
Abstract
Cytokine receptor subunits are released from cells in a regulated manner and circulate in soluble forms at concentrations that are orders of magnitude greater than the concentrations of the cytokines themselves. The purpose of this study was to determine if the circulating concentrations of soluble receptor subunits for interleukin-1 beta (IL-1β), tumor necrosis factor alpha (TNFα) and interleukin-6 (IL-6) might serve as early indicators of vascular dysfunction independent of the traditional cardiovascular disease (CVD) risk factors in women. Healthy women, aged 20–50 years (n = 36), were assessed for circulating concentrations of the cytokines IL-1β, IL-6 and TNFα and the soluble cytokine receptor subunits interleukin-1 receptor type I (sIL-1RI), sIL-1RII, sIL-6Rα, glycoprotein 130 (s-gp130), soluble TNF receptor type 1 (sTNFR1), and sTNFR2, along with traditional CVD risk factors. Cytokine receptor subunit expression on mononuclear cells and the release of these subunits in vitro were also determined. Brachial artery flow-mediated dilation (FMD), carotid intima-media thickness (cIMT) and carotid-femoral pulse wave velocity (cfPWV) were assessed by ultrasonography and Doppler probes. Circulating sIL-6Rα correlated negatively with FMD (r = −0.56, p = 0.007) independent of age and other CVD risk factors. Circulating sTNFR1 correlated positively with cfPWV (r = 0.60, p = 0.002). TNFR1 receptor expression on monocytes correlated positively with cIMT (r = 0.51, p = 0.004). Plasma concentrations of IL-1β, IL-6 and TNFα were not significantly associated with FMD, cIMT or cfPWV. These data suggest that the receptors for IL-6 and TNFα, rather than the cytokines themselves, may be better indicators of early vascular changes that are associated with CVD.
Introduction
The pathogenesis of atherosclerosis involves chronic, low-level inflammation and endothelial dysfunction,1,2 both of which are associated with altered subendothelial cell matrix and arterial stiffness. 3 Activated monocytes play a critical role in atherogenesis because they secrete pro-inflammatory cytokines that are central mediators of the initiation and progression of the inflammatory response, and these cytokines can also directly affect vascular cells, causing vascular dysfunction. 4 Circulating concentrations of inflammatory cytokines are often measured in clinical studies in order to assess inflammatory status, but due to their high bioactivity and short half-life, circulating concentrations tend to be low (a few pg/ml), often near the lower limits of detection of the assays. As a result, their strongest predictive value appears to be in those already identified at moderate risk for cardiovascular disease (CVD) or for prognosis in patients with established CVD.5,6
In contrast, soluble cytokine receptor subunits, produced by proteolytic cleavage of extracellular domains or by secretion of alternatively spliced variants, circulate at concentrations that are orders of magnitude higher, often in the ng/ml range, even in healthy individuals. 7 Soluble cytokine receptors can indicate cell activation when shed from leukocyte membranes, act as chaperones to extend cytokine bioavailability (soluble TNF receptor type 1 (sTNFR1), sTNFR2), 8 inhibit cytokine signaling (soluble interleukin-1 receptor type I (sIL-1RI), sIL-1RII, soluble glycoprotein 130 (s-gp130)), 9 or even contribute to signaling in cells lacking requisite high-affinity receptors (soluble interleukin-6 receptor alpha (sIL-6Rα)).10,11 To our knowledge, no studies have explored these soluble cytokine receptors as potential biomarkers for the early detection of CVD. However, soluble TNFR1 has shown some predictive value for mortality and heart failure following myocardial infarction.12,13
Therefore, we hypothesized that elevated concentrations of soluble receptor subunits for interleukin-1 beta (IL-1β), interleukin-6 (IL-6) and tumor necrosis factor alpha (TNFα) would be more sensitive indicators of low-level inflammatory processes associated with vascular dysfunction than the cytokine ligands themselves. This hypothesis was tested in healthy women by assessing circulating cytokine receptor subunit concentrations in vivo, expression on monocytes, and shedding in vitro. These data were then related to vascular function assessed by carotid-femoral pulse wave velocity (cf PWV), flow-mediated dilation (FMD) and carotid intima-media thickness (cIMT). The study population was originally recruited to investigate the influence of follicle-stimulating hormone (FSH) on cytokine synthesis and action in relation to bone density. Those results have been published. 14 FSH was not related to any of the cardiovascular variables or soluble receptors examined in the present study.
