
Abstract
To determine the role of endothelial progenitor cells (EPCs) in the pathogenesis of thromboangiitis obliterans (TAO), EPC numbers and colony-forming units, migratory function and tubular structure formation in vitro were compared between 13 young male TAO patients and two age-matched healthy control groups: 11 smokers and 12 non-smokers. TAO patients had significantly lower numbers of EPCs and EPC colonies compared to both non-smokers [190 (97.0–229) vs 528 (380–556), p < 0.001 for EPCs and 0.80 (0.53–1.00) vs 2.80 (2.08–4.00) per mm2, p = 0.001 for EPC colonies] and smokers [190 (97.0–229) vs 272 (229–326), p = 0.012 for EPCs and 0.80 (0.53–1.00) vs 2.80 (1.80–3.93) per mm2, p = 0.001 for EPC colonies]. However, there were no significant differences in migratory function or tube formation between the three groups. These results suggest that TAO patients have an intrinsic decrease in EPCs not entirely associated with smoking, which may be the cause of endothelial dysfunction seen in TAO patients leading to the development of this disease at early ages.
Keywords
Introduction
Thromboangiitis obliterans (TAO), also known as Buerger’s disease, is a non-atherosclerotic segmental inflammatory occlusive disease affecting small and medium-sized vessels in the extremities.1,2 TAO is rare in North America and Europe but relatively more common in Asia and the Middle East. 3 Since its first description by Von Winiwarter in 1879, 4 many attempts have been made to understand its pathogenesis, yet it remains an unknown disease with poor treatment results. The inflammatory nature of the disease was first described by Buerger in 1908, 5 and many studies have shown that inflammatory cells are involved in the arterial occlusions, suggesting the presence of acute intimal injury in these vessels.6,7 In fact, we previously demonstrated that T-cell-mediated injury was deeply involved in the pathogenesis of TAO based on pathobiological studies from arterial biopsies. 7 In healthy individuals, inflammatory injury to vessels is counteracted by reparative mechanisms to achieve vascular homeostasis. A group of cells known as endothelial progenitor cells (EPCs) was identified as having reparative properties in injured endothelium. EPCs were first described by Asahara as a subset of CD34 hematopoietic stem cells, which differentiated into endothelial lineage cells expressing various endothelial marker proteins. 8 These cells were found to be circulating in the peripheral blood and adhered to vessel walls at sites of ischemia, contributing to neovascularization and re-endothelialization of the injured endothelium.8–10
Several studies have shown that a decrease in EPCs was significantly related with cardiovascular risk,11,12 including patients with atherosclerosis obliterans 13 and chronic renal failure. 14 Smoking was also found to inhibit the recruitment of EPCs from the bone marrow. 15 A few studies have also investigated the role of EPCs in TAO in terms of numbers and function, but the results reported were somewhat contradictory.16–18 We hypothesized that the pathogenesis of TAO involves an impairment in the repair mechanisms of inflammation-induced intimal injury and that a decrease in EPC numbers/function may explain the development of this disease at early ages. Therefore, we designed this study with a homogeneous population of young patients to define the role of EPCs in TAO.
Materials and methods
Study subjects
Under the approval of the Institutional Review Board, a total of 36 patients were enrolled in this study between 2004 and 2007. The study individuals were comprised of 13 TAO patients, 11 age-matched smokers and 12 age-matched non-smokers. TAO patients were diagnosed at our hospital using the diagnostic criteria proposed by Olin (Table 1). 2 All individuals were males and otherwise healthy, without other cardiovascular comorbidities. None of them had undergone surgical intervention or medical management at the time of enrollment. The control groups were all healthy individuals without any history of known diseases, including cardiovascular or cerebrovascular disease, diabetes mellitus and dyslipidemia. None of the study subjects in the three groups were on medications, including statins. Both TAO patients and smokers were actively smoking at the time of enrollment, while non-smokers denied any history of smoking during their entire life. Blood samples were drawn from the study subjects early in the morning after at least 8 hours of starving the night before. Patients had a 30-minute rest before blood sampling, after which a total of 50 mL of blood was drawn from the arm vein and immediately sent to the laboratory for EPC isolation.
Olin criteria for thromboangiitis obliterans and frequency of each component in the TAO group.
