
Abstract
Introduction
Carotid atherosclerotic disease is a known independent risk factor of post operative stroke after coronary artery bypass grafting (CABG). The best management of concomitant coronary artery disease and carotid artery disease remains debated. Current strategies include simultaneous carotid endoarterectomy (CEA) and CABG, staged CEA followed by CABG, staged CABG followed by CEA, staged transfemoral carotid artery stenting (TF-CAS) followed by CABG, simultaneous TF-CAS and CABG and transcarotid artery stenting.
Methods
We report our experience based on a cohort of 222 patients undergoing combined CEA and CABG surgery who come to our observation from 2004 to 2020. All patients with >70% carotid stenosis and severe multivessel or common truncal coronary artery disease underwent combined CEA and CABG surgery at our instituion. 30% of patients had previously remote neurological symptoms or a cerebral CT-scan with ischemic lesions. Patients with carotid stenosis >70%, either asymptomatic or symptomatic, underwent CT-scan without contrast media to assess ischemic brain injury, and in some cases, if necessary, CT-angiography of the neck and intracranial vessels.
Results
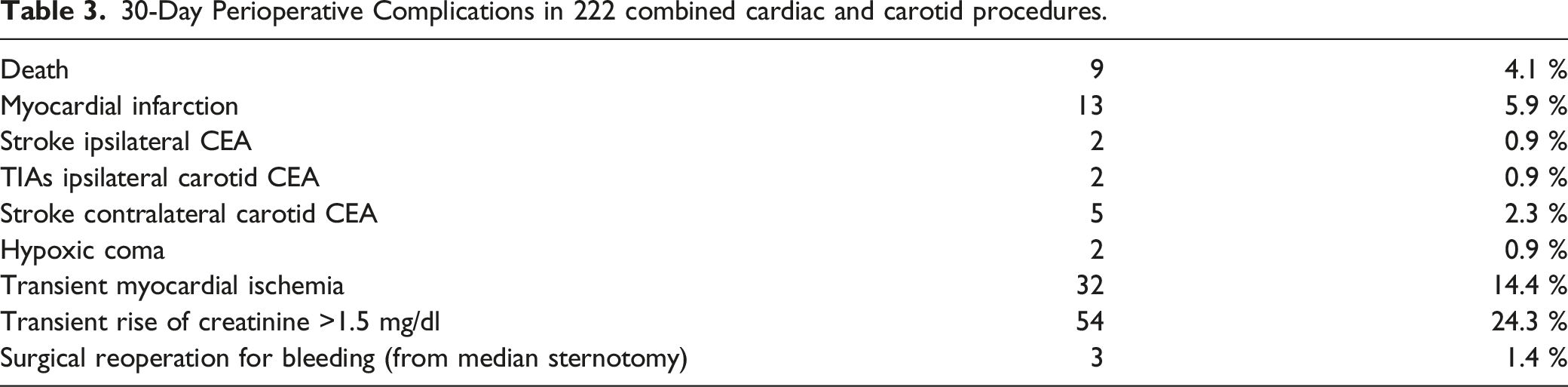
The overall perioperative mortality rate was 4.1% (9/222 patients). Two patients (.9%) had periprocedural ipsilateral transient ischemic attack (TIA) which completely resolved by the second postoperative day. Two patients (.9%) had an ipsilateral stroke, while 7 patients (3.2%) had a stroke of the controlateral brain hemisphere. Two patients (.9%) patients were affected by periprocedural coma caused by cerebral hypoperfusion due to perioperative heart failure. There were no statistically significant differences between patients in Extracorporeal Circulation (ECC) and Off-pump patients in the onset of perioperative stroke.
Conclusion
Our experience reported that combined surgical treatment of CEA and CABG, possibly Off-Pump, is a feasible treatment procedure, able to minimize the risk of post-operative stroke and cognitive deficits.