Materials and methods
Subjects
A total of 46 non-smoking, healthy women aged 20–50 years, experiencing natural menstrual cycles and not taking any prescription or non-steroidal anti-inflammatory drugs underwent testing after giving informed consent. The study was approved by the Human Assurance Committee at Georgia Health Sciences University.
Subjects reported to the laboratory between 7:30 and 9:00 a.m. after an overnight fast of 8–12 hours and at least 24 hours post-exercise and alcohol intake. Subjects completed questionnaires regarding their physical activity, 15 menstrual history and general health. 14 Cardiovascular testing was standardized as outlined by Laurent et al. 16 This was followed by body composition testing and venipuncture. Premenopausal women were tested during the early follicular phase of their menstrual cycle.
Common carotid artery intima-media thickness
Following a 10-minute resting period in the supine position, a longitudinal image of the cephalic portion of the right common carotid artery was acquired 1–2 cm proximal to the carotid bulb by high-resolution, B-mode ultrasonography using a linear array 5- to 10-MHz transducer (Philips Envisor; Philips Medical Systems, Bothell, WA, USA). IMT was measured at end-diastole for a minimum of 10 cardiac cycles with the lumen-intima and media-adventitia boundaries of the far wall traced automatically and calculated as the average of 0.1-mm samples over 10 mm using specialized software (Q Lab; Philips Medical Systems). Reliability testing for all vascular measures was conducted on eight men and women with and without hypertension on 2 separate days, at least 1 week apart. Reliability was measured by a one-way, random effect model intraclass correlation (ICC1,1). For cIMT, the mean difference between days was 0.02 ± 0.02 mm and the ICC1,1 was 0.96.
Brachial artery flow-mediated dilation
FMD was employed as a non-invasive measure of endothelial function. 17 A blood pressure cuff placed around the subject’s right proximal forearm was inflated to 230 mmHg (EC20; D.E. Hokanson, Issaquah, WA, USA). After 5 minutes of arterial occlusion, the cuff was rapidly deflated. Brachial artery mean diameter and blood velocity were measured via ultrasound duplex imaging (Envisor) 30 seconds before cuff inflation (resting diameter), 30 seconds prior to cuff deflation and for 3 minutes post cuff release. The artery was imaged approximately one inch above the antecubital fossa and magnification and focal zone settings were adjusted to optimize imaging of the near and far vessel wall. Arterial images were captured on a computer interfaced with the ultrasound machine and stored for off-line analysis. Semi-automated edge-detection software (Brachial Analyzer for Research; Medical Imaging Applications LLC, Coralville, IA) was used to measure the mean arterial diameter, which was the distance between the two media-adventitia borders. All post-occlusion diameters were automatically plotted over time to generate a curve. One hundred diameters (roughly 5 seconds and ≥ three cardiac cycles) at the peak of the curve (identified by visual inspection) were averaged to obtain a maximal brachial diameter. FMD was calculated as the percent increase in diameter above resting values. The day-to-day variability for FMD was 1.3% (range of 0.1% to 4%) for values of FMD that ranged from 3.6% to 15.4%. The correlation coefficient was 0.90 and the ICC1,1 was 0.85.
Mean blood velocity during FMD was measured simultaneously with 2-D imaging as described above using a pulsed wave Doppler signal. A pulsed Doppler signal was obtained at an insonation angle between 60° and 65° with the velocity gate set to include the middle third of the lumen area. The Doppler velocity waveform was traced and the mean velocity calculated using automatic tracing software (Doppler Flow Analysis Module; Medical Imaging Applications LLC). The peak shear rate was calculated as 4 × mean blood velocity / diameter. The mean difference for test-retest reliability for peak shear rate was 0.09 ± 0.77 s−1 and the ICC1,1 was 0.76.
