
Abstract
Diabetes has been inconsistently associated with increased risk of venous thromboembolism (VTE) and there is little direct evidence on the associations of glycemia levels with VTE. We used data from the Atherosclerosis Risk in Communities study to test the hypothesis that glycemia, as measured by hemoglobin A1c (A1c), is positively associated with VTE. Participants aged 45–64 years (n = 12,298) had A1c measured in 1990 and were followed for incident VTE (n = 345) through 2005. Because A1c is affected by diabetes treatment, analyses were stratified by history of diagnosed diabetes. Owing to evidence of non-linearity, we categorized A1c according to clinical cut-points: <5.7, 5.7–6.4, and ≥6.5% in those with no diagnosed diabetes; <7.0 and ≥7.0% in those with diagnosed diabetes. After adjustment for potential confounders, the hazard ratios (95% CIs) for VTE across increasing A1c categories were 1 (referent), 1.02 (0.77, 1.35) and 0.72 (0.41, 1.29) for those without diagnosed diabetes, and 1.30 (0.77, 2.17) and 1.41 (0.95, 2.09) for those with diagnosed diabetes. To explore the relation, we employed various models to adjust for potential confounding variables and modeled A1c as tertiles. We consistently found elevated hazard ratios in those with diagnosed diabetes, though the association was not statistically significant in every model. Hazard ratios in those without diagnosed diabetes were close to 1. In conclusion, our results are mildly suggestive that diagnosed diabetes and high levels of glucose, per se, may increase the risk of VTE. Elevated glucose was not related to VTE in those without diagnosed diabetes.
Introduction
Diabetes has been proposed as a risk factor for venous thromboembolism (VTE), the theoretical mechanism being that hyperglycemia contributes to elevated coagulation factors and impaired fibrinolysis.1,2 Indeed, laboratory evidence suggests that high glucose levels: (1) increase oxidative stress, which in turn increases gene transcription of coagulation factors; (2) degrade the glycocalyx layer of the endothelial wall, which releases coagulation factors; and (3) increase glycation of proteins involved in coagulation and fibrinolysis, shifting their activity towards a procoagulant state. 1 However, reported associations of diabetes with VTE are inconsistent,3–23 and more than half of prior investigations did not adjust for adiposity – an important confounding variable – hampering interpretation. A previous systematic review and meta-analysis 24 estimated a 40% increased risk of VTE for persons with diabetes compared to persons without diabetes. However, the meta-analysis was based on crude results; therefore, the reported association is likely confounded by age, adiposity, and other confounders.
One way to address this controversy is to evaluate the full spectrum of hyperglycemia, including below and above the threshold for the diagnosis of diabetes. Because there is little evidence20,21 on whether hyperglycemia is a long-term risk factor for VTE, we tested the hypothesis that hyperglycemia, as measured by hemoglobin A1c (A1c) – a marker of long-term glycemic control – is positively associated with incident VTE before and after adjustment for adiposity.
Methods
Study population
The Atherosclerosis Risk in Communities (ARIC) study is an ongoing community-based cohort designed to examine risk factors for cardiovascular disease. In 1987–89 (Visit 1), ARIC recruited and examined 15,792 participants aged 45–64 years living in four US communities: Forsyth County, NC; Jackson, MS; suburban Minneapolis, MN; and Washington County, MD. 25 The study was approved by the Institutional Review Boards of the collaborating institutions and informed consent was obtained from all participants before inclusion in the study. ARIC’s Visit 2 (1990–1992), attended by 14,348 participants, was the only visit for which stored whole blood samples were available for measurement of A1c; therefore, ARIC’s Visit 2 served as the baseline visit for the present study. Individuals were excluded from analyses if they had a history of VTE or anticoagulant use at baseline (n = 407); were of a race other than African American or white (due to small numbers) (n = 42); were African American from Washington County or Minneapolis suburbs (due to small numbers) (n = 49); or had missing data on any variable included in the main analysis (n excluded = 1552: 272 missing A1c, 57 missing diagnosed diabetes status, 1191 missing hormone use status, eight missing smoking status, 20 missing body mass index (BMI), and four missing waist-to-hip ratio (WHR)). Our final sample size was 12,298.
VTE ascertainment
Hospitalizations were identified by annual telephone calls to all participants and active surveillance of community hospitals. VTEs were identified using hospital discharge ICD codes and validated by physician review using standardized criteria. 26 VTE events were categorized as provoked or unprovoked. Provoked VTE was defined as occurring within 90 days of major trauma, surgery, marked immobility, active cancer or chemotherapy. Unprovoked were all other confirmed VTE cases. The present study includes follow-up for VTE from baseline until December 31, 2005.