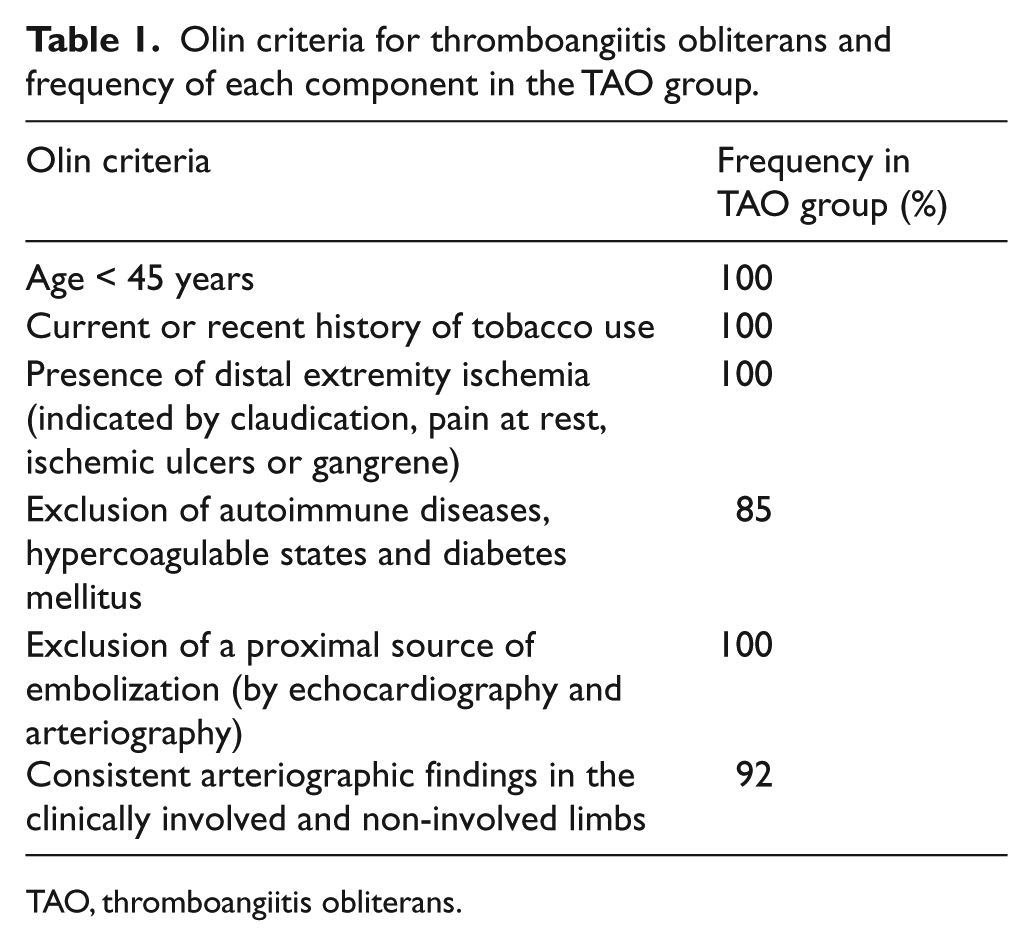
TAO, thromboangiitis obliterans.
EPC isolation
The methodology used for the culture, isolation and identification of EPCs was similar to a previous study performed on chronic renal failure (CRF) patients. 14 EPCs were obtained by isolating mononuclear cells from the peripheral blood of the subjects using a density gradient method with Ficoll-Plaque PLUS (Amersham, Buckinghamshire, UK). The initial seeding density was standardized at 4 × 106 cells per well and these mononuclear cells were suspended in EGM-2 medium containing several growth factors (VEGF-A, EGF, FGF-2, IGF-1 and ascorbic acid). After 3 days of culture, non-adherent cells were removed, the medium was changed and the culture was maintained through day 7. The number of EPCs and EPC colonies were counted and the cells were assayed or harvested for further study.
EPC identification and count
At day 7, adherent cells were incubated with 1,1’-dioctadecyl-3,3,3’,3’-tetramethylindocarbocyanine perchlorate (DiI)-labeled acetylated low-density lipoprotein (LDL) (Molecular Probes, Eugene, OR, USA) at 37°C for 3 hours and with fluorescein-isothiocyanate (FITC)-conjugated Ulex europaeus agglutinin (UEA)-1 lectin (10 µg/ml; Sigma, St Louis, MO, USA) for 4 hours. Cells exhibiting double fluorescence under inverted fluorescence microscopy were identified as EPCs.19,20 The phenotypic characteristics of these cells were investigated with fluorescence-activated cell sorter (FACS) analysis by incubation of the cells with primary antibodies von Willebrand factor (vWF; BD Pharmigen, San Diego, CA, USA), VE-cadherin (BD Pharmigen), CD34 (Abcam, Cambridge, UK) and CD133 (Abcam) and, subsequently, with their respective FITC and rhodamine-linked secondary monoclonal antibodies. Peripheral blood mononuclear cells served as controls.
EPC numbers and colonies were determined by counting 12 random high-power (×100) microscope fields per subject and were expressed as cells or colonies per mm2. Spindle-shaped cells and colonies consisting of multiple thin, flat cells emanating from a central cluster of round cells were counted.
Matrigel tube formation assay
A Matrigel tube formation assay was performed to assess the ability of EPCs to incorporate into endothelial cell vascular structures, an important process in angiogenesis. 9 Matrigel (Becton Dickinson, San Jose, CA, USA) was spread onto 4-well chamber slides (Nalge Nunc, Rochester, NY, USA). EPCs were marked with DiI to distinguish them from human umbilical vein endothelial cells (HUVECs). DiI-labeled EPCs (1 × 105) and HUVECs (4 × 104) were plated together and incubated at 37°C for 24 hours with EGM-2. The areas and line lengths of the circles formed by cells were calculated with Image-Pro Plus 4.5 (Media Cybermetics Inc., Bethesda, MD, USA) from four random high-power (×100) microscope fields per well.
Migration assay (Boyden chamber assay)
A modified Boyden chamber assay was used to examine EPC migratory function, an essential process during angiogenesis. A 24-well Transwell apparatus (Costar, Corning, NY, USA) was used; each well contained a 6.5 mm polycarbonate membrane with 8 µm pores coated with type I collagen (Sigma, St Louis, MO, USA). EPCs (4 × 104) were placed on the membrane, and the chamber was immersed in a 24-well plate filled with VEGF-supplemented medium. After incubation for 24 hours, the membrane was washed briefly with phosphate-buffered saline (PBS) and the upper side of the membrane was wiped gently with a cotton ball. The membrane was removed and stained using Giemsa solution. The magnitude of EPC migration was evaluated by counting the number of migrated cells in four random high-power (×100) microscope fields.