Carotid-femoral pulse wave velocity
cf PWV, a measure of the speed at which a pressure or flow wave travels from a proximal to a distal point in the arterial tree, was obtained using simultaneous Doppler probes (Parks Medical, OR, USA) placed at the carotid and femoral arteries on the right side of the body. The time delay between the foot of the carotid flow wave and the femoral flow wave was determined for a minimum of 15 consecutive wave forms. The distance traveled by the pulse wave from the carotid to the femoral artery site was measured in triplicate with a tape measure placed on the body surface using the random zero method. cfPWV was calculated as distance traveled / time delay.
Body composition
Body composition was measured using dual energy X-ray absorptiometry (Hologic Discovery-W Densitometer; Hologic Inc., Bedford, MA, USA). Each scan was compartmentalized and analyzed using Hologic whole body software for total bone mineral density, fat-free soft tissue and percent body fat.
Blood collection and leukocyte isolation
Blood was drawn by venipuncture of the antecubital vein and collected into a 7-ml untreated tube for serum and a 6-ml EDTA-treated tube for plasma. The serum and plasma were aliquotted and frozen at −70°C for later analysis. Three 10-ml sodium heparin-treated tubes were drawn and the mononuclear cells were isolated by density gradient centrifugation (Histopaque 1077; Sigma Chemical, St Louis, MO, USA) for flow cytometry and cell culture.
Cardiovascular risk factors
Plasma concentrations of glucose, total cholesterol, low-density lipoprotein (LDL)-cholesterol, high-density lipoprotein (HDL)-cholesterol, and triglycerides were determined by enzymatic methods with a semi-automated chemistry system (Vitros DT60 II; Johnson & Johnson, Rochester, NY, USA). Oxidized LDL and insulin were measured by ELISA kits (both from ALPCO Immunoassays, Salem, NH, USA). The detection limit for the oxidized LDL assay was 0.8 ng/ml, with intra- and inter-assay coefficients of variability (COV) of 5.8% and 8.5%, respectively. The detection limit for the insulin assay was 0.8 mIU/L, with intra- and inter-COVs of 4.3% and 6.8%. The homeostatic model of assessment–insulin resistance (HOMA-IR) was calculated as: fasting glucose (mmol/L) × fasting insulin (mU/L) / 22.5.
Spontaneous cytokine secretion in vitro
Isolated mononuclear cells were washed with sterile saline (0.9% NaCl) and resuspended in phenol red-free RPMI-1077 medium supplemented with 2 mM of
Cytokine ligand and receptor analysis in plasma, serum, and supernatants
Concentrations of IL-1β, IL-6, and soluble cytokine receptors (sIL-1R types I & II, sTNFR1 & 2, sIL-6Rα and s-gp130) were measured in plasma, serum and supernatants by cytometric bead array (CBA; BD Biosciences, San Jose, CA, USA). All assays had detection limits of <5 pg/ml, based on 95% confidence intervals over blank. The intra-assay COVs were between 4% and 10%; the inter-assay COVs were between 4% and 15%.
Flow cytometric analysis of receptor expression on leukocytes
Membrane expression of interleukin-1 receptor type I (IL-1RI, CD121a) and type II (IL-1RII, CD121b), tumor necrosis factor receptor type 1 (TNFR1, CD120a) and type 2 (TNFR2, CD120b), IL-6 receptor alpha (IL-6Rα, CD126) and IL-6 receptor beta (gp130, CD130) was identified by one-color flow cytometry using phycoerythrin (PE)-conjugated monoclonal antibodies (BD Biosciences). Non-specific binding was assessed using appropriate PE-labeled isotype control antibodies. Receptor expression is presented as the relative fluorescence intensity (RFI) of cells stained with the anti-receptor antibody minus the RFI of the cells stained with the isotype control antibody. Monocytes were differentiated from lymphocytes in the isolated mononuclear cell preparations by forward- and side scatter characteristics. Owing to unavoidable variations in blood collection volumes and isolated cell yields, not all analyses were possible in all subjects.
