
Abstract
Aortic manipulation releases embolic material, thereby enhancing the probability of adverse neurologic outcomes following coronary artery bypass grafting (CABG). We prospectively evaluated 59 patients undergoing CABG. Patients in the single (SC, n = 37) and multiple clamp (MC, n = 22) groups were comparable in relation to age and operative risk (p > 0.05). Neurocognitive evaluation consisted of the Auditory Verbal Learning Test (AVLT), Color Trails Test A, the Grooved Pegboard test and the Mini-Mental State Examination. Data acquisition was performed preoperatively, early postoperatively and at the 4-month follow-up. Intraoperative transcranial Doppler (TCD) monitoring was used to quantify the embolic load in relation to different aortic clamping strategies. Preoperative neurocognitive results were similar between the groups (p > 0.05). The incidence of postoperative delirium was greater in the MC group but this failed to reach statistical significance (23% vs 8%, p = 0.14). SC patients had fewer embolization signals (270 ± 181 vs 465 ± 160, p < 0.0001). Early postoperative neurocognitive results were depressed in comparison to preoperative values in both groups (p < 0.05 for multiple comparisons). The magnitude of this cognitive depression was greater in the MC group (p < 0.05 for multiple comparisons). Preoperative levels of neurocognition were restored at follow-up in the SC group in all tests except the AVLT. A trend towards improvements in neurocognitive performances at follow-up was also observed in the MC group. Residual attention, motor skill and memory deficits were, however, documented with multiple tests. In conclusion, the embolic burden was significantly lower in the SC group. This TCD imaging outcome translated into fewer early cognition deficits and superior late restoration of function.
Keywords
Introduction
Loss of neurological integrity following cardiac surgery may become evident as either a new onset motor deficit or a reduction in neurocognitive performance. While the former is relatively rare it constitutes one of the most dreaded complications following coronary artery bypass grafting (CABG). In contrast to the relative rarity of stroke, postoperative cognitive dysfunction (POCD) is common in this setting and may present itself as a combination of deficits in fine motor function, attention, memory consolidation and psychomotor dexterity. 1 The etiology of POCD is not clearly defined, but a multifactorial genesis has been postulated. Embolic events, inflammation, hypoperfusion, cerebral edema and hyperthermia all likely play a role in the decline in neurocognitive performance that is seen in as many as 50–70% of cardiac surgical patients.1–5
Transcranial Doppler ultrasound (TCD) detects embolic events via enhancement of ultrasound reflection in comparison with the background signal caused by blood flow. 6 High-intensity transient signals (HITS) are the TCD equivalents of cerebral embolism. Contradictory observations on the correlation between HITS and POCD have been published. While certain publications enforce the notion that embolic signals detected on TCD exert an adverse impact on neurocognitive performance, others refute these findings.1,4,6–9 A major drawback of TCD is its inability to discriminate between solid particular emboli and micro-cavitational phenomena. 8 While the former harbor potential for inducing neurological impairment, the latter are clinically benign. This lack of specificity of transcranial Doppler ultrasound may account for the fact that HITS have not been unequivocally linked to inferior neurocognitive performances. A variety of different aspects of initiating and maintaining cardiopulmonary bypass (CPB) have been implicated in the generation of embolic material.7,8 Aortic manipulation plays a pivotal role in the release of showers of embolic material, which are visualized on TCD. 8
The mechanism by which emboli induce cerebral injury surpasses simple mechanical obstruction to involve activations of the inflammatory, complement and coagulation cascades. 10
We hypothesized that the recognition and quantification of the microembolic burden using transcranial Doppler may serve as a guide for improving the surgical technique of on-pump coronary revascularization.
Methods
Following the approval from our institutional ethics committee, 59 patients scheduled to undergo elective CABG using CPB were enrolled into our prospective observational study from July 2010 to May 2011. Exclusion criteria were concomitant valvular pathology that required surgery, emergent CABG, ejection fraction < 35%, atrial fibrillation, prior stroke or transient ischemic attack, significant carotid disease, inability or refusal to provide informed consent, poor TCD bone window and significant anxiety. While preoperative brain imaging was not a part of the study protocol, all patients underwent non-invasive carotid imaging. Patients in whom CABG was performed following a single aortic cross-clamp (SC) strategy comprised the SC group, whereas patients in whom a side-biting clamp was used for the construction of proximal anastomoses were included into the multiple clamp (MC) group. Patient recruitment into either group was based on surgeon discretion. All patients participating in this study signed an informed consent form prior to enrollment.
Perioperative management
The patients received diazepam and morphine 30 minutes prior to induction of anesthesia. Endotracheal tube, urinary catheter, as well as radial artery and pulmonary artery catheters were inserted. The anesthetic protocol included induction and maintenance of anesthesia with midazolam, fentanyl and pancuronium bromide. This was coupled with sevoflurane inhalation. The ascending aorta and right atrium were cannulated for CPB. Myocardial protection consisted of both antegrade and retrograde cardioplegia. Systemic heparinization aiming at an activated clotting time (ACT) > 480 seconds was used, followed by full reversal with protamine after decannulation. Tepid CPB was employed, targeting the flow at 2.2 L/min/m2. The target mean arterial pressure during CPB was 60 mmHg. If necessary, norepinephrine was employed to reach the aimed blood pressure. The distal coronary anastomoses were performed on an arrested heart, during a single period of aortic cross-clamping. Patients in the SC group had their proximal aortic anastomoses constructed during the period of aortic cross-clamping. The aortic cross-clamp was universally applied at the distal ascending aorta, below the level of the innominate artery. Conversely, the proximal anastomoses were constructed with the aorta partially occluded with a side-biting clamp in the MC group. The side-clamp was applied to the right lateral aspect of the ascending aorta, with the CPB flows temporarily reduced during the actual clamp placement. Patients in the SC group suffered less aortic manipulation, at the expense of prolonging the cross-clamp time. Weaning from CPB was initiated once the patient’s rhythm had stabilized and normothermia had been achieved. Inotropic support was initiated in order to maintain a cardiac index greater than 2.2 L/min/m2.