Immunohistochemical analysis
A subgroup analysis was done in four TAO patients who subsequently underwent surgical bypass during the study period. Arterial tissues obtained during surgery were sent for pathologic confirmation and immunohistochemical staining was performed. Inducible nitric oxide synthase (iNOS) staining was performed to determine the inflammatory nature of endothelial damage, and terminal deoxynucleotidyl transferase-mediated dUTP-digoxigenin nick-end-label (TUNEL) staining was done to detect apoptotic endothelial cells.
Arterial tissues were deparaffinized by immersion in xylene twice for 5 minutes and in a graded series of ethanol (100%, 95%, 75%, 0%) for 3 minutes each. The sections were washed in phosphate-buffered saline (PBS) containing 0.5% H2O2 to inactivate endogenous peroxidases and incubated with 20 µg/ml of proteinase K in PBS. For iNOS staining, the tissues were incubated with iNOS antibodies (Affinity Bioreagents Inc., Golden, CO, USA) in PBS for 2 hours. The tissues were then incubated with an appropriate secondary antibody for 20 minutes and treated with peroxidase-labeled avidin-biotin complex for 30 minutes. 3,3’-Diaminobenzidine was used as a chromagen for visualization. For TUNEL staining, an ApoTag in situ apoptosis detection kit (Oncor Inc., Gaitesburg, MD, USA) was used to determine the DNA fragments in the tissue sections. The labeling procedure was carried out following the manufacturer’s instructions and counterstaining was performed by immersion in 0.5% methyl green in 0.1 mol/L sodium acetate solution (pH 4.0) for 5 minutes at room temperature.
Statistical analysis
All data are presented as medians and interquartile ranges. Statistical analysis for the three groups was performed using a Kruskal–Wallis test, and pairwise comparisons between each group were performed using the Mann–Whitney U-test. SPSS release 18.0 (SPSS Inc., Chicago, IL, USA) was used for analysis, and differences were considered statistically significant when p < 0.017 (for adjustment of type I error).
Results
Patient characteristics
The baseline clinical characteristics of the study subjects are summarized in Table 2. All patients were males and the median age was 21.0 (20.3–22.0), 22.0 (21.0–23.0) and 25.0 (21.0–32.5) years for the non-smoker, smoker and TAO groups, respectively. Systolic blood pressure, fasting blood sugar and total cholesterol levels were within the normal range, and there were no significant differences in systolic blood pressure, body mass index (BMI), white blood cell (WBC) count, fasting blood sugar level, total cholesterol level and C-reactive protein (CRP) between the three groups. There were no differences in amount or period of smoking (measured in pack years) between TAO patients and smokers.
Clinical characteristics of the study subjects.
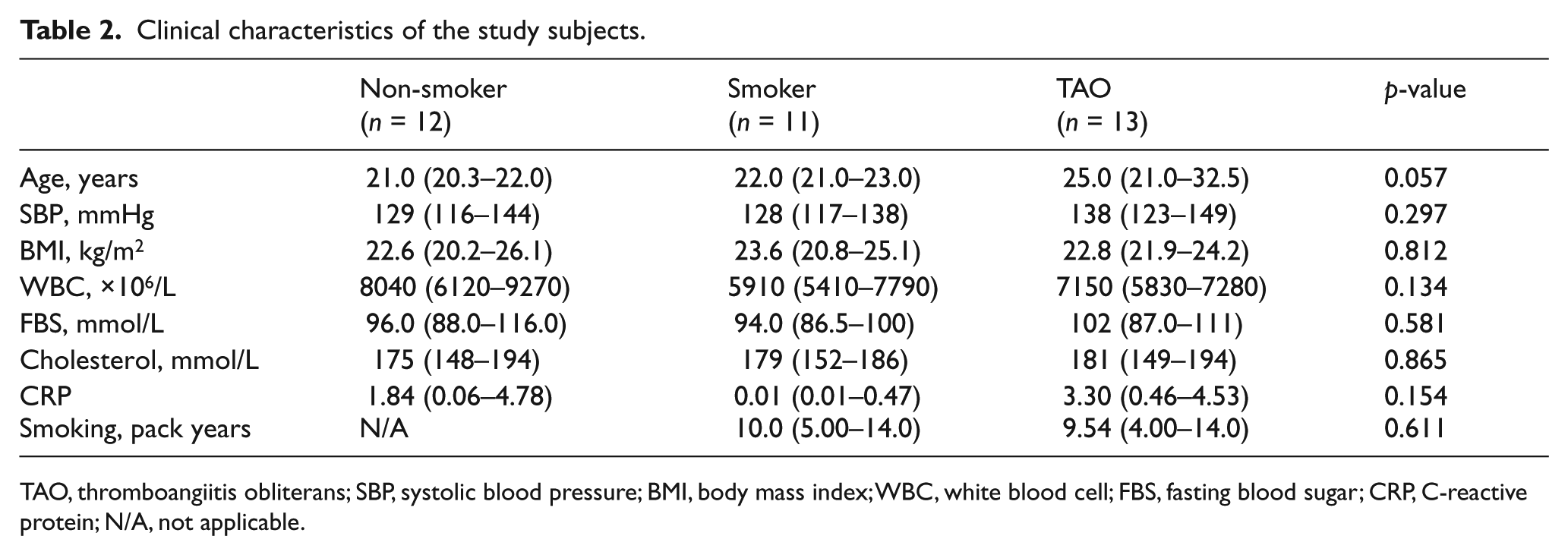
TAO, thromboangiitis obliterans; SBP, systolic blood pressure; BMI, body mass index; WBC, white blood cell; FBS, fasting blood sugar; CRP, C-reactive protein; N/A, not applicable.