Statistical analysis
All statistical analyses were performed using Statview statistical software (SAS, Cary, NC, USA). Descriptive statistics were used to describe the study subjects and results were reported as mean (standard deviation) or as median (interquartile range) for non-normally distributed data. Such data were normalized by log transformation prior to statistical analysis. Initial correlation matrices were conducted for each of the cardiovascular variables versus the 10 cytokine ligands and soluble receptor subunits. To avoid detecting spurious statistical significance as a result of performing 10 correlations per cardiovascular variable, calculated p-values were multiplied by 10, according to the Bonferroni method. 18 For multiple regression analysis, independent variables were selected based on proposed associations with the dependent variables of interest as supported by the literature, our hypothesis, and significant univariate correlations. A p-value of <0.05 was considered statistically significant for all statistical analyses. One outlier was visually detected in the oxidized LDL data and confirmed by performing a robust non-linear regression to fit a curve not influenced by outliers. The residuals of the robust fit were analyzed for outliers as described by Motulsky and Brown. 19
Results
Subject characteristics
Of the 46 subjects tested, serum progesterone measurements indicated that seven women were in the luteal phase, and procedural difficulties were encountered in three additional subjects; therefore, data are reported for 36 women. Eighteen women were Caucasian, 15 were African-American, two were Hispanic and one was Asian.
Subject characteristics with respect to modifiable CVD risk factors are presented in Table 1. All subjects met the threshold recommendations for desirable glucose, lipids, and cholesterol concentrations, and had optimal blood pressure. Self-reported physical activity indicated that, on average, the women were meeting the general exercise recommendations for healthy adults. 20
Subject characteristics.
Data given as means (SD).
Hormonal data is expressed as median (IQR).
BP, blood pressure; HOMA, homeostatic model assessment; HDLc, high-density lipoprotein cholesterol; LDLc, low-density lipoprotein cholesterol.
Flow-mediated dilation and sIL-6Rα
The average increase in brachial diameter was 0.204 mm (SD 0.112) with a peak shear rate of 295 s−1 (SD 76) resulting in a median percent dilation of 5.1% (interquartile range of 3.6% to 7.7%) of baseline diameter. An FMD ≤3.5% is reported to predict future cardiovascular events in women with CVD risk factors; 21 six of our subjects had an FMD below this level. FMD was not associated with the traditional modifiable CVD risk factors in this healthy population.
Of the 10 circulating cytokines and soluble receptors tested, only sIL-6Rα concentrations were significantly related (inversely) to FMD (r = −0.56, p = 0.007; Figure 1). Circulating concentrations of sIL-6Rα were also positively correlated with spontaneous secretion of sIL-6Rα by isolated peripheral blood mononuclear cells (r = 0.38, p = 0.002). Multiple regression indicated these secretion rates were negatively associated with HDL and positively associated with oxidized LDL (Table 2).
