
Abstract
The Walking Estimated-Limitation Calculated by History (WELCH) questionnaire has recently been proposed as a valid and simple instrument for assessing walking limitation in patients with intermittent claudication. The aim of this study was to validate an English version of the WELCH questionnaire in an English native population. Thirty-nine patients (ankle–brachial index 0.59 ± 0.16, age 65 ± 11 years, 82% male) completed an English version of the WELCH questionnaire. Maximum walking distance was measured objectively using the Gardner–Skinner treadmill test and the 6-minute walk test. The median WELCH score was 24 (9–39). Maximum walking distances were 412 m (149–675 m) for the treadmill test and 381 ± 88 m for the 6-minute walking test. The Spearman’s correlation coefficient was ρ = 0.59 between the WELCH score and treadmill distance (p < 0.001) and ρ = 0.82 between the WELCH score and 6-minute walk distance (p < 0.001). These findings suggest that the English version of the WELCH questionnaire is a valid instrument for assessing walking impairment in patients with intermittent claudication.
Introduction
Approximately one third of patients with lower-limb peripheral artery disease (PAD) have ‘typical’ intermittent claudication, 1 which is defined as lower-limb pain or discomfort that is evoked by walking and relieved by rest of less than 10 minutes. 2 Intermittent claudication impairs patients’ walking capacity, 3 and the degree of limitation can be quantified by treadmill testing. 4 However, treadmills are not readily available to most physicians and testing procedures can be time-consuming and expensive. The use of questionnaires facilitates the estimation of walking impairment and they are particularly useful for those who cannot perform treadmill tests or in large epidemiological studies. 5 Various questionnaires have been proposed, among which the recently developed Walking Estimated-Limitation Calculated by History (WELCH) questionnaire 6 seems to compare favourably to the Walking Impairment Questionnaire (WIQ), a largely studied tool.7 –10 Compared to the WIQ, the WELCH is shorter, suffers fewer errors when self-completed, provides comparable correlation with treadmill results, and can be scored easily without a calculator or computer spreadsheet. 6 These characteristics make it attractive for routine clinical use. However, the WELCH has only been validated in France (i.e. French language) and against a single specific treadmill procedure. The aim of the present study was to validate an English version of the WELCH in a group of English patients with intermittent claudication.
Methods
Study design and population
With local research ethics committee approval, 39 patients with intermittent claudication due to PAD were recruited from the Sheffield Vascular Institute at the Northern General Hospital, Sheffield, United Kingdom. The diagnosis of PAD was based on an ankle–brachial index <0.90 at rest on one or both legs and/or a prior imaging investigation showing stenoses or occlusions of the aorta and/or lower-limb arteries. Exclusion criteria included the absence of PAD, asymptomatic PAD, rest pain attributable to PAD, walking limitation by factors other than claudication (e.g. dyspnoea, angina, arthritic pain), history of intermittent claudication <6 months, and revascularization or other major surgery within the previous 6 months. Written, informed consent was obtained from patients prior to their participation in this study.
All participants visited the testing facility on two occasions. On visit 1, participants’ medical history was recorded and all testing procedures were described. On visit 2, participants underwent a clinical examination by a consultant vascular surgeon (SN) before completing the English version of the WELCH questionnaire, 6 the Gardner–Skinner incremental treadmill test, 11 and the 6-minute corridor walk test. 12 The tests were completed in this order with >20 minutes of recovery between the two objective walking tests.
Completion, correction and scoring of the WELCH questionnaire
Patients were asked to complete the WELCH questionnaire without help and with no time limitation. The questionnaire version used was the one proposed by the authors in the original paper. 6 The questionnaires were then checked for errors by a researcher (GT). Missing, duplicate (i.e. two or more answers for the same item) and paradoxical (i.e. higher duration reported for a harder task) answers were discussed with the patient and corrected as appropriate. Questionnaires were scored as described previously 6 and an example of scoring is provided in Figure 1. In brief, each of the eight answers within the first three questionnaire items has a value ranging from 0 to 7, and each of the five answers proposed for the last item dealing with usual walking speed has a coefficient ranging from 1 to 5. The score is calculated as the sum of the values for the first three, minus one, multiplied by the coefficient for the final (walking speed) questionnaire item. The WELCH score ranges from 0 to 100, with zero indicating a patient who can only walk for 30 seconds when walking slowly and who usually walks much slower than relatives, friends or people of the same age. A score of 100 would indicate a patient who can walk 3 hours or more, even when walking fast, and who usually walks faster than relatives, friends or people of the same age.
