
Abstract
Understanding the impact of peripheral artery disease (PAD) requires broad evaluation of how functional limitations of PAD affect patients’ perceptions of health-related quality of life (HRQL). The objective of this study was to describe the development, testing, and psychometric properties of the PAD Quality of Life Questionnaire (PADQOL). The PADQOL was developed in three steps: (1) interviews of symptomatic PAD patients provided content of the initial questionnaire; (2) co-administration with the SF-36 (a 36-item short-form health survey), Walking Impairment Questionnaire, and Profile of Mood States examined construct validity; and (3) a three-phased factor analysis identified factors and shortened the questionnaire. Data analyses from 297 symptomatic PAD patients resulted in a 38-item questionnaire of five factors: Social relationships and interactions, Self-concept and feelings, Symptoms and limitations in physical functioning, Fear and uncertainty, and Positive adaptation (α = 0.92–0.73) and items related to sexual function, intimate relationships and employment. Between-instrument correlations established construct validity. In conclusion, PADQOL is a validated measure to assess the disease-specific physical, psychosocial and emotional effects of PAD for research and practice.
Introduction
Peripheral artery disease (PAD) is a progressive atherosclerotic disease that affects approximately eight million adults in the United States, 1 and is associated with increased mortality, morbidity and cardiovascular disease.2–4 The most common symptom of PAD is claudication, which is characterized by pain, cramping or aching in the calves, thighs, or buttocks, is initiated by walking, and subsides with rest. Symptoms of PAD may also include atypical exertional pain and, in those with more severe disease, ischemic pain at rest or tissue loss. Symptomatic PAD is associated with severe limitations in physical function, particularly walking, and activities of daily living.
These PAD-related symptoms, physical limitations, as well as mental, social, and emotional function have been characterized in several validated questionnaires. The Vascular Quality of Life Questionnaire (VASCUQOL) 5 contains 25 items categorized into the domains of social and emotional well-being, pain, symptoms and activities. This questionnaire was originally developed for patients who had symptomatic PAD and had a Fontaine classification of II–IV (claudication, ischemic rest pain or tissue loss). 6 The Intermittent Claudication Questionnaire 7 is a 16-item questionnaire addressing physical limitations, worry, and interference with activities. The Peripheral Artery Questionnaire (PAQ) 8 is a 20-item questionnaire measuring physical limitations, symptoms, symptom stability, treatment satisfaction, quality of life, and social function. The Walking Impairment Questionnaire (WIQ) 9 is a well-validated measure of community-based walking that addresses perceived pain and difficulties in response to walking distance, speed, and stair climbing, but was not designed to address frequency of symptoms, function, or quality of life.
These PAD-specific questionnaires have increased our ability to assess the functional consequences of PAD. However, the patient’s perception of the impact of PAD on other aspects of health-related quality of life (HRQL), including self-concept, sense of burden, emotional health, well-being, and life-satisfaction, remains poorly understood.10,11 These aspects of life may be as or more important to the patient with PAD, and thus a reliable, valid, and sensitive measure that captures the impact of PAD on these aspects of quality of life is needed.
‘Quality of life’ is a term used in multiple disciplines, but is often poorly defined and misinterpreted, even within the realm of healthcare. 12 The seminal research of Cantril, 13 Bradburn, 14 and Campbell et al.15,16 identified two primary themes related to quality of life: well-being and satisfaction. Whereas physical, social, psychological, and spiritual well-being include both positive and negative feeling states, life-satisfaction is the evaluation of life circumstances in the context of cultural and individual values, 12 the perceived discrepancy between one’s aspirations and one’s achievement, and ranges from a sense of fulfillment to one of deprivation. 15 Thus, quality of life is conceptually related to, but distinct from, functional and health status, although these terms are often used interchangeably.12,17
Assessment of HRQL is focused more specifically on the quality of life experience in the context of health and illness.18–20 Evaluating HRQL outcomes can provide researchers and clinicians with a more holistic view of the experience of living with PAD 21 and augments objective assessment of disease severity and response to intervention. The purpose of this paper is to describe the development, testing, and psychometric properties of the PAD Quality of Life Questionnaire (PADQOL), which was designed to assess the impact of PAD on HRQL.
Development of the PADQOL
The PADQOL was developed in three major steps. Institutional Review Board approval and informed consent were obtained at each phase of development. First, the experience of living with PAD was solicited from those afflicted with the disease. Subsequently, factor domains capturing the experience were identified, and then validated.
Foundational qualitative interviews
In the first stage of tool development, qualitative interviews were conducted with 38 individuals with symptomatic PAD in Minnesota and Colorado. This group of participants intentionally comprised those with symptoms ranging from claudication to ischemic rest pain, tissue loss, and previous amputation. Interviews were transcribed and analyzed for common themes according to accepted qualitative analysis methods. 22 The themes that emerged from the qualitative interviews included challenges with diagnosis and management of PAD, symptom experience, impact of disease on physical and social functioning, perceived compromise of self, fear and uncertainty, and an expression of positive adaptation. 10 The details of this foundational work have been published elsewhere. 10
Initial questionnaire formulation
The themes identified from the qualitative interviews were formulated into specific questions, and focused on concepts such as the impact of physical limitations and impaired walking on the ability to perform usual activities, the ability to feel ‘normal’, the ability to interact with friends or family, and the perceived burden of PAD. These questions were then compiled into a 65-item questionnaire with potential responses offered that ranged from ‘strongly agree’ to ‘strongly disagree’ and ‘not important’ to ‘very important’ on two Likert-type scales.