Transcranial Doppler ultrasound
Transcranial Doppler ultrasound was used for the bilateral detection of embolic signals in both middle cerebral arteries (Sonara TCD System; Viasys Healthcare, Inc., Conshohocken, PA, USA). Two 2-MHz probes were used for bilateral data acquisition. Both middle cerebral arteries were insonated at the depth of 55 mm with a sample volume of 7 mm. An offline analysis and quantification of the HITS was performed by an independent vascular neurologist blinded to the patient group allocation. Every effort was made to visually and audibly differentiate between artifacts and true HITS phenomena according to pre-specified criteria with an intensity threshold of 7 dB.11,12 Data acquisition started before aortic cannulation and ended 5 minutes after aortic decannulation. All aortic manipulation events within that time interval were recorded.
Neurocognitive testing
A uniform battery of neurocognitive tests was utilized to quantify each individual patient’s performance preoperatively (PRE), at postoperative day 7 (POD 7) and at a 4-month follow-up. It consisted of the Rey Auditory Verbal Learning Test (AVLT), Color Trails Test A (CTT), Grooved Pegboard test (GP) and the Mini-Mental State Examination (MMSE). In order to reduce the impact of anxiety on a patient’s neurocognitive performance, the State Trait Anxiety Inventory Test (STAI) was employed.13,14 STAI is an instrument designed to assess the level of anxiety, which may be an independent confounder when evaluating neurocognitive outcomes. Patients with a STAI score greater than 40 were excluded from the study.
AVLT is a commonly used instrument for testing the individual’s capacity to assess short-term memory, resistance to interference and memory consolidation.15,16 In brief, it involves a five-trial presentation of a 15-noun list of words, followed by a single presentation of a 15-noun interference list and concludes with a two-trial post-interference recall. Patients are expected to repeat as many items as they can remember at different time intervals and after hearing an interfering list. Deficits in attention, psychomotor speed and mental flexibility were monitored with the CTT. The test requires the participant to connect numbered colored circles in as short a time interval as possible. The GP test is designed to assess fine motor skills and requires complex visual–motor coordination. Bilateral manual dexterity is determined by the time it takes to complete the designated task. 17 The neurocognitive evaluation was completed with the MMSE. It is a questionnaire-based test aimed to evaluate arithmetic problem resolution, language comprehension and basic motor skills. Clinicians blinded to patient group assignment performed all neurocognitive tests.
Statistical analysis
The data are presented as mean value ± standard deviation or median followed by the interquartile range for variables with a distribution that is not normal. Longitudinal comparisons among samples of the same subject were analyzed using the Wilcoxon matched pairs test. Analyses between different groups of patients were performed using the Mann–Whitney U-test. A p < 0.05 was considered to be of statistical significance. The differences in categorical variables between the two groups were processed using Fisher’s exact test. The data were processed using the Statistica software package (StatSoft Inc., Tulsa, OK, USA).
Results
The patient demographic data and preoperative characteristics are presented in Table 1. The two patient cohorts were well matched with respect to the severity of their cardiac pathology as well as to the commonly observed comorbidities. Patients with hypertension had inferior GP scores preoperatively in comparison to normotensive ones (right hand: 118 ± 24 vs 96 ± 21, p = 0.007; left hand: 130 ± 29 vs 99 ± 22, p = 0.002). Similarly, 4-month follow-up testing revealed that hypertensive patients retained inferior motor skills in comparison to normotensive patients (right hand: 123 ± 28 vs 96 ± 23, p = 0.003; left hand: 136 ± 34 vs 102 ± 25, p = 0.002). Furthermore, inferior follow-up CTT results were noted in hypertensive patients (93 ± 31 vs 74 ± 20, p = 0.04). The studied groups were well matched with regard to hypertension (84% in SC group vs 77% in MC group, p = 0.73). The effect of hyperlipidemia on neurocognitive function was less pronounced in our study. The only statistically significant comparison between patients with and without hyperlipidemia was in the preoperative CTT group (89 ± 27 vs 73 ± 16, p = 0.05). Again, the distribution of hyperlipidemic patients was uniform among the groups (81% in the SC group vs 77% in the MC group, p = 0.75). Perioperative data are summarized in Table 2. Patients in the SC group had longer aortic cross-clamp times, consistent with the strategy of performing proximal anastomoses during one period of aortic occlusion (67 ± 23 vs 44 ± 15, p < 0.0001). Discharge medications included beta-blockers, aspirin and 3-hydroxy-3-methylglutaryl-coenzyme A reductase inhibitors in all patients. Postoperative delirium was defined in accordance with the Society of Thoracic Surgeons’ definition as an acute state characterized by illusions, confusion, cerebral excitement, and having a comparatively short course. 18 Its incidence was greater in the MC group, and while this difference trended towards statistical significance it failed to reach it (23% vs 8%, p = 0.14). There was one stroke in the MC group. The motor deficit in this patient correlated with the computed tomographic brain imaging data. No other patient was found to have neurologic symptoms requiring brain imaging. One patient in the SC group died. The cause of death was massive pulmonary embolism despite adequate anticoagulation in a patient with antiphospholipid syndrome who had two preoperative episodes of pulmonary embolism. The total number of HITs on TCD representative of embolic events was statistically significantly higher in the MC group of patients (465 ± 160 vs 270 ± 181, p < 0.0001). The increase in the total number of embolic events in patients in the MC group is reflective of the cumulative effect of multiple aortic manipulations. Each such aortic manipulation harbors potential to release embolic showers. A more detailed description of the embolic potential of various manipulations during the revascularization procedure is given in Table 3. A number of interventions unrelated to aortic manipulation also have the potential to provoke embolic signals on TCD. These include defibrillation, heart manipulation, blood sampling and drug infusions.19,20 Embolic events related to these types of interventions, in addition to those of unknown origin, were also accumulated and presented in Table 3.
