
Abstract
Patients with critical limb ischemia have higher rates of death and amputation after revascularization compared to patients with intermittent claudication. However, the differences in patency after percutaneous revascularization of the superficial femoral artery are uncertain and impact the long-term risk of amputation and function in critical limb ischemia. We identified 171 limbs from 136 consecutive patients who had angioplasty and/or stenting for superficial femoral artery stenoses or occlusions from July 2003 through June 2007. Patients were followed for primary and secondary patency, death and amputation up to 2.5 years, and 111 claudicants were retrospectively compared to the 25 patients with critical limb ischemia. Successful percutaneous revascularization occurred in 128 of 142 limbs (90%) with claudication versus 25 of 29 limbs (86%) with critical limb ischemia (p = 0.51). Overall secondary patency at 2.5 years was 91% for claudication and 88% for critical limb ischemia. In Cox proportional hazards models, percutaneous revascularization for critical limb ischemia had similar long-term primary patency (adjusted hazard ratio = 1.1, 95% CI = 0.4, 2.6; p = 0.89) and secondary patency (adjusted hazard ratio = 1.1, 95% CI = 0.2, 6.0; p = 0.95) to revascularization for claudication. Patients with critical limb ischemia had higher mortality and death rates compared to claudicants, with prior statin use associated with less death (p = 0.034) and amputation (p = 0.010), and prior clopidogrel use associated with less amputation (p = 0.034). In conclusion, percutaneous superficial femoral artery revascularization is associated with similar long-term durability in both groups. Intensive treatment of atherosclerosis risk factors and surveillance for restenosis likely contribute to improving the long-term outcomes of both manifestations of peripheral artery disease.
Keywords
Introduction
Death and amputation after revascularization are more common in patients with critical limb ischemia than in patients with intermittent claudication. 1 This is related to severe comorbidities and advanced coronary and cerebrovascular atherosclerosis in patients with critical limb ischemia. However, the long-term patency of percutaneous revascularization of the superficial femoral artery for critical limb ischemia compared to claudication is uncertain. If critical limb ischemia is associated with poorer long-term patency after percutaneous procedures, this would impact long-term limb survival and function after percutaneous revascularization for critical limb ischemia.
We previously showed the importance of lesion length in determining long-term patency in patients with claudication. 2 In this study, we assessed whether percutaneous superficial femoral artery revascularization among patients with critical limb ischemia had inferior long-term patency compared to patients revascularized for claudication. We also compared the long-term risk of death and amputation among critical limb ischemia patients compared to claudicants and assessed factors associated with these outcomes.
Methods
Patients
We used a retrospective cohort design to identify consecutive patients who had angioplasty and/or stenting of the superficial femoral artery for intermittent claudication or critical limb ischemia from July 2003 through June 2007 by the Interventional Vascular Medicine Services at the Brigham and Women’s Hospital and the VA Boston Healthcare System. We compared the patency and outcomes of 111 patients with claudication to 25 patients with critical limb ischemia. Patients were referred to each tertiary care center from providers within and outside the hospitals, and evaluated in the Interventional Vascular Medicine Clinic prior to proceeding to revascularization. The Research Ethics Committees at each institution approved the protocol.
We reviewed the electronic medical records and procedure reports to collect data on patient demographics, procedure characteristics, atherosclerotic risk factors at the time of their index procedure and subsequent outpatient visits, and vascular studies (ankle–brachial indices (ABIs) and duplex ultrasound). Chronic kidney disease was defined as a creatinine > 1.5 mg/dl or dialysis dependence, coronary artery disease was defined as angiographically documented coronary stenosis > 50% or past coronary revascularization, and diabetes and hypertension by a history of these risk factors or medical treatment. Runoff was defined as the number of patent anterior and posterior tibial arteries into the foot and peroneal artery to the ankle. Lesion length was defined as the total length of stents used in the index procedure or estimated from the angiogram using the known length of the angioplasty balloons and grouped into three categories (lesions < 100 mm, > 100–200 mm, or > 200 mm).