The interview participants were then given the newly developed questionnaire to elicit their impressions regarding the adequacy of the questionnaire with respect to clarity of instruction, accuracy, and comprehensiveness of content in reflecting the full impact of PAD. Participants were asked to rate each item. This process resulted in a revised 60-item questionnaire that comprehensively represented the self-reported experiences of these patients, thus establishing content validity.
Exploratory factor analysis
Procedures
During the first phase of questionnaire validation, 242 additional patients with symptomatic PAD were identified through a number of sources including clinician referral, participation in PAD clinical trials, and advertisement. Participants primarily included those with claudication or other exertional PAD-related leg symptoms, but also included individuals with ischemic rest pain. Participants were asked to complete the 60-item PADQOL questionnaire and were asked to rate the extent to which they agreed or disagreed with and the importance of each item on two six-point Likert-type scales. To address construct validity (i.e. the extent to which concepts are associated with a similar concept (convergent validity) or a different concept (divergent validity)), 23 participants were asked to simultaneously complete three additional questionnaires that assessed separate constructs contributing to health-related quality of life: perceived community-based walking ability, health status, and mood.
The questionnaires were either given directly to participants during a face-to-face visit or mailed with a stamped, addressed return envelope. Participants who were mailed questionnaires were contacted 1 week later to verify delivery, to answer any questions, and to encourage prompt return. Follow-up phone calls were made weekly until the questionnaires were returned.
Completion of the PADQOL took approximately 9 minutes. Total time to complete the four questionnaires averaged 30–40 minutes and participants were able to do this with little difficulty. Questionnaires were reviewed for completeness and, when possible, participants were asked to provide responses for missing items. Participants were also instructed that they could decline to respond to any question if they wished. Such omissions were coded as missing data.
Factor analysis methods
The structure of the questionnaire was assessed by exploratory factor analysis, applying varimax rotation to identify linear combinations of correlated items (factors) that represent distinct underlying constructs. Prior to factor analysis, PADQOL items were re-coded so that high scores on all items represented a positive direction. Both eigenvalues and a scree plot were used to determine the number of factors retained. The eigenvalues of the retained factors were > 1.5. Cronbach’s alpha coefficients were calculated for each factor as a measure of internal consistency (reliability): the extent to which items within a factor correlate with each other and the factor total. Items with adequate loading (greater than > 0.40) on a factor were totaled to create factor scores. Items that loaded on more than one factor were assigned to the factor with the highest loading. The scale was examined with and without the item, and the extent to which the item added to the reliability of the factor was determined. The strength of the loading and the conceptual fit of the item with the other items and respective factor determined the final placement of the item. Factor scores were then transformed to a 0–100 scale, with 100 indicating the most positive score. The transformation equation was: ((∑item scores – # items in subscale)/(5* # items)*100). Item reduction was performed to eliminate items that were redundant or did not contribute to the validity of the questionnaire.
The mean, standard deviation, and range of raw and transformed scores of the PADQOL factors, as well as the subscales of the WIQ, SF-36, and POMS were calculated. Construct validity (convergent and divergent validity) of this revised version of the PADQOL was evaluated with Pearson’s correlation coefficients for PADQOL factors and the subscales of the WIQ, SF-36, and POMS. It was expected that the correlation between these instruments and the PADQOL factors would reflect a partial overlap between similar concepts, little overlap between different concepts, and none of the questionnaire subscales would be able to completely explain the variance in the PADQOL factors.
Exploratory factor analysis results
Factor analysis was performed on this sample: the Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy was 0.93 and Bartlett’s test of sphericity was < 0.001. The initial factor analysis resulted in a four-factor solution comprised of 38 items. Additionally, three items were considered to be important but loaded poorly (< 0.4) on all factors, in part due to low response rates from study participants. These questions addressed the effect that PAD had on a respondent’s work role functioning, and satisfaction with sexual function and intimacy. A final individual item that assessed the impact of PAD on life in general was also retained, resulting in a total of 42 items in this version of the PADQOL. The eigenvalues for the four factors were all > 1.5. The coefficient alpha reliabilities for the four factors ranged from 0.73 to 0.95. The component of the questionnaire that asked respondents to rate the importance of each item (‘not important to me’ to ‘very important to me’) showed little variability and was thus eliminated to simplify the questionnaire.
Confirmatory factor analysis results
The 42-item questionnaire was administered to an additional 55 individuals with symptomatic PAD participating in other PAD clinical research studies. A separate confirmatory factor analysis was completed, resulting in factors similar to those identified in the original exploratory factor analysis. In this analysis, the alpha reliability of the four factors ranged from 0.76 to 0.95.
