
Abstract
Objectives
To measure the rate of Demodex folliculorum mite infestation in patients with type 2 diabetes mellitus and to investigate if it was related to blood glucose control.
Methods
Patients with type 2 diabetes were classified according to their glycosylated haemoglobin (HbA1c) level into two groups: a well controlled blood glucose group (HbA1c ≤ 7%) and a poorly controlled blood glucose group (HbA1c > 7%). A standardized skin surface biopsy method was used to determine if the patients had D. folliculorum infestation (>5 mites/cm2 of skin).
Results
A total of 69 patients (38 female) were enrolled in the study. Seventeen (24.6%) patients had D. folliculorum infestation. There were no significant differences in age, sex or body mass index between patients with and without D. folliculorum infestations. A significantly higher proportion of patients with poor blood glucose control had D. folliculorum infestation compared with patients with well controlled blood glucose.
Conclusions
These current findings suggest that poor blood glucose regulation increases the susceptibility to D. folliculorum mite infestation in patients with type 2 diabetes.
Introduction
Diabetes mellitus is a group of metabolic diseases characterized by hyperglycaemia due to defects in insulin secretion, insulin action, or a combination of both of these metabolic disturbances. 1 Infections occur frequently in patients with diabetes mellitus and their presence can trigger acute metabolic complications. 2 The long-term complications of diabetes mellitus have negative effects on both the cellular and humoral immune systems. For example, the chemotactic function of polymorphonuclear leucocytes is impaired in patients with diabetes. 3 Several abnormalities might contribute to the enhanced susceptibility and severity of infections in patients with diabetes: for example, reduced mastocyte function, lower neutrophil chemotactic activity, poor leukocyte–endothelial cell interactions and reduced leucocyte numbers in inflammatory lesions, low oxidant molecule production, decreased lymph node retention capacity and reduced cytokine release.4–7
Demodex is a tiny spindle-shaped mite 0.3–0.4 mm long that lives on mammals. Although there are numerous species of Demodex, only Demodex folliculorum and D. brevis live on the hair follicles and pilosebaceous glands of humans. Demodex mites most frequently colonize the eyelids, forehead, nose, nasolabial folds, cheek and chin, but they can also be found anywhere on the skin. Although most people are colonized by Demodex mites, they rarely cause clinical symptoms. Demodex mite infestation is associated with rosacea, pityriasis folliculorum, acne vulgaris and blepharitis.8–11 The presence of D. folliculorum infestation is associated with immune suppression and has a higher prevalence in patients with chronic renal failure, diabetes mellitus and HIV. It may cause skin conditions, including pruritis and itching, in patients with type 2 diabetes mellitus.12–15
To our knowledge, there have not been any reports describing the relationship between blood glucose control in patients with type 2 diabetes mellitus and the presence of D. folliculorum mites. The aim of the current study was to investigate the effect of blood glucose control on the existence of opportunistic D. folliculorum mites in patients with type 2 diabetes mellitus.
Patients and methods
Patient population
Patients diagnosed with type 2 diabetes mellitus were enrolled sequentially from the Outpatient Clinic of the Department of Endocrinology and Metabolism, Medical Faculty, Mustafa Kemal University, Hatay, Turkey between January 2012 and December 2012. Type 2 diabetes mellitus was diagnosed by demonstrating any one of the following criteria: (i) fasting plasma glucose level ≥7.0 mmol/l (126 mg/dl); (ii) an oral glucose tolerance test showing a plasma glucose level ≥11.1 mmol/l (200 mg/dl) at 2 h after a 75 g oral glucose load; (iii) symptoms of hyperglycaemia such as polyuria, polydipsia and polyphagia in conjunction with a random plasma glucose level ≥11.1 mmol/l (200 mg/dl). 1 The patients were further classified according to their glycosylated haemoglobin (HbA1c) level into two groups: a well controlled blood glucose group, HbA1c ≤ 7% and a poorly controlled blood glucose group, HbA1c > 7%.1,16
The exclusion criteria for both groups of patients with type 2 diabetes were as follows: age <18 years; dermatological disease on the face (such as herpes infection, impetigo, perioral dermatitis, seborrhoeic dermatitis, lupus erythematous); pregnancy; lactation; systemic diseases (malignancy, chronic liver and renal disease); radiotherapy; chemotherapy; topical acaricidal usage; and use of oral or topical antibiotics in the previous month.