Procedure details
All procedures were performed in the cardiac catheterization laboratory by interventionalists with endovascular certification by the American Board of Vascular Medicine. Selective angiography was performed under local anesthesia via contralateral retrograde or ipsilateral antegrade common femoral artery access. Patients were anticoagulated with unfractionated heparin or direct thrombin inhibitors. Lesions were crossed using a variety of techniques including 0.014-inch, 0.025-inch, and 0.035-inch stainless steel or hydrophilic wires. Long lesions were usually crossed with either 0.014-inch coronary wires or 0.025-inch hydrophilic wires using a support balloon or catheter. The wire-loop method (‘subintimal technique’) was used rarely. All procedures used balloon angioplasty, and most were stented with nitinol self-expanding stents (70% of successful index procedures). Balloon diameters with a 1:1 ratio to the reference segment were used for balloon angioplasty. Nitinol self-expanding stents were deployed after balloon angioplasty if there were flow-limiting dissections or significant residual stenoses (> 50%). Adjunctive therapy in the 153 successful cases included atherectomy in 10 (7%) limbs, laser therapy in 19 (12%) limbs, and a lumen re-entry device in nine (6%) limbs. Patients either received clopidogrel for 5 days prior to the procedure or received a loading dose of 300 mg after the index procedure. Antiplatelet therapy post-procedure included aspirin 81–325 mg daily indefinitely and clopidogrel 75 mg daily for at least 1 month. Statin treatment was used almost universally (90% of patients).
Post-procedure follow-up
All patients were followed in the outpatient Interventional Vascular Medicine Clinic at their institution 1–2 months post-procedure, 6 months post-procedure, and then at 6–12-month intervals as previously described. 2 At each follow-up visit, patients were asked about the return of ischemic symptoms, had a physical exam including assessment of limb ulceration, had ABIs measured, and in most patients duplex ultrasound of the femoral artery was reviewed. Asymptomatic patients with more than a twofold acceleration in peak systolic velocity of the femoral artery by duplex ultrasound were followed more frequently to identify the recurrence of symptoms or more progressive stenosis.
Outcomes
Outcomes included primary patency, secondary patency, death, amputation and major adverse vascular events. A major adverse vascular event was defined as failed primary patency, amputation or death. Failed patency was defined as recurrent claudication symptoms with a decline in ABI to less than 0.9 and a decrease more than 0.15 below the post-procedural value, or a threefold or greater increase in peak systolic velocity in the femoral artery on duplex ultrasonography (> 70% luminal stenosis)2,3 or target vessel revascularization. Failed secondary patency was defined as failed patency after reintervention for restenosis or reocclusion of the treated vessel. Review of the electronic medical record and subsequent procedures identified patients with recurrent claudication symptoms or restenosis, reintervention with percutaneous treatments or bypass surgery, amputation and all-cause death up to 2.5 years after the index procedure.
Statistical analysis
All data were analyzed using STATA statistical software. Descriptive statistics used proportions or means and standard deviations where appropriate. Baseline differences were compared by ANOVA for continuous variables or chi-square tests for categorical variables. To address the main hypothesis, event curves were defined for failure of each of the patency outcomes grouped by lesion length at the index procedure. The different outcomes of failed patency were analyzed using separate survival analyses with hazard ratios, 95% confidence intervals and p-values from Cox proportional hazards models. Multivariable models were developed using a backward stepwise process entering variables with a univariate p < 0.3, and a p < 0.1 for removal. All Cox models used clustering by patient to account for any correlations in outcomes of different limbs in the same patient.
Results
Description of patients
Table 1 describes the baseline clinical characteristics of patients with claudication or critical limb ischemia. Of the 136 patients, 111 (82%) presented with claudication and 25 (18%) for critical limb ischemia. Patients with critical limb ischemia tended to be older (p = 0.016) with a higher percentage having chronic kidney disease (p = 0.07) compared to patients with claudication. There were no differences in past (p = 0.25) or current (p-value = 0.16) smoking status between the groups. More patients with claudication were taking aspirin prior to their procedure (p = 0.031).