Results of final factor analysis
Given the similarity of the results of the separate factor analyses, data from the two samples were pooled, resulting in a total combined sample of 297 individuals. The combined sample was primarily male (74%) and predominantly Caucasian (85%). Ages ranged from 40 to 91 years. This sample had risk factors and co-morbid conditions similar to the general PAD population described in other studies.2,28–31 A majority of patients had hypertension and dyslipidemia and were previous or current smokers, with a total tobacco burden ranging from 3 to 144 pack years. The lower leg ankle–brachial indices (ABI) ranged from 0.24 to 1.24. Only a minority of patients had undergone a previous peripheral revascularization procedure. Table 1 provides detail of the demographic and medical characteristics of this combined sample.
Sample demographic and medical characteristics
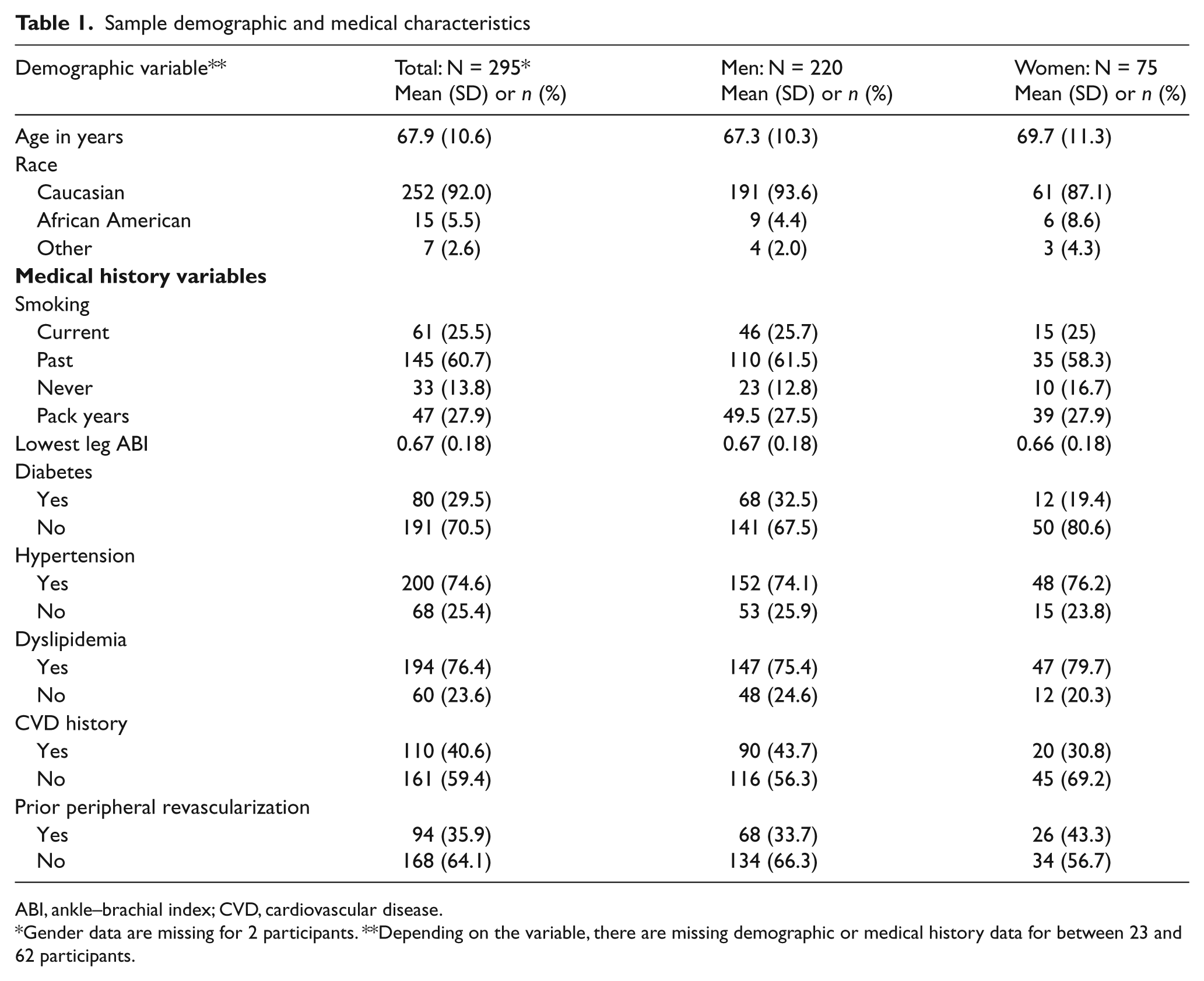
ABI, ankle–brachial index; CVD, cardiovascular disease.
Gender data are missing for 2 participants. **Depending on the variable, there are missing demographic or medical history data for between 23 and 62 participants.
Factor re-analysis was performed on the combined sample; the KMO measure of sampling adequacy was 0.94 and Bartlett’s test of sphericity was < 0.001. Similar to the factor structure of the previous factor analyses, this analysis also resulted in a four-factor solution that accounted for 55% of total variance. Eigenvalues for the four factors were > 1.5. After careful review by content and clinical experts (DTJ and RAL), it was determined that Factor 1 represented two separate constructs; therefore the 16 items in Factor 1 were separated according to content into two factors of nine and seven items. Three items were eliminated because they did not correlate (r < 0.3) with any other items in the factor and/or the alpha reliability for that factor was higher with the item removed. The final individual item that assessed the impact of PAD on life in general was also eliminated. Thus, the final questionnaire comprises five factors with a total of 35 items plus three separate non-scaled individual items that address satisfaction with sexual function, satisfaction with intimacy, and impact on employment (Appendix 1). Figure 1 provides a summary of the development of the PADQOL.