Measuring and modeling A1c
Frozen whole-blood samples were thawed and assayed for A1c using high-performance liquid chromatography (Tosoh Corp.) and standardized to the Diabetes Control and Complications Trial assay. 27 Because A1c is affected by diabetes treatment, the main analysis was stratified by history of diagnosed diabetes, defined as a self-reported physician diagnosis or use of diabetes medication. To assess the association between A1c modeled as a continuous measure and VTE, we used Cox regression with restricted cubic splines. 28 We used splines to visually check the linearity of the association by graphing the natural log of the hazard ratio (HR) on the Y-axis. Owing to evidence of non-linearity, we categorized A1c. For ease of interpretation, the main analysis was categorized according to clinical cut-points established by the American Diabetes Association: 29 <5.7% (normal), 5.7–6.4% (prediabetes), and ≥6.5% (undiagnosed diabetes) in those with no diagnosed diabetes; and <7.0% (good glycemic control) and ≥7.0% (poor glycemic control) in those with diagnosed diabetes. Since the number of participants in each A1c category varied greatly when using clinical cut-points, we also modeled A1c as group-specific tertiles.
Baseline measurements
BMI, WHR, smoking status, diabetes medication use, and hormone use (females only) were assessed by trained personnel using standardized protocols. 30
Statistical analyses
Participant characteristics were compared across baseline categories of A1c: ANOVA F-tests were used to compare means and chi-squared tests were used to compare counts. VTE incidence rates were calculated by dividing the number of VTE events by person-years of follow-up, and 95% confidence intervals (CIs) were obtained using Rothman’s Episheet (krothman.hostbyet2.com/Episheet.xls). Cox regression was used to calculate HRs and 95% CIs of VTE according to A1c categories, using those without diagnosed diabetes and in the lowest A1c category as the referent. Model 1 was adjusted for age, race, and sex. Model 2 was adjusted for age, race, sex/hormone therapy use, and smoking status. Model 3 was adjusted for variables in Model 2 plus BMI and WHR. Model 4 was adjusted for variables in Model 3 plus diabetes medication use. We included covariates known to be risk factors for VTE in ARIC. As a sensitivity analysis, people taking diabetes medications were excluded. We verified the proportional hazards assumption through inspection of ln(–ln) survival curves by A1c category.
