
Abstract
Peripheral artery disease (PAD) is a highly morbid condition affecting more than 8 million Americans. Frequently, PAD patients are unrecognized and therefore do not receive appropriate therapies. Therefore, new methods to identify PAD have been pursued, but have thus far had only modest success. Here we describe a new approach combining genomic and metabolic information to enhance the diagnosis of PAD. We measured the genotype of the chromosome 9p21 cardiovascular-risk polymorphism rs10757269 as well as the biomarkers C-reactive protein, cystatin C, β2-microglobulin, and plasma glucose in a study population of 393 patients undergoing coronary angiography. The rs10757269 allele was associated with PAD status (ankle–brachial index < 0.9) independent of biomarkers and traditional cardiovascular risk factors (odds ratio=1.92; 95% confidence interval, 1.29–2.85). Importantly, compared to a previously validated risk factor-based PAD prediction model, the addition of biomarkers and rs10757269 significantly and incrementally improved PAD risk prediction as assessed by the net reclassification index (NRI=33.5%; p=0.001) and integrated discrimination improvement (IDI=0.016; p=0.017). In conclusion, a model including a panel of biomarkers, which includes both genomic information (which is reflective of heritable risk) and metabolic information (which integrates environmental exposures), predicts the presence or absence of PAD better than established risk models, suggesting clinical utility for the diagnosis of PAD.
Introduction
Peripheral artery disease (PAD) is a common atherosclerotic disease of the non-coronary, non-cerebral vasculature that affects 8–12 million people in the US.1,2 The public health impact of this disease is significant, owing to its high prevalence in our aging population1,3 and the increased risk for negative clinical outcomes.4–8 Despite this, PAD remains highly underdiagnosed; for instance, over half the patients identified as having PAD in the PARTNERS study were newly diagnosed. 2 These low rates of diagnosis in non-specialty primary care clinics are similarly found among cardiologists, 9 and may be due to the low occurrence of the classic overt symptomology of intermittent claudication (11%) 2 or to practitioners lacking the appropriate equipment, training, or staff.10,11
Because PAD remains highly undiagnosed, 2 PAD patients do not receive optimal treatment and are exposed to higher risks for adverse outcomes.5–8 Compared to patients with coronary artery disease (CAD) or cerebrovascular disease (CVD), patients with PAD actually have higher rates of all-cause mortality and major cardiovascular events. 4 Although there are many similarities between CAD and PAD patients, genetic, metabolomic and epidemiological differences suggest subtle pathophysiological distinctions between these two conditions.12–17 Improved methods of risk classification are needed to enhance proper PAD diagnosis and treatment.
Conventional risk factors for CAD are also associated with PAD and have been the basis of current risk prediction models. 18 While useful for risk stratification, these risk prediction algorithms do not fully capture an individual’s likelihood of having disease. Ideally, risk prediction models would incorporate a range of independent factors, extending beyond just clinical risk factors to include circulating biomarkers reflective of environmental exposures, as well as genetic markers indicative of heritable risk. We have previously used an agnostic, mass spectrometry-based approach to identify proteomic makers, which are dysregulated in those with PAD compared to those without. 11 This panel of biomarkers is correlated with PAD status, regardless of whether or not the patient also has CAD. Despite the clinical value of these biomarkers, we are unable to perfectly identify those at risk and seek new approaches for PAD diagnosis. Human genetics studies have suggested that genetic factors may account for up to half of one’s lifetime risk of cardiovascular disease, 19 and several recent studies report an association between polymorphisms at the non-coding chromosome 9p21 locus and cardiovascular diseases.20 –22 The aims of this study were to develop a new approach to identify subjects with PAD that combines classical risk factors with circulating biomarkers and genomic factors, while also determining if this risk prediction technique improves clinically relevant discriminatory indices, such as the integrated discrimination index and net reclassification index.
Methods
Study population
The Genetic Determinants of Peripheral Arterial Disease (GenePAD) study consists of individuals who underwent an elective coronary angiogram for angina, shortness of breath or an abnormal stress test at Stanford University or Mount Sinai Medical Centers between 1 January 2004 and 1 March 2008.9,23 As previously described, 24 a subgroup of individuals was selected to characterize the role of biomarkers in PAD. The GenePAD study was approved by the Stanford University and Mount Sinai School of Medicine Committees for the Protection of Human Subjects. All participants provided informed consent.