Baseline clinical characteristics of 111 patients with intermittent claudication and 25 patients with critical limb ischemia (CLI)
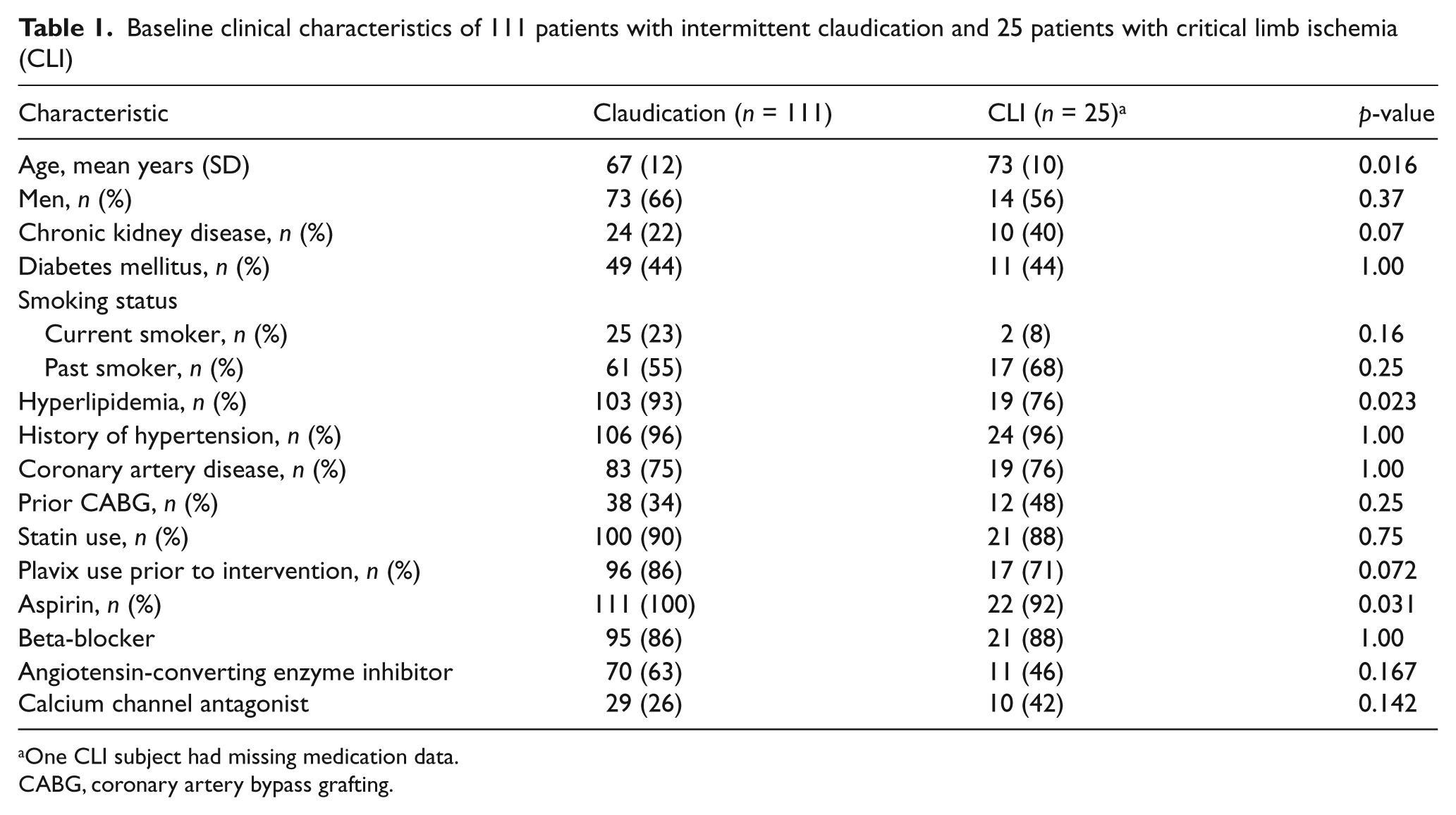
One CLI subject had missing medication data.CABG, coronary artery bypass grafting.
