
Abstract
Flow-mediated dilation (FMD) is a non-invasive index of endothelial function. In an attempt to standardize FMD for shear stimulus, shear rate (velocity/diameter), rather than shear stress (viscosity*velocity/diameter), is commonly used as a surrogate measure, although it is limited by individual differences in blood viscosity. The purpose of this study was to determine the contribution of whole blood viscosity to FMD and other key measures of vascular function. Blood viscosity, FMD, carotid artery compliance, and carotid–femoral pulse wave velocity (cfPWV) were measured in 98 apparently healthy adults varying widely in age (18–63 years). Whole blood viscosity was not significantly correlated with FMD, cfPWV, or carotid artery compliance. Shear rate was a stronger correlate with FMD than shear stress that takes blood viscosity into account (r = 0.43 vs 0.28). No significant differences were observed between whole blood viscosity and traditional risk factors for cardiovascular disease. Age was positively correlated with cfPWV (r = 0.65, p < 0.001) and negatively correlated with FMD (r = −0.24, p < 0.05) and carotid artery compliance (r = −0.45, p < 0.01). Controlling for viscosity did not reduce the strength of these relations. These results indicate that whole blood viscosity does not significantly impact measures of vascular function and suggests that the common practice to use shear rate, rather than shear stress, in the adjustment of FMD is valid.
Introduction
Flow-mediated dilation (FMD) is a non-invasive index of endothelial function. 1 During the measurement, blood flow is occluded and then reintroduced in a manner sufficient to elicit a reactive hyperemic response in the conduit artery of interest. The shear stimulus caused by the sudden reperfusion stimulates the endothelium to release nitric oxide causing vasodilation. Investigators have proposed normalizing FMD by the shear stimulus in an effort to adjust FMD for a given stimulus.2–4 Common practice in the literature is to estimate shear rate (velocity/diameter) rather than shear stress (viscosity*velocity/diameter) because of the more invasive nature of measuring blood viscosity and/or a lack of specialized equipment to measure viscosity. In these instances, blood viscosity is assumed constant across subjects. Although this assumption appears reasonable, emerging evidence linking individual differences in viscosity to cardiovascular disease5–8 casts doubt on such an assumption. Currently, it remains unclear whether such an assumption is valid and the degree by which viscosity affects FMD.
Accordingly, the primary purpose of this study was to determine the contribution of whole blood viscosity to a measure of FMD. Additionally, as the secondary purpose, we determined the potential contribution of blood viscosity on other key vascular measures (pulse wave velocity and arterial compliance).
Methods
Subjects
A total of 98 adults varying in age (18–63 years) were studied. All subjects were non-smokers and free of overt cardiovascular disease as assessed by medical history. None of the subjects was taking cardiovascular-acting or hematological medications. The study was reviewed and approved by the Institutional Review Board. All subjects provided their written informed consent prior to participation.
Measurements
Following a 12-hour overnight fast, a blood sample was collected from the antecubital vein by venipuncture. Plasma concentrations of total, low-density lipoprotein (LDL)-, and high-density lipoprotein (HDL)-cholesterol, triglycerides, and glucose were determined by standard enzymatic methods. Brachial blood pressure was measured in triplicate at rest in a supine position with an automated oscillometric device (HEM-907XL; OMRON Healthcare, Vernon Hills, IL, USA). Whole blood viscosity was measured immediately after blood collection at 60 revolutions/minute (representing a shear rate of 212/s) using a micro cone-plate viscometer (LVT-I; Brookfield Engineering Laboratories, Stoughton, MA, USA). The coefficient of variation for whole blood viscosity is 8% in our laboratory.
All vascular measurements below were performed after fasting and abstaining from caffeine for ≥ 4 hours. Participants were asked to avoid strenuous physical activity and alcohol for ≥ 24 hours before measurement. For premenopausal women, measures of vascular function were performed during the early follicular phase of their menstrual cycle to control for the effects of estrogen. 9 Subjects were studied in a supine position after ≥ 15 minutes of rest in a quiet temperature-controlled (22–24°C) laboratory setting.
Flow-mediated dilation (FMD)
Brachial FMD measurements were performed as previously described. 10 A longitudinal image of the brachial artery was obtained using an ultrasound machine equipped with a high-resolution (15 MHz) linear-array transducer (iE 33; Phillips, Bothel, WA, USA). A customized transducer-holding device secured the transducer in place 5–10 cm proximal to the antecubital fossa. Following the baseline recording, the blood flow occlusion cuff placed on the forearm distal to the elbow was inflated to 100 mmHg above baseline systolic blood pressure for 5 minutes using a rapid cuff inflator (E20; Hokanson, Bellevue, WA, USA). All ultrasound-derived images were transferred and analyzed using image analysis software (Brachial Analyzer; Medical Imaging Applications, Coralville, IA, USA). FMD was calculated using the following equation: (maximum diameter – baseline diameter) / baseline diameter × 100%. Shear rate was obtained using the equation: blood velocity/brachial artery diameter. Shear stress was calculated as whole blood viscosity*blood velocity/brachial artery diameter.