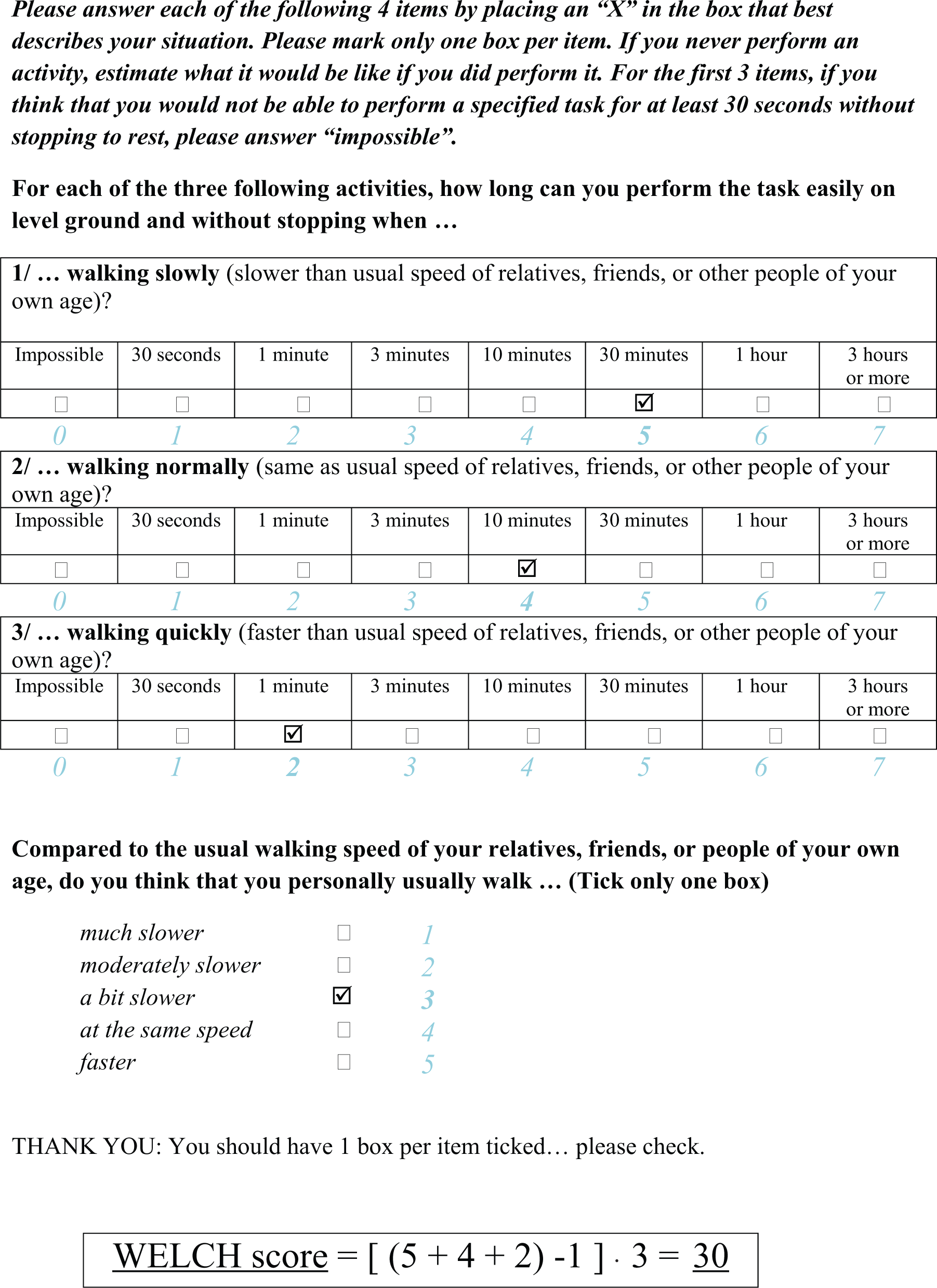
Example of the scoring of a WELCH questionnaire (note that item values and coefficients are presented in the present figure to facilitate the reading but are not available to the patient). Modified with permission. 6
Gardner–Skinner incremental treadmill walking test
Each participant performed the Gardner–Skinner incremental treadmill walking test, as previously described. 11 In brief, participants walked at 3.2 km/h (2 miles/h) with a 2% increase in gradient every 2 minutes, starting from 0%. The treadmill test duration was maximized to 20 minutes. Participants were instructed to walk until leg pain forced them to stop, at which point maximum walking distance was recorded. We also recorded the initial claudication distance (i.e. the distance at which claudication symptoms were first noticed by the patient). Heart rate was recorded continuously by electrocardiogram (Cardioperfect; Welch Allyn, Skaneateles Falls, NY, USA).
Six-minute walk test
At least 20 minutes after the treadmill test, participants completed a 6-minute walk test in which they were instructed to walk as far as possible within 6 minutes. 