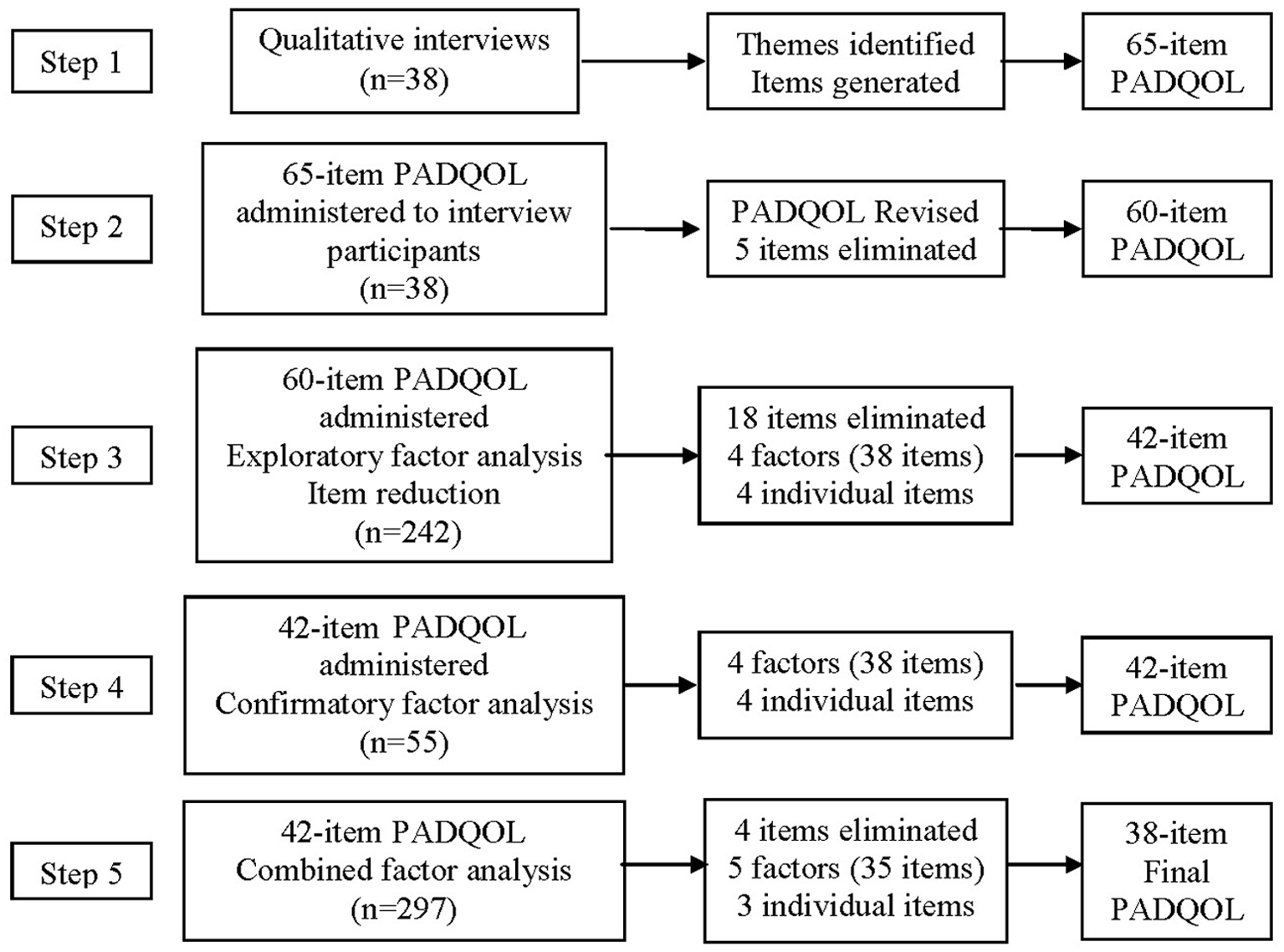
Development of the PADQOL.
