
Abstract

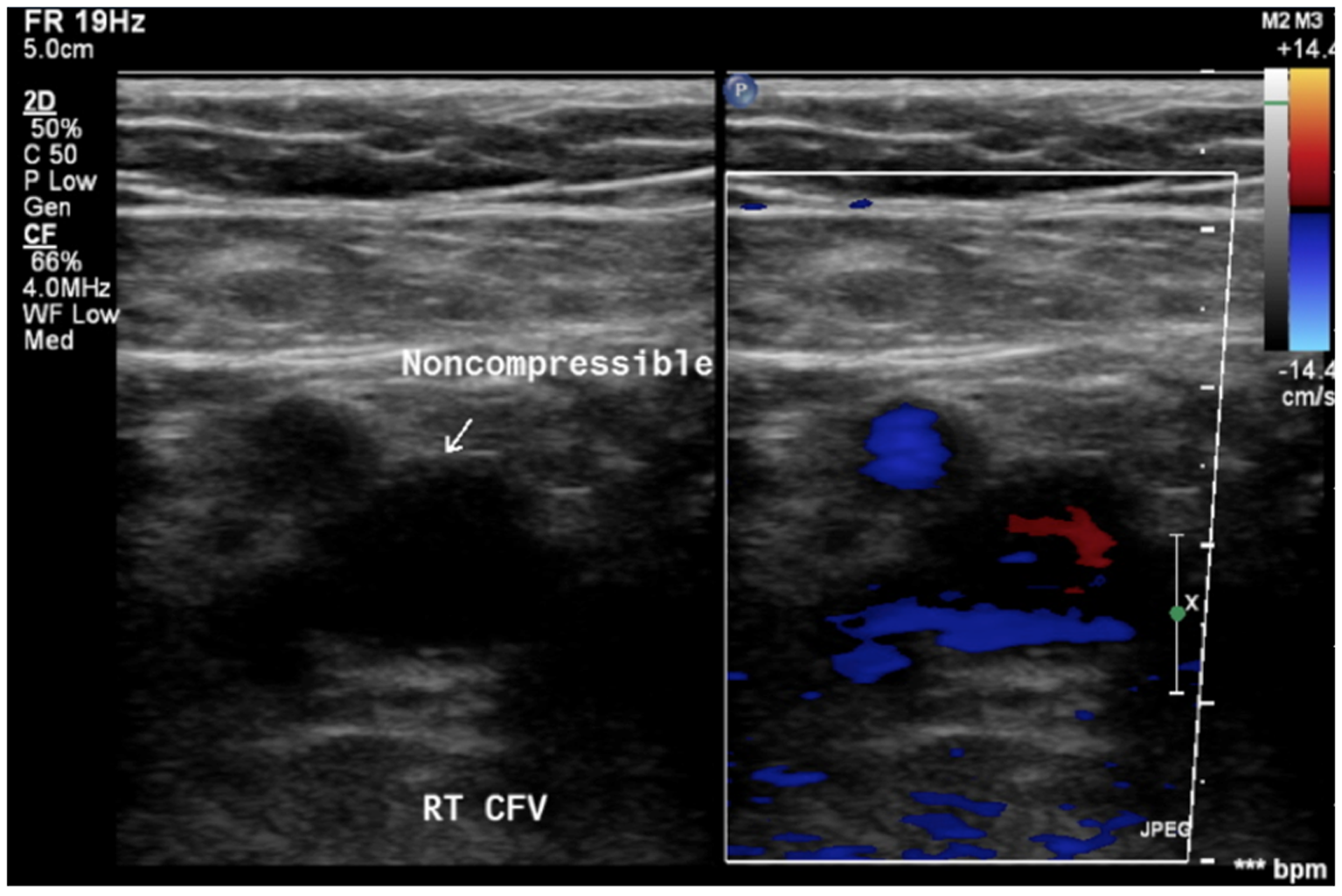
We present a case of a spindle cell tumor, initially diagnosed as deep venous thrombosis (DVT), in a previously healthy 50-year-old man presenting with acute onset shortness of breath. The patient had no known risk factors for development of thromboembolic disease. However, multiple bilateral pulmonary emboli were detected on spiral computed tomography (CT) of the chest. Duplex study demonstrated a non-compressible right common femoral vein with minimal flow that was read as an acute DVT (Panel A). The patient did not complain of any leg pain at this time and there were no palpable masses on physical exam. The patient was started on anticoagulation with intravenous heparin and subsequently bridged to warfarin and discharged.
