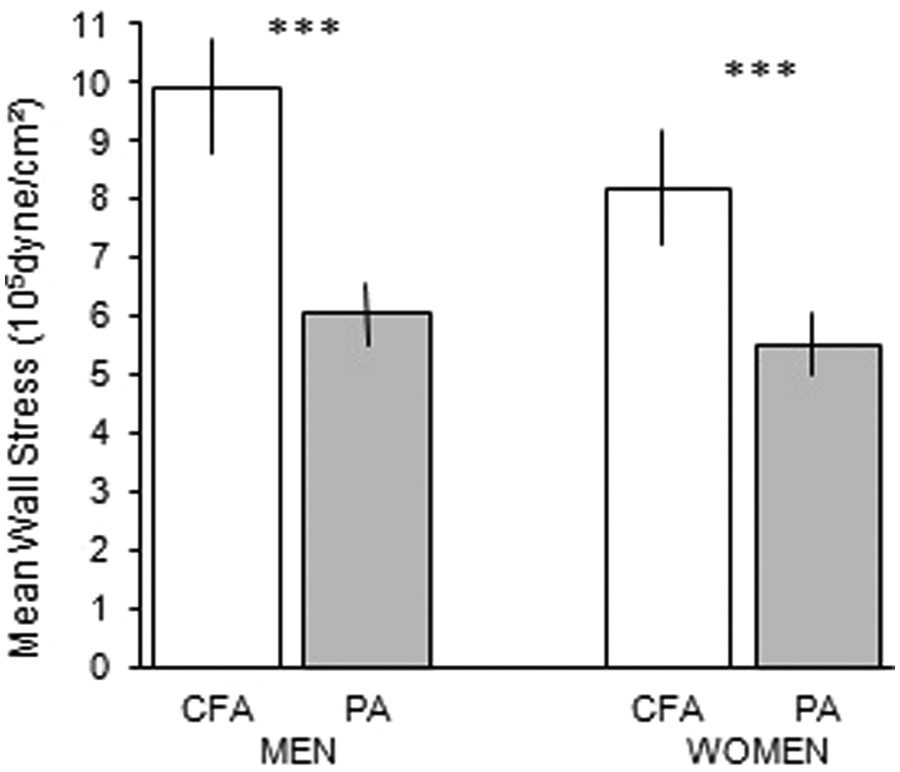
Mean wall stress in the popliteal artery (PA) (grey bars) and in the common femoral artery (CFA) (white bars) in males and females. Note the lower wall stress in the PA compared with the CFA in both males and females (***p<0.001).
Blood pressure
There was an age-related increase in SBP (p<0.001), DBP (males, p<0.001; females, p<0.005), mean arterial blood pressure (p<0.001) and pulse pressure (males, p<0.05; females, p<0.001) without any pressure differences between the sexes.
Discussion
The arterial wall structure changes with age, with an increase in collagen, decrease in elastin and thickening of the vessel wall. In healthy subjects, the mechanical properties in central elastic arteries such as the aorta show an age-related pronounced decrease in distensibility, while peripheral muscular arterial walls seem practically unaffected, indicating less of an age-related arterial wall remodelling and degeneration.3–8 In central elastic arteries, the structure of the wall is the main determinant of wall mechanics, while in muscular arteries – intrinsic myogenic mechanisms, the endothelial-dependent detection of a change in wall shear force with a resultant release in nitric oxide, as well as sympathetic modulation of vascular smooth muscle tone, may be more important in the regulation of arterial wall compliance.28,29
Despite the fact that the PA is characterized as a muscular artery, it is, after aorta, the most common location in the arterial system for aneurysm formation. Thus, about 5% of patients with AAA may be affected by popliteal aneurysm 2 and about 30% of those found with popliteal aneurysm also have an AAA. 1 Why the PA is more susceptible than other peripheral muscular arteries to aneurysmal disease is at present unknown. A study from our laboratory showed, however, that the wall properties of the PA are affected by a marked decrease in distensibility and an increase in stiffness during aging, and show similar pattern of abdominal aorta. 9 This is not the behaviour of a true muscular artery, and differs from the near superficial and CFA region, as well as other regions of muscular arteries where no decrease in distensibility with age has been found.3–5,8,30,31 The reduced distensibility of the popliteal wall, as in the aorta, probably reflects a decreased elastin to collagen ratio.