12 This test simulates community walking conditions better than treadmill testing; 13 however, patients are still required to walk at a forced pace. A straight 20-m course was used and the distance completed after 6 minutes was recorded. Heart rate was continuously monitored using heart rate telemetry (Polar Electro, Kempele, Finland).
Sample size calculation and statistical analysis
The sample size calculation was based on the number of patients required to find a significant correlation between WELCH scores and maximum walking distance on the Gardner–Skinner test. Assuming a correlation coefficient of at least 0.5, 6 and using a two-tailed alpha = 0.05 and power of 90%, the estimated sample size was 37 (www.quantitativeskills.com).
Normality of distribution was tested using the Shapiro–Wilk test. Data are presented as mean ± SD for normally distributed variables and median (25th to 75th percentiles) for non-normally distributed variables. The correlations between WELCH scores and the objectively measured maximum walking distance (from both the treadmill and 6-minute walk tests) were quantified using Spearman’s rank correlation coefficient (ρ). Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS, Version 19.0; SPSS UK Ltd, Bedfont Lakes, UK) and statistical significance was accepted at p ≤ 0.05.
Results
Thirty-nine participants completed the study. Characteristics of the recruited population are presented in Table 1.
Demographic and descriptive variables (n = 39).
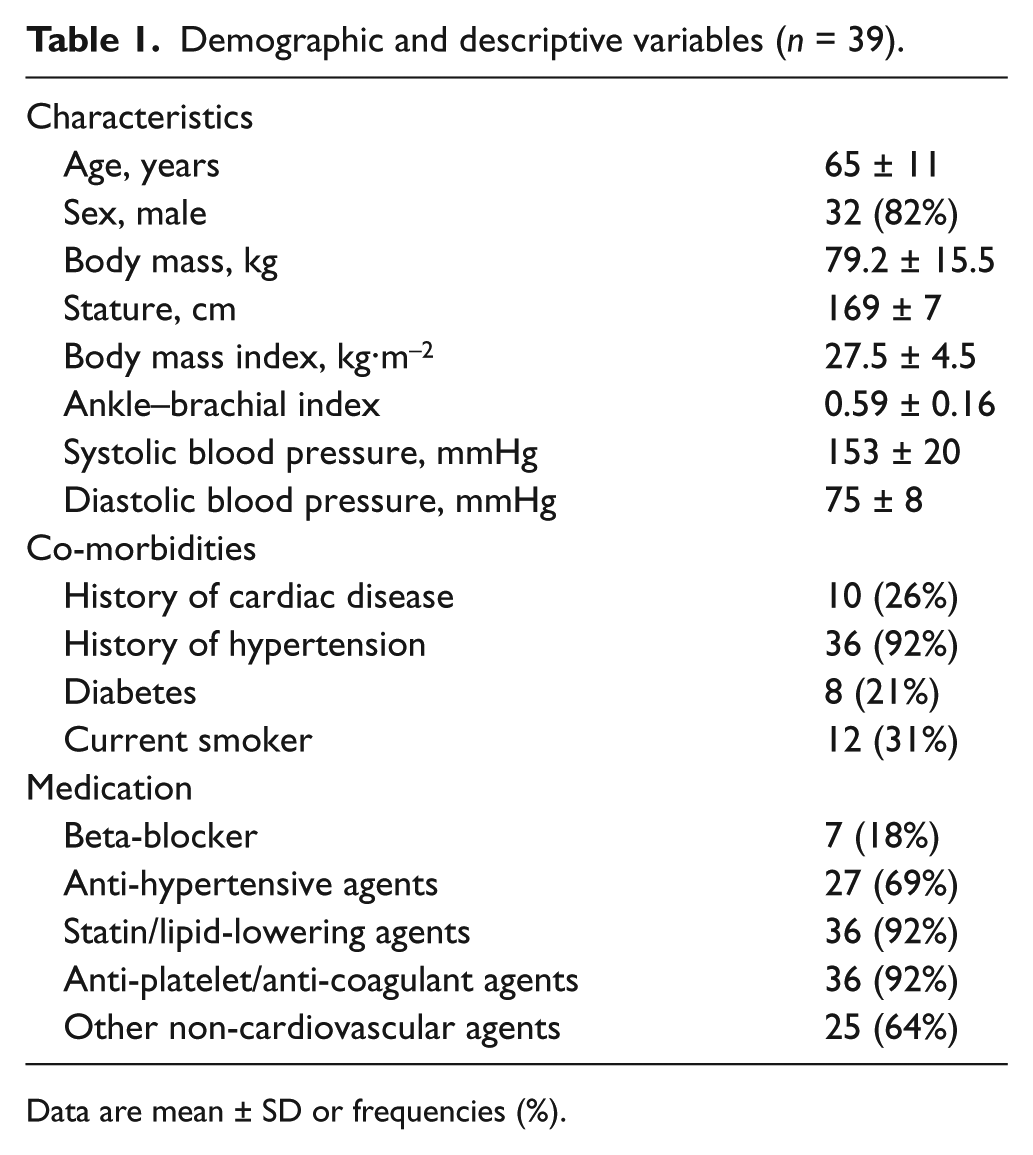
Data are mean ± SD or frequencies (%).
The WELCH questionnaire and treadmill test data were non-normally distributed. The median WELCH score was 24 (9–39). The median initial and maximal claudication walking distance on the treadmill were 68 m (23–113 m) and 412 m (149–675 m), respectively. The mean maximum walking distance for the 6-minute walking test was 381 ± 88 m. There was a moderate positive correlation between the WELCH score and treadmill maximum walking distance (Figure 2A; ρ = 0.59, p < 0.001) and a strong positive correlation between the WELCH score and 6-minute walk test performance (Figure 2B; ρ = 0.82, p < 0.001). In addition, there was a low-to-moderate positive correlation between the WELCH score and the ankle–brachial index (ρ = 0.39, p = 0.014), and a moderate positive correlation between the WELCH score and initial claudication distance on the treadmill (ρ = 0.47, p < 0.003).
