
Abstract

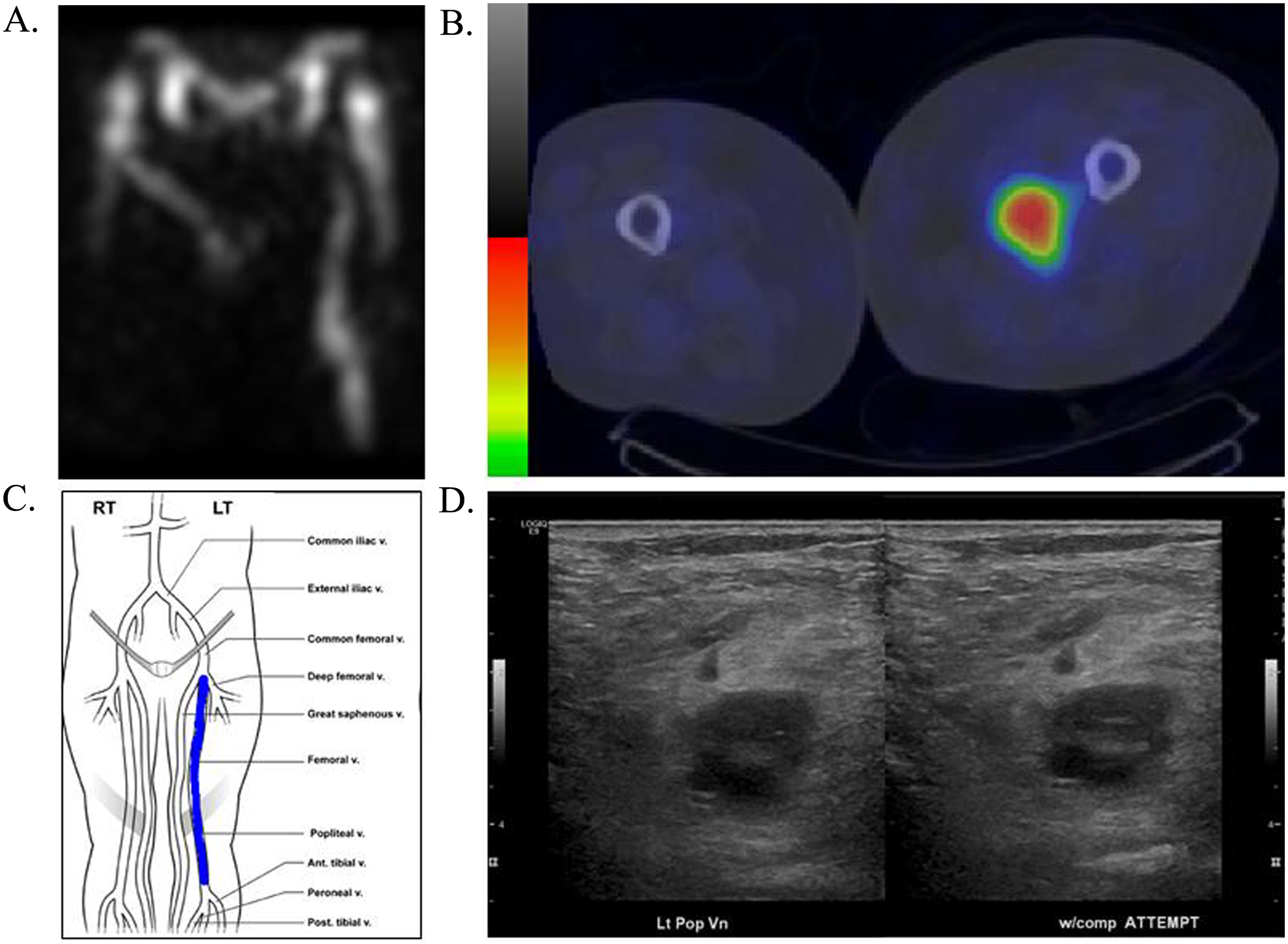
A 61-year-old man was admitted to an outside medical facility with left leg deep vein thrombosis and bilateral pulmonary emboli. His clinical course was complicated by hypotension, azotemia and declining mental status. Positive blood cultures for gram-positive cocci prompted transfer to our institution. Despite broad-spectrum antibiotics (vancomycin, cefepime, and ciprofloxacin), the patient remained febrile (temperature 39.4°C) with persistent leukocytosis. An echocardiogram revealed no valvular vegetations. Bacteremia persisted with methicillin-sensitive Staphylococcus aureus despite antimicrobial therapy. In the absence of a clear source of infection, an indium-111- labeled white blood cell (WBC) scan was performed, revealing radiotracer enhancement of the left popliteal, femoral, and common femoral veins (Panels A and B) corresponding to thrombus location as assessed by ultrasound (Panels C and D). Radiotracer uptake within these segments was greater than would be demonstrated by bland inflammatory thrombus. Excessive tracer uptake was not evident in the pulmonary arteries.
Septic thromboembolism should be considered in the differential diagnosis of patients with persistent bacteremia despite adequate antibiotic therapy. 1 Successful management of sepsis requires prompt identification and eradication of the infective source. 2 Failure to identify the source of infection nearly doubles the risk of sepsis-related death. 3 Septic thromboembolism may lead to bacterial seeding of other organs, with increased mortality rates if inappropriately treated. 1 Although the diagnosis of venous thromboembolism preceded the onset of bacteremia in this patient, the association between the two events was not initially apparent. In this case, the tagged WBC imaging was instrumental in the identification of the focus of infection. However, the broad utility of WBC scanning in the evaluation of patients with septic thromboembolism is unclear. 4 Non-infected thrombi may be inherently inflamed due to granulocyte adhesion common to the thrombotic evolution. 5 The magnitude of radiotracer activity in the setting of persistent bacteremia, despite appropriate antibiotic therapy and lack of identifiable focal infection, argues for the diagnosis of septic thrombosis in our case. Although surgical thrombectomy is often considered in such cases, conservative management with appropriate antibiotics and anticoagulants can be successful. Furthermore, surgical or mechanical thrombectomy may augment the risk of septic embolization. 6
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Mark A Creager, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors have no conflicts to disclose.