The study was approved by the Ethics Committee of Mustafa Kemal University Medical School, Hatay, Turkey (registration number: MKU-2012) and written informed consent was obtained from all patients. The study procedures complied with the current laws of the Republic of Turkey and the Declaration of Helsinki.
Laboratory measurements
Blood samples were collected after a 12-h fast from the ulnar vein of each patient for the analysis of fasting plasma glucose and whole blood HbA1c levels. The blood was anticoagulated with ethylenediaminetetra-acetic acid to produce plasma. All of the biochemical analyses were completed on the same day as the blood collection. Fasting plasma glucose levels (ARCHITECT c8000 Analyser; Abbott Diagnostics, Lake Forest, IL, USA) and whole blood HbA1c levels (VARIANT II System; Bio-Rad, Hercules, CA, USA) were determined routinely according to the manufacturers’ instructions. Body mass index (BMI) was determined using the ratio of weight (kg) to height squared (m2).
Analysis of D. folliculorum mite infestation
The presence of D. folliculorum mites was investigated in all patients using the standardized skin surface biopsy (SSSB) technique for measuring the density of Demodex mites. 17 In this method, clinical samples were taken using cyanoacrylate-containing glue. Before taking the skin samples, the selected skin regions (nose, chin, left cheek, right cheek and forehead) were cleaned with alcohol to remove any creams and lotions and the areas were allowed to dry. A 1 cm2 circle was drawn on one side of a glass slide with an appropriate pen and 1 ml of cyanoacrylate-containing glue was added to the other side of the glass slide. The adhesive-containing side of the glass slide was pressed against the skin to be sampled and left for 1 min. The slide was removed carefully from the skin at the end of this period. The slides were mounted using Hoyer’s solution 18 (1 ml) and the density of D. folliculorum mites was evaluated using a light microscope (Olympus CH20; Olympus Optical, Tokyo, Japan) at magnifications of × 40 and × 100. The identification of >5 mites/cm2 of skin was classified as a D. folliculorum mite infestation.
Statistical analyses
All statistical analyses were performed using the SPSS® software package, version 13.0 (SPSS Inc., Chicago, IL, USA) for Windows®. Continuous variables were analysed using the Kolmogorov–Smirnov test in terms of their normal distribution. Relationships between nominal variables were calculated using χ2-test and Fisher's Exact test. For continuous variables, Student’s t-test and Mann–Whitney U-test were used. A P-value < 0.05 was considered statistically significant.
Results
The relationship between the presence of a Demodex folliculorum infestation a and the age, body mass index (BMI) and glycosylated haemoglobin (HbA1c) level in patients with type 2 diabetes mellitus (n = 69).

D. folliculorum infestation (i.e. positive) was classified as >5 mites/cm2 of skin.
Mann–Whitney U-test.
NS, no statistically significant difference (P ≥ 0.05).
Analysis of the relationship between the presence of a Demodex folliculorum infestation a , demographic characteristics and blood glucose regulation in patients with type 2 diabetes mellitus (n = 69).