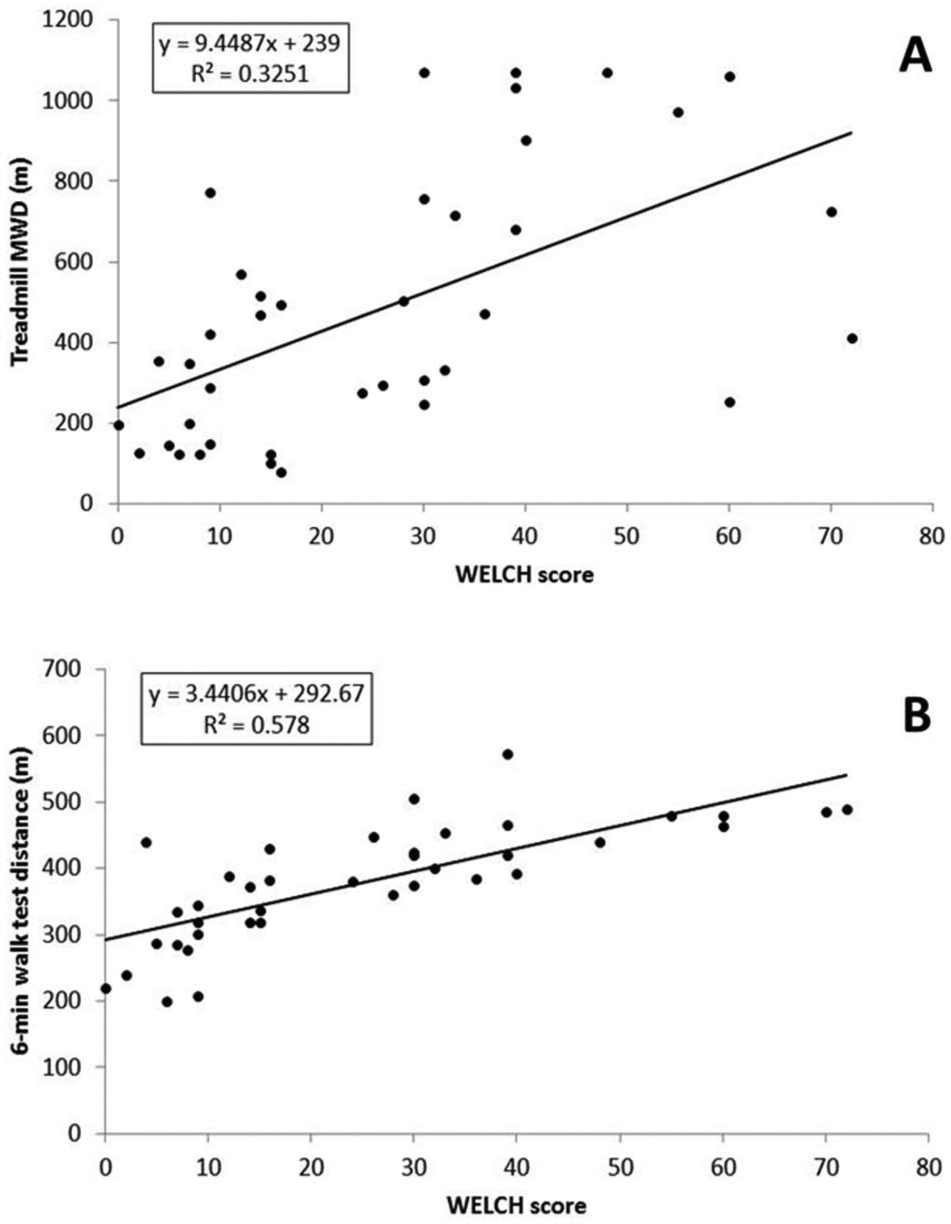
Scatterplots of the WELCH score versus treadmill maximum walking distance (A) and the WELCH score versus 6-minute walk test distance (B).
Discussion
The purpose of this study was to validate an English version of the WELCH questionnaire in an English native population. We observed a moderate positive correlation between the WELCH score and maximum walking distance on the Gardner–Skinner incremental treadmill test, and a strong positive correlation between the WELCH score and walking distance achieved on the 6-minute walk test. The findings suggest that the WELCH questionnaire translated into English demonstrates good validity for the evaluation of walking impairment in patients with intermittent claudication.