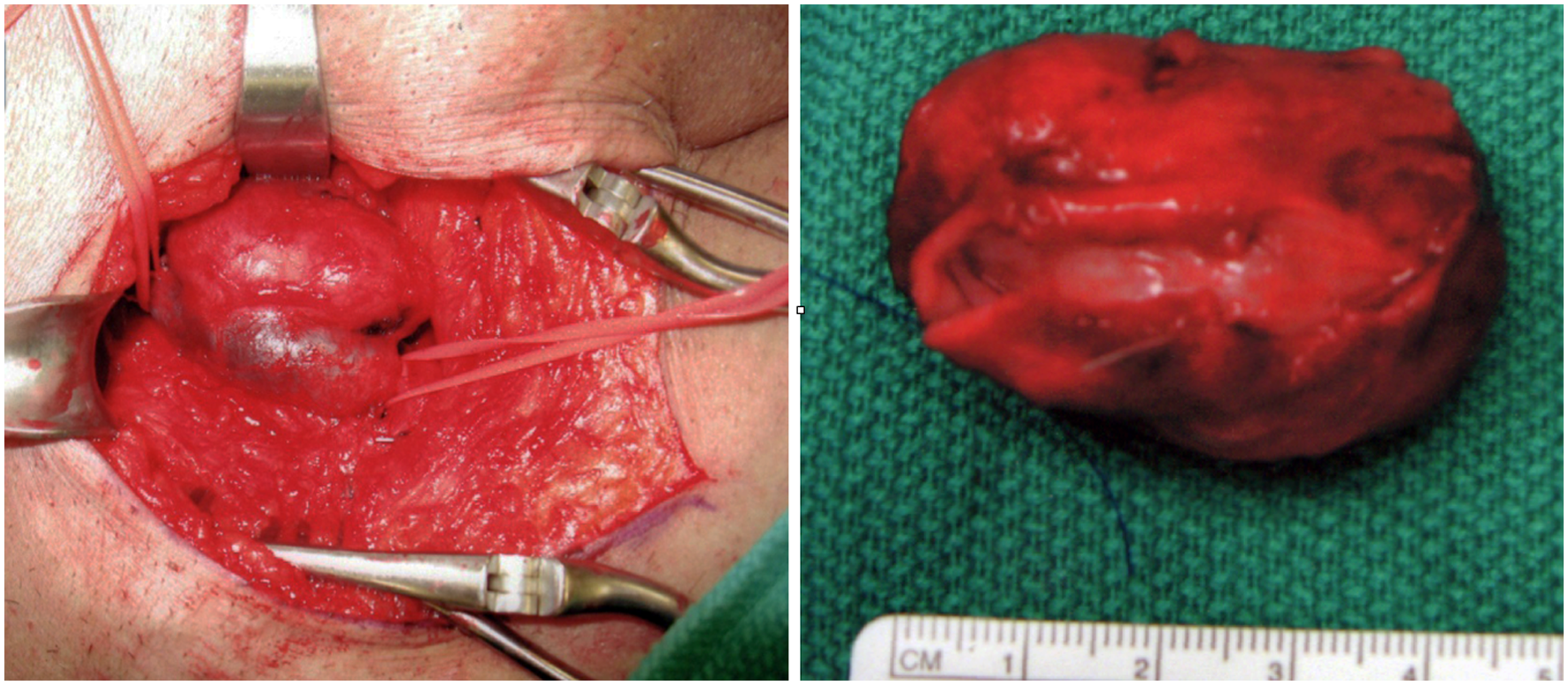
Despite adequate anticoagulation, the patient complained of progressively worsening symptoms of tenderness and edema of the right lower extremity. Two months after initial presentation, a repeat duplex study revealed enlargement of the right common femoral vein with minimal vascularity appreciable on ultrasound (Panel B). Given the interval growth, a contrast-enhanced CT was ordered, which revealed an enhancing 4.6 × 2.3 cm soft tissue mass intrinsic to the right common femoral vein (Panel C). The patient underwent surgical exploration of the right groin and excision of a 4.5 × 2.9 × 2.5 cm tumor within the right common femoral vein (Panel D). Histopathology was consistent with spindle cell sarcoma. Venous reconstruction was accomplished using an 8 mm PTFE Propaten graft. The patient tolerated the procedure well with resolution of symptoms postoperatively.