Inclusion criteria
Individuals were eligible for inclusion in the study sample if complete data were available on rs10757269, the biomarkers β2-microglobulin, cystatin C, C-reactive protein, and plasma glucose, in addition to age, sex, race, smoking history, body mass index (BMI), systolic blood pressure (SBP), use of lipid-lowering and anti-hypertensive medications, use of insulin or oral hypoglycemic agents, total cholesterol, high-density lipoprotein (HDL) cholesterol, ankle–brachial index (ABI) and history of CAD, CVD, and congestive heart failure (CHF). Additionally, we only included Caucasian, African-American and Asian-American individuals as the 9p21 locus has previously been shown to be potentially predictive of cardiovascular events in these racial-ethnic groups.25–28 Using these criteria, 393 subjects were identified. The prevalence of PAD was similar among those included or excluded from the study for reasons of ethnicity (p=0.727) or incomplete data (p=0.292).
Covariates
Prior to the coronary angiogram, posterior tibial, dorsalis pedis, and brachial artery systolic pressures were measured using a 5 MHz Doppler ultrasound. The ABI for each patient was calculated by dividing the higher ankle pressure of each leg over the higher of the left or right brachial pressures. Each patient was then classified as having PAD by an ABI of < 0.9 in either leg or not having PAD with an ABI ≥ 0.9 in both legs. There were no participants with an ABI > 1.4.
Detailed information on all included covariates was obtained by a trained nurse or clinical research assistant at enrollment. Age, sex, race, smoking history and history of CVD, CHF and CAD were acquired by self-report and BMI and SBP were measured. The use of lipid-lowering and anti-hypertensive medications was evaluated by direct medication inventory. Diabetes status was classified as self-reported use of insulin or oral hypoglycemic agents. Total and HDL cholesterol levels were measured at the time of coronary angiography. The biomarkers were measured with standard nephelometry using the BN II nephelometer system (Dade Behring Inc.) for fasting blood samples collected while the patient was being prepped for scheduled coronary angiography. Patients completed the Walking Impairment Questionnaire (WIQ) at enrollment with a trained nurse or clinical research assistant as previously described in the GenePAD study. 29 The WIQ consists of three categories assessing subjective walking distance, stair-climbing and walking speed ability and has been previously validated as an objective measure of walking distance.30,31
Genotyping
The rs10757269 single nucleotide polymorphism (SNP) on the chromosome 9p21 locus was genotyped using TaqMan® and assays pre-designed by Applied Biosystems.
Statistical methods
The biomarkers β2-microglobulin, cystatin C, C-reactive protein, and plasma glucose were log-transformed to achieve a normal distribution. The association of rs10757269 with PAD was tested using a multivariable logistic regression analysis and for association with ABI and with the WIQ category scores using a multivariable linear regression analysis. The fully adjusted model included β2-microglobulin, cystatin C, C-reactive protein, plasma glucose, age, sex, race, smoking history, BMI, hypertension stage, use of lipid-lowering and anti-hypertensive medications, diabetes status, total cholesterol and HDL cholesterol. All covariates were continuous, except race (categorical), smoking, use or non-use of lipid-lowering and anti-hypertensive medications and diabetes status (dichotomous).
The integrated discrimination improvement (IDI) and the net reclassification improvement (NRI) were evaluated to determine whether the addition of rs10757269 to a baseline model significantly improved risk discrimination and reclassification, respectively. 32 In this analysis, we used a baseline model previously validated for PAD that included the risk factors age, sex, race, smoking history, BMI, hypertension stage, diabetes status and history of CVD, CHF, and CAD. 18
The IDI compares two models according to the average difference in predicted risk between those who have the outcome and those who do not. If the new model assigns a higher risk to those who have PAD and a lower risk to those who do not, as compared to the baseline model, the IDI will be greater than zero. Therefore, the IDI can be interpreted as the average net improvement in the predicted risk of PAD in the model with rs10757269 compared to the baseline model.
The category-free NRI was used in this study, as a priori risk categories for PAD do not exist. This NRI quantifies the degree of correct upward or downward absolute risk reclassification with the addition of rs10757269 to the baseline model. Furthermore, the NRI was calculated separately among individuals with and without PAD.
