
Abstract
We investigated patients with a primary diagnosis of peripheral artery disease (n = 69) and coronary heart disease (CAD; n = 520) at baseline and on changes in psychosocial risk factors (depression, anxiety, quality of life, negative and positive affect) during a cardiovascular rehabilitation program. Patients completed psychosocial questionnaires at the beginning and at discharge of a 12-week rehabilitation program. Depression and anxiety were measured with the Hospital Anxiety and Depression Scale (HADS), positive and negative affect with the Global Mood Scale, and health-related quality of life with the SF-36 Health Survey. Patients with PAD showed improvements in anxiety (p < 0.001), negative affect (p < 0.001) and bodily pain (p < 0.001). Patients with CAD reported significant improvements in all measured dimensions (all p-values < 0.001).
Keywords
Introduction
The participation in comprehensive cardiovascular rehabilitation programs is highly recommended as a means of secondary prevention in patients with cardiovascular disease.1,2 Based on the findings from recent meta-analyses,1,3 there is strong evidence for a reduced risk of re-infarction after myocardial infarction as well as reduced cardiovascular and all-cause mortality after participation in a cardiovascular rehabilitation program. Also, with respect to psychological risk factors, rehabilitation programs are beneficial, particularly with regard to increased quality of life, decreased depression and anxiety, 4 as well as decreased stress levels. 5 After participating in cardiovascular rehabilitation programs, feelings of energy are increased and fatigue is decreased. 6 Cardiac rehabilitation programs have become a key therapeutic element to improve quality of care in MI patients worldwide. 7
Most of these studies included patients with coronary artery disease (CAD).3,8 Reviewing the literature, Linden (2000) 9 concludes that patients with CAD profit from cardiac rehabilitation as well as in terms of psychological end points (e.g. depression). Very little is known about psychosocial outcomes in patients with peripheral artery disease (PAD) or in outcome differences between diagnostic groups, including those with PAD, referred to cardiovascular rehabilitation programs. 10 The positive impact of exercise-based interventions on quality of life in patients with PAD has recently been shown. 11 Another study compared patients with PAD and CAD during an outpatient rehabilitation program. 12 Main outcome measures were workload during a bicycle stress test and health-related quality of life. The authors found that both groups profited equally from the rehabilitation program.
PAD is a systematic atherosclerotic disease characterized by the occurrence of walking-induced pain. 13 Since PAD often leads to more functional impairments and disabilities 14 compared to CAD, these differences might be also reflected in the psychological functioning of the patients. Cross-sectional studies have shown significant relationships between severity of disease and psychological risk factors in patients with PAD, such as depression,15,16 anxiety 16 and type D personality. 13 Ruo et al. 14 showed that patients with PAD and depression had a greater annual decline in physical functioning than patients without depression. Accordingly, the reduction of psychological distress during rehabilitation programs might also be important in terms of benefiting the progression of the disease. The aim of this study was therefore to assess baseline levels as well as changes of psychosocial risk factors during a cardiovascular rehabilitation program in patients with PAD and CAD. We decided to examine each diagnostic group separately because of the differences in their recovery paths and thus refrained from directly comparing PAD with CAD patients. From a clinical perspective, differential knowledge about the recovery paths of PAD and CAD patients might inform rehabilitation programs about specific needs in terms of psychological treatments.
Methods
Study design and patient population
All patients participating in a comprehensive 12-week outpatient cardiovascular rehabilitation program at the Bern University Hospital, Switzerland, between January 2004 and December 2010 were enrolled consecutively. Before patients agreed to participate in the cardiac rehabilitation program, they received written information about the possible scientific use of the routinely collected data by administrative staff. All patients who agreed to participate provided written informed consent to the study protocol that was approved by the local ethical committee. Patients with a minimum of 2 weeks in cardiovascular rehabilitation were included if they suffered either from (a) angiographically confirmed coronary one-, two- or three-vessel disease (defined as a stenosis > 50%) (CAD patients) or (b) an angiographic stenosis of the lower extremity associated with relevant clinical impairment (PAD patients). Patients completed questionnaires for psychosocial risk factors at the beginning of and at discharge from cardiovascular rehabilitation. Eighteen patients were excluded due to concomitant cancer or chronic obstructive pulmonary disease. Medical and demographic data were obtained from hospital charts. Cardiologists performed physical exams before starting the program as well as at discharge of patients. A total of 69 patients with PAD and 520 patients with CAD were included.