The diameter in the PA and CFA and blood pressure increased with age. It has been demonstrated experimentally both in vitro and in vivo that increased pressure as well as diameter activates the smooth muscle cell production of connective tissue components, with an increase in matrix production as well as wall thickness.32–35 This might be modulated by the matrix metalloproteinase system (e.g. MMP-2 and MMP-9) that has an important role in maintaining the homeostasis of the extracellular matrix.36–39 Despite the age-related pressure and diameter increase, the circumferential wall stress in the PA and CFA remained unchanged, which seems to be due to a compensatory increase in wall thickness and thus stabilized at a pre-determined level according to the law of Laplace (Figures 1 and 2). This indicates that circumferential wall stress is an important determinant for vessel wall remodelling during aging in man. 32 The wall stress has been shown to be high in the abdominal aorta, with an age-related increase in wall stress in the abdominal aorta observed only in males and not in females, which is in accordance with the increased prevalence of AAA in males. 18 In diabetic patients, however, the wall stress of the abdominal aorta is reduced, probably due to the compensatory wall remodelling response of an increased IMT compared to healthy controls, and reflects the reduced risk of aneurysmal disease in diabetic patients. 27
The possibility of an imbalance between circumferential wall stress and wall strength, being an underlying factor responsible for arterial dilatation, is emphasized by the found relation between blood pressure and diameter increase both in healthy arteries and in arteries affected by aneurysmal dilatation.9,10,40 Despite the fact that the PA is more prone to aneurysmal dilatation than the CFA, the circumferential wall stress was lower in the PA than in the CFA (Figures 1 and 2). This indicates that predisposing factors other than circumferential wall stress may be of importance. Since there is an intricate balance between circumferential wall stress and wall strength, it might be argued that not only circumferential wall stress, but also wall strength, might be lower in the PA than in the CFA, making the PA more susceptible to risk factors. Repetitive longitudinal deformation by flexion has been correlated to subsequent lesion progression and may also be of relevance for the preponderance of pathological dilatation in the PA. Anecdotal evidence from cavalry officers indicates that tight boots together with repeated flexion and extension while riding may traumatize the PA and cause an aneurysm.41,42 Further, the propagating arterial pulse wave causes cyclic changes in arterial lumen size and shape. For the femoral artery, the change in lumen diameter is about 10%. 8 In the PA, however, it becomes much smaller with age because of the increase in wall stiffness. 9 Thus, a zone of compliance mismatch between the femoral artery and PA occur. In combination with stiff atherosclerotic plaques bending at the junction between stiff plaques and vessel wall, the wall constituents may weaken, in accordance with findings in the coronary tree.43,44
Another factor to consider is that the PA below the knee is divided into three much smaller arteries that may be of relevance for increased pressure wave reflections, possibly making the PA more susceptible to aneurysmal dilatation, in analogy with the increased risk of AAA in patients with traumatic above-knee amputations. 45 Finally, during the daytime, the PA is repetitively exposed to upright posture with increased local haemodynamic burden. 46
In conclusion, this study shows that wall stress both in the popliteal and CFA is unaffected by aging. This seems to be caused by a compensatory remodelling response with an increase in arterial wall thickness. The absence of high wall stress in the PA, and instead lower stress than in the CFA – a peripheral muscular artery not affected by aneurysmal dilatation to the same extent, indicates that mechanisms other than wall stress contribute to the process of pathological arterial dilatation in the PA.
Footnotes
Declaration of conflicting interest
The authors declare no conflicts of interest.
Funding
This study was supported by grants from: The Swedish Research Council [12661]; Swedish Heart and Lung Foundation [20130650]; Futurum – the Academy for Healthcare, County Council, Jönköping, Sweden [259701]; King Gustav V and Queen Victoria’s Foundation.