PADQOL factor structure
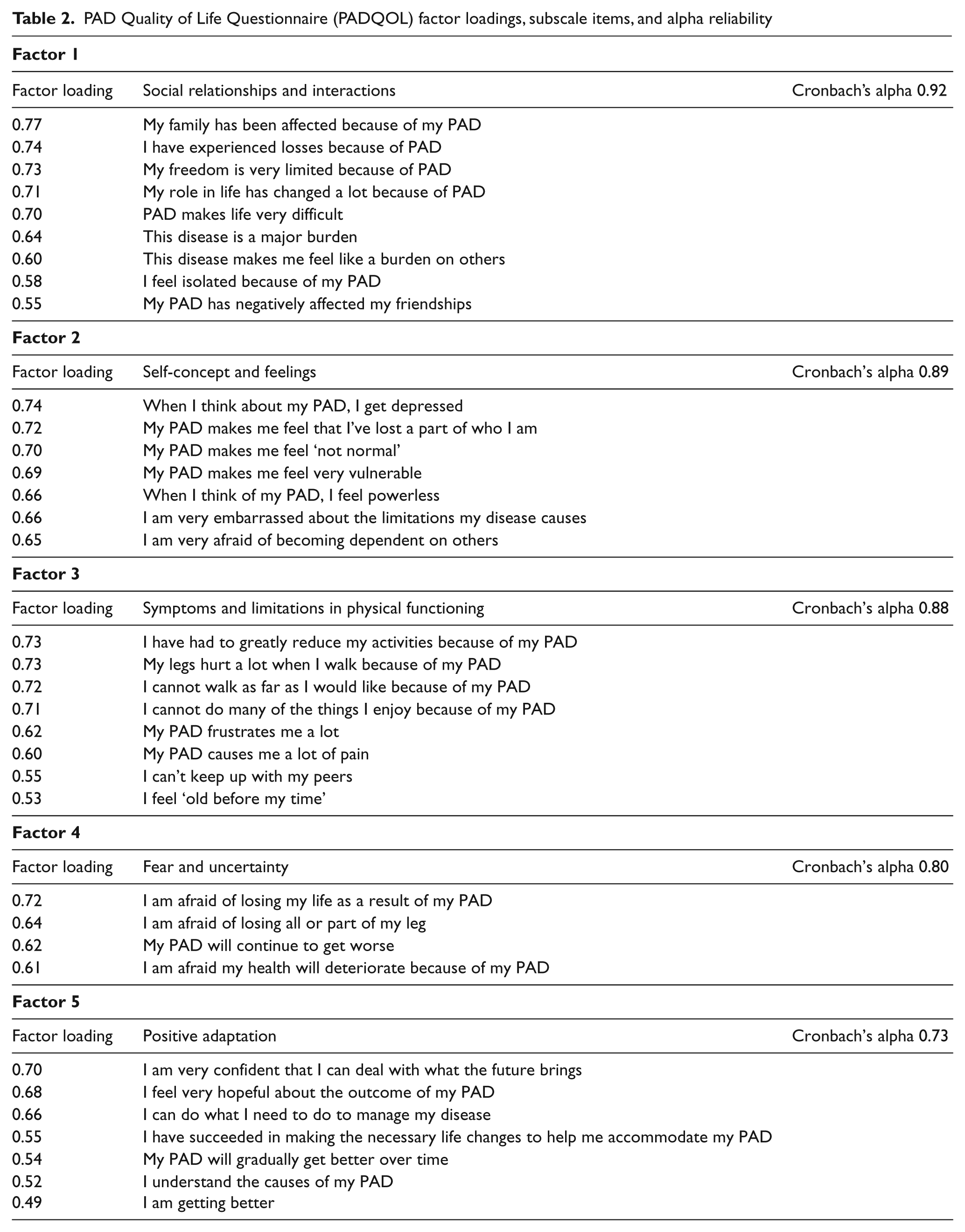
Factor 1: Social relationships and interactions (α reliability = 0.92) contains nine items that reflect the impact that living with PAD has on social relationships and interactions with others. The mean item-to-total correlation for this factor was 0.71, SD = 0.07. Factor 2: Self-concept and feelings (α reliability = 0.89) consists of seven items related to the impact that PAD has on one’s sense of self and feeling states. The mean item- to-total correlation for this factor was 0.68, SD = 0.07. Factor 3: Symptoms and limitations in physical functioning (α reliability = 0.88) contains eight items addressing physical function and limitations associated with PAD. The mean item-to-total correlation for this factor was 0.66, SD = 0.04. Factor 4: Fear and uncertainty (α reliability = 0.80) includes four items that reflect the fear and uncertainty that individuals experience in living with PAD. The mean item-to-total correlation for this factor was 0.62, SD = 0.06. Factor 5: Positive adaptation (α reliability = 0.73) contains seven items related to the positive adaptations that are made by individuals living with PAD. The mean item-to-total correlation for this factor was 0.44, SD = 0.07. These factor themes reflect the themes identified during the previous qualitative study. Table 2 describes the items, factor loadings and internal consistency (α reliability) of each factor.
PAD Quality of Life Questionnaire (PADQOL) factor loadings, subscale items, and alpha reliability
Participants’ responses resulted in a wide range of scores within each factor. With the exception of Factor 5, scores included the entire range of possible factor scores. Histograms for each of the factor scores demonstrated normal distributions. Table 3 provides a summary of the mean, standard deviation, possible range, and actual minimum and maximum scores for this sample.