Tests were considered significant if the two-sided p-value was < 0.05. All analyses were performed using Stata version 12.0 (StataCorp, College Station, TX, USA). Study data were collected and managed using REDCap electronic data capture tools hosted at Stanford University. 33
Results
The baseline characteristics of our study population are presented in Table 1. Genotype frequencies are presented in the Appendix.
Baseline study population characteristics (n=393).
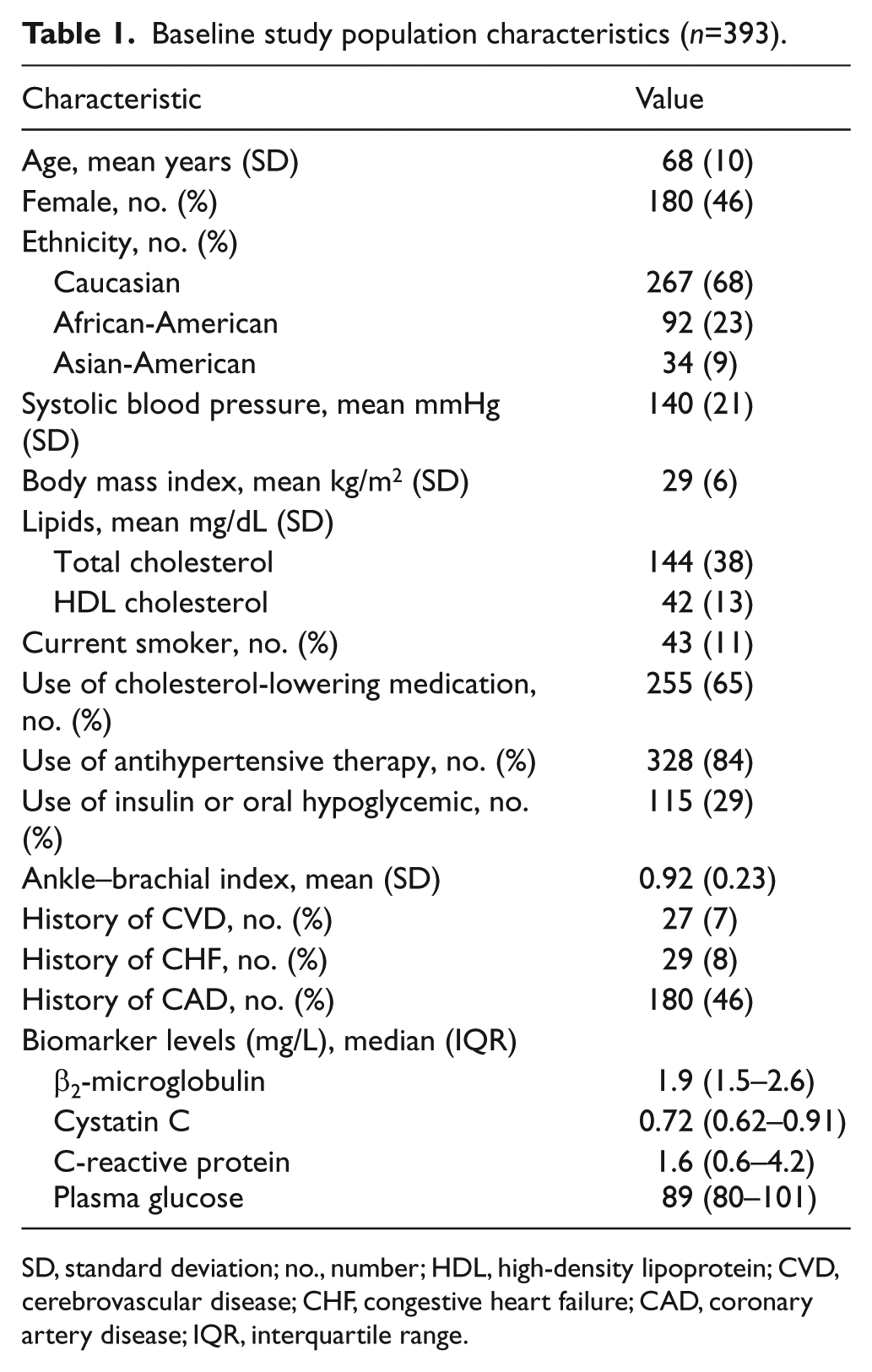
SD, standard deviation; no., number; HDL, high-density lipoprotein; CVD, cerebrovascular disease; CHF, congestive heart failure; CAD, coronary artery disease; IQR, interquartile range.
