
Abstract
Spontaneous celiac artery (CA) dissection is an uncommon cause of acute abdominal pain, accounting for 4% of visceral artery dissections and aneurysms, with the majority of symptomatic visceral artery dissections involving the splenic, hepatic, and superior mesenteric arteries.1,2 Despite a recent increase in the frequency of diagnosis of CA dissection with the use of advanced imaging modalities, its pathogenesis and natural history remain unclear. 3 Approximately half of CA dissections are symptomatic, presenting most commonly with acute abdominal pain and unremarkable physical examination and laboratory findings.3,4
A 54-year-old man with a history of hypertension and no recent trauma presented with 6 hours of severe epigastric pain with transient radiation to the back. An initial abdominal computed tomography (CT) angiogram demonstrated a CA aneurysm with an intimal flap extending from the distal celiac artery to the trifurcation (Panels A and B) and a thrombus nearly occluding the splenic artery (Panel C). Hemorrhage was noted in the left anterior pararenal space, and multiple splenic infarctions were present. Repeat imaging 14 hours after presentation showed CA dissection with 90% stenosis at the origin of the common hepatic and splenic arteries and a stable pararenal hematoma with no extravasation of contrast. The patient’s blood pressure was controlled and his pain resolved spontaneously. Given his pararenal hematoma, anticoagulation was not initiated. Repeat imaging 2 months after discharge showed persistent CA intimal disruption with no flow-limiting stenosis.

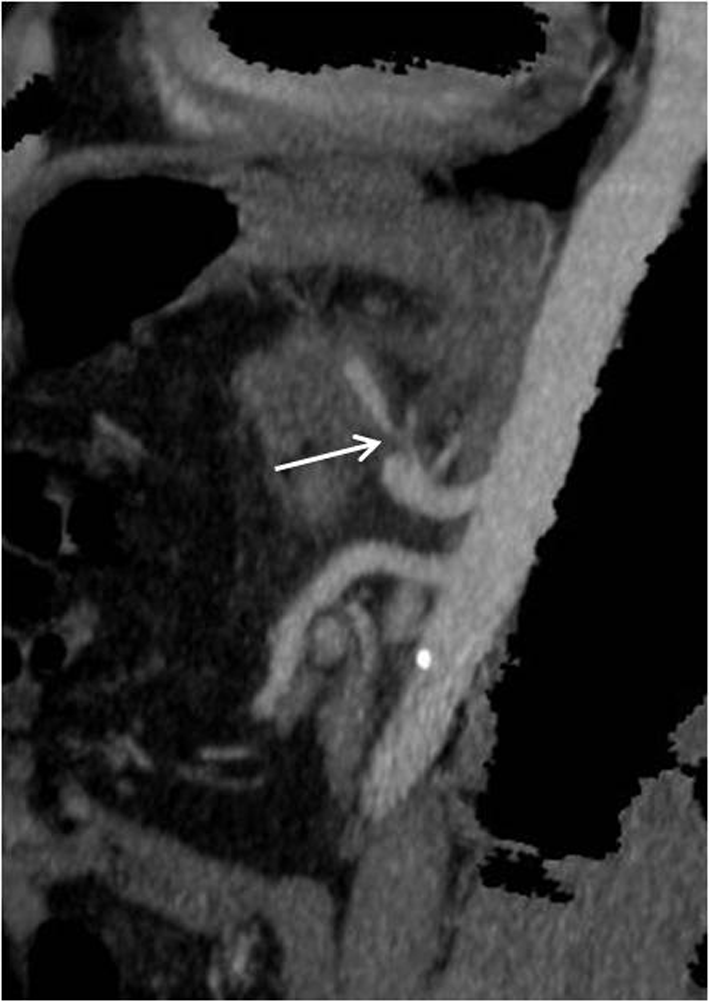
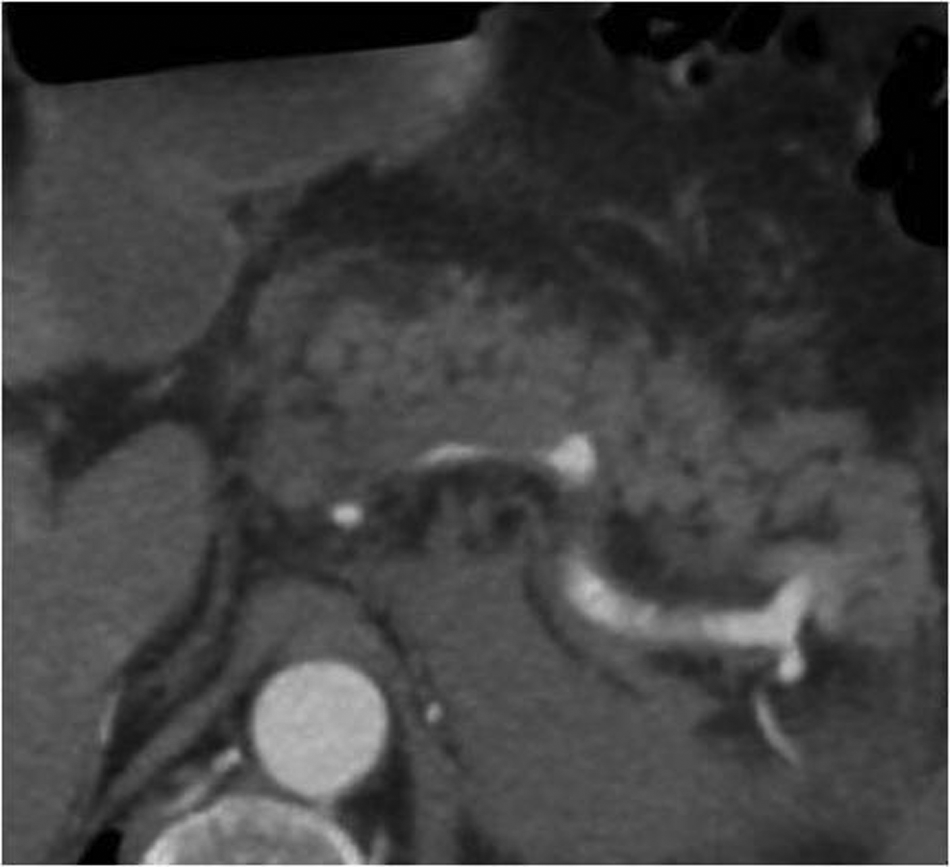
Though conventional angiography remains as the gold standard for CA dissection diagnosis, a CT angiogram has become the diagnostic modality of choice for visceral artery dissection as it is less invasive and allows localization and characterization of the intimal flap as well as associated thrombus or hemorrhage. 4 In the absence of indications for emergent surgical or endovascular intervention (persistent pain, uncontrolled hypertension, aneurysm enlargement, expanding retroperitoneal hematoma, or hepatic or splenic ischemia), it is safe for patients to be managed conservatively with blood pressure control and anticoagulation for 3–6 months.1,4,5 Further evaluation includes autoantibody testing for vasculitides such as giant-cell arteritis, Takayasu arteritis, and polyarteritis nodosa, as well as investigation of hereditary connective tissue disorders (e.g. Marfan syndrome, Ehlers-Danlos syndromes, and fibromuscular dysplasia). 6 Segmental arterial mediolysis should be considered in the absence of positive inflammatory markers. 7 Follow-up with serial imaging shows regression of the false lumen in the majority of patients. 3
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Mark A Creager, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.