Preoperative patient characteristics.
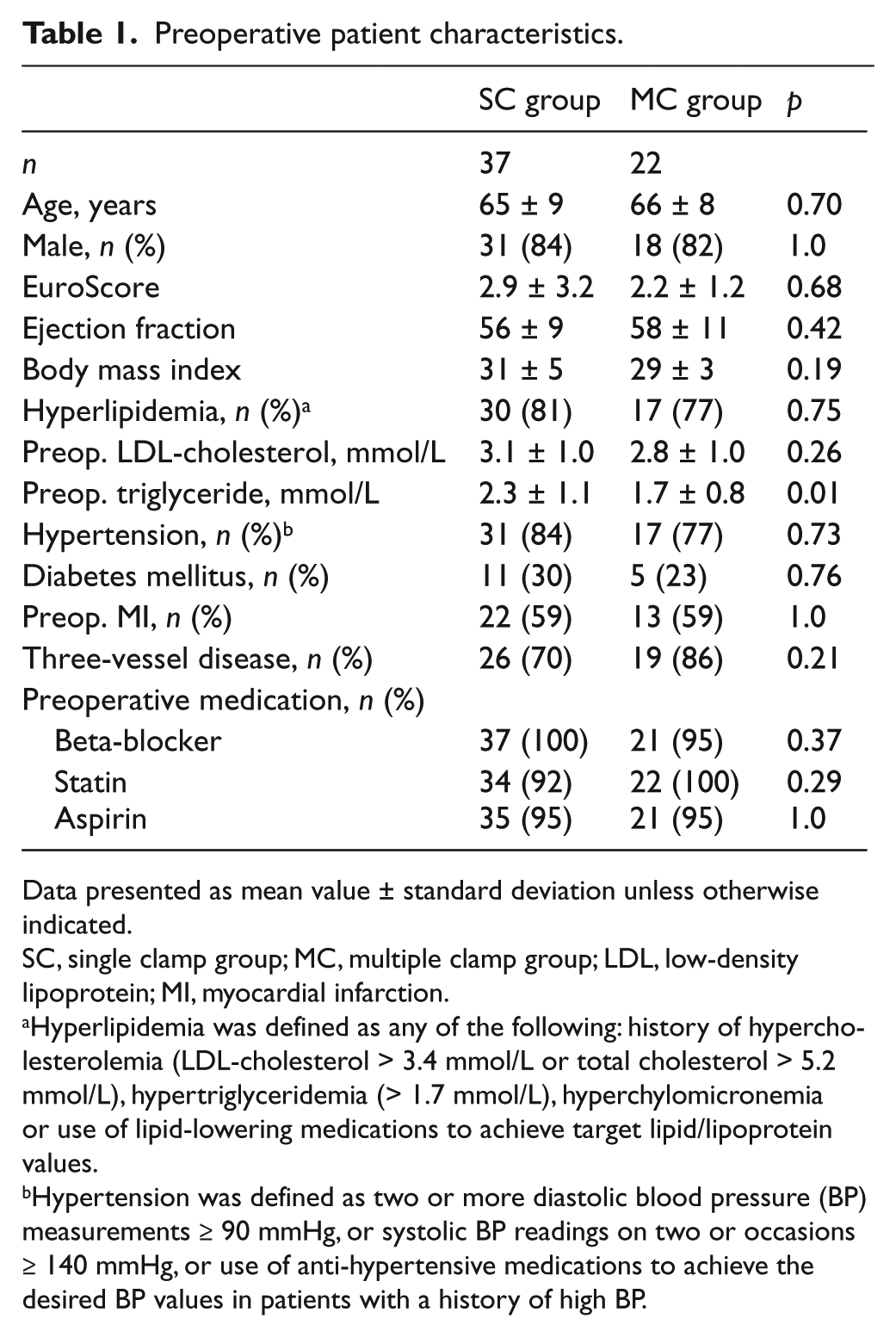
Data presented as mean value ± standard deviation unless otherwise indicated.
SC, single clamp group; MC, multiple clamp group; LDL, low-density lipoprotein; MI, myocardial infarction.
Hyperlipidemia was defined as any of the following: history of hypercholesterolemia (LDL-cholesterol > 3.4 mmol/L or total cholesterol > 5.2 mmol/L), hypertriglyceridemia (> 1.7 mmol/L), hyperchylomicronemia or use of lipid-lowering medications to achieve target lipid/lipoprotein values.
Hypertension was defined as two or more diastolic blood pressure (BP) measurements ≥ 90 mmHg, or systolic BP readings on two or occasions ≥ 140 mmHg, or use of anti-hypertensive medications to achieve the desired BP values in patients with a history of high BP.
Perioperative summary of data for patients in both the single clamp (SC) and multiple clamp (MC) groups.