Carotid–femoral pulse wave velocity (cfPWV)
The cfPWV was determined using an automated previously validated device (VP-2000; Colin Medical Instruments, San Antonio, TX, USA), as previously described.11,12
Carotid artery compliance
Carotid artery compliance was measured in a subgroup of 40 subjects with a combination of ultrasound imaging of the common carotid artery (by B-mode ultrasound) and recording of contralateral carotid arterial pressure (by applanation tonometry; VP-2000; Colin Medical Instruments), as previously described.13,14
Statistical analyses
Pearson product-moment correlation analyses were used to determine relations among whole blood viscosity and cardiovascular risk factors and measures of vascular function. Partial correlation analyses were used to control for the effect of whole blood viscosity on measures of vascular function. Because both shear rate and shear stress were not normally distributed based on the Shapiro–Wilk test, the data were transformed using either the log scale or square root, and Spearman correlation analyses were then used to evaluate associations. Significance was set a priori at p < 0.05. All data are expressed as mean ± SEM.
Results
Selected subject characteristics are displayed in Table 1. Whole blood viscosity displayed a wide range of distribution from 1 to 5.5 cP60. No significant associations were observed between whole blood viscosity and traditional risk factors for cardiovascular disease (Pearson-r ranging from 0.01 to −0.31). Whole blood viscosity was not significantly correlated with FMD (r = −0.11; Figure 1) or any other measures of vascular function (cfPWV and carotid artery compliance). Shear rate was found to be a stronger correlate with FMD than shear stress (r = 0.43 and 0.28; Figure 2). The results were essentially the same when both shear rate and shear stress data were normalized and Spearman correlation analyses were performed. Spearman correlation coefficients were 0.41 and 0.20. As expected, age was negatively correlated with FMD (r = −0.24, p < 0.05) and carotid artery compliance (r = −0.45, p < 0.01), and positively correlated with cfPWV (r = 0.65, p < 0.001). Accounting for blood viscosity did not reduce the strength of the associations as these relations remained statistically significant (FMD, r = −0.24; cfPWV, r = 0.65; carotid artery compliance, r = −0.44).
Selected subject characteristics
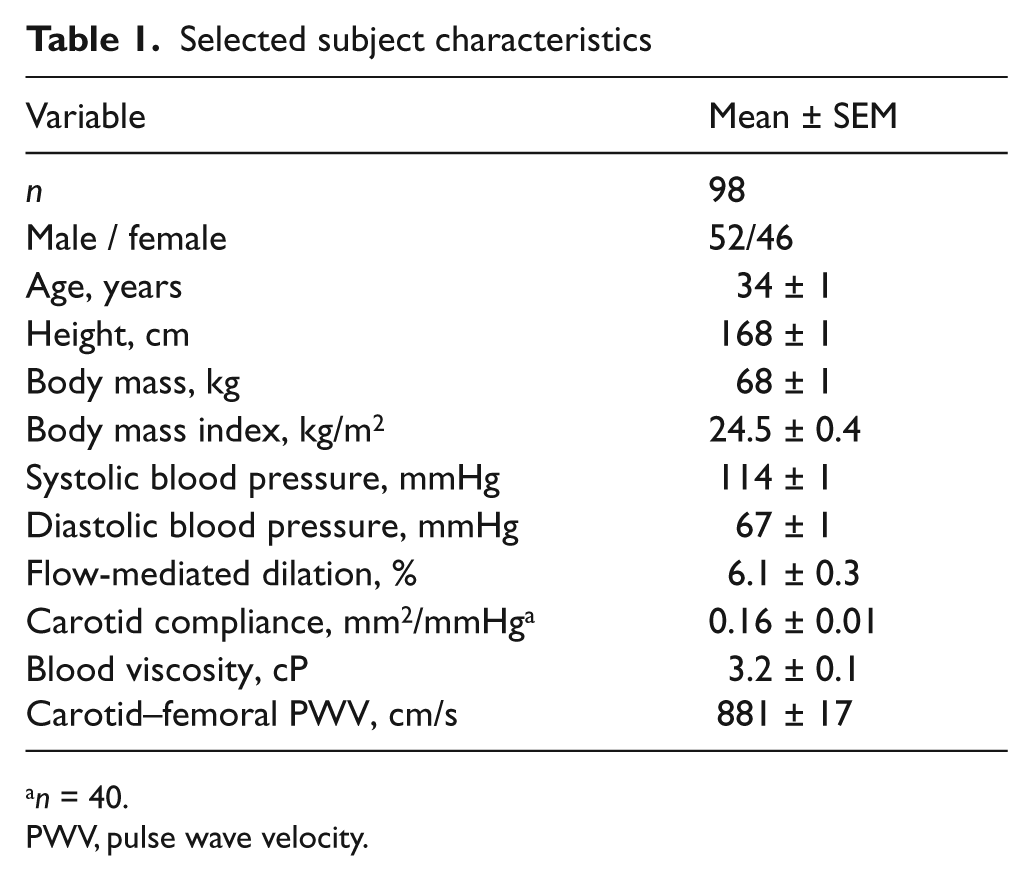
n = 40.