EPC identification
Cultured mononuclear cells isolated from peripheral blood showed spindle-shaped cells characteristic of early EPCs, in contrast to late EPCs, which are more round and with a pebble-shaped appearance (Figure 1A). The early EPCs used in our study showed uptake of both acetylated LDL (red) and UEA-1 lectin (green), as shown by the merging (yellow) of the two markers (Figure 1B). Phenotypic analysis of these cells using FACS analysis showed positive phenotypes for vWF and VE cadherin (51% and 47%, respectively), while CD34 and CD133 showed negative results. These results demonstrate that EPCs were successfully isolated and that culture-expanded EPCs maintained their phenotypes.
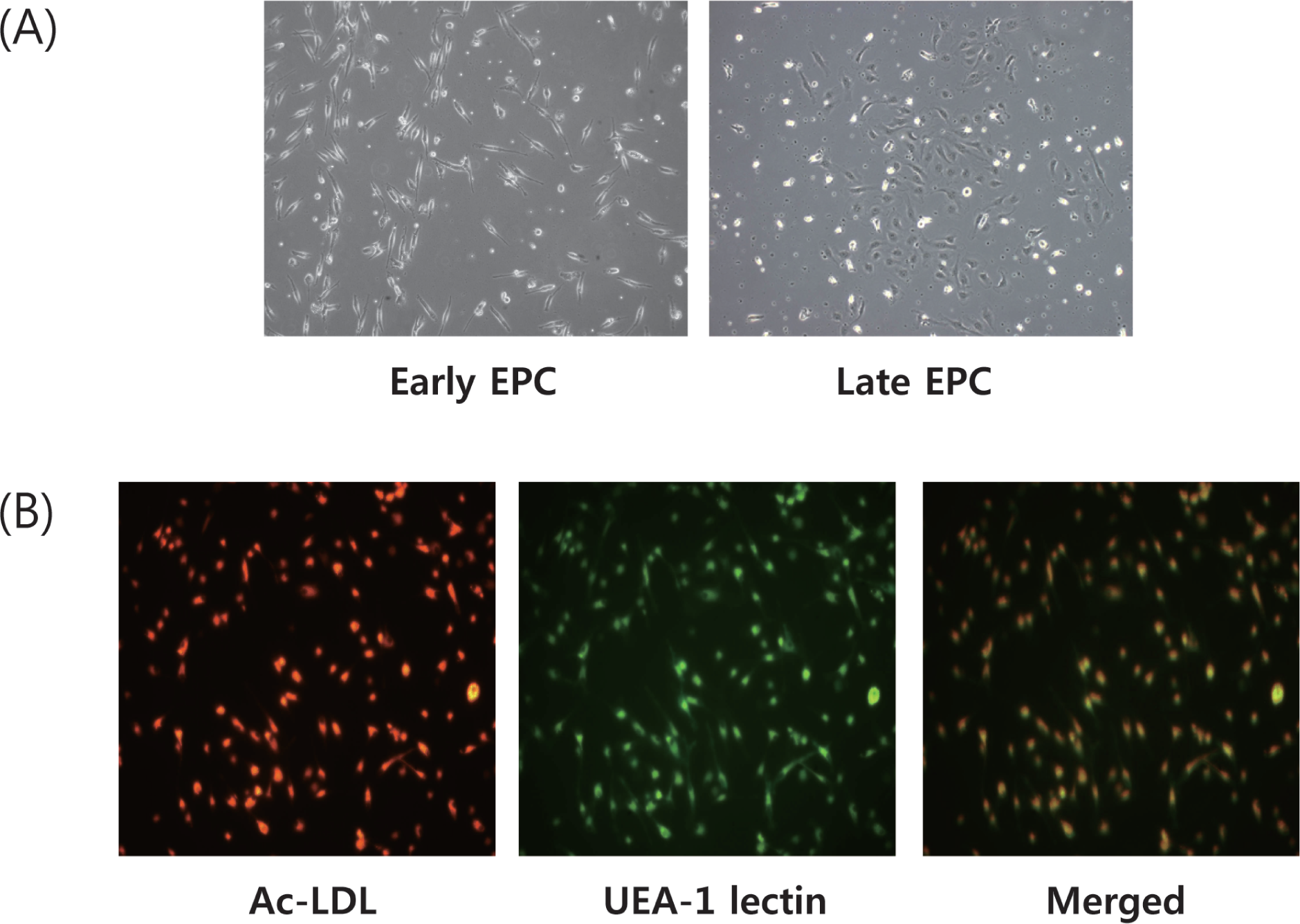
Endothelial progenitor cell (EPC) identification. (A) EPCs used in our study were early EPCs, which have characteristic spindle-shaped morphology. When these cells were cultured for longer periods, morphological changes to round, pebble-shaped cells characteristic of late EPCs were visible. (B) Early EPCs show uptake of acetylated LDL and UEA-1 lectin, and cells showing positive expression of both markers (merged yellow color) were identified as EPCs.
EPC count
The number of EPCs and EPC colonies formed were counted for the three groups. Significantly fewer EPCs were found in TAO individuals compared to non-smokers [190 (97.0–229) vs 528 (380–556) per mm2, p < 0.001] and smokers [190 (97.0–229) vs 272 (229–326) per mm2, p = 0.012] (Figure 2A). Smokers also had fewer EPCs circulating in their blood compared to non-smokers [272 (229–326) vs 528 (380–556) per mm2, p = 0.002].