Cardiovascular rehabilitation program
Patients participated in the outpatient cardiovascular rehabilitation program three times a week for a duration of 12 weeks. Exercise training was a major part of the program and consisted of aerobic endurance and strength training but it also included relaxation sessions. 17 Physical fitness (i.e. maximum exercise capacity) was measured by symptom-limited incremental exercise testing on a bicycle ergometer. In addition, pain-free and total walking distance was determined in PAD patients on a treadmill (speed of 3.2 km/h and an elevation of 12%). 15 Additionally, patients were educated about PAD or CAD related issues, such as medication, risk factor control or etiology. Patients underwent educational sessions in terms of dietary counseling, stress management and smoking cessation. Educational sessions comprised disease-specific information and were tailor-made for the different diagnostic groups.
Psychometric assessment
We used the German version of the 14-item Hospital Anxiety and Depression Scale (HADS) to measure the severity of depressive (HADS-D) and anxiety (HADS-A) symptoms. 18 Both of these subscales consist of seven items, each with a total range of 0–21. Internal consistency was good in our sample (HADS-D: Cronbach α = 0.80; HADS-A: Cronbach α = 0.84). The HADS does not consider somatic symptoms of depression, as they might evolve from an underlying somatic condition. Bjelland et al. 19 report cut-off values for HADS-D and HADS-A of 8 for somatic patients as well as in the general population.
Positive and negative affect were assessed with the German version of the Global Mood Scale (GMS). 20 The subscales ‘positive affect’ (e.g. cheerful, lively, dynamic) and ‘negative affect’ (e.g. fatigued, wearied, worn out) each consist of 10 mood items rated on a 5-point Likert scale (0 = not at all, 4 = extremely). Internal consistency in our sample was good for both subscales (positive affect Cronbach’s α = 0.92; negative affect Cronbach’s α = 0.91). The two-factorial structure of the GMS has been confirmed. 20
Health-related quality of life was measured with the German version of the SF-36 Health Survey.21,22 The 36 items reflect the eight scales: physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional and mental health. 22 Sometimes, the SF-36 is also described as a health status instrument. 22 As previously described, 23 each scale is computed by first transforming the raw scores into a range with a minimum of 0 and a maximum of 100 points, higher scores indicate better functioning. The eight subscales can be summarized in two sum scores. The mental and physical sum scores are computed by z-transforming these scores, multiplying them with American coefficients and summing them up. Finally, we t-transformed these scores, multiplying them by 10 and adding 50 to the product. Good reliabilities of the mental and the physical sum scores have been reported. 22
Statistical analysis
Data were analyzed using PASW 17.0 statistical software package (SPSS Inc., Chicago, IL, USA) and the significance level was set at p < 0.05 (two-tailed). Normal distribution was verified with the Kolmogorov–Smirnov test. When scores were not normally distributed, we applied non-parametric procedures. The two groups of CAD and PAD patients were compared on continuous and categorical variables, respectively, using an independent t-test, Mann–Whitney test and chi-squared test.
We applied a dependent group t-test to compare psychosocial scores before and after cardiac rehabilitation. In order to adjust for multiple comparisons, only p-values < 0.0036 were deemed to be statistically significant. Effect sizes are expressed as Cohen’s d, where 0.2, 0.5, and 0.8 mean small, medium, and large effects in clinical terms, respectively. 24
Results
Sample description
Table 1 shows the characteristics of PAD and CAD patients at baseline. Groups differed in terms of age, sex and education. Patients with PAD reported hypertension and smoking more frequently, whereas patients with CAD had higher levels of body mass index (BMI), greater exercise capacity, and more frequent use of beta blockers and statins. Patients with CAD reported higher levels of anxiety, higher levels of negative affect and lower levels of positive affect. PAD patients showed higher levels in role-physical, vitality, social functioning, role-emotional, mental health as well as in the mental health sum score.
Baseline data for patients with peripheral artery disease and coronary artery disease.