Introduction
Postoperative stroke is one the most important complication after coronary artery grafting (CABG) in patients with severe coronary disease. The rate of post-CABG stroke range between .5% and 7%.1,2 The etiology of post-CABG stroke is multifactorial. Carotid atherosclerotic disease is a known independent risk factor of post operative stroke after coronary revascularization.3,4 The risk of stroke after CABG surgery has been closely related to the degree of carotid stenosis.5, 6 However, the best management of concomitant coronary artery disease and carotid artery disease remains controversial. Current treatment options include simultaneous carotid endoarterectomy (CEA) and CABG, staged CEA followed by CABG, staged CABG followed CEA, staged transfemoral carotid artery stenting (TF-CAS) and CABG, and simultaneous TF-CAS and CABG. None of these procedures have been universally accepted.
We report our experience based on a large group of patients suffering from severe carotid stenosis and concomitant severe coronary artery disease through a combined approach of carotid CEA and CABG.
Materials and Methods
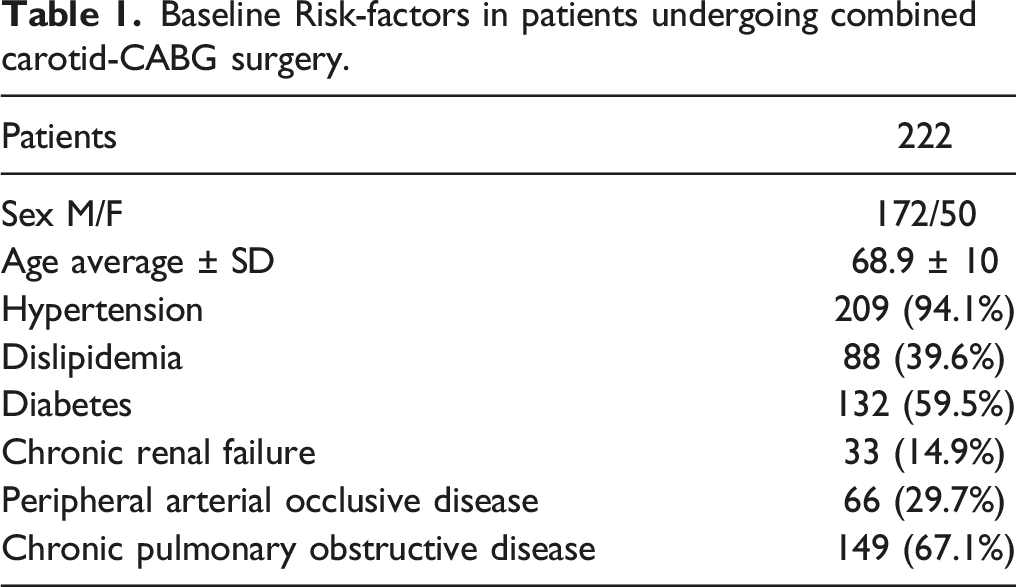
Baseline Risk-factors in patients undergoing combined carotid-CABG surgery.
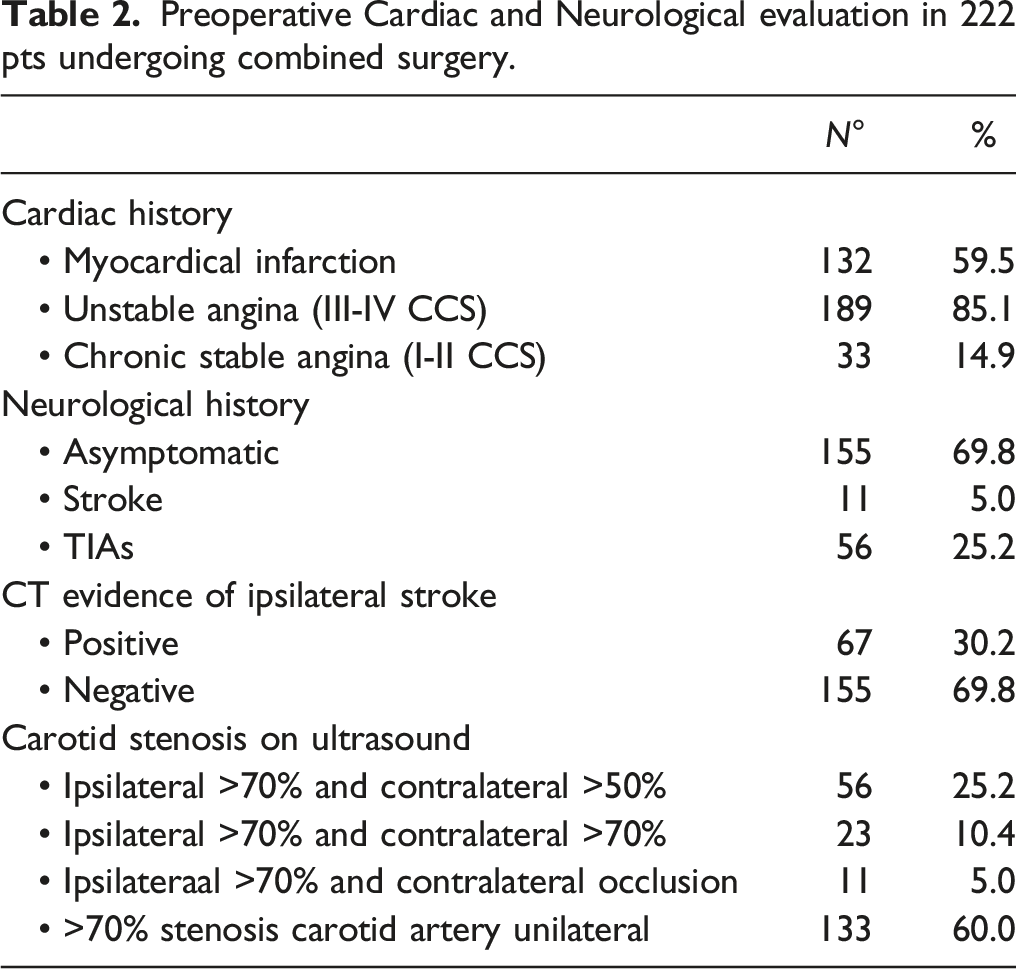
Preoperative Cardiac and Neurological evaluation in 222 pts undergoing combined surgery.
Surgical Treatment