We found that the G-allele of rs10757269 was associated with a significantly increased risk of PAD (Table 2). A statistically significant 80% increased risk of PAD per rs10757269 risk-allele remained even when accounting for risk factors and biomarkers previously shown to predict PAD. Accordingly, rs10757269 was also associated with a significantly decreased ABI per rs10757269 PAD risk-increasing allele.
Association of rs10757269 with peripheral artery disease (PAD) and the ankle–brachial index (ABI).
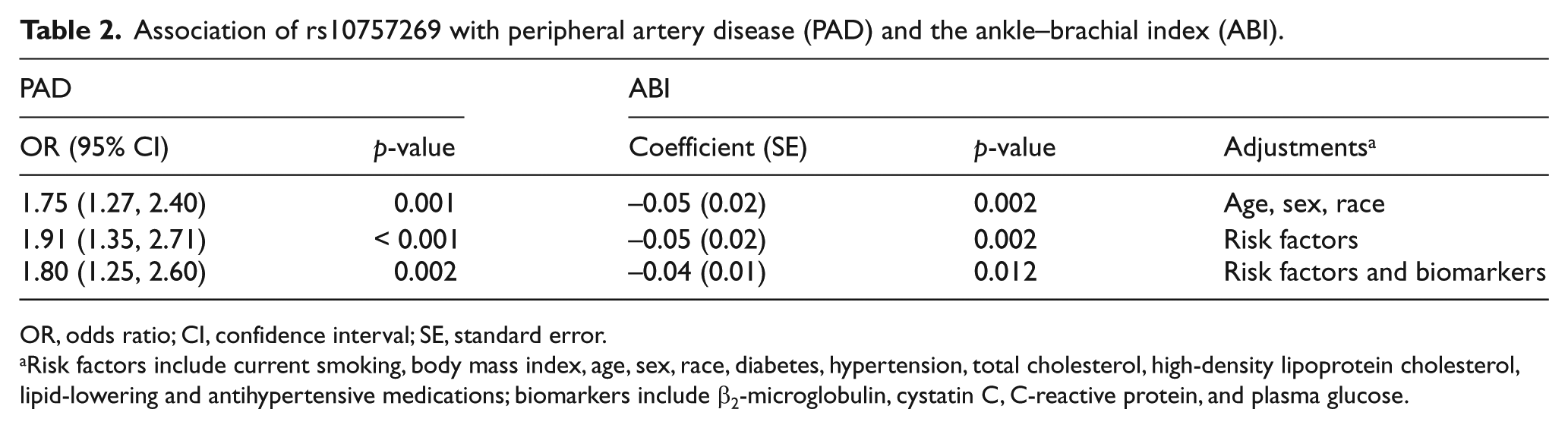
OR, odds ratio; CI, confidence interval; SE, standard error.
Risk factors include current smoking, body mass index, age, sex, race, diabetes, hypertension, total cholesterol, high-density lipoprotein cholesterol, lipid-lowering and antihypertensive medications; biomarkers include β2-microglobulin, cystatin C, C-reactive protein, and plasma glucose.
Additionally, the rs10757269 G-allele was associated with worse WIQ distance, speed and stair-climbing scores (Table 3). The G-allele was found to predict a statistically significant reduction in the WIQ walking distance and stair-climbing scores even when adjusting for a wide range of PAD risk factors.
Association of rs0757269 with the Walking Impairment Questionnaire category scores.