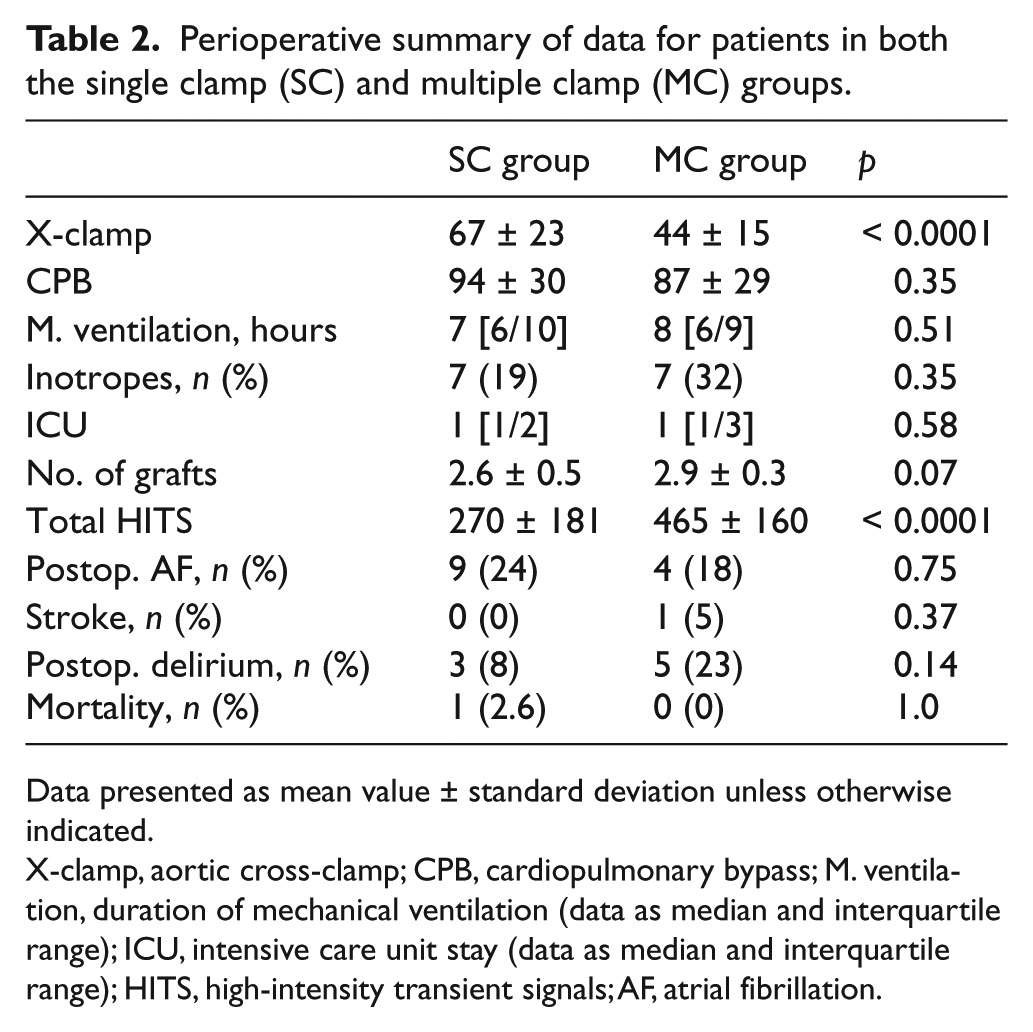
Data presented as mean value ± standard deviation unless otherwise indicated.
X-clamp, aortic cross-clamp; CPB, cardiopulmonary bypass; M. ventilation, duration of mechanical ventilation (data as median and interquartile range); ICU, intensive care unit stay (data as median and interquartile range); HITS, high-intensity transient signals; AF, atrial fibrillation.
Microembolic signals detected on transcranial Doppler examination at various stages of CABG. The number of microembolic signals summarized in the table is an aggregate from both the left and right TCD probes.
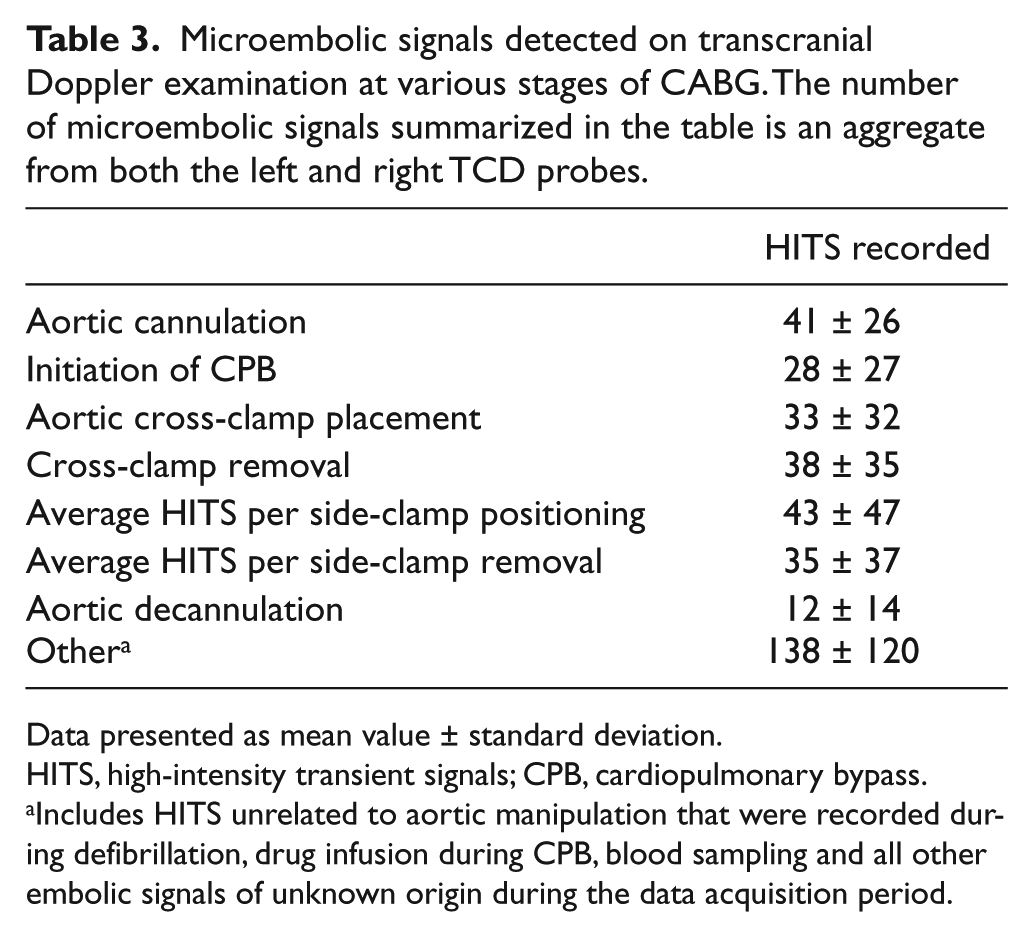
Data presented as mean value ± standard deviation.