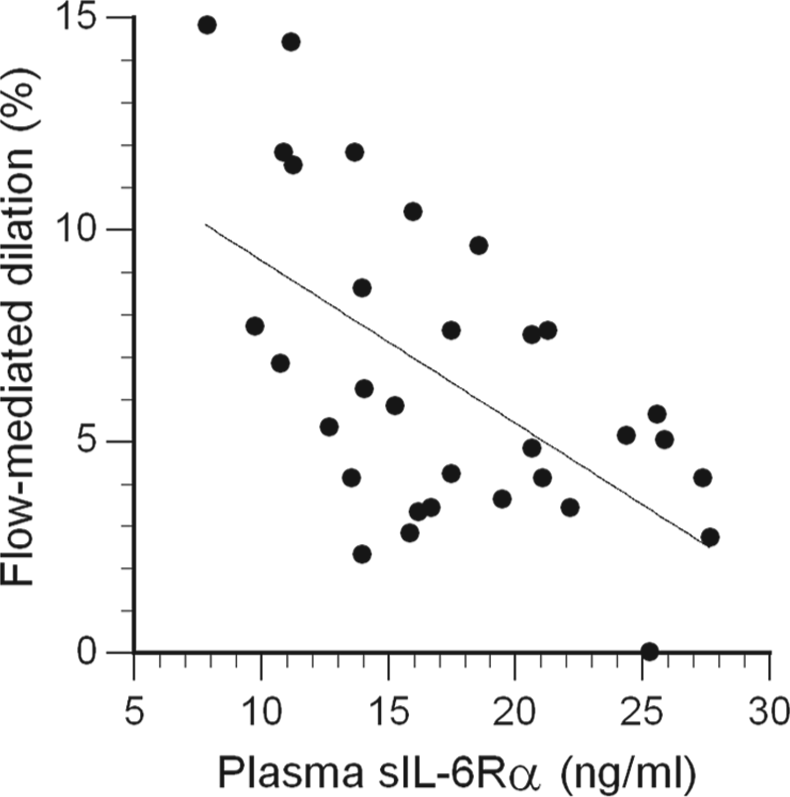
The inverse association of circulating soluble IL-6 receptor β (sIL-6Rα) concentration with flow-mediated dilation (FMD); r = −0.56, p = 0.007 (after Bonferroni correction).
Multiple regression with secreted sIL-6Rα as the dependent variable.
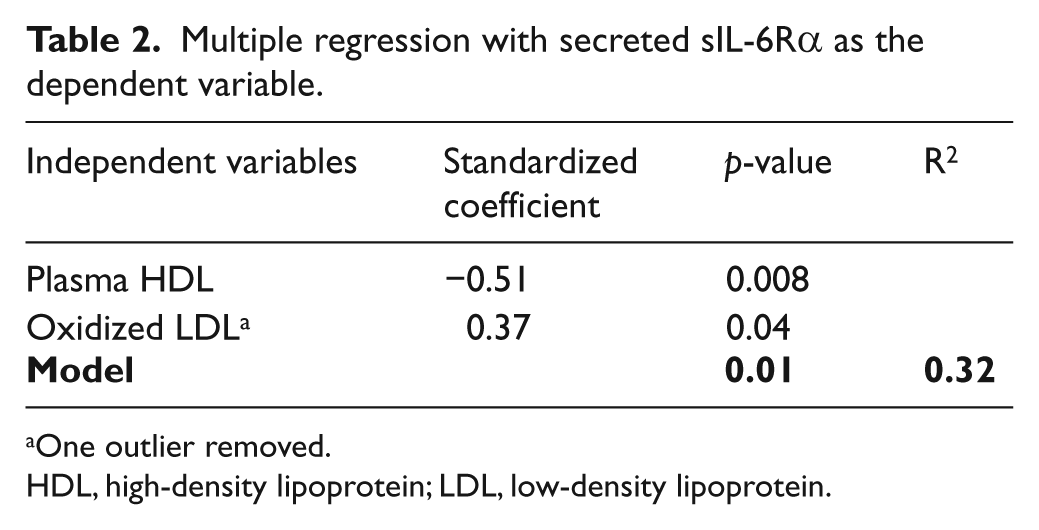
One outlier removed.
HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Arterial stiffness and sTNFR1
The average cfPWV was 743 cm/s, ranging from 512 to 1449 cm/s, and exhibiting a modest increase with age (r = 0.35, p = 0.04). These values are in line with published age-specific normal values for individuals with optimal blood pressure and no cardiovascular risk factors. 22
Of the 10 circulating cytokines and soluble receptors tested, only sTNFR1 and sTNFR2 concentrations were significantly related to cfPWV by simple regression (r = 0.60, p = 0.002 for sTNFR1 (Figure 2), and r = 0.51, p = 0.03 for sTNFR2 (not shown)), independent of age. In a multiple regression including both soluble receptors, only sTNFR1 was identified as an independent significant factor. TNFR1 expression on monocytes correlated with cIMT (r = 0.51, p = 0.004; Figure 3).