Results
The mean age of participants at baseline was 57 years, approximately 50% were female, and three-quarters were white. For the most part, characteristics of ARIC participants differed by A1c groups (Table 1).
Characteristics of ARIC participants according to hemoglobin A1c clinical cut-points at ARIC Visit 2, 1990–1992.
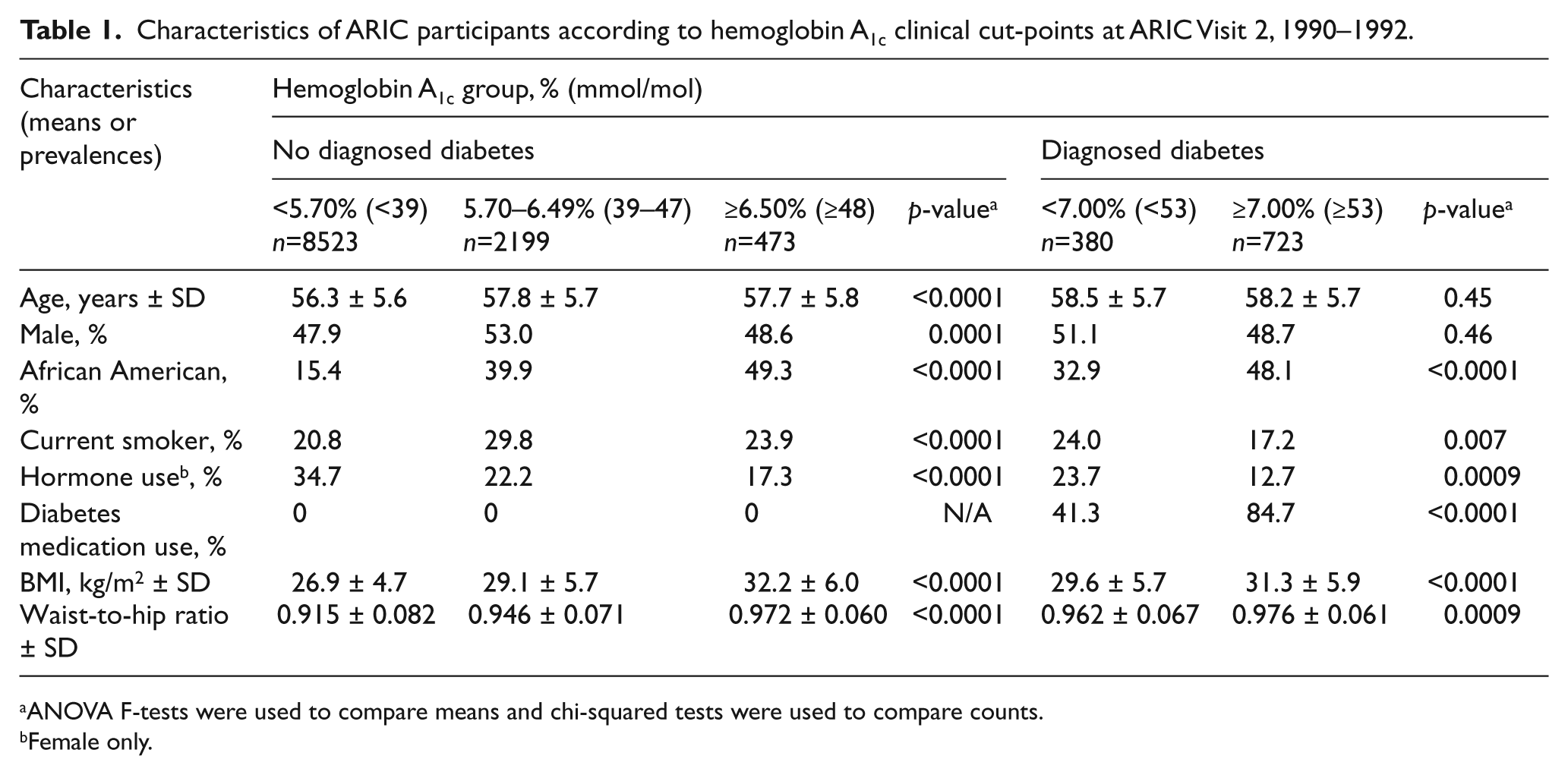
ANOVA F-tests were used to compare means and chi-squared tests were used to compare counts.
Female only.
Participants were followed for a total of 162,608 person-years (median 14.1, maximum 15.9 years). The number of VTE events across increasing A1c categories was 210, 74, and 13 for those without diagnosed diabetes, and 16 and 32 for those with diagnosed diabetes. The crude incidence rates (95% CIs) of VTE per 1000 person-years across increasing A1c categories were 1.82 (1.59, 2.08), 2.60 (2.06, 3.25), and 2.17 (1.21, 3.60) for those without diagnosed diabetes, and 3.39 (2.02, 5.37) and 3.87 (2.70, 5.40) for those with diagnosed diabetes.
Diagnosed diabetes
There was a modest positive association between diagnosed diabetes and VTE (Table 2). The Model 1 HRs (95% CIs) – comparing participants with diagnosed diabetes and an A1c value of <7.00% (<53 mmol/mol) or ≥7.00% (≥53 mmol/mol), respectively, to a reference group of those without diagnosed diabetes in the lowest A1c category – were 1.56 (0.94, 2.60) and 1.78 (1.21, 2.61). Model 2 HRs, which additionally adjusted for hormone therapy use and smoking status, were similar to Model 1 HRs. However, the association was attenuated and non-significant after adjustment for known confounding variables BMI and WHR: Model 3 HRs (95% CIs) for those with diagnosed diabetes and an A1c of <7.00% (<53 mmol/mol) or ≥7.00% (≥53 mmol/mol), respectively, were 1.30 (0.77, 2.17) and 1.41 (0.95, 2.09). After further adjustment for diabetes medication use (Model 4), there was a statistically significant elevated risk for unprovoked VTE [HR (95% CI): 3.06 (1.15, 8.15)] in those with diagnosed diabetes in the highest A1c category as compared to the referent, but this must be viewed cautiously as it was based on few events. When A1c was modeled as tertiles (Table 3), those with diagnosed diabetes and A1c≥9.10% had about twice the risk of total VTE as those with no diagnosed diabetes and low A1c values, an HR that was statistically significant in Models 1, 2 and 3, but not Model 4. Excluding those on diabetes medication as a sensitivity analysis did not materially change results (data not shown).