HITS, high-intensity transient signals; CPB, cardiopulmonary bypass.
Includes HITS unrelated to aortic manipulation that were recorded during defibrillation, drug infusion during CPB, blood sampling and all other embolic signals of unknown origin during the data acquisition period.
The adverse impact of cardiac surgery on the early postoperative neurocognitive performance was seen in both groups on almost all evaluators (Tables 4 and 5). The amplitude of the relative reduction in early neurocognitive performance, however, was observably greater in the MC group (Table 6; p < 0.05 for multiple comparisons). More specifically, early cognitive outcomes were worse in the MC group, when compared to the SC group, in multiple trials of the Rey AVLT, as well as CTT, bilateral GP tests and MMSE. At the 4-month follow-up, a universal trend toward improvement of cognitive performance was seen in both groups. This restoration of neurocognition reached preoperative levels in the SC group of patients as evaluated by the CTT, GP test and MMSE (Table 4). Residual deficits at the 4-month follow-up in the SC group were noted only in the Rey AVLT, indicating a persistent problem with memory consolidation (Table 4). Conversely, three of the four neurocognitive tests employed in the current study showed significant residual depression of performance in memory acquisition, attention and fine motor skills in the MC cohort of patients (Table 5).
The neurocognitive outcome of the single clamp (SC) cohort of patients.
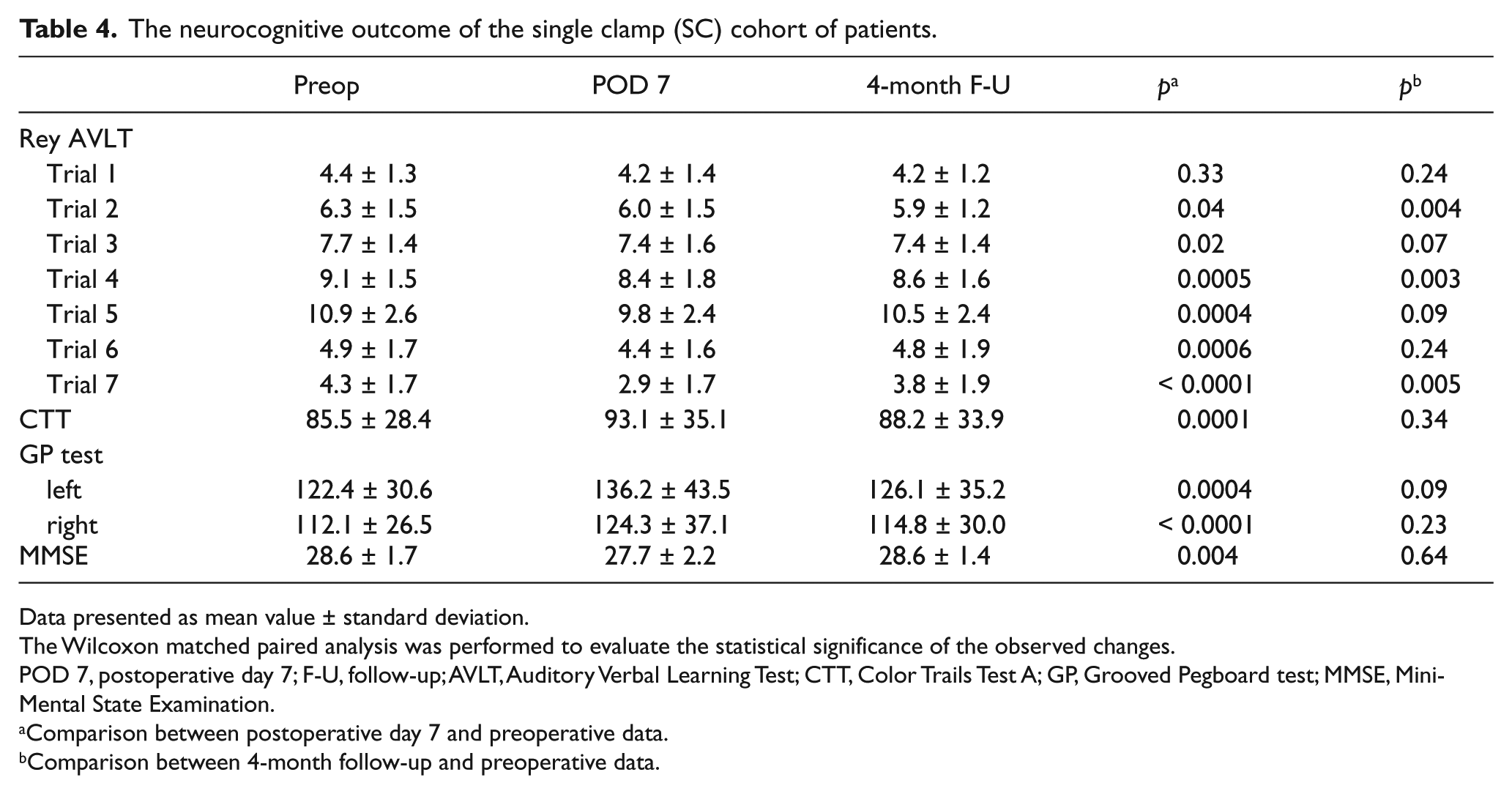
Data presented as mean value ± standard deviation.