Description of limbs and lesions
There were 142 limbs treated among the 111 patients with claudication and 29 limbs treated among the 25 patients with critical limb ischemia. Successful percutaneous revascularization occurred in 128 of 142 limbs (90%) with claudication versus 25 of 29 limbs (86%) with critical limb ischemia (p-value for difference = 0.51). Limbs that were not successfully revascularized included 14 with claudication and four with critical limb ischemia; all were total occlusions where the lesion could not be crossed.
Both groups of successful interventions were followed for clinical outcomes for 2.5 years (median 1.5 years). Table 2 describes the characteristics of 128 limbs with claudication and 25 limbs with critical limb ischemia which were successfully revascularized. Pre-procedure the ABI ratio was lower in limbs with critical limb ischemia (p = 0.001) compared to limbs with claudication. Also, post-procedure ABI was lower in limbs with critical limb ischemia (p = 0.002) compared to limbs with claudication. However, the change in ABI was similar between both groups (claudication = 0.26, critical limb ischemia = 0.34; p = 0.22). Lesions in limbs with critical limb ischemia were longer (Table 2; p = 0.007), with a higher percentage of chronic total occlusions (p = 0.002) and a higher percentage of TASC II C-D lesions (p = 0.001).
Characteristics in 128 limbs with claudication and 25 limbs with critical limb ischemia (CLI) that were successfully revascularized percutaneously
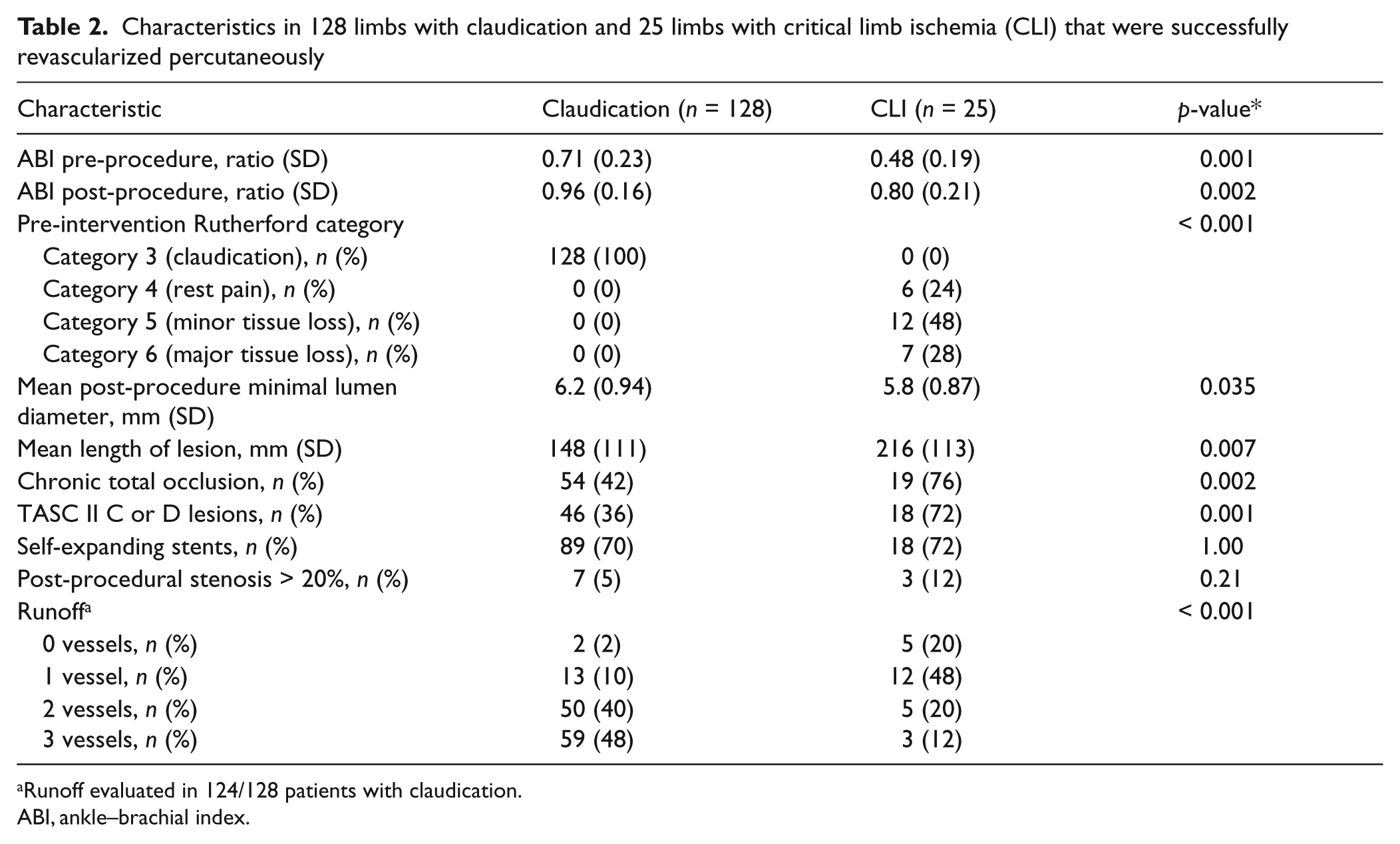
Runoff evaluated in 124/128 patients with claudication.