All procedures were performed under general anesthesia with full invasive monitoring, before onset of cardiopulmonary bypass (CPB). In no cases was CEA performed using loco-regional anesthesia. 72 (32.5%) patients underwent off-pump bypass. Neurological assessment was monitored with near infrared refractory spectroscopy and stump pressure measurement with 40 mmHg threshold. In particular, the intra-operative neuromonitoring was performed by the INVOS™ system (Medtronic, Dublin, Ireland), so as to provide a continuous non-invasive measurement of cerebral oxygen saturation and a reliable indication of changes in cerebral perfusion.
Surgical dissection of the carotid arteries was usually completed while cardiac surgeons harvested the saphenous vein. All patients were anticoagulated with heparin 5000 IU before the carotid arteries were cross-clamped. During the CEA, carotid shunting was performed in 200 patients (90%) and all reconstructions were performed with bovine pericardium patch. After CEA, the neck wound was usually left open to identify any suture bleeding during cardiac surgery due to anticoagulation with heparin. In particular, in our experience, in all patients undergoing synchronous CEA and CABG, the ECC was performed lowering brain temperature by 2-5°C during ischemia (mild intra-ischemic hypothermia). This procedure was found the most efficacious neuro-protective strategy because it was associated to a reduction in the incidence and severity of cognitive deficits. 7 The intra-operative anticoagulation status was managed using a thromboelastograph (Haemonetics®, Boston, USA). After CABG and removal of the ECC cannulae, the heparin was reversed with protamine sulphate. The cervical wound was closed at the completion of the cardiac surgery.
Results
30-Day Perioperative Complications in 222 combined cardiac and carotid procedures.