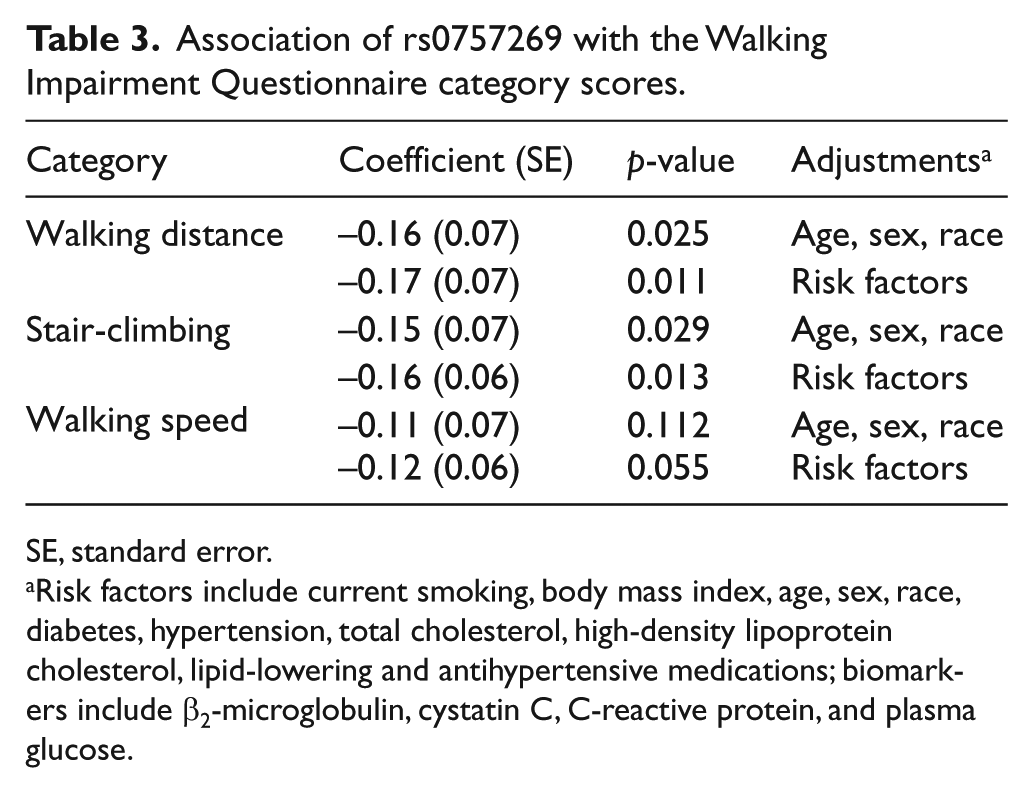
SE, standard error.
Risk factors include current smoking, body mass index, age, sex, race, diabetes, hypertension, total cholesterol, high-density lipoprotein cholesterol, lipid-lowering and antihypertensive medications; biomarkers include β2-microglobulin, cystatin C, C-reactive protein, and plasma glucose.
As rs10757269 was independently associated with PAD, we examined whether the addition of rs10757269 to a validated PAD risk factors model could improve risk discrimination and reclassification (Table 4). The addition of rs10757269 to the established risk factors model significantly improved the IDI. Similarly, a significant improvement in the IDI was seen with the addition of the biomarkers β2-microglobulin, cystatin C, C-reactive protein, and plasma glucose, which have previously been shown to predict PAD. Interestingly, a significant improvement in model risk discrimination was still seen with the addition of rs10757269 to a baseline model including both established risk factors and biomarkers (IDI=0.016; p=0.017).
The IDI and NRI for the addition of rs10757269 and biomarkers to a baseline model.