ABI, ankle–brachial index.
Stents were used in 89 (70%) claudicants and 18 (72%) limbs from patients with critical limb ischemia (p = 1.0). Although not statistically significant, patients with critical limb ischemia had a slightly greater length of stenting (mean = 222 mm, SD = 117 mm) than claudicants (mean = 175 mm, SD = 119 mm; p = 0.12). Runoff below the knee was significantly greater in limbs from claudicants, where 88% had two or more vessel runoff, compared to 32% of critical limb ischemia (Table 2).
Procedural complications
Of the 128 successful procedures for intermittent claudication, four (3%) had complications. These were one hematoma related to a perforated circumflex branch and successfully treated by manual compression, one occlusion of the common femoral access site related to a vascular closure device and successfully treated by balloon angioplasty, and two cases of distal embolization including one asymptomatic posterior tibial artery occlusion and one distal popliteal artery embolus successfully aspirated with a multipurpose catheter.
Of the 25 successful procedures for critical limb ischemia, two (8%) had complications. These were one access site bleed successfully treated with blood transfusion and contralateral access with balloon tamponade of the common femoral artery, and another case of transient intra-procedure hypoxia and hypotension from pneumonia and sepsis.
Outcomes over 2.5 years
The clinical outcomes are listed in Table 3, and Figures 1 and 2 show event curves for failed primary patency, secondary patency, and major adverse vascular events for each group. Although primary and secondary patency were slightly higher in claudicants (Table 2), event curves and survival analysis showed no significant difference in either patency between the groups (Figure 1, Table 3).
Adverse clinical events over 2.5 years in 128 limbs with claudication and 25 limbs with critical limb ischemia (CLI) that underwent initial successful percutaneous revascularization
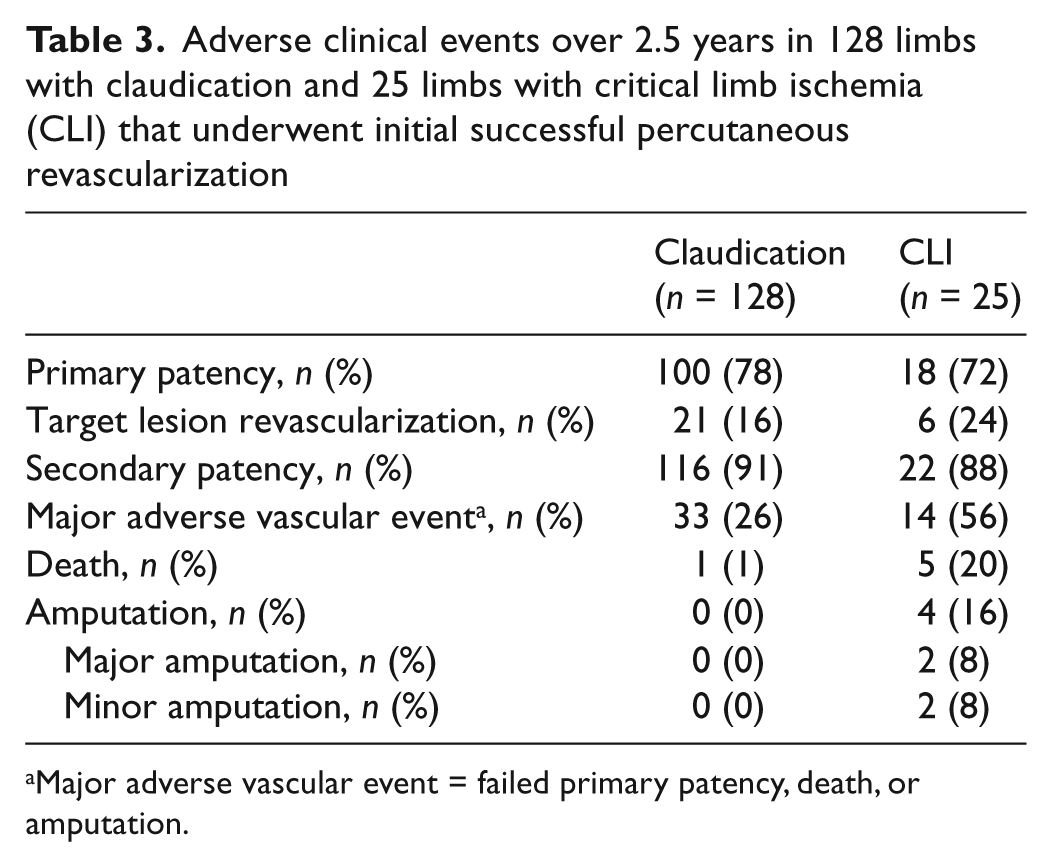
Major adverse vascular event = failed primary patency, death, or amputation.
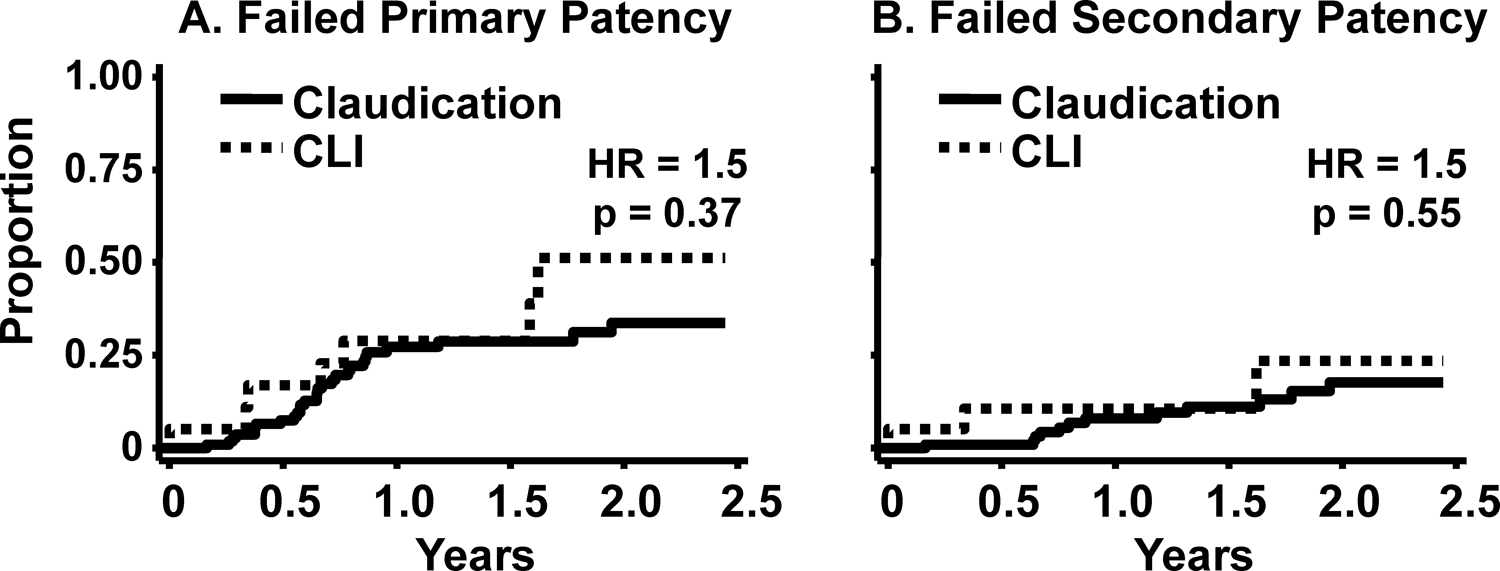
Failed primary (A) and secondary (B) patency rates up to 2.5 years after the index procedure in 128 limbs for intermittent claudication and 25 limbs for critical limb ischemia (CLI) with an initial successful procedure.