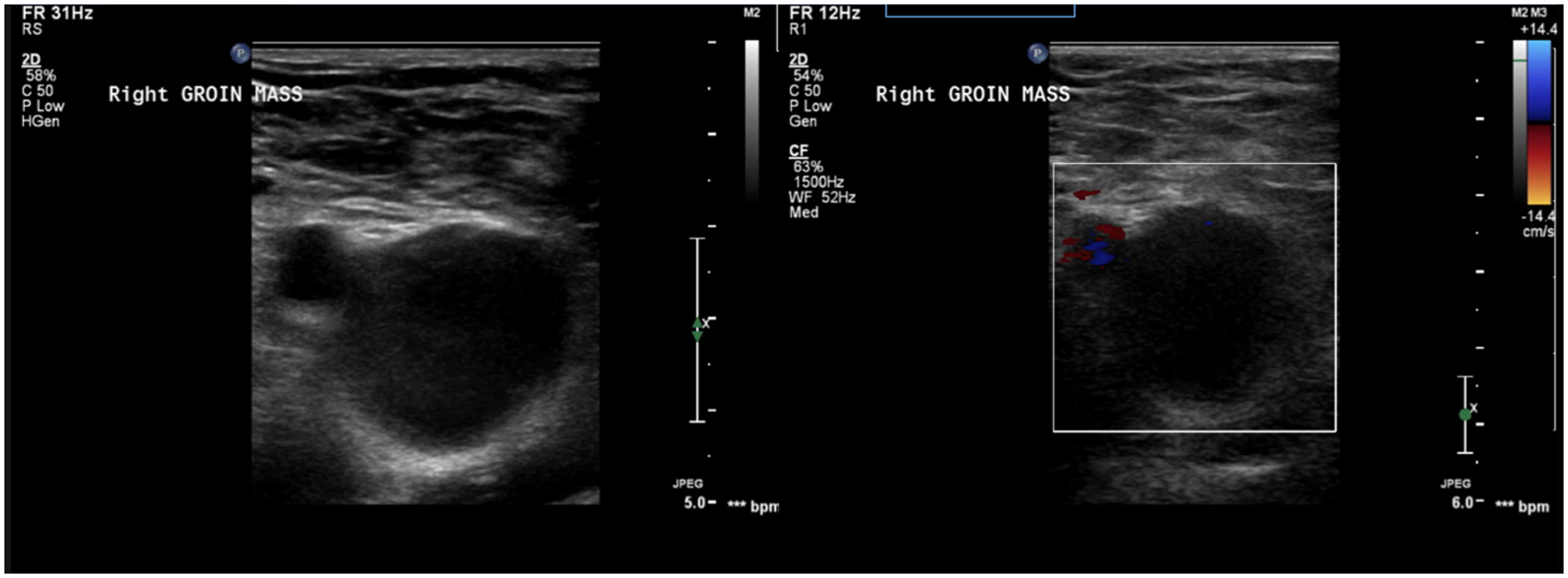
Duplex study without (left) and with (right) color.