Adjusted hazard ratios (95% CIs) for incident venous thromboembolism (VTE) by hemoglobin A1c clinical cut-points, ARIC, 1990–2005.
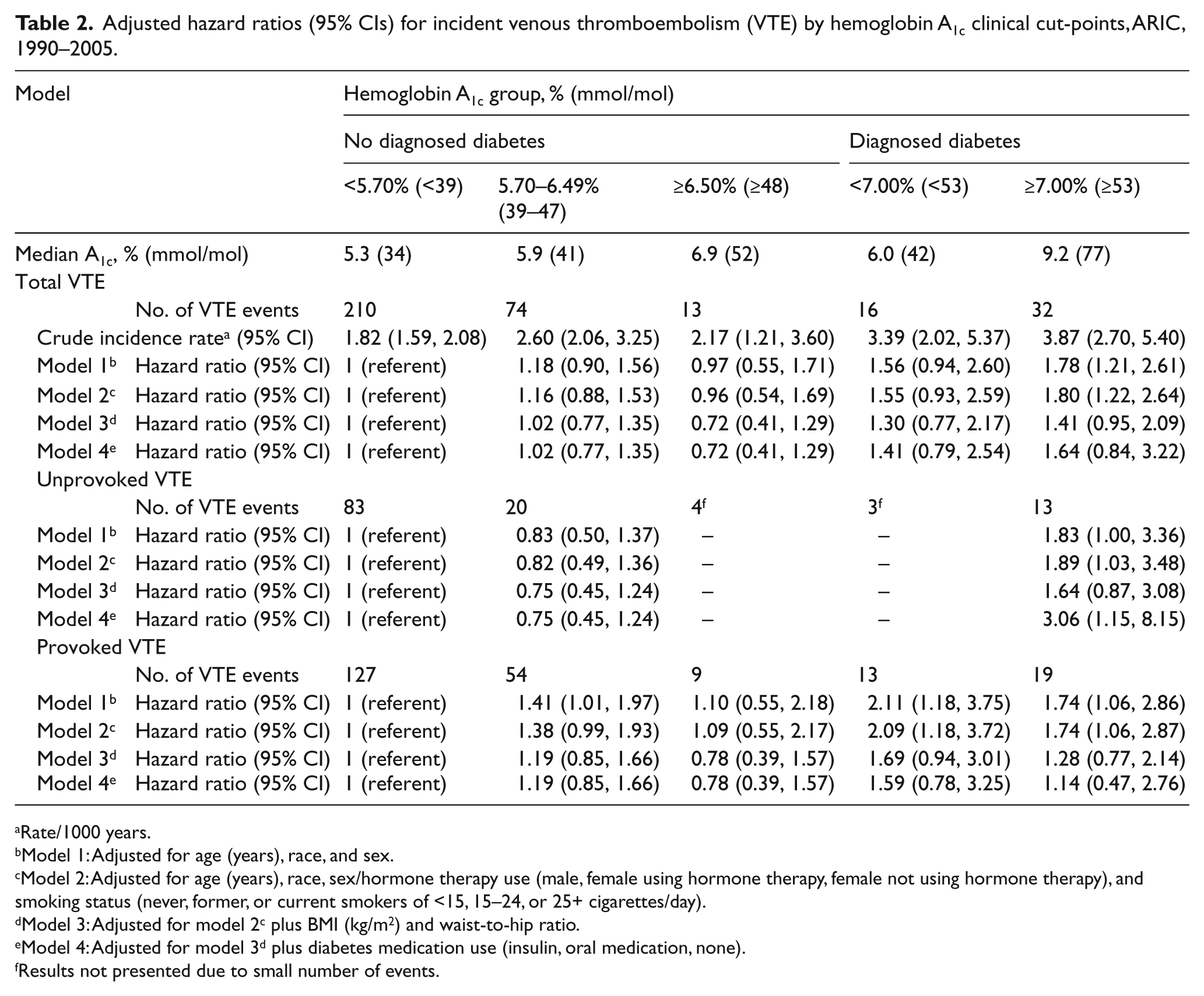
Rate/1000 years.
Model 1: Adjusted for age (years), race, and sex.
Model 2: Adjusted for age (years), race, sex/hormone therapy use (male, female using hormone therapy, female not using hormone therapy), and smoking status (never, former, or current smokers of <15, 15–24, or 25+ cigarettes/day).
Model 3: Adjusted for model 2c plus BMI (kg/m2) and waist-to-hip ratio.