Individual factor summed scores and transformed scales and item descriptions
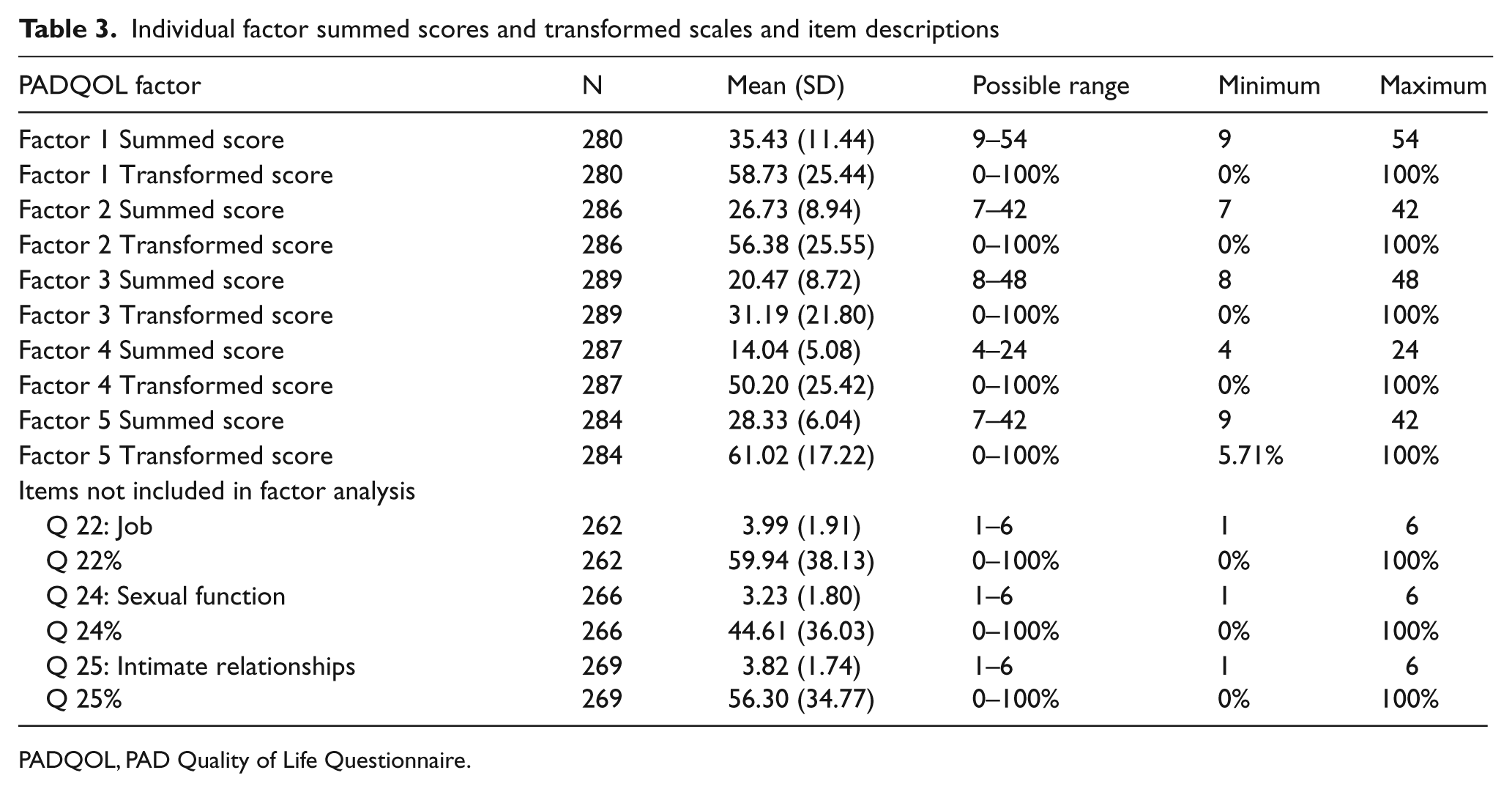
PADQOL, PAD Quality of Life Questionnaire.
PADQOL correlations with demographic medical variables
Relationships between the five PADQOL factors and demographic and medical variables were examined. Those with diabetes scored significantly lower on average than non-diabetics on Factor 1 – social relationships and interactions (x⩄ = 54.16 vs 61.45; t = 2.13, p = 0.034), Factor 3 –symptoms and limitations in physical functioning (x⩄ = 25.21 vs 33.77; t = 3.02, p = 0.001) and Factor 4 – fear and uncertainty (x⩄ = 44.15 vs 52.72; t = 2.53, p = 0.012). Only Factor 3 was statistically significantly correlated with the ABI, but the correlation was very weak (r = 0.13; p = 0.042). There was a weak but statistically significant correlation (r = 0.14; p = 0.019) between Factor 4 and age, with the fear and uncertainty score decreasing with increasing age. There were no other statistically significant associations between PADQOL factors and demographic and medical variables.