PWV, pulse wave velocity.
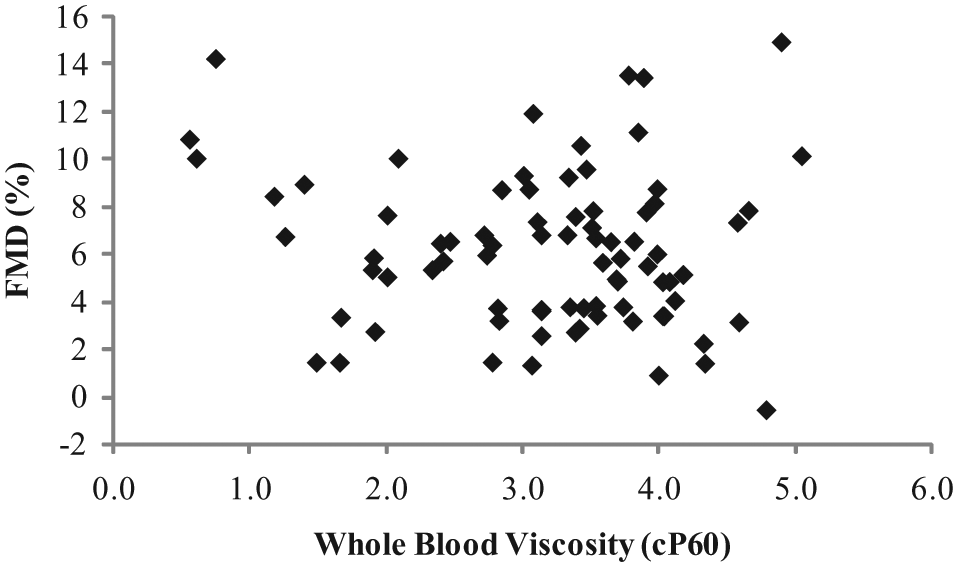
Association between flow-mediated dilation (FMD) and whole blood viscosity.
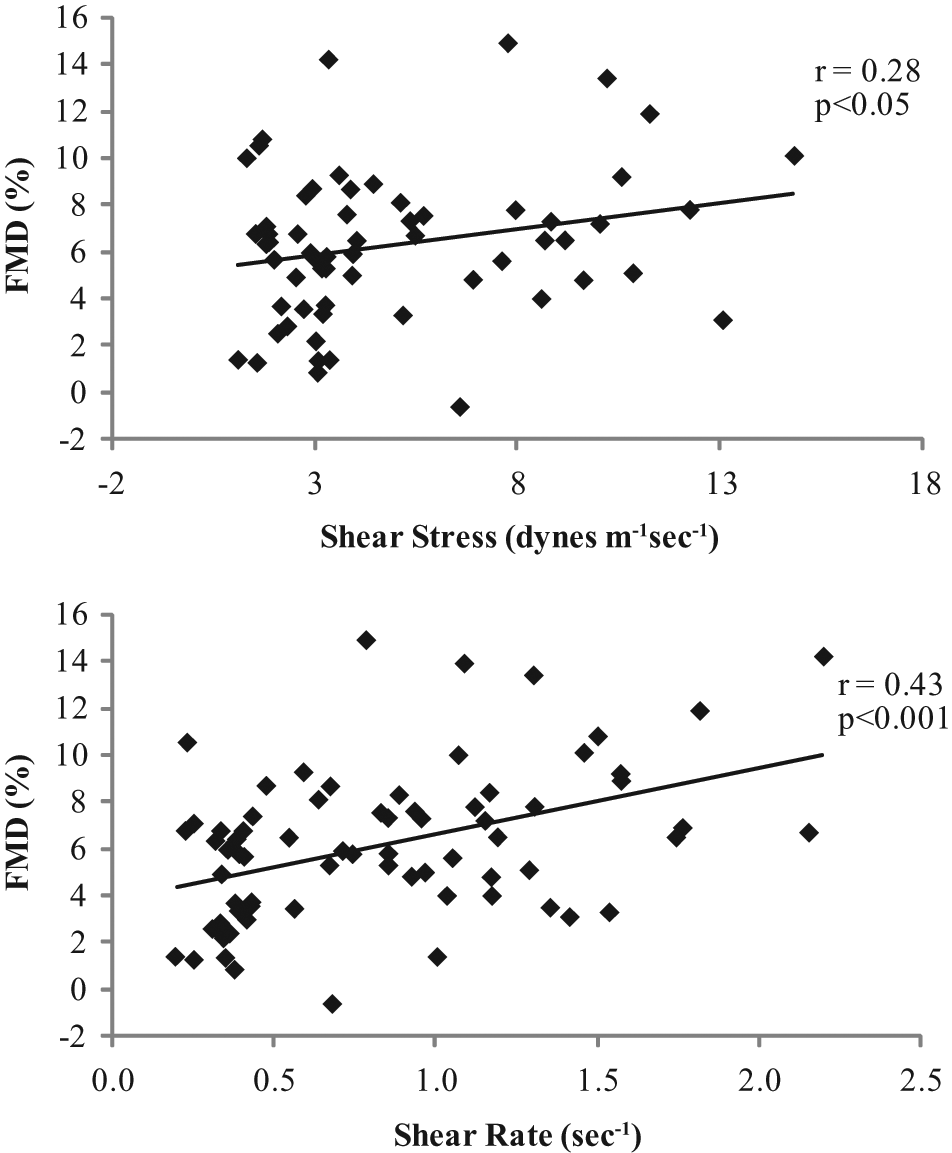
Associations between flow-mediated dilation (FMD) and shear stress and shear rate.
Discussion
The purpose of this study was to determine the impact of whole blood viscosity on measures of vascular function. We found no significant correlations between whole blood viscosity and FMD or other key measures of vascular function (cfPWV and carotid artery compliance). Shear rate was a stronger correlate with FMD compared with shear stress in the present study. It appears that the inclusion of blood viscosity, which has its own inherent variability, may have introduced greater variability and reduced the association of shear stress with FMD. The present findings indicate that blood viscosity may not be a necessary component when adjusting FMD for shear stimulus.
It is well established that FMD and carotid artery compliance decreases and cfPWV increases with advancing age.14–17 Consistent with the previous studies, measures of vascular function were significantly associated with age in the present study. To confirm the impact of blood viscosity on these measures, we performed partial correlation analyses controlling for blood viscosity. The relation between vascular function and age remained statistically significant even after the individual differences in whole blood viscosity were incorporated. These findings suggest that blood viscosity does not appear to modulate the relations between vascular function and age.
Whole blood viscosity is determined by hematocrit, plasma viscosity, aggregation of red blood cells, and deformability of red blood cells. 18 It was not until the 1960s that the ability to measure blood viscosity drastically improved and became considered a component of blood flow. Since then, a number of studies have focused on the importance of this measure with regard to both age and disease status.6,18–22 In our sample of apparently healthy adults, blood