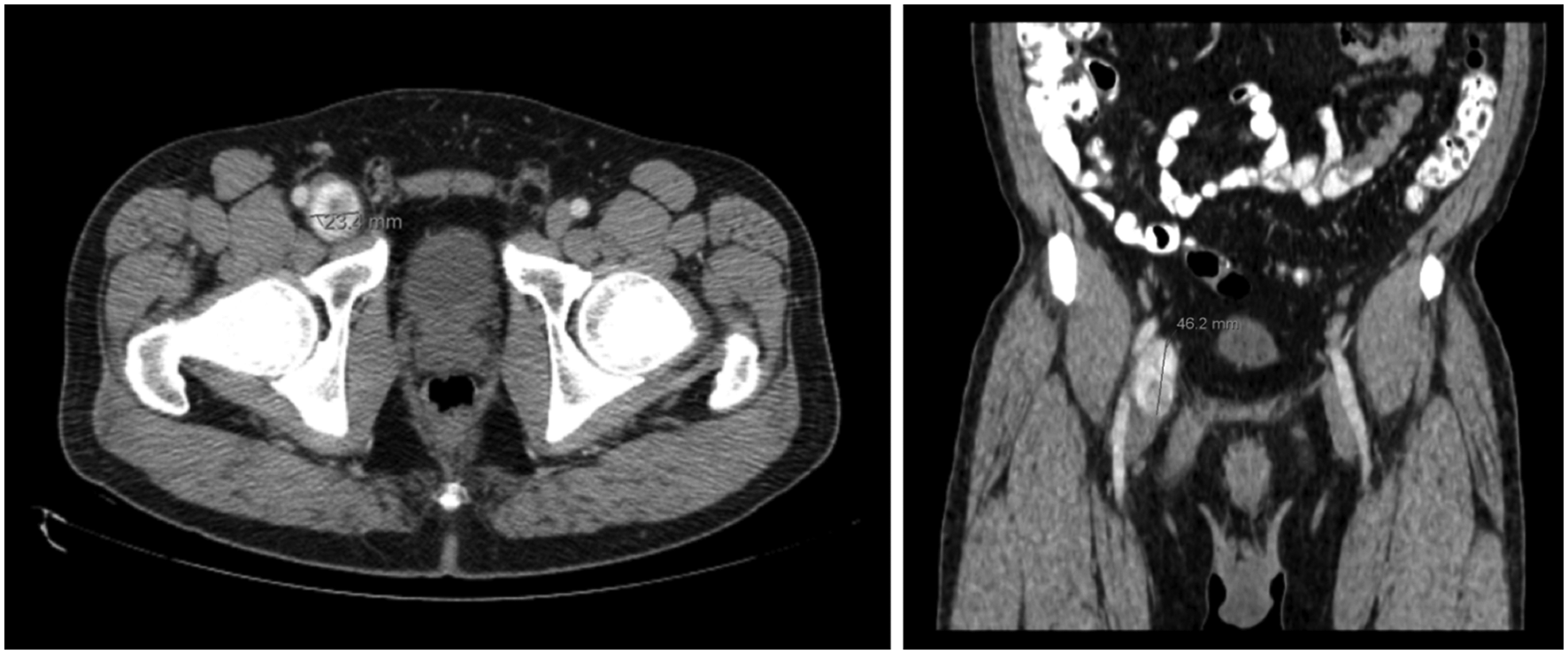
Axial (left) and coronal (right) contrast enhanced CT.
Spindle cell sarcomas intrinsic to blood vessels are rare connective tissue malignancies. Reported cases have included involvement of the pulmonary artery, where they can clinically mimic thromboembolic disease, and the portal vein.1–3 Our findings suggest that vascular spindle cell tumors may appear very similar to DVT on ultrasound and thus should be considered in the differential diagnosis. Of note, a repeat CT of the chest showed interval resolution of the previously detected pulmonary emboli. This suggests that the emboli were likely composed of thrombotic material secondary to the tumor rather than tumor involvement in the pulmonary arteries.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Mark A Creager, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors have no conflicts of interest to declare.