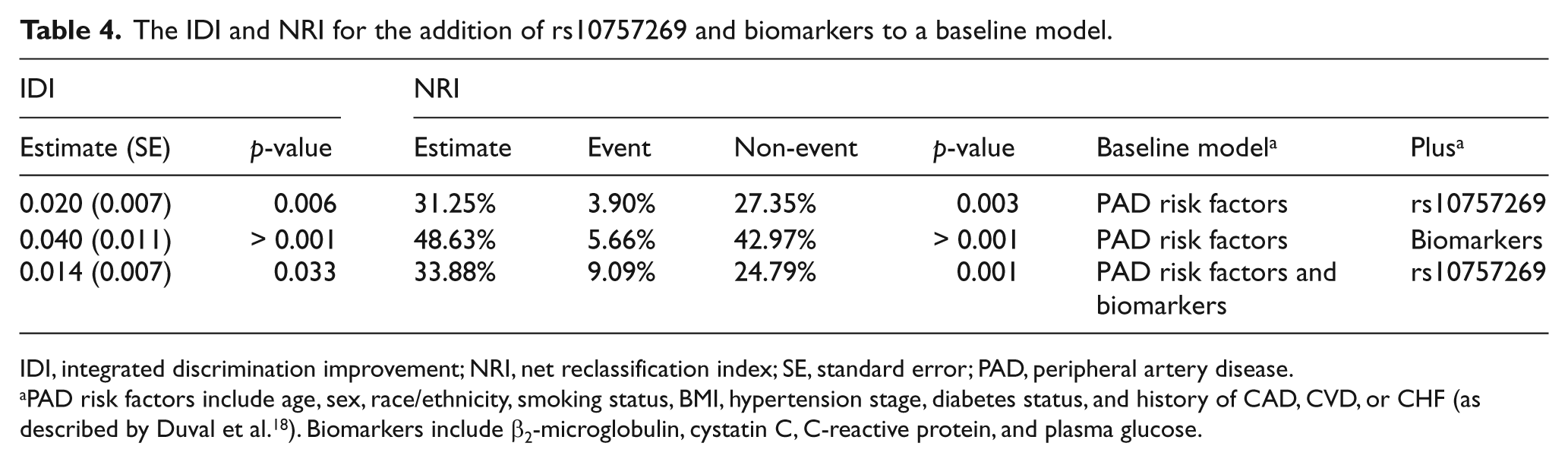
IDI, integrated discrimination improvement; NRI, net reclassification index; SE, standard error; PAD, peripheral artery disease.
PAD risk factors include age, sex, race/ethnicity, smoking status, BMI, hypertension stage, diabetes status, and history of CAD, CVD, or CHF (as described by Duval et al. 18 ). Biomarkers include β2-microglobulin, cystatin C, C-reactive protein, and plasma glucose.
Finally, we evaluated whether rs10757269 could improve PAD risk reclassification using the category-free NRI. We observed that both rs10757269 and the biomarkers were separately able to improve risk reclassification when added to the baseline model of established PAD risk factors. Importantly, rs10757269 was able to improve model risk reclassification even when added to a baseline model consisting of established risk factors and biomarkers (NRI=33.5%; p=0.001).
Discussion
New methods to identify subjects with PAD are needed, as patients with this disease remain both underdiagnosed and undertreated.2,34 The purpose of this study was to determine if we could integrate a subject’s genomic and metabolic information into currently available PAD risk prediction models, and improve our capacity to identify those at risk. The main findings of this study were that (1) both the 9p21 cardiovascular-risk allele and a panel of circulating biomarkers are associated with the presence of PAD as well as with walking ability, (2) these associations are independent of traditional cardiovascular risk factors, and (3) a combined model, which simultaneously measures a subject’s genotype, clinical data, and biomarker status, provides superior risk discrimination and net reclassification capacity over established models, and may therefore have clinical utility.
Recently, Duval et al. developed a nomogram that assigns point values to traditional risk factors including age, sex, race, BMI, current smoking status, degree of hypertension, and presence or absence of diabetes, CAD, CVD, or CHF to create an evidence-based PAD risk score. 18 Although easy to administer, this score lacks a clearly defined threshold for PAD that exhibits both high sensitivity and specificity, suggesting the need for more discriminating risk factors. Moreover, it is now appreciated that traditional risk factors account for only half of one’s lifetime risk of cardiovascular disease, 35 suggesting that the balance is accounted for by genetic and environmental factors, which may not be captured in classical risk factor-based models. We therefore have pursued circulating biomarkers and genetic risk factors as an approach to quantify this ‘unmeasured risk’. Our group has previously identified a panel of agnostically identified biomarkers that is associated with PAD, and which improves mortality risk prediction.11,24 Genetic risk factors for PAD have been more difficult to ascertain due to the limitations of candidate gene studies and the modest effect size of individual gene contributions to polygenic atherosclerotic disease.16,36,37 A meta-analysis of genome-wide association studies, on the other hand, has successfully confirmed an association between SNPs at the non-coding 9p21 chromosome region and low ABI, 28 suggesting the 9p21 genotype may be useful to identify at-risk populations.