viscosity was not significantly correlated with any of the risk factors for cardiovascular disease, including age. While some studies have found a positive correlation between blood viscosity and certain cardiovascular disease risk factors,5–8,22 others have not.18,21 Similarly, the relation between aging and blood viscosity is highly debated within the literature. Some studies have found an increase in blood viscosity with age,20,23,24 whereas others, like the present study, have failed to discover similar findings.25,26 Thus, the association between blood viscosity and risk factors for cardiovascular disease remains controversial.
Limitations to the present study include the lack of diseased populations. All of the subjects studied were considered apparently healthy without any overt disease. This would diminish the generalizability of the present study findings to other populations. However, the subject selection is also a strength of the present study since the influence of disease states and the use of medications that potentially confound the data interpretation are minimized by this approach. Despite the choice of subject selection, we were able to achieve a wide range of whole blood viscosity values in our sample ranging from 1 to 5.5 cP60. To the best of our knowledge, this is the first study to determine the impact of blood viscosity on FMD and arterial stiffness in a healthy population. Previous research in patients with chronic anemia has also found no correlation between blood viscosity and FMD. 27
In summary, whole blood viscosity was not associated with FMD and other vascular functional measures. Shear rate was more strongly correlated with FMD than shear stress. Taken together, these results are not consistent with the assertion that measurements of whole blood viscosity should be included when evaluating vascular function. The next step in this line of investigation is to assess what level of blood viscosity is necessary in order to register an influence on FMD.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.