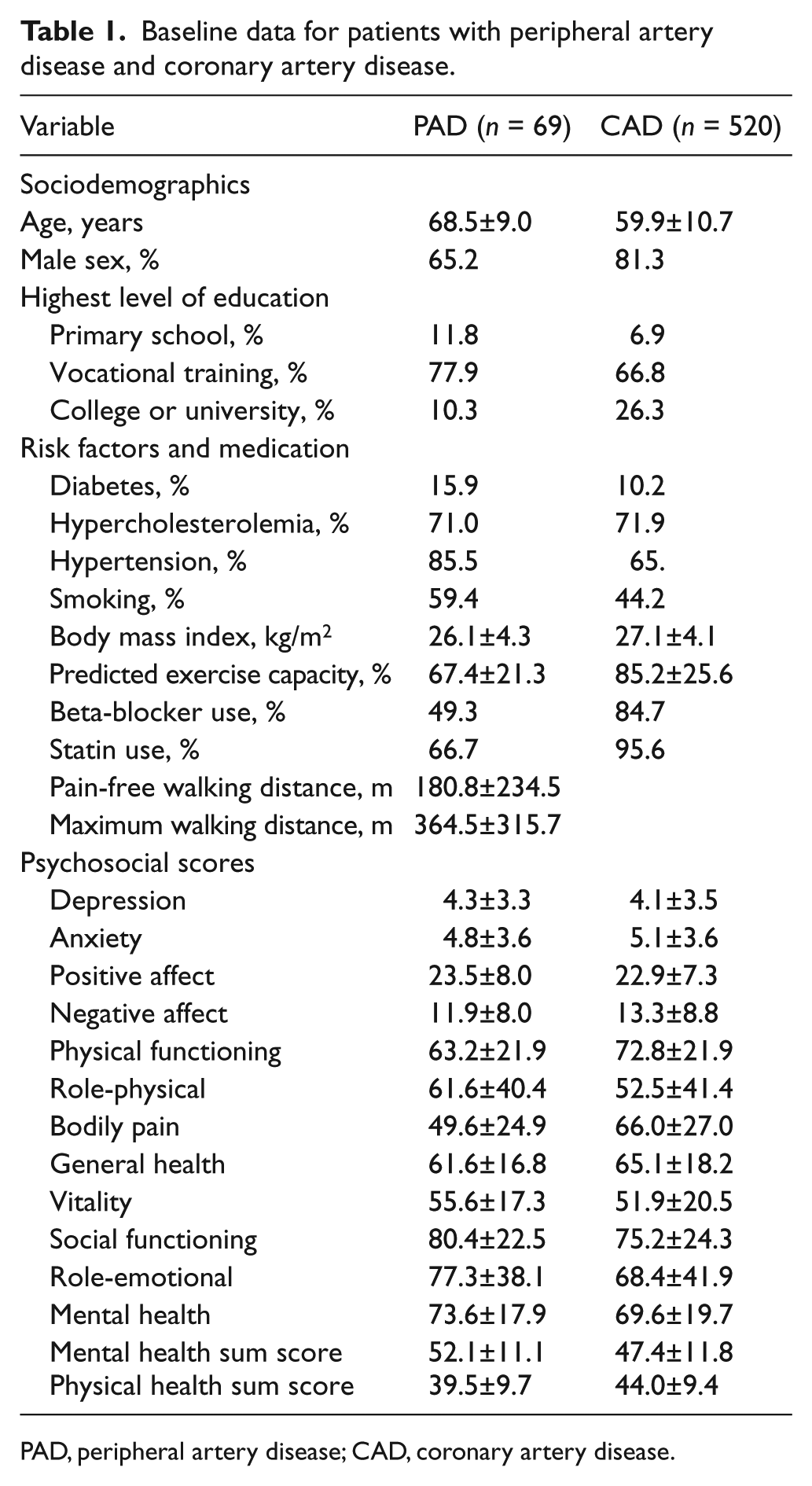
PAD, peripheral artery disease; CAD, coronary artery disease.
Pre/post comparison of PAD and CAD patients
Change of psychosocial risk factors in PAD patients (Table 2)
The pain-free (p<0.05) and maximum walking distance (p<0.001) increased significantly during rehabilitation. Furthermore, pre/post comparisons in PAD patients showed a significant decrease in BMI (p<0.001). Patients with PAD showed significant improvements in anxiety (p<0.001, d = 0.49), and positive (p=0.02, d = 0.32) and negative affect (p<0.001, d = 0.48) with medium effect sizes. In terms of health-related quality of life, PAD patients showed a significant increase in the subscale bodily pain (p<0.001) with a medium effect size (d = 0.41). All other dimensions of quality of life showed no significant change during rehabilitation after adjusting for multiple comparisons.
Pre- and post-cardiovascular rehabilitation program comparison for patients with peripheral artery disease.