Model 4: Adjusted for model 3d plus diabetes medication use (insulin, oral medication, none).
Results not presented due to small number of events.
Adjusted hazard ratios (95% CIs) for incident total venous thromboembolism (VTE) by group-specific tertiles of hemoglobin A1c, ARIC, 1990–2005.
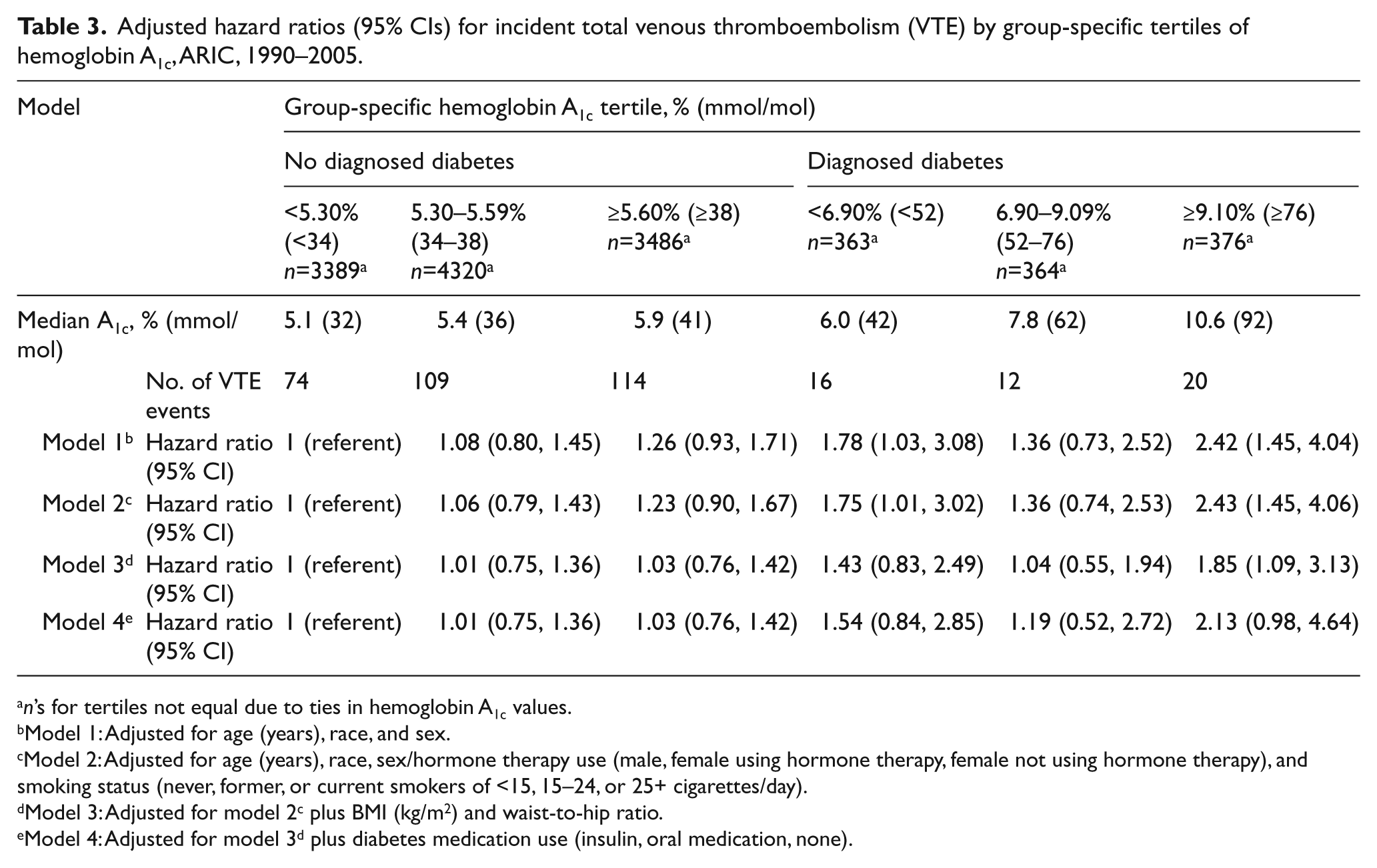
n’s for tertiles not equal due to ties in hemoglobin A1c values.
Model 1: Adjusted for age (years), race, and sex.
Model 2: Adjusted for age (years), race, sex/hormone therapy use (male, female using hormone therapy, female not using hormone therapy), and smoking status (never, former, or current smokers of <15, 15–24, or 25+ cigarettes/day).