The Wilcoxon matched paired analysis was performed to evaluate the statistical significance of the observed changes.
POD 7, postoperative day 7; F-U, follow-up; AVLT, Auditory Verbal Learning Test; CTT, Color Trails Test A; GP, Grooved Pegboard test; MMSE, Mini-Mental State Examination.
Comparison between postoperative day 7 and preoperative data.
Comparison between 4-month follow-up and preoperative data.
The neurocognitive outcome of the multiple clamp (MC) cohort of patients.
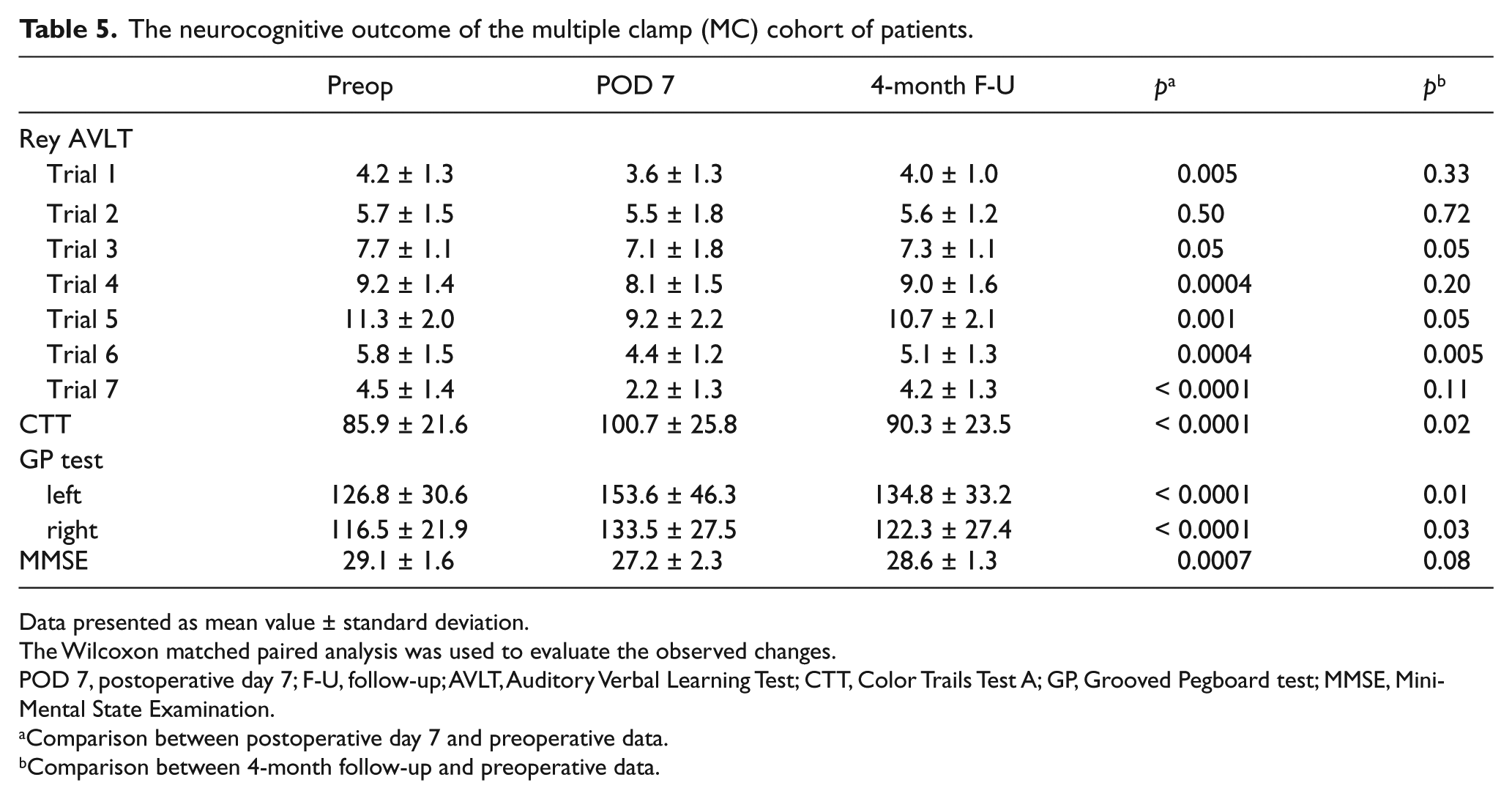
Data presented as mean value ± standard deviation.
The Wilcoxon matched paired analysis was used to evaluate the observed changes.
POD 7, postoperative day 7; F-U, follow-up; AVLT, Auditory Verbal Learning Test; CTT, Color Trails Test A; GP, Grooved Pegboard test; MMSE, Mini-Mental State Examination.
Comparison between postoperative day 7 and preoperative data.
Comparison between 4-month follow-up and preoperative data.
The relative reductions in postoperative neurocognitive outcomes in comparison to preoperative values for the single clamp (SC) and multiple clamp (MC) groups.