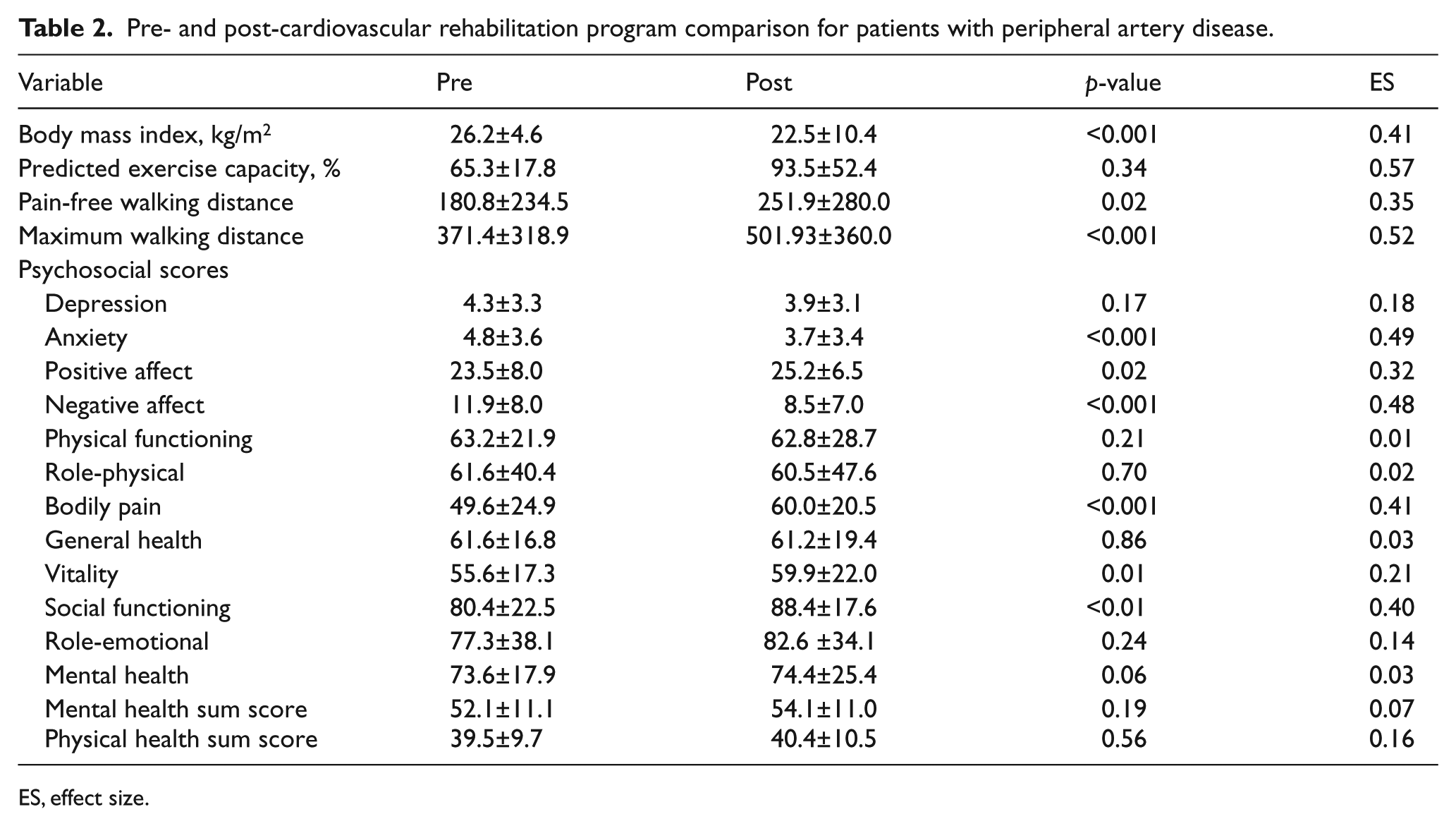
ES, effect size.
Change of psychosocial risk factors in CAD patients (Table 3)
Among patients with CAD, maximum exercise capacity increased during rehabilitation (p<0.001) with a large effect (d = 0.92). BMI was significantly reduced (p<0.001) but the effect was negligible (d = 0.03). Improvements in psychosocial risk factors were reported in all measured dimensions (all p-values <0.001). Large effect sizes emerged for improvements in negative affect (d = 0.65), physical functioning (d = 0.59) and the physical health sum score (d = 0.55).