Discussion
Atherosclerosis is a disease that simultaneously affects the carotid and coronary arteries. Concomitant disease can occur in 2-20% of patients, with an average incidence of 8%. Approximately 28% of patients undergoing CEA have significant coronary disease requiring revascularization . 8 Similarly, 12% of patients undergoing coronary revascularization have hemodynamically significant carotid disease. 9 The presence of significant carotid disease increases the risk of stroke after CABG.10,11 Patients undergoing CABG who are free from significant carotid disease have been shown to have a relatively low risk of stroke; as low as 1.9%. While those with hemodynamically significant stenosis run a greater risk of cerebrovascular complications following CABG. Indeed risk of stroke has been shown to be as high as 3% in patients with unilateral stenosis >70%, 5% in patients with bilateral stenosis >70% and 7-11% in patients with unilateral carotid occlusion and carotid stenosis contralateral >70%. 12 The principal risk of stroke during CABG can be explained by manipulation of the atherosclerotic aorta during cannulation and its clamping necessary to establish the cardiopulmonary bypass (CPD) .13,14 Therefore avoiding the use of CPB could help to reduce this incidence. CABG without CPB, so-called “beating heart” CABG, could represent an acceptable alternative to conventional CABG with CPB, in order to reduce the incidence of adverse events in patients with significant carotid artery stenosis. A number of studies have shown no difference in mortality and cerebrovascular complications between CABG on-pump and CABG off-pump (14). On the other hand, off-pump CABG is associated with shorter operative time, shorter ICU stay, as well as shorter overall hospitalization, and decrease in postoperative bleeding and blood transfusion. 15 There is no consensus on the optimal management of synchronous carotid and coronary disease, although several retrospective studies have attempted to answer this question.
A recent meta-analysis compared simultaneous carotid endarterectomy (CEA) and CABG vs staged CEA and CABG for patients with concomitant CAD and carotid artery stenosis in terms of perioperative outcomes. 16 Eleven studies comprising 44 895 patients were included in this analysis (21 710 in the synchronous group and 23 185 patients in the staged group). The reported results showed that the synchronous CEA and CABG group had a statistically significant lower risk for myocardial infarction and higher risk for stroke and death. In addition, transient ischemic attacks, postoperative bleeding and pulmonary complications were similar between the 2 groups.
On the other hand, research conducted by Snider et al. 17 asserted that combined CEA and CABG surgery have an acceptable 30-day morbidity and mortality (2% deaths, 3% myocardial infarctions 1% major stroke). However, these authors emphasize that the management of these patients requires the use of carotid shunting during CEA and a careful and appropriate pre, intra and post-operative assessment as well as short intra-operative time to reduce the ischemic injuries especially during CBP time. 17
Another meta-analysis by Sharma et al. 18 found no difference in mortality and stroke between combined CEA-CABG and Staged CEA-CABG. In this case, twelve studies were identified with a total of 17 469 and 7552 patients in the combined and staged group respectively. A pooled analysis revealed no difference in the early mortality, post operative stroke, combined early mortality or stroke and combined endpoint of MI or stroke between the 2 surgical approaches. The authors conclude that the 2 strategies can be used interchangeable in clinical practice, with each having specific applications linked to specific clinical conditions.
Another approach is the TransFemoral Carotid Artery Stenting (TF-CAS) as an alternative to CEA in patients with severe coronary artery diseases. However, TF-CAS has not been widely adopted in the setting of patients requiring concomitant CABG and carotid interventions because of the higher stroke rates compared with CEA. 19 In fact, a meta-analysis of 31 studies by Paraskevas et al. 19 reported a perioperative stoke rate of 15% for patient with symptomatic carotid disease undergoing TF-CAS and CABG.