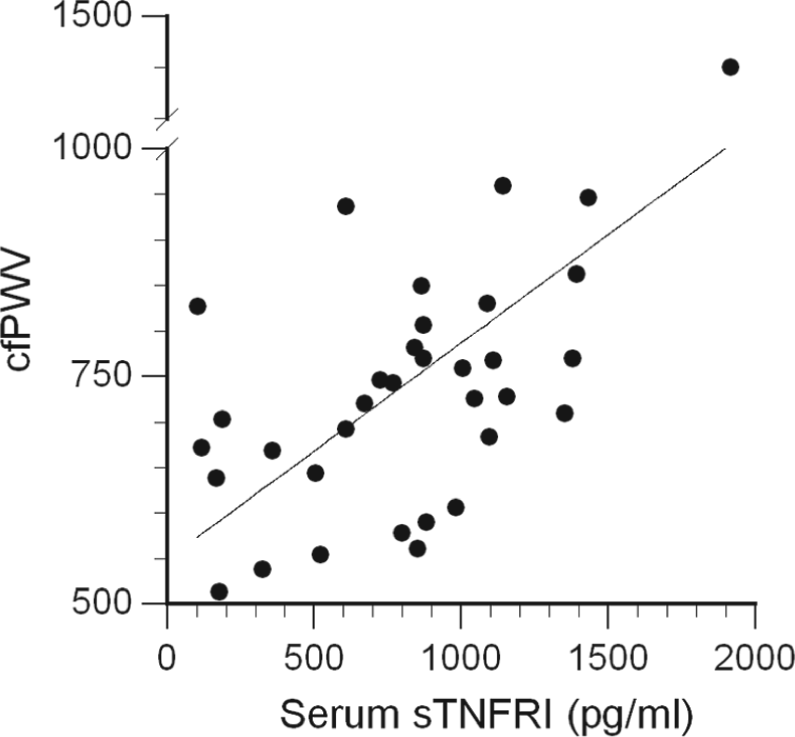
The correlation of circulating soluble TNF receptor type I (sTNFR1) concentration with carotid-femoral pulse wave velocity (cfPWV); r = 0.60, p = 0.002 (after Bonferroni correction).
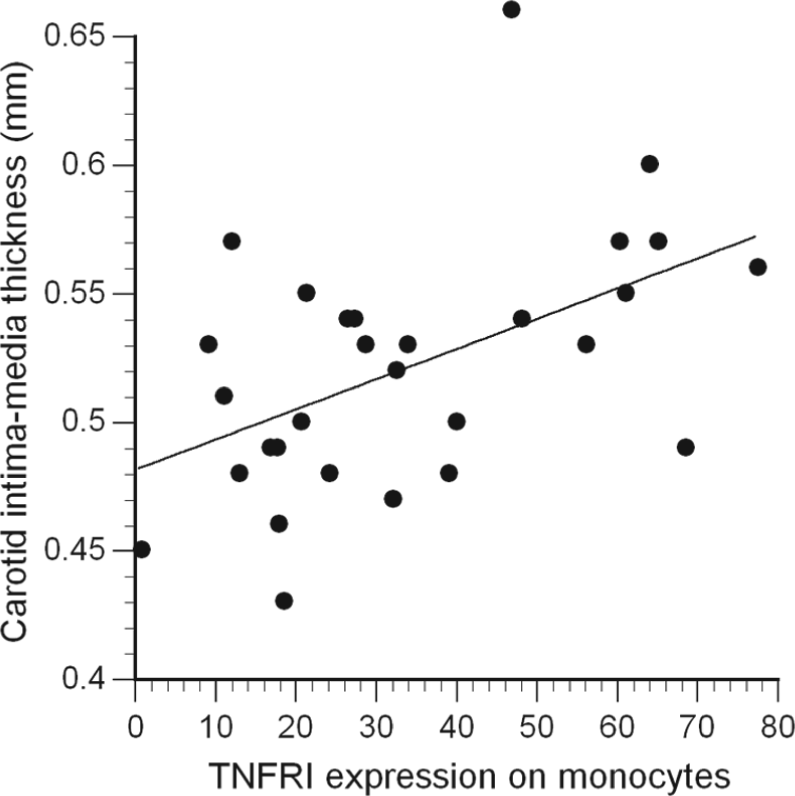
Relation between surface expression of TNFR1 on monocyte membranes and carotid intima-media thickness (cIMT) (r = 0.51, p = 0.004). Receptor expression is presented as the relative fluorescence intensity (RFI) of cells stained with the anti-receptor antibody minus the RFI of the cells stained with the isotype control antibody.