Construct validity of the PADQOL
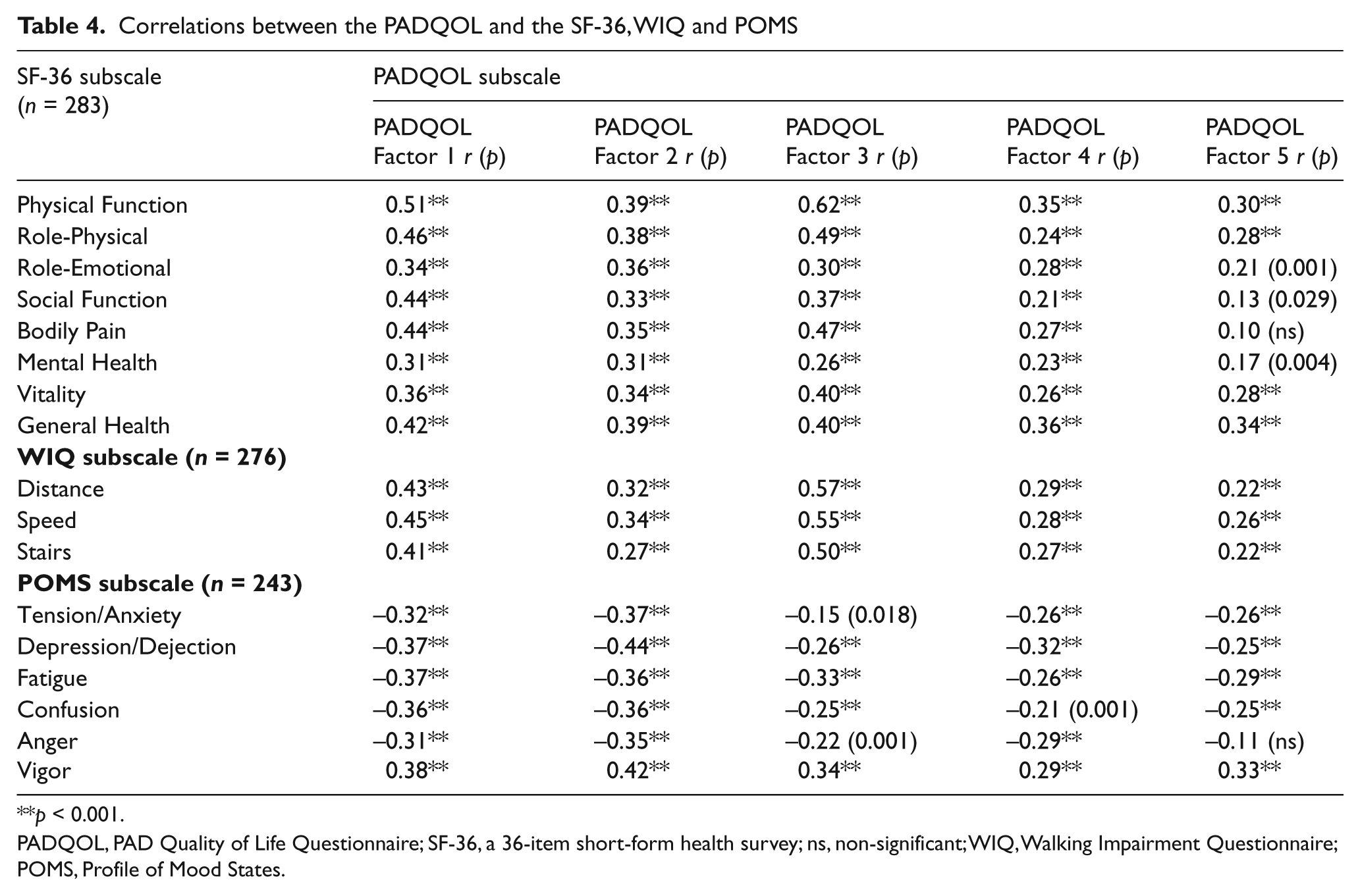
To establish construct validity (convergent and divergent validity), the relationship of the PADQOL subscale scores with the subscales of the SF-36, WIQ, and POMS were examined (Table 4). Factor 1, which reflects the social and interpersonal impact of living with PAD, was positively correlated (r = 0.31 to 0.51) with several SF-36 subscales, particularly those related to physical function, social function, vitality and bodily pain. Factor 1 was also positively correlated (r = 0.41 to 0.45) with the WIQ distance, speed and stairs subscale scores. This factor was also correlated in the expected direction with all of the POMS subscales (r = 0.31 to 0.38), particularly the vigor, depression, and fatigue subscales. Factor 2, which is related to sense of self and feeling states, also correlated with the subscales of the other questionnaires (r = 0.27 to 0.44), although not as highly as Factor 1. Factor 2 was most highly correlated with the vigor and depression subscales of the POMS. As expected, Factor 3, which reflects physical function and the limitations associated with PAD, was most highly correlated with the physical function and bodily pain subscales of the SF-36 (r = 0.47 to 0.62) and all of the WIQ subscales (r = 0.50 to 0.57). This factor was not as highly correlated with the POMS subscales. Factor 4, in which lower scores reflect greater uncertainty and fear associated with PAD, was moderately correlated with the physical function and general health subscales of the SF-36 (r = 0.35 to 0.36 ), but was only modestly correlated with the subscales of the WIQ and POMS. Of all of the PADQOL factors, Factor 5, positive adaptation, had the lowest correlations with the SF-36, WIQ and POMS subscales. This may reflect that this subscale assesses a component of HRQL that is not addressed in the other questionnaires.
Correlations between the PADQOL and the SF-36, WIQ and POMS
p < 0.001.
PADQOL, PAD Quality of Life Questionnaire; SF-36, a 36-item short-form health survey; ns, non-significant; WIQ, Walking Impairment Questionnaire; POMS, Profile of Mood States.