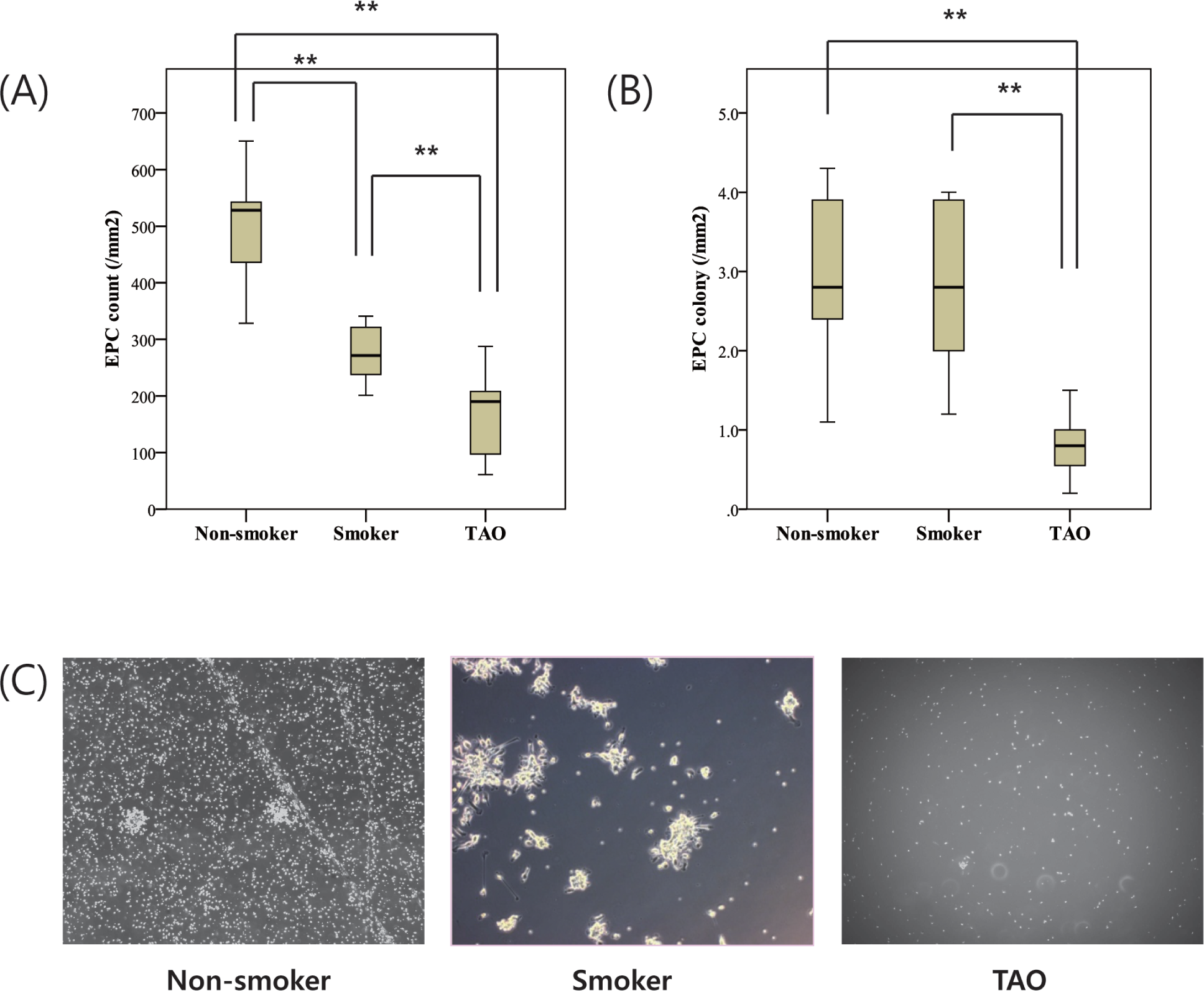
Endothelial progenitor cell (EPC) numbers and colonies between non-smokers, smokers and TAO patients. (A) TAO patients had significantly reduced EPC numbers compared to non-smokers and smokers. Smokers also had significantly reduced EPC numbers compared to non-smokers. (B) TAO had significantly reduced EPC colonies compared to non-smokers and smokers. (C) Microscopic images showing characteristic EPCs and colonies for non-smokers, smokers and TAO patients (40× magnification). Asterisks (**) represent statistical significance (p < 0.017).
The number of EPC colonies, which is considered to be a more sensitive parameter because cells are in a state of proliferation and can be used to determine their growth potential, were also significantly reduced in TAO individuals compared to non-smokers [0.80 (0.53–1.00) vs 2.80 (2.08–4.00) per mm2, p = 0.001] and smokers [0.80 (0.53–1.00) vs 2.80 (1.80–3.93) per mm2, p = 0.001] (Figures 2B and 2C). EPC colony numbers between smokers and non-smokers were not significantly different.
EPC tube formation and migration
EPC tube formation and migratory functions, which are believed to be important in angiogenesis, were assessed for the three groups. Tube formation assessed by Matrigel showed that EPCs in the TAO group had no significant difference compared to both smokers and non-smokers, while only smokers showed a significantly lower tube formation rate compared to non-smokers (Figures 3A and 3C). EPC migration showed no significant differences between the three groups (Figures 3B and 3D). Overall, there was no consistent correlation in EPC tube formation and migration between the three groups.