Discussion
The major findings of this study were that endothelial function was negatively associated with circulating sIL-6Rα concentrations, and arterial stiffness was positively associated with circulating sTNFR1, independent of the traditional modifiable CVD risk factors in women without clinical signs of CVD. Emphasis on early detection to prevent atherosclerosis, and knowledge that atherosclerosis is largely the result of an inflammatory process, has led researchers to search for inflammation-related proteins and cytokines involved in the initiation of the disease. Although IL-6 has shown some promise in this regard, its strongest predictive value appears to be in those already identified at moderate risk for CVD or for prognosis in patients with established CVD.5,6 Our findings support the value of sIL-6Rα as a marker of endothelial dysfunction in women without CVD risk factors or elevated inflammatory cytokines.
IL-6 directly affects endothelial cells by inducing endothelial cell adhesion molecule expression 23 and inhibiting endothelial nitric oxide synthase (eNOS) activation. 24 FMD depends upon eNOS activation, which is responsible for the synthesis of the endothelium-derived relaxing factor nitric oxide. The fact that we observed a negative correlation between FMD and sIL-6Rα (Figure 1), and not with IL-6, is consistent with the trans-signaling function of sIL-6Rα. Trans-signaling is necessary for IL-6 to influence endothelial cells because these cells express the gp130 subunits of the IL-6 receptor complex, but not IL-6Rα. Although endothelial function was not related to circulating IL-6 concentrations, this may be reconciled by evidence that endothelial cells constitutively produce IL-6 23 and can be stimulated by other cytokines, such as IL-1β, 25 to increase local IL-6 production. Therefore, the availability of sIL-6Rα may provide the actual regulatory control of the IL-6 effects on endothelial cells. 23
In our study, plasma concentrations of oxidized LDL were positively associated with spontaneous secretion of sIL-6Rα in unstimulated mononuclear cell cultures (Table 2). This observation is consistent with evidence that sIL-6Rα shedding can be induced by calcium mobilization, 26 and that oxidized LDL increases intracellular calcium concentrations in macrophages. 27 Secreted sIL-6Rα was also negatively associated with plasma concentrations of HDL. In addition to its well-known role in reverse cholesterol transport, HDL has been shown to inhibit LDL oxidation. 28 Therefore, HDL would inhibit the accumulation of LDL and its oxidation, thus diminishing its influence on monocytes. Furthermore, our observation corresponds with the anti-inflammatory influences that HDL (and its core constituent apolipoprotein A-I) has on monocytes and macrophages, including decreased expression of the adhesion molecule CD11b, 29 decreased production of the pro-inflammatory cytokines IL-1β, IL-6 and TNFα,30,31 and increased production of the anti-inflammatory cytokine IL-10. 32
The present study found an association between arterial stiffness and the TNF signaling system. TNFα can affect the mechanical properties of arteries by increasing the stiffness of vascular endothelial cells, 33 promoting proliferation, 34 and stimulating collagen deposition by fibroblasts. 35 Clinically, anti-TNFα treatment for rheumatoid arthritis and inflammatory diseases reduces aortic stiffness.36,37
However, we did not observe any correlation between cfPWV and TNFα itself. Instead, we found a strong positive correlation with sTNFR1 (Figure 2). This result is consistent with a previous study of older, non-obese, type 2 diabetic men and women. 38 In these subjects, who had much stiffer arteries than our subjects (80% exhibited cfPWV > 1400 cm/s), cfPWV correlated with sTNFR1, and more strongly with sTNFR2, but not TNFα. Thus, our results confirm and extend to a younger, healthy population the concept that circulating concentrations of soluble TNF receptors (but not TNFα) are related to vascular stiffness. Soluble TNFR1 has also been shown to have a predictive value in prospective studies of patients with CVD. Circulating sTNFR1 was superior to TNFα, sTNFR2, IL-6, IL-1 receptor antagonist, IL-10, and monocyte chemoattractant protein (MCP)-1 as a predictor of heart failure and death in patients following myocardial infarction.12,13 In chronic heart failure, sTNFR1 was a better predictor of mortality than TNFα, sTNFR2, IL-6 or sCD14. 39 Elkind and coworkers have reported that serum sTNFR1 concentrations were significantly related to carotid plaque thickness in a community study population between the ages of 40 and 70 years, even after adjustment for sex, race-ethnicity, hypertension, diabetes mellitus, LDL cholesterol, smoking, and body mass index. 40