Transcarotid artery revascularization (TCAR) with dynamic flow reversal is a new endovascular option for carotid revascularization. The initial results appear to be superior to TF-CAS and has decreased incidence of stroke in some part perhaps due to the fact that, unlike TF-CAS, TCAR avoids arch manipulation . 20 Williams et al. 21 have recently described TCAR performed concomitantly at the time of CABG. In this setting, TCAR can be achieved via a small supraclavicular incision. However, this hybrid strategy during CABG requires deviation from protocol of perioperative DAP so critical to protect against early stent thrombosis. Indeed these authors did not administer Clopidogrel preoperatively and only loaded the patient with Clopidogrel postoperatively. In our experience based on 222 patients undergoing simultaneous carotid and coronary revascularization, the overall mortality was 4.1% and neurologic morbidity was 5.0%. In our opinion, the 2 patients with perioperative hypoxic coma due to diffuse cerebral hypoperfusion and severe perioperative heart failure must not be counted in neurological morbidity. The incidence of perioperative stroke and transient cerebrovascular complications (TIAs) were 4.1% (9 patients) and .9% (2 patients), respectively. The 2 perioperative strokes were ipsilateral to carotid CEA, while the remaining 7 occurred in the contralateral hemisphere. In the present study, the stroke rate for asymptomatic carotid stenosis was .9% (2/222 patients), while the overall stroke rate was 3.2% (7/222 patients) in contralateral hemisphere. Taking into account the incidence of stroke in relation to the type of coronary revascularization, it must be underlined that the 2 ipsilateral strokes occurred in ECC (1 patient) and in Off-Pump (1 patient), while the contralateral strokes occurred in Off-Pump (3 patients) and in ECC (4 patients).
The occurring of 7 strokes contralateral to the CEA and only 2 ipsilateral to the CEA suggest that the cause of cerebral embolization is mainly related to manipulations of the ascending aorta rather than clamping or cannulation for ECC in patients with aggressive atherosclerosis.
Our results for unilateral vs bilateral disease are very similar. In our opinion, this is because bilateral carotid stenosis (˃70%) were treated as first with CEA for isolated carotid and then, after 7 days, CEA + CABG. In this way, the patient comes to CABG with both carotid surgery, then reducing the risk of stroke.
Unilateral aymptomatic stenosis is still a controversial area today. In our clinical practice, the historical tendency was to treat the unilateral asymptomatic stenosis with CEA + CABG for ˃70% stenosis. In the last 4 years, however, patients with unilateral asymptomatic stenosis ˃70% underwent CEA only and only if they show ipsilateral ischemic lesions on brain-CT. If these patients do not report ischemic lesions on brain-CT, they undergo only to CABG but not to CEA.
The findings of the present study are supported by the results of a recent large multicentric observational study 22 aimed to evaluate the association of CEA and CABG with postoperative outcomes. Klarin et al. 22 identified 994 off-pump CABG patients (497 CABG only and 497 CABG-CEA) and 5952 on-pump CABG patients (2976 CABG only and 2976 CABG-CEA). In patients who received on-pump operations, those undergoing CABG-CEA had no observed difference in rate of in-hospital stroke (OR, .93; 95% CI, .72-1.21; P = .6), higher incidence of STS morbidity composite events (OR, 1.15, 95% CI, 1.01-1.31; P = .03), and no observed difference in 30-day mortality (OR, 1.28; 95% CI, .97-1.69; P = .08) compared with those undergoing CABG only. For off-pump procedures, CABG-CEA patients had no observed difference in rate of in-hospital stroke (OR, .80; 95% CI, .37-1.69; P = .56) compared with those undergoing CABG only.
Limitations of our study include its retrospective and nonrandomized nature. Next, our analysis describes only CABG-CEA in the setting of CABG using CPB vs off-pump CABG but does not include other strategies such as staged CABG followed by CEA or CEA followed by CABG. Finally, the availability of CT findings for all patients deserves a thorough analysis and we aimed to explore and analyze the correlation between CT findings and symptom status in a new paper.
Conclusions
In conclusion, our experience reported that the concomitant CEA+CABG treatment is safe and effective in patients with severe and multivessel coronary artery disease and symptomatic severe carotid stenosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants or on human tissue were in accordance with the ethical standards of the institutional and/or national research committee and with the 1975 Helsinki declaration and its later amendments or comparable ethical standards. Ethics approval was not sought for the present study because of the retrospective observational nature of the study; the patient information was anonymized and de-identified to protect patient confidentiality.
Informed Consent
Informed consent was not obtained because the study was in retrospective design.