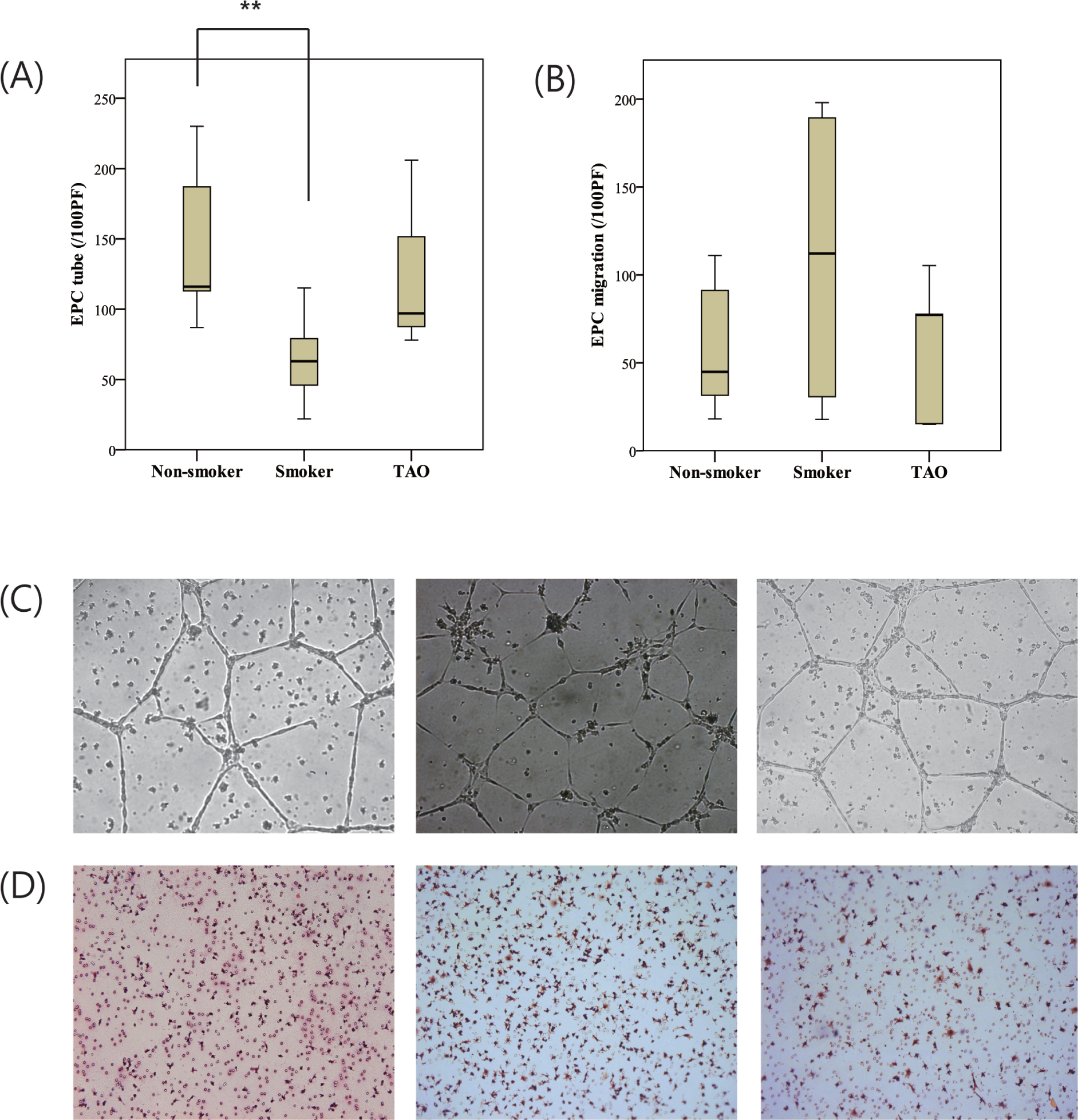
Endothelial progenitor cell (EPC) function between non-smokers, smokers and TAO patients. (A) EPC tube formation assay showed significantly lower tube formation in smokers compared to non-smokers, but there was no difference compared to TAO patients. (B) EPC migratory function assay showed no significant difference in migration between the three groups. (C) Representative images of EPC tube formation for non-smokers, smokers and TAO patients, respectively (100× magnification). (D) Representative images of EPC migration for non-smokers, smokers and TAO patients, respectively (100× magnification). Asterisks (**) represent statistical significance (p < 0.017).
Immunohistochemical analysis
Arterial tissues obtained from a subgroup of TAO patients had characteristic pathological findings of TAO: occlusion of the artery with organizing thrombus and areas of recanalization, adventitial fibrosis, swelling of endothelial cells of the vasa vasorum with edema beneath the external elastic lamina, and no definite evidence of atherosclerotic plaque. iNOS staining showed positive iNOS-expressing cells in the endothelial layer (Figures 4A and 4B). Such staining was more prominent in the occluded segment of the artery compared to the non-occluded segment. TUNEL staining to detect apoptotic cells also showed positive expression of cells in the endothelium (Figures 4C and 4D).