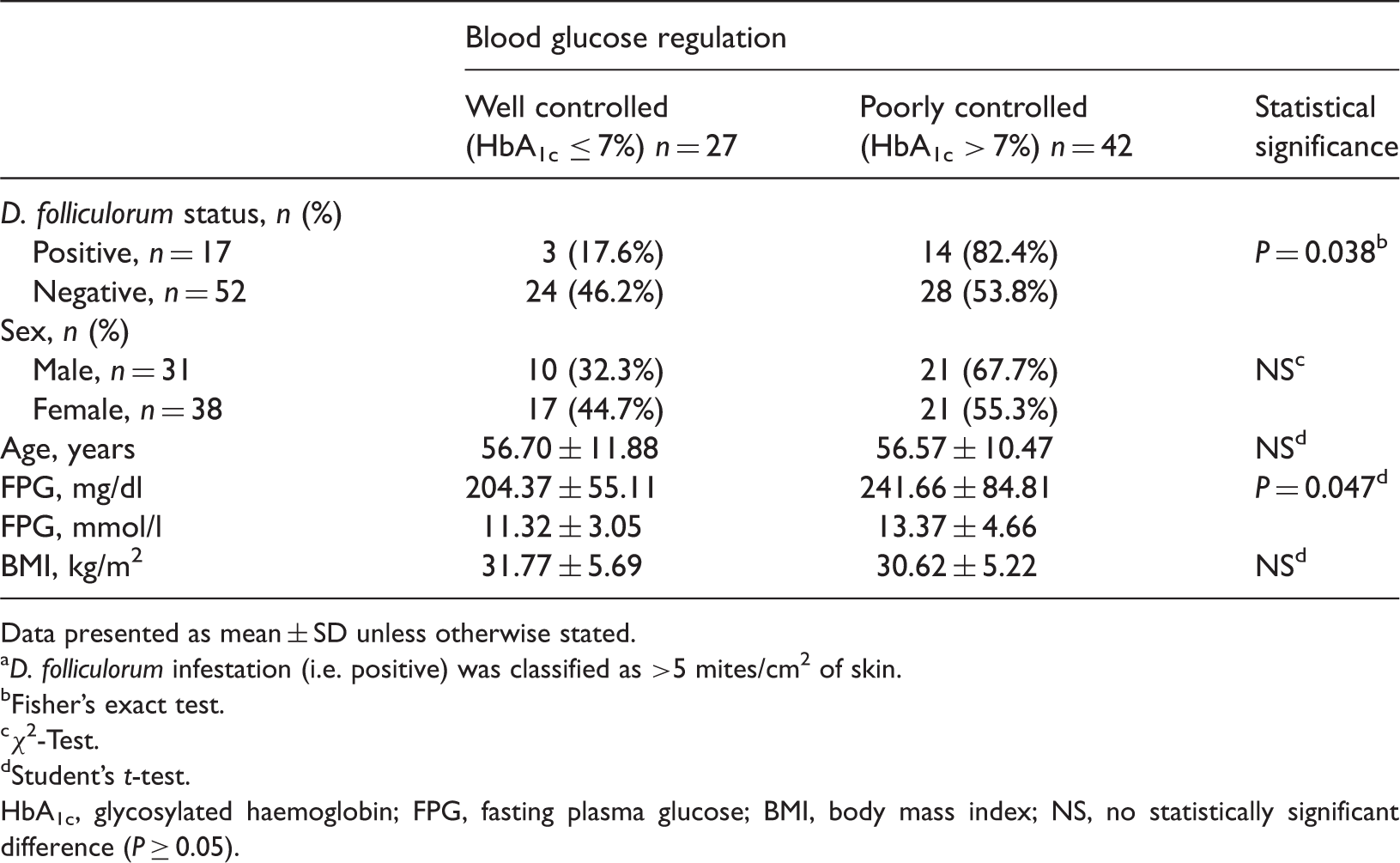
Data presented as mean ± SD unless otherwise stated.
D. folliculorum infestation (i.e. positive) was classified as >5 mites/cm2 of skin.
Fisher's exact test.
χ2-Test.
Student's t-test.
HbA1c, glycosylated haemoglobin; FPG, fasting plasma glucose; BMI, body mass index; NS, no statistically significant difference (P ≥ 0.05).
Discussion
The current study demonstrated that 24.6% of patients with type 2 diabetes had a D. folliculorum mite infestation as defined as >5 mites/cm2 of skin and mite infestation was significantly more common in women than men. This current study also demonstrated that a significantly higher proportion of patients with poorly controlled blood glucose levels had D. folliculorum mite infestation compared with patients with well controlled blood glucose levels.