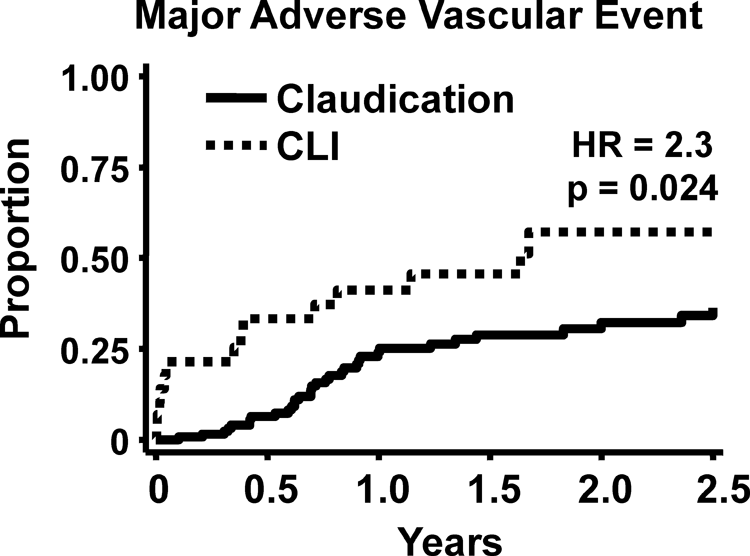
Major adverse vascular event rates up to 2.5 years after the index procedure in 128 limbs for intermittent claudication and 25 limbs for critical limb ischemia (CLI) with an initial successful procedure.
Major adverse vascular events, defined as failed primary patency, death or amputation, were twice as high among limbs with critical limb ischemia (Table 3 and Figure 2). Patients with critical limb ischemia had a higher mortality rate compared to claudicants (Table 3; p = 0.003), with all deaths occurring before a second intervention.
There were four amputations in the critical limb ischemia group and none in the claudication group. These included two planned minor amputations, which were both related to gangrene at the time of initial presentation for the procedure. After successful percutaneous revascularization, one patient required a toe amputation on day 1 and the other a transmetatarsal amputation on day 6. The remaining two patients had major amputations. One patient had successful stenting of an occluded superficial femoral artery but failed percutaneous and surgical attempts to revascularize occluded tibial vessels and required an elective below the knee amputation. The second patient presented to an outside hospital 18 months following successful percutaneous revascularization of the superficial femoral artery with recurrent critical limb ischemia and subsequently underwent an above the knee amputation.
Univariate and multivariate associations for risk, failed patency and clinical events over 2.5 years in critical limb ischemia versus intermittent claudication are shown in Table 4. On univariate analysis, lesion length > 200 mm was associated with failed primary patency (HR = 1.6, p = 0.007) while residual stenosis > 20% was associated with failed secondary patency (HR = 5.0, p = 0.015). The patients with chronic kidney disease tended to have higher failed primary patency (p = 0.06). Runoff was not associated with primary patency (p = 0.82) or secondary patency (p = 0.23). Although the number of deaths over 2.5 years was small, age was associated with increased mortality, while statin and clopidogrel use prior to the index procedure and better runoff were associated with lower mortality (Table 4). Similarly, statin and clopidogrel use prior to the index procedure and better runoff were associated with a lower risk of amputation during follow-up (Table 4).
Univariate and multivariate associations from Cox proportional hazards models for risk over 2.5 years in critical limb ischemia (CLI) versus claudication