The results of the present study confirm that previously identified biomarkers (β2-microglobulin, cystatin C, C-reactive protein, and plasma glucose) and genetic markers (SNPs at the 9p21 locus) are independently associated with PAD, and, more importantly, provide additive improvements in risk discrimination and risk reclassification. The independence of the biomarkers and the 9p21 SNP likely reflect their correlation with distinct pathways related to atherogenesis in the periphery. Circulating biomarkers provide a ‘readout’ of activated disease-related metabolic pathways, and incorporate a subject’s recent exposure to environmental factors, which may alter the epigenetic, transcriptional or translational regulation of a given pathway. The panel employed in this study has relevance to PAD, as it may simultaneously contribute information about the subject’s current level of peripheral ischemia-reperfusion injury, renal dysfunction and vascular inflammation. 11 The 9p21 status, on the other hand, is a genetic risk factor that signifies a potentially fixed, lifelong exposure. The rs10757269 SNP is not only associated with ABI and the presence of PAD, but also with WIQ scores, which signify a patient’s degree of functional impairment. We have previously demonstrated that these scores predict mortality in patients, regardless of PAD status. SNPs at the 9p21 locus correlate with disease independent of traditional risk factors, and represent a novel aspect of the vascular biology responsible for disease initiation or progression. Recent work by our laboratory suggests that variation in the 9p21 locus may accelerate smooth muscle cell apoptosis and alter the integrity of the developing neointimal lesion, perhaps explaining how it promotes risk regardless of whether a patient also happens to be hypertensive or dyslipidemic. 38
The use of a high-risk cohort in this study may limit the application of these findings to the general population. Despite being a multi-ethnic, multi-center study, certain race subgroups were excluded due to lack of informative data regarding architecture of the risk haplotype across racial groups. Accordingly, future analyses should continue to explore racial ethnic differences in PAD risk. Our model predicts baseline PAD; however, we do not yet know if it can predict future cardiovascular events. The clinical impact of our risk prediction model should be confirmed with randomized controlled trials. While our results do show improved risk prediction, future studies should also consider the cost effectiveness of our test in comparison to gold standard office-based tests, such as the ABI. Despite these limitations, our results expand our knowledge base regarding PAD and vascular biology. We conclude that this novel risk prediction model, which is the first to integrate genomic and metabolic information related to PAD, will enhance our capacity to identify a disease which is highly prevalent, significantly underdiagnosed, and now responsible for every fifth dollar spent on inpatient cardiovascular care in the United States. 39
Footnotes
Appendix
Genotype distribution of rs10757269 by race.
| GG | AG | AA | |
|---|---|---|---|
| Caucasian | 83 (0.31) | 129 (0.48) | 55 (0.21) |
| African-American | 63 (0.68) | 23 (0.25) | 6 (0.07) |
| Asian-American | 19 (0.56) | 14 (0.41) | 1 (0.03) |
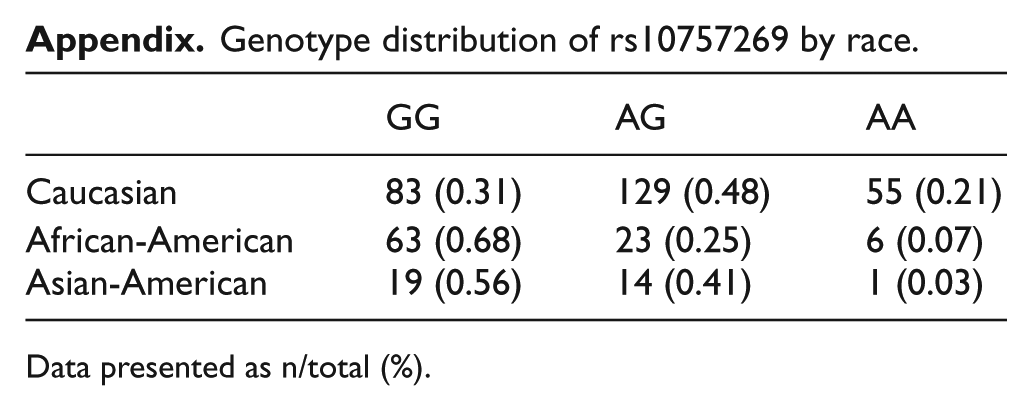
Data presented as n/total (%).
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the National Institutes of Health [grant numbers T32HL098049 (KD), K08HL10360501A1 (NL) and R01HL103635 (TQ)] and the LeDucq Foundation (TQ).