Model 3: Adjusted for model 2c plus BMI (kg/m2) and waist-to-hip ratio.
Model 4: Adjusted for model 3d plus diabetes medication use (insulin, oral medication, none).
No diagnosed diabetes
HRs in those without diagnosed diabetes were close to 1, regardless of VTE type and whether A1c was modeled using clinical cut-point categories (Table 2) or tertiles (Table 3).
Further analyses
The relation between A1c modeled as a continuous measure and VTE was non-significant (data not shown).
Discussion
In this community-based study with more than a decade of follow-up, we found that participants with diagnosed diabetes tended to be at greater risk of incident VTE, though the associations were not statistically significant in every model. Importantly, there were few VTE events in participants with both diagnosed diabetes and high values of A1c, giving low precision to the HRs in these subgroups. Overall, we found little evidence to suggest an independent association between hyperglycemia and VTE risk below the threshold for diagnosis of diabetes.
There is little prior evidence to suggest glycemia, per se, is a risk factor for VTE. Two prior studies reported no association.20,21 However, they only had information on non-fasting glucose, which has high within-person variability 31 and is affected by recent food intake and other factors. A1c, which was measured in the present study, is an indicator of average glucose exposure over the previous 2–3 months and tracks well in individuals over time. 32 In the present study, diagnosed diabetes and high values of A1c tended to be associated with higher VTE risk. This association remained after adjusting for diabetes medication use and, separately, after excluding those on diabetes medication, suggesting that use of diabetes medications were not the explanation.
There have been many more studies of whether diabetes, as opposed to glycemia levels, is a risk factor for VTE. Yet, more than half of prior studies of the association of diabetes with VTE did not adjust for adiposity,5,6,8,10,12–16,19,20,22,23 a known confounder.17,33,34 This lack of adjustment for adiposity may have yielded overestimates of the association of diabetes and VTE in prior studies. Indeed, we observed strong confounding by adiposity in the present study; all HRs were lower after adjustment for BMI and WHR.
Of the seven prior studies that did adjust for adiposity,3,4,7,9,11,17,18 four3,4,7,9 reported a positive association between diabetes and VTE. However, two of the four7,9 modeled adiposity as a binary variable (e.g. obesity or no obesity), raising a strong possibility of residual confounding. The other two studies adjusted for adiposity as BMI (kg/m2): Lutsey et al. 4 reported a HR of diabetes for VTE of 1.22 (95% CI: 1.04, 1.44) and Tsai et al. 3 reported a HR of 1.46 (95% CI: 1.03, 2.05). Tsai’s report of a positive diabetes–VTE association included ARIC plus the Cardiovascular Health Study, but a 2012 ARIC paper that updated diabetes status over follow-up did not find a statistically significant association between diabetes and VTE in ARIC: 1.20 (95% CI: 0.92, 1.55). 11 This discrepancy might be explained by differences in exclusions, follow-up time, adjustments for confounding factors, choice of baseline visit, and study population (ARIC alone versus ARIC plus the Cardiovascular Health Study). In summary, existing (limited) evidence supports only a modest positive or no association of diabetes or glycemia with VTE.
Limitations of this study include the single measurement of A1c, an inherently time-varying variable. And, despite our large, community-based sample, there were few VTE events at high values of A1c, making our HRs at high values imprecise. Also, it is possible that residual confounding remains. This seems particularly plausible when comparing extreme groups (e.g. highest to lowest A1c group) and might explain the observed association between high values of A1c and VTE.
In conclusion, our results are mildly suggestive that diagnosed diabetes and high levels of glucose, per se, may increase the risk of VTE. However, elevated glucose does not seem to be related to VTE in those without diagnosed diabetes. Further research, with more power to determine whether high levels of glucose raise the risk of VTE, is warranted. Our findings also demonstrate the importance of rigorous measurement and adjustment for measures of adiposity in future studies of diabetes or glycemia and VTE.
Footnotes
Acknowledgements
The authors thank the staff and participants of the ARIC study for their important contributions. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of conflicting interest
All authors reported no conflict of interest associated with this study.
Funding
This work was supported by NIH NIDDK (R21 DK080294) and the National Heart, Lung, and Blood Institute contracts (HHSN 268201100005C, HHSN268201100006C, HHSN268201100007C, HHSN268201100008C, HHSN268201100009C, HHSN2682 01100010C, HHSN268201100011C, HHSN268201100012C, and T32HL007779).