Demodex folliculorum is a saprophytic mite located at the human pilosebaceous unit with a preference for facial skin and eyelashes. Infestation is usually asymptomatic, but suppurative or granulomatous inflammation may be seen with a high mite density. Dermatological disorders including rosacea, pityriasis folliculorum and blepharitis have been attributed to Demodex parasite infestation.8,9,11,12,19 It seems likely that there is usually a control mechanism limiting the number of follicle mites, but that local and systemic factors may cause an environment that is preferable to their growth. Immunosuppression may be related to an increase in the density of D. folliculorum, and demodicidosis has been identified in children with leukaemia who are taking chemotherapy. 20 Hypotheses suggest that either an immunological deficiency resulting in an increase in the number of Demodex mites or an abnormal immunological reaction of the skin to the parasites causes the dermatological lesions. 13 An increased incidence of Demodex mites was found in subjects with human leucocyte antigen (HLA)-Cw2 and HLA-Cw4 alleles, which was related to a decrease in natural killer cells. 21 Immunosuppression may result in an increase in the mite numbers, favouring an inflammatory reaction, or it may cause an impaired immunological response in the skin to the mite infestation.
Data regarding the prevalence of Demodex mite infestations in patients with diabetes are rare. In addition, there are no published data regarding the prevalence of Demodex mite infestations in patients with diabetes stratified according to the quality of their blood glucose control. A study of cheek biopsies from patients with diabetes found a significantly higher mean mite density and a greater mean mite size compared with cheek biopsies from control subjects. 15 A study that evaluated the prevalence of Demodex mites on the eyelashes of 256 subjects also reported that the mites were more common in patients with diabetes mellitus. 22
Many studies that have investigated the association between Demodex infestation and acquired immunodeficiency syndrome and cancer chemotherapy, and studies that have reported the higher prevalence of demodicidosis in potentially immunosuppressed subjects such as pregnant women and haemodialysis patients, have proposed that immunological deficiency may cause the overgrowth of the Demodex mites.20,23–25 Patients with diabetes mellitus have an increased risk for infections, but the exact pathophysiology of their immunocompromised state remains unknown.
Demodex infestation results in disruption of the skin barrier and the mites are responsible for epithelial erosion. 26 However, an increasing number of case reports and epidemiological studies show that in certain conditions the number of follicle mites increases, and this increase in mite numbers probably causes or contributes to the development of cutaneous disorders, such as granulomatous rosacea, bald papulopustular dermatosis, pustular folliculitis, blepharitis and spinulosis of the face.27–30
Although many cases are asymptomatic, the clinical features of demodicosis can include itching, vascular (flushes, erythema and telangiectasia) and inflammatory symptoms (folliculitis, papules and pustules) of the skin.26–29 For example, papulopustular rosacea disease is a multifactorial skin disease involving infestation by D. folliculorum.26–29 In some patients, the symptom of itching may be the only symptom experienced. Treatment with acaricidal agents can resolve the cutaneous symptoms of demodicosis and lead to wound healing. 30 Acaricidal creams and oral isotretinoin have been used to treat different cutaneous demodicosis lesions.26–30However, there are no clinical data about the use of acaricidal agents in patients with diabetes mellitus who have the symptoms of itching without any obvious skin disorders. Based on these current findings, we would recommend the use of acaricidal creams in patients with diabetes, particularly those with poorly controlled blood glucose levels, who have clinical findings suggestive of a Demodex mite infestation.
In conclusion, type 2 diabetes is an extremely common metabolic disorder, the only clinical symptom of which in some patients is itching or pruritis, which could be caused by an undiagnosed D. folliculorum mite infestation of the skin. The findings of this current study suggest that the prevalence of D. folliculorum mite infestation is high in patients with type 2 diabetes and that those patients with poorly controlled blood glucose levels are particularly susceptible. Therefore, in addition to considering the risk of microvascular and macrovascular complications associated with poor blood glucose control, physicians may also need to consider the possibility of the presence of parasitic infestations such as D. folliculorum. Further research is required to determine the clinical implications of Demodex mite infestations in patients with type 2 diabetes, particularly those with poor blood glucose control, and how these infestations can be best treated.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.