Pre- and post-cardiovascular rehabilitation program comparisons for patients with coronary artery disease.
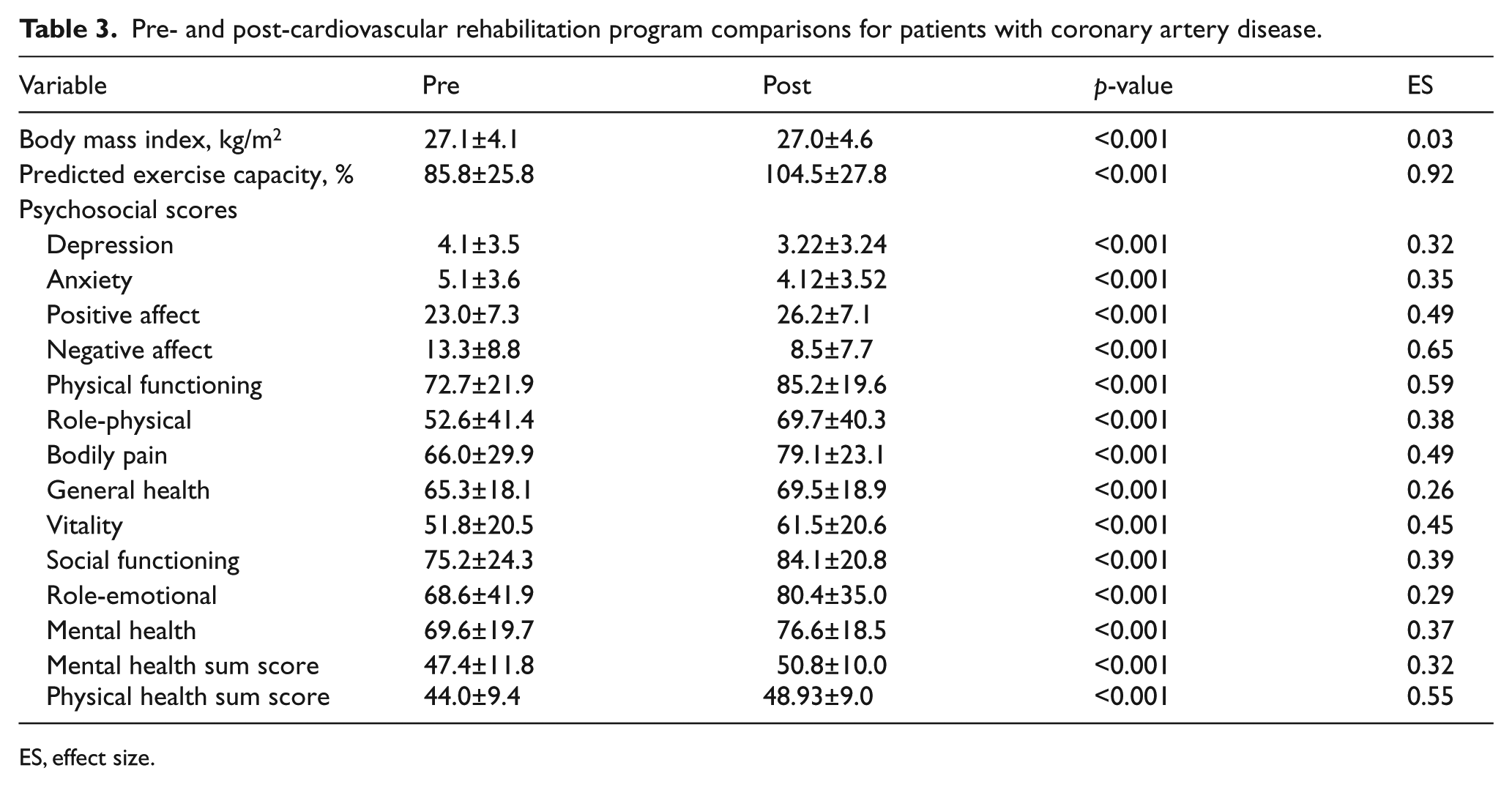
ES, effect size.