The correlation coefficient between the WELCH score and treadmill maximum walking distance (ρ = 0.59) is very similar to that observed in the two initial French validation studies (r = 0.65 and 0.61),6,14 despite them using a different treadmill protocol (constant load 3.2 km/h and 10% gradient for 15 minutes then incremental after minute 15). These values appear greater than those previously reported for the PAVK-86 questionnaire (r = −0.47) 15 and the physical function sub-scale of the SF-36 questionnaire (r = 0.31), 9 and greater or similar to those reported for the overall WIQ score (r = 0.52–0.62).6,16,17 Furthermore, the WELCH has been validated in a heterogeneous group of patients with and without PAD 14 and has been demonstrated to have good reliability and a low rate of errors during self-completion.6,14 Further work is needed to investigate if the WELCH questionnaire is sensitive to changes in walking capacity that might be evoked by various treatments, and we are currently piloting its use in a preliminary trial of a novel home-based exercise programme for patients with intermittent claudication (Clinicaltrials.gov: NCT01776710). Additionally, external validation (i.e. cross-validation of the regression equations shown in Figure 2 on an independent group of similar patients), as has been recently done for the French version of the questionnaire, 14 is still to be done with the present English version.
We correlated the WELCH score against both the Gardner–Skinner incremental treadmill test and the 6-minute corridor walking test because there does not appear to be a clear consensus as to which is the best objective measure of walking capacity in patients with intermittent claudication.4,18,19 Although maximum walking distance on the Gardner–Skinner test has probably been used many more times as a primary outcome in clinical trials, a benefit of the 6-minute walking test is that it more closely correlates with physical activity during daily life. 13 Further, we previously showed that questionnaires correlate better with community-based walking capacity than with treadmill walking performance in individuals with PAD. 16 Interestingly, we observed that the correlation with the WELCH score was higher with the 6-minute walking test data than with treadmill data. Perhaps this is because the WELCH questionnaire and 6-minute walk test are relatively good indicators of community-based walking limitation, whereas treadmill maximum walking distance is not. Although it is recommended to test the walking limitation of patients with PAD on a treadmill, 4 self-report tools may correlate better with community-based walking capacity (assessed using Global Positioning System technology) than with objective measures of walking capacity recorded in a laboratory. 16
This study has some limitations. First, the WELCH questionnaire was compared with walking distances measured in a laboratory and not with the actual walking distance of patients in daily life. Although laboratory procedures such as the Gardner–Skinner treadmill test have face validity for walking capacity, self-report tools appear to correlate better with community-based walking capacity than with laboratory data. 16 Therefore, a more appropriate ‘gold standard’ for determining validity may be a test with a patient walking on the street. However, disease management guidelines recommend the use of treadmill testing, or the 6-minute walk test when a treadmill is not available, for quantifying the magnitude of walking limitation and the response to therapy. 20 We used both of these procedures in the present study. A second limitation is that our results are only generalizable to patients who had not previously undergone objective assessment of walking capacity. We have recently reported that the relationship between subjective (i.e. self-report questionnaires) and objective measures of walking capacity is stronger when patients had previously undergone objective assessment. 16 Our assumption here was that, due to physical inactivity, most patients struggle to rate the difficulty of walks that they do not routinely perform, and that they find it easier to self-report after they have faced some of these tasks at least once. The implication to the present study is that the relationship between the WELCH score and laboratory-measured walking capacity would likely have been stronger if we had included patients who had previously undergone objective walking assessment. Third, the tested WELCH questionnaire did not result from the forward-backward translation method proposed by Beaton et al. 21 However, we are confident that the meaning of each questionnaire item was not altered during the translation process. Finally, a population bias cannot be excluded specifically due to the small number of females in the studied group.
Conclusions
The assessment of walking impairment is an essential outcome measure and a primary endpoint in evaluating the effect of treatment of PAD. The WELCH is a short, easily-scored and valid measure of walking impairment in patients with symptomatic PAD, which compares favourably with other disease-specific questionnaires. We conclude that the English version of the WELCH is a valid instrument for assessing walking impairment in patients with intermittent claudication.
Footnotes
Acknowledgements
We would like to thank the technical support team at the Centre for Sport and Exercise Science, Sheffield Hallam University, for their help with data collection.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.