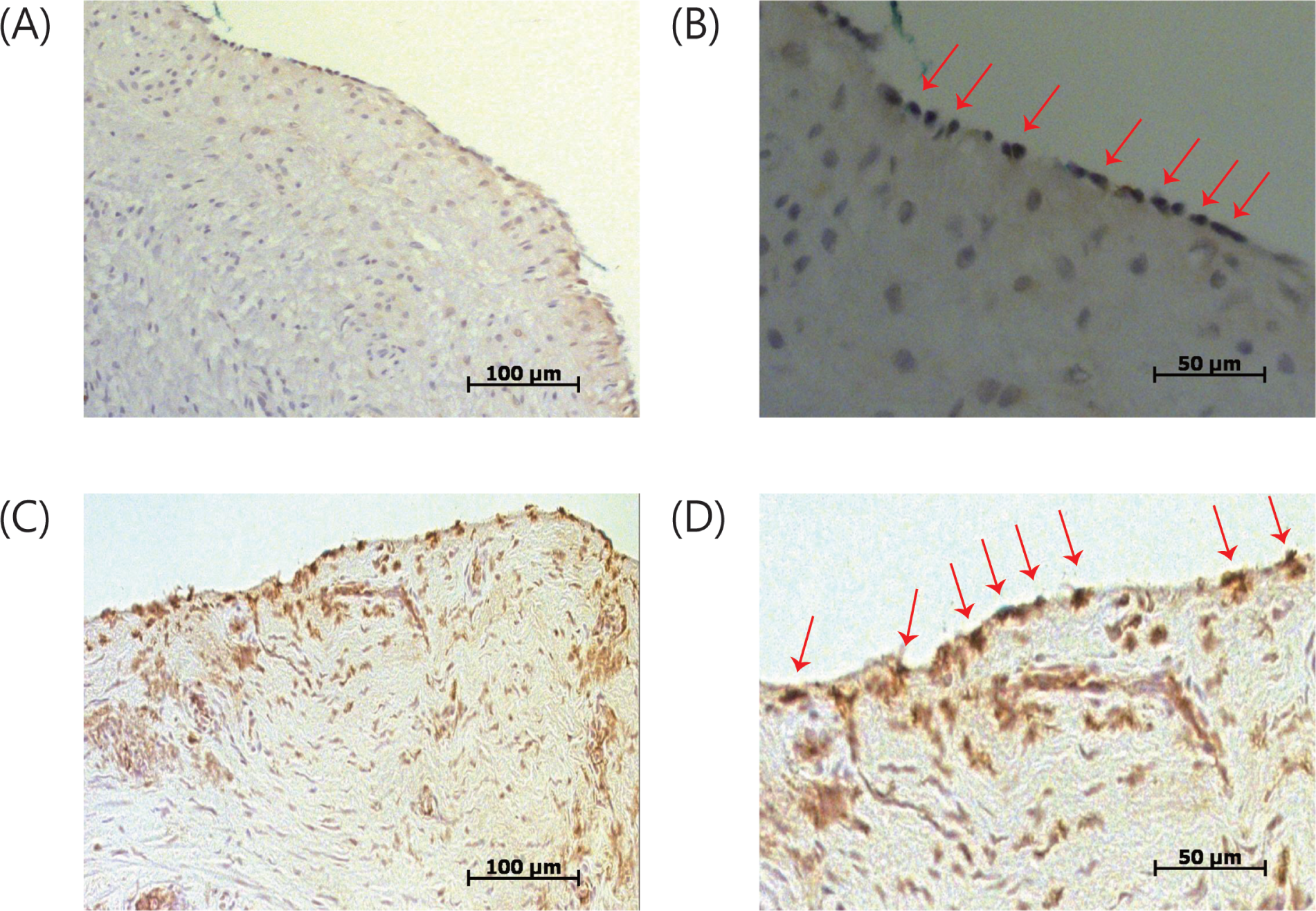
Immunohistochemical analyses of arterial specimens from TAO patients. (A) Inducible NOS staining from harvested artery of a TAO patient (200× magnification). (B) Higher magnification (400×) of iNOS staining shows positive staining cells in the intima layer (red arrows). (C) TUNEL staining from harvested artery of a TAO patient (200× magnification). (D) Higher magnification (400×) of TUNEL staining shows positive apoptotic cells in the intima layer (red arrows).
Discussion
The major findings of this study are that TAO patients had a significantly lower number of EPCs and EPC colonies compared to both healthy non-smokers and smokers. However, there were no differences in migration or tube formation of EPCs.
TAO has always been associated with smoking, and smoking cessation is the only proven method to halt disease progression. However, the causal relationship between TAO and smoking is not well understood. It has been reported that smoking reduces EPC levels significantly and cessation leads to restoration of EPC levels. 15 Our results also showed a significantly decreased number of EPCs in smokers compared to non-smokers. However, we were able to further demonstrate that EPC levels were significantly decreased in TAO patients compared to smokers, which implies that decreased EPC levels in TAO patients cannot be solely attributed to smoking. This suggests that TAO patients have a possible intrinsic decrease in EPC which could be innate in nature and may explain its prevalence at early ages as well as the increasing incidence of TAO in non-smokers. 21 Smoking may act as a triggering or aggravating factor, leading to an overall decrease in EPCs (responsible for endothelial repair function and neovascularization after ischemic insult).
The increase in apoptotic cells in the endothelium as shown by TUNEL staining from arterial biopsies provides evidence for the profound endothelial injury found in TAO patients. The insult to the endothelium occurs by the inflammatory nature of the disease, as shown by the increased expression of iNOS in the endothelial layer, since iNOS is only expressed when stimulated by endotoxins and inflammatory mediators under inflammatory and infectious conditions. 22 This increased iNOS produces an excess amount of NO, causing tissue damage and organ dysfunction through the generation of reactive species. 23 One interesting finding was that in contrast to this increase in iNOS-induced NO, the amount of endothelial nitric oxide synthase (eNOS)-dependent NO after stimulation with VEGF from the peripheral blood of TAO patients was lower than that of healthy individuals (data not shown), which can lead to impaired endothelium-dependent vasorelaxation in TAO patients. 24 The balance between eNOS-induced NO and reactive species is known to have a critical role in EPC dysfunction, 25 since eNOS is essentially involved in the mobilization of bone marrow-derived stem and progenitor cells. 26 Therefore, we speculate that the inflammatory nature of TAO may cause a decrease in eNOS expression, which in turn may affect the mobilization of EPCs, consequently leading to decreased circulating EPCs and endothelial dysfunction.