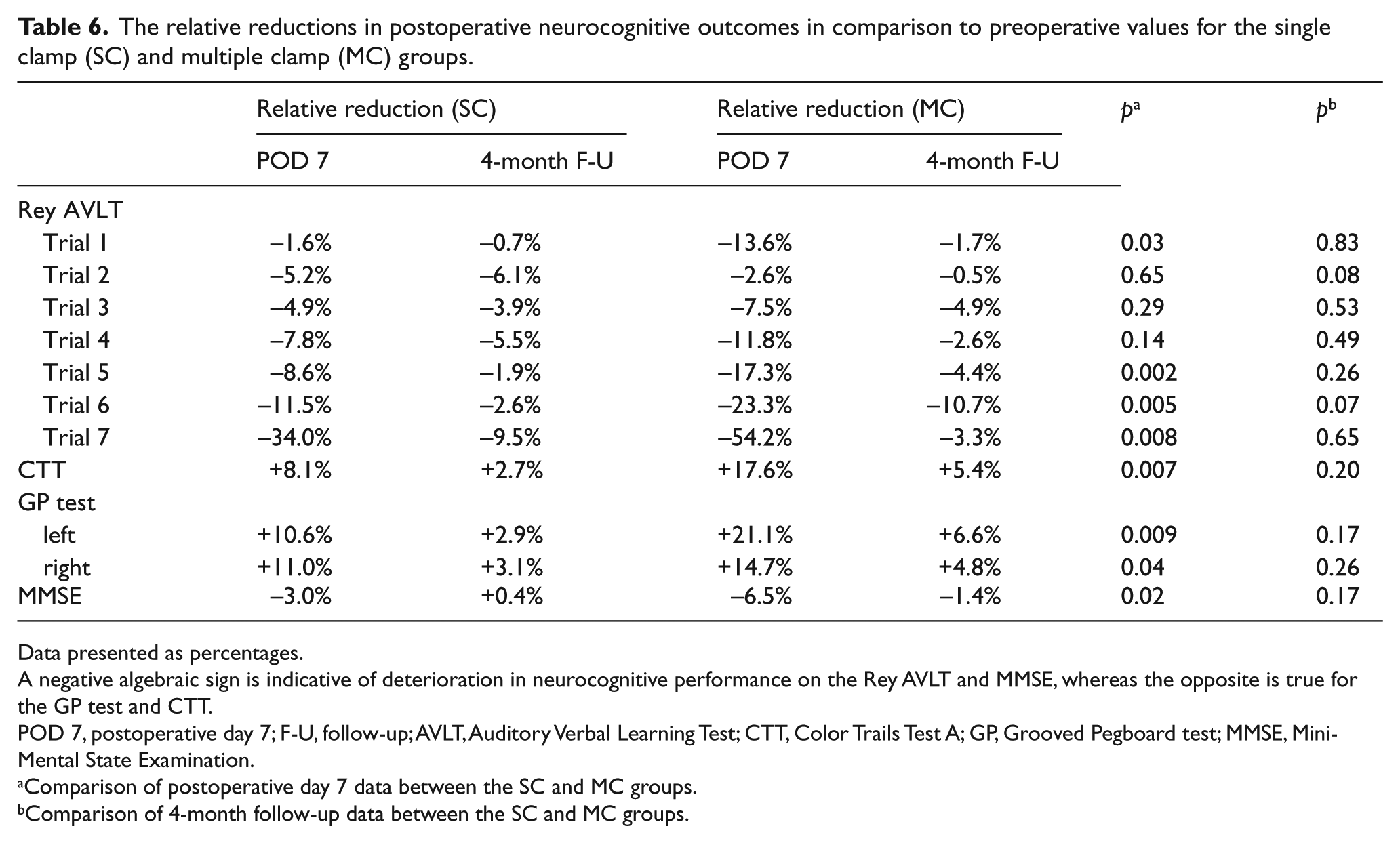
Data presented as percentages.
A negative algebraic sign is indicative of deterioration in neurocognitive performance on the Rey AVLT and MMSE, whereas the opposite is true for the GP test and CTT.
POD 7, postoperative day 7; F-U, follow-up; AVLT, Auditory Verbal Learning Test; CTT, Color Trails Test A; GP, Grooved Pegboard test; MMSE, Mini-Mental State Examination.
Comparison of postoperative day 7 data between the SC and MC groups.
Comparison of 4-month follow-up data between the SC and MC groups.
The correlation of the number of HITS with neurocognition is depicted in Table 7. The strongest correlation between the number of embolic signals and inferior cognitive performances was seen in the attention and fine motor skill domains.
The Spearman correlation analysis between the total number of embolic signals and various aspects of neurocognition.
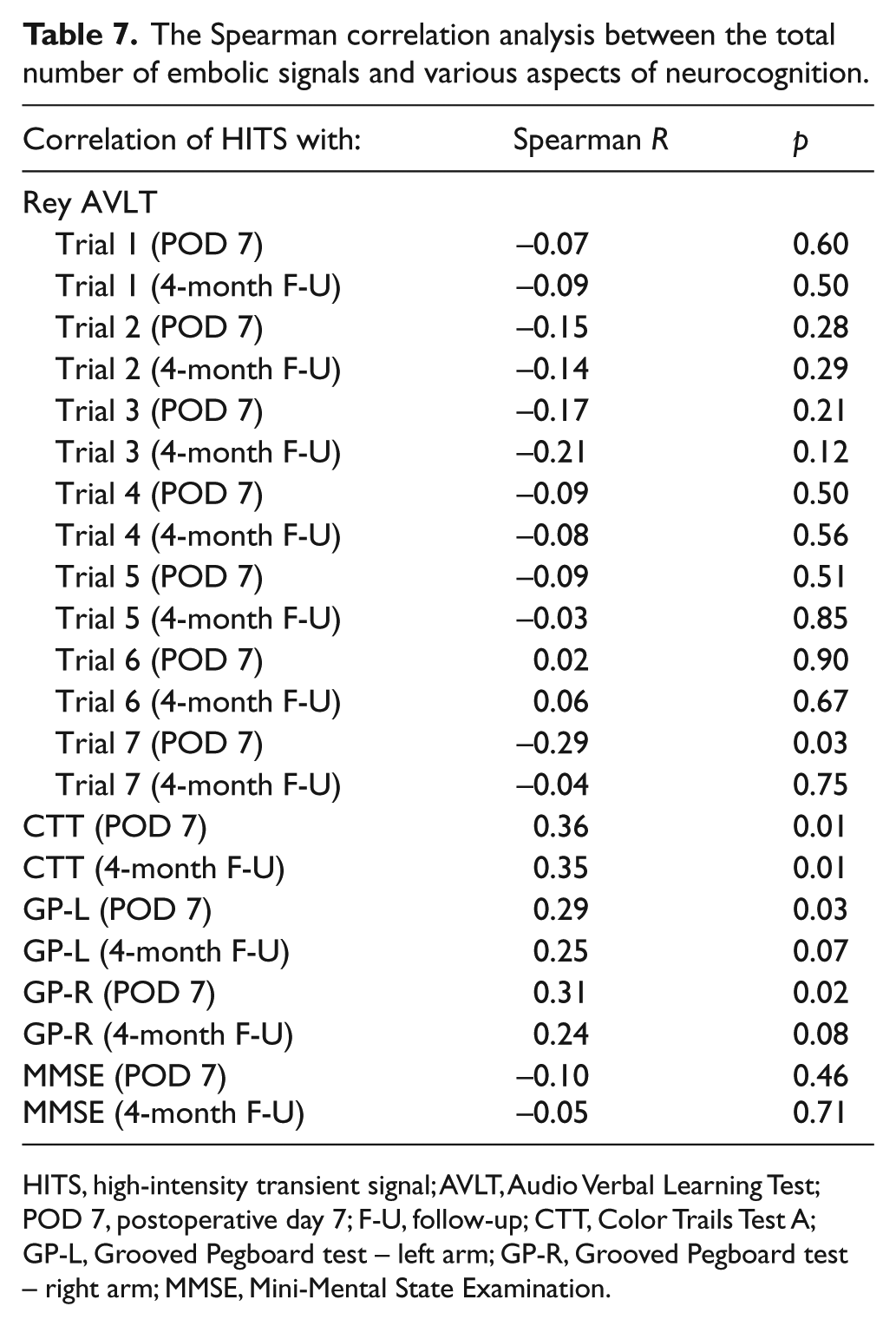
HITS, high-intensity transient signal; AVLT, Audio Verbal Learning Test; POD 7, postoperative day 7; F-U, follow-up; CTT, Color Trails Test A; GP-L, Grooved Pegboard test – left arm; GP-R, Grooved Pegboard test – right arm; MMSE, Mini-Mental State Examination.
Discussion
Postoperative neurocognitive dysfunction following cardiac surgical procedures is a commonly seen problem affecting as many as 50–70% of patients. 1 While neurocognitive impairment remains much less feared than the motor deficits associated with stroke, it still significantly prolongs hospitalization and impacts on quality of life. 1 Neurologic sequelae following cardiac surgery stem from a variety of possible culprits, and these include embolism, hypoperfusion, inflammation and cerebral edema. Reducing mortality and improving neurologic outcomes remain the two most important benchmarks in contemporary cardiac surgical practice. Our study focused on the dissimilar embolic potentials of two different aortic manipulation strategies during surgical myocardial revascularization. We hypothesized that the strategy of aortic manipulation during CABG is paramount to postoperative neurocognitive outcomes. The single clamp CABG strategy has shown capacity to improve neuropsychological results and reduce the incidence of motor deficits.21,22 We have demonstrated that every form of surgical trauma to the aorta led to a systemic release of embolic material that produced microembolic signals on transcranial Doppler. Reducing aortic manipulation consistently reduced the number of embolic showers detected on TCD. The pivotal disadvantage of the multiple clamping strategy of coronary revascularization lies in the fact that individual aortic manipulations produce a cumulative embolic effect. The present study showed that cardiac surgery adversely influenced early neurocognitive performance in both groups of patients. The magnitude