Discussion
We found a significant decrease in depressive symptoms from pre to post assessment in patients with CAD but not in those with PAD, with effect sizes showing these findings were clinically meaningful. These results are of clinical importance because PAD patients with depressive symptoms often fail in revascularization, which impacts the prognosis, and they also suffer from greater functional impairments.14,25–27 Chronic forms of depression especially are related to a decline of functional capacity in patients with PAD. 14 These results might also be explained by the overlap of walking-related impairments and functional disabilities with depressive symptoms in PAD patients. 28 With regard to CAD patients, our results support previous studies showing a decrease of depressive symptoms during rehabilitation.29,30 Improving depression was not a specific target of cardiovascular rehabilitation. However, the rehabilitation program confers a high amount of physical exercise that might be expected to alleviate depressive symptoms in its own right. 31 Therefore, one might speculate that depressive symptoms were less responsive to the program in PAD patients than was seen for functional impairments. Furthermore, Thomas et al. 32 propose a bi-directional relationship between depression and vascular disease, which might explain how PAD increases depression and vice versa. That study found that depression itself induces or worsens vascular disease, which is related to the concept of ‘vascular depression’. Furthermore, it may be hypothesized that patients with PAD suffer from more chronic forms of depression, which might explain the small responsiveness of depression in rehabilitation programs. Some stability of depressive mood in patients with PAD was also shown by Smolderen et al. 33 during an observation period of 18 months. Future research is needed to find possible disease-specific aspects in PAD patients with regard to depressive mood.
In terms of changes in anxiety, positive affect, and negative affect, patients with PAD, as well as those with CAD, profited from the cardiac rehabilitation program. Except for positive affect, both patient groups showed small to medium effect sizes for these improvements. Previous studies found that anxiety was reduced after 12 weeks of cardiovascular rehabilitation in patients with CAD.34,35 However, our study is the first to show that anxiety significantly decreases in patients with PAD during cardiovascular rehabilitation. This observation is clinically meaningful for both patient groups, as anxiety has been related to adverse health outcomes in patients with cardiovascular disease. 36
Across all dimensions of quality of life, CAD patients showed consistently significant improvements during the rehabilitation program. In patients with PAD, the results were less consistent. Significant improvements were only found in the dimensions bodily pain and social functioning, whereas no significant changes were seen in the other dimensions.
Health-related quality of life is an important measure for functional status from a patient’s perspective and has been shown to be predictive for prognosis in patients with CAD. 37 Another study showed that in patients with PAD, quality of life was associated with leg-related symptoms, whereas in patients with CAD, quality of life was related to cardiac symptoms. 38 Because symptoms of PAD constantly attract a patient’s attention in daily life in terms of pain or functional impairments while walking, self-efficacy might be decreased through a perceived lack of control.39,40 The improvements in PAD patients’ bodily pain might originate from an increase in the maximum and pain-free walking distance. These disease-specific characteristics might account to some extent for the health-related quality of life in patients with PAD. On the other hand, patients with myocardial infarction have a much better chance to become pain free after a coronary intervention and rehabilitation.41,42 It is important to mention that the effect of the rehabilitation program with regard to quality of life and pain-related symptoms in particular might also depend upon whether patients have been revascularized.
At baseline, patients with CAD reported higher levels of negative affect as well as anxiety compared to patients with PAD. Our results concur with a prior study that showed differences among three diagnostic groups referred to cardiovascular rehabilitation. 10 In that study, part of which also included patients from the present investigation, patients with PAD reported lower levels of depression and vital exhaustion than patients with CAD or chronic heart failure after adjusting for covariates.
The present study has several limitations. We enrolled patients who completed the program and who were capable and willing to participate in outpatient cardiovascular rehabilitation, which may seem a selected population. It is possible that non-participants had a higher symptom burden than participants. The two patient groups differed in their sample size, which affects the level of statistical significance, thereby making a direct group comparison on changes in psychosocial scales problematic. Therefore, we provide effect sizes as a measure of clinical relevance for the changes within each patient group. Unfortunately, we were unable to show data concerning the ankle–brachial index (ABI). We did not control for comorbidities, which also might affect patients’ health or psychosocial aspects.
In conclusion, our study showed that patients with CAD had reliable and clinically meaningful changes towards improvements in their psychosocial risk profile. Improvements in patients with PAD were less consistent, although the walking distance improved. Future studies with larger samples are needed to clarify possible moderating variables which might explain these differences. Given that PAD patients exhibit a disadvantage with regard to elevated psychosocial risk when compared to patients with CAD, cardiovascular rehabilitation might consider disease-specific aspects in addressing psychosocial risk factors.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.