Discussion
We have developed and validated a PAD-specific quality of life questionnaire that quantifies the subjective patient experience and addresses the impact of PAD on those living with this debilitating disease. The questionnaire proved to be valid when correlated with instruments known to assess elements of functioning in PAD. Assessment of HRQL is essential for clinicians and researchers since interventions should be tailored to address the specific health concerns and limitations of individuals with PAD. To be fully meaningful, HRQL assessment should go beyond measurement of functional limitations such as walking capability or the ability to perform activities of daily living, to include the patient’s perspective regarding how those functional limitations impact life-satisfaction and well-being. The PADQOL captures these perspectives.
Qualitative data from patient interviews revealed that PAD can result in significant limitations in all aspects of life, including relationships with family and friends, and can even compromise a patient’s sense of self. 10 The five factors that emerged during questionnaire development reflect the themes that were identified from those interviews, thus supporting our primary findings. 10
The impetus for the development of this questionnaire came from the conviction that it is important to consider the numerous ways a disorder can affect a patient’s life and well-being, both physically and emotionally. It is not only important to assess a patient’s walking capability, but also how that walking capability impacts the patient’s life. For example, a retired sedentary individual may feel less impacted by a two-block walking limitation than would a younger individual who is still employed. This instrument allows us to examine these relative differences for the individual. This ability distinguishes the PADQOL from currently existing PAD-specific HRQL questionnaires. Additionally, patient scores on individual subscales may provide guidance to clinicians to tailor interventions. A patient who scores poorly on the uncertainty and fear subscale may benefit most from an educational intervention, whereas a patient whose score demonstrates poor self-concept or social isolation may need an intervention targeted at increasing social support.
Many existing instruments, such as the SF-36, 25 the EuroQOL, 32 the Nottingham Health Profile, 33 and the Sickness Impact Profile, 34 explore the general aspects of functional status, health status and quality of life for individuals living with chronic illness and are therefore non-disease specific. There are advantages and disadvantages to using such quality of life instruments. Though generic quality of life measurement tools can provide valuable insights and allow comparisons across populations, they may not be sensitive enough to adequately detect change over time, especially in disease-specific symptoms. 35
PAD-specific quality of life questionnaires that are accurate, simple, effective, and gleaned from the patient’s perspective provide optimal value for assessing the impact of the disease, and in determining effective treatment options and tailoring interventions. Such measurement tools should capture the burden of living with PAD and address the patient’s perceived social, emotional and physical well-being. 20
Recently, there has been an increase in the development of quality of life questionnaires designed specifically to address PAD, including the VASCUQOL, 5 the PAQ, 8 and the WIQ. 9 As discussed earlier, the majority of items in each of these questionnaires focus strongly on physical, social, and emotional functioning, walking impairment, and symptoms. However, they focus less on the perceived burden of the disease and its effects on well-being and quality of life. This gap was the impetus for our development of the PADQOL.
The 38-item PADQOL offers clinicians and researchers a tool to measure the impact and burden of PAD on the HRQL of patients living with this debilitating disease. It is easy to complete in approximately 5–10 minutes and is comprised of items to which PAD patients can relate. The samples included in its development included men and women having a broad range of age and disease severity. The risk factors and co-morbid conditions seen in these samples were similar to those seen in the general PAD population, thus increasing the generalizability of our results. Factor analysis results were consistent across samples with good internal consistency and construct validity. Internal consistency of all of the factors exceeded the recommended threshold for questionnaires. 23 Correlations of the PADQOL factors with the subscales of the WIQ, SF-36, and POMS were moderate, but did not completely overlap. Overall, the factors were most highly correlated with the SF-36, WIQ, and POMS subscales with conceptually similar factor constructs: correlation coefficients ranged from 0.40 and 0.80, supporting convergent validity. 36 For example, Factor 3, which focuses on symptoms and limitations in physical functioning was most highly correlated with the WIQ subscales and the SF-36 physical function subscales, while Factor 2, which focuses on sense of self and feeling states was most highly correlated with the vigor and depression subscales of the POMS.
There are some limitations to the PADQOL at this point in time. Test-retest reliability and assessment of sensitivity to change over time with disease progression and following intervention have yet to be established. Studies are ongoing to complete this work. Validation of the PADQOL should also be established in more racially and ethnically diverse populations with more equal gender representation. The PADQOL was validated in a heterogeneous group of PAD patients through convenience sampling. Further validation is also needed in distinct populations of PAD patients, those with moderate versus severe claudication, and critical limb ischemia.
The PADQOL will be available for use in research trials and clinical settings. Future directions include investigation of changes in the PADQOL following intervention and as an adjunct assessment to objective and subjective functional evaluation. Investigations will be conducted to assess the impact of disease progression on changes in the PADQOL in order to fully discern the potential clinical benefits of using the PADQOL to guide therapy. Additional validation work will also continually examine possibilities for further shortening of the PADQOL to increase its ease of use in both clinical and research settings.
Conclusion
The PADQOL is a validated questionnaire designed to specifically address the significant disease-specific physical, psychosocial and emotional consequences of living with PAD. This questionnaire will be a valuable clinical and research tool to enhance understanding of HRQL in patients with PAD, helping to guide treatment strategies and improve care for this patient population.
Footnotes
Appendix
Funding
This work was supported in part by a grant from the Society for Vascular Nursing.
Conflict of interest statement
The authors have no conflicts of interest to declare.