of early cognitive depression was invariably greater in the MC group, and likely parallels the increased amount of aortic trauma inherent to that type of revascularization. We have found a statistically significant correlation between the number of embolic events on TCD and inferior neurocognitive outcomes. Patients in whom a single clamp strategy of revascularization was pursued demonstrated better early postoperative results in learning and memory consolidation domains, and had fewer attention deficits coupled with significantly better fine motor skills. The cognitive performance significantly improved in both groups of patients, across almost the entire spectrum of tests utilized in this study at the 4-month follow-up when balanced against the early postoperative results.
Cognitive dysfunction after cardiac surgery stems from multiple factors. In addition to embolic events, cerebral edema, hyperthermia and CPB duration are likely contributors to the problem. Isolated reports notwithstanding, off-pump coronary artery bypass surgery (OPCAB) has failed to reliably reduce the incidence of neurocognitive impairment in comparison to the conventional method utilizing CPB. 23 Conventional OPCAB does not eliminate aortic manipulation as the proximal anastomoses are still created to the aorta in most cases. The dogma that any surgical trauma to the aorta influences the embolic burden of the procedure may lead to a more liberal use of techniques that completely avoid aortic manipulation. One procedure that may rise to the challenge is total arterial OPCAB revascularization utilizing the aortic no-touch strategy. This technique, however, is not likely to ever become universally applicable to all patient populations, nor is it without its own specific shortcomings.
The limitations of the study stem from its non-randomized design, which may bring into focus surgeon bias as a factor. This is, however, unlikely to be of major concern since the surgeons pursuing single clamp revascularization perform it unselectively to all their patients. The same holds true for surgeons who prefer multiple clamping of the aorta. Each individual surgeon invariably used only one of the techniques. The other limitation of the study stems from an important TCD drawback: transcranial Doppler cannot reliably dichotomize embolic signals into those that bear clinical relevance and those that do not.
In summary, minimizing aortic manipulation is the principal idea of the single cross-clamp CABG strategy and is reflected in our study by a lower incidence of cerebral embolic events. The clinical correlate of pursuing this surgical technique is the improvement in early neurocognitive outcomes and more complete restoration of cognitive function at mid-term follow-up.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or non-profit sectors.