There are several possible reasons why the circulating soluble TNF receptor concentration may be a better biomarker than TNFα itself. The soluble receptors have longer half-lives and greater stability. The variability observed in repeated daily, weekly and monthly plasma measurements of soluble receptor concentrations in healthy subjects was almost half that for TNFα 41 Moreover, soluble TNF receptors may protect TNFα from glomerular filtration and enzymatic degradation, and serve as a reservoir that releases TNFα to membrane-bound receptors with higher affinities for the cytokine. 8
Carotid IMT is a good surrogate marker for atherosclerotic disease and has a positive predictive value for future cardiovascular events independent of the traditional CVD risk factors in asymptomatic adults. 42 In the present study, TNFR1 expression on monocytes was positively related to cIMT (Figure 3). Because soluble TNF receptors are released from leukocytes stimulated by TNFα and other cytokines, 43 as well as by adhesion to activated endothelium, 44 increased circulating concentrations of these receptors may indicate leukocyte activation and/or leukocyte–endothelial cell interactions relevant to vascular function. Activation is also indicated by enhanced TNFR1 expression on monocyte membranes. 45 Animal studies have shown that atherosclerosis-prone mice, irradiated to ablate their bone marrow and then reconstituted with TNFR1-null leukocytes, develop smaller atherosclerotic lesions than mice reconstituted with normal cells. 46 Thus, TNFR1-expressing leukocytes appear to have a causal role in atherosclerotic plaque development.
Limitations
Our sample size was small due to the strict selection criteria, but we felt that these criteria were necessary to limit confounding factors that are not easily accounted for by statistical methods. For example, subjects taking non-steroidal anti-inflammatory drugs were excluded because of the large impact these drugs have on cytokine synthesis. 47 Also, women taking birth control medications were excluded and naturally cycling women were tested only during the follicular phase of their menstrual cycles due to the influence of reproductive hormones on monocyte function and cytokine secretion. 48 Ideally, our findings should be verified in a larger group of men and women at low risk for CVD along with objective measures of physical fitness, such as aerobic capacity.
We did not measure endothelium-independent dilation and therefore it is possible that the negative relation between FMD and sIL-6Rα is due to reduced vascular smooth muscle responsiveness to nitric oxide and not purely diminished endothelial production of NO. However, this seems unlikely because endothelial-independent dilation is not impaired in apparently healthy, young and middle-aged women.49,50
Because our study focused on women, our results may not be generalizable to men. Nonetheless, the HDL-cholesterol concentration has been shown to be positively associated with FMD and oxidized LDL-cholesterol negatively associated with FMD in young healthy men. 51 In that report, the men were selected for their consistently high or low HDL-cholesterol concentrations and the range in HDL-cholesterol concentrations was similar to that of our study subjects. Therefore, our findings in this regard (as shown in Table 2) complement this previous study by implicating sIL-6Rα shedding as the link between HDL and FMD.
Conclusions
These data suggest that the soluble receptors for IL-6 and TNFα, rather than the cytokines themselves, may be better indicators of early vascular changes that are associated with cardiovascular disease. Early detection of nascent vascular dysfunction can enable better preventive medicine strategies to reduce the burden of atherosclerotic disease.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was funded by NIH grant AG027714.