Our results did not show any differences in EPC migration and tube formation in TAO patients compared to healthy individuals, which demonstrates that in TAO, the function of each EPC is preserved, while only the numbers are decreased. However, another explanation is that our cells were early EPCs, since the cells were cultured for 1 week.27–29 Early EPCs are characterized by early growth spindle-shaped cells, with acetylated LDL, lectin and CD14 expression, weak endothelial cell marker expression and without the ability to form tubes on Matrigel, while late EPCs grow slowly and have a smooth-bordered, pebble-shaped appearance, with strong EC marker expression and active tube formation on Matrigel.30,31 The features of our EPCs resemble those of early EPCs, which have little ability for tube formation.
Our results differ from other studies that have investigated EPC numbers and function for TAO. In terms of EPC numbers, both Katsuki et al. 16 and Idei et al. 17 demonstrated similar circulating EPC levels by FACS analysis between TAO and healthy individuals, but Katsuki et al. further demonstrated that early EPCs were decreased in TAO patients after culture isolation. Hewing et al. 18 compared TAO patients against both healthy smokers and non-smokers and demonstrated that the putative EPC subset (CD45dim CD34+ VEGFR2+) was increased compared to smokers and was similar to non-smokers, while the immature CD45dim CD34+ CD133+ subset was similar in TAO individuals compared to smokers and decreased compared to non-smokers. In terms of EPC function, both Katsuki et al. and Idei et al. showed similar results between TAO and healthy individuals while Hewing et al. showed decreased functions in TAO compared to non-smokers. Such discrepancies may be due to differences in the method of EPC isolation and characterization. There is still controversy about the identification and origin of EPCs and there is no standardized method yet of isolation or culture. 32 Isolation from mononuclear cells by culture has the disadvantage that the culture conditions may vary the phenotypes of the cultured cells, which may differ from the EPCs that are actually circulating in the body, but isolation by FACS also has the disadvantage that the most specific marker subset is found in small numbers and therefore quantification may be unreliable. However, another explanation for this discrepancy is that our study involved very young TAO patients and age-matched controls, their median ages being 15–20 years younger than the other studies. This is a very powerful advantage of our study since it is less likely that degenerative risk factors which can influence EPC numbers may present in our study subjects. Additionally, the total amount of smoking in our TAO patients was probably lower than other studies, which may be more advantageous in identifying an intrinsic decrease in EPC in TAO patients compared to smokers. Therefore, it is likely that the young age of our patients was important in showing a difference in EPC numbers in TAO patients compared to smokers, as well as non-smokers, which may have not been apparent in other studies, and supports our hypothesis that TAO patients have an intrinsic decrease in EPC numbers not associated with smoking. In terms of EPC function, we have stated the nature of our EPCs as being of the early type, which may explain the similar tube formation and migration rate between TAO and healthy individuals. However, the possibility of a bias due to a small population size cannot be excluded, since EPC tube formation was significantly decreased in healthy smokers compared to non-smokers, yet TAO patients (who were also smokers) did not show a significant decrease in tube formation. Since tube formation rate in TAO patients was lower than non-smokers, it may be possible that this difference may be statistically significant with a larger population size. Even if statistical significance is reached, there is always the possibility that the difference may merely be the effects of smoking. Further studies with larger numbers are needed to verify any functional derangements in EPCs in TAO.
There are also several limitations to our study. Our study population was small (although the low prevalence of TAO should be considered, leading to a limitation of large clinical studies), age-matching between the groups was not rigorous enough, and the study was performed at a single institution. The role of EPCs in the pathogenesis of TAO, including the underlying mechanism by which TAO patients had lower levels of EPCs, needs to be determined further. This may be achieved by performing follow-up studies comparing TAO patients against a group of atherosclerosis obliterans patients (smokers and non-smokers), which would provide further insights regarding the difference in clinical presentation and pathogenesis between these two disease entities. Circulating EPC isolation by other methods such as FACS may provide further evidence about the nature of our cultured EPCs for more precise analysis. However, several studies have suggested that the functional activity of cells to augment neovascularization and endothelial repair is independent of the type of endothelial progenitor cell used, 10 and knowing these functional activities might be more important from a therapeutic point of view. From this point of view, another possible follow-up study is to verify the levels of EPC after exercise therapy in TAO patients. Physical training has been shown to increase EPC levels and enhance angiogenesis in cardiovascular diseases. 33 Since smoking cessation and exercise therapy are known efficient methods for the treatment of TAO, all of which are known to increase EPC levels, a study to determine the interactions involved may be of significance.
From a clinical perspective, recent studies in TAO have attempted the use of stem cell therapy through autologous transplantation to achieve therapeutic angiogenesis.34,35 Such clinical trials are the only option since animal models for TAO do not exist yet and thus preclinical studies are not possible. Unfortunately, stem cell therapy has its drawbacks, such as the unknown mechanism of action and fate of the implanted cells. Additionally, replenishing the lack of EPCs in TAO patients has a more direct mode of action and can be used for the prevention as well as the treatment of TAO. Several studies have suggested the use of EPCs for therapeutic purposes in other diseases,36 –38 and the results were promising. Since studies of EPC injection in TAO have not been performed yet, this could be another possible target for further studies.
In conclusion, TAO is a complex disease in which smoking plays a key role, but other mechanisms are also involved. We found that TAO patients have a possible intrinsic decrease in the number of EPCs which is further aggravated by smoking. This decrease in EPC numbers may cause endothelial dysfunction by impairment of endothelial repair mechanisms and neovascularization, which may contribute to the pathophysiology of TAO.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by grant SNUBH 04-2004-003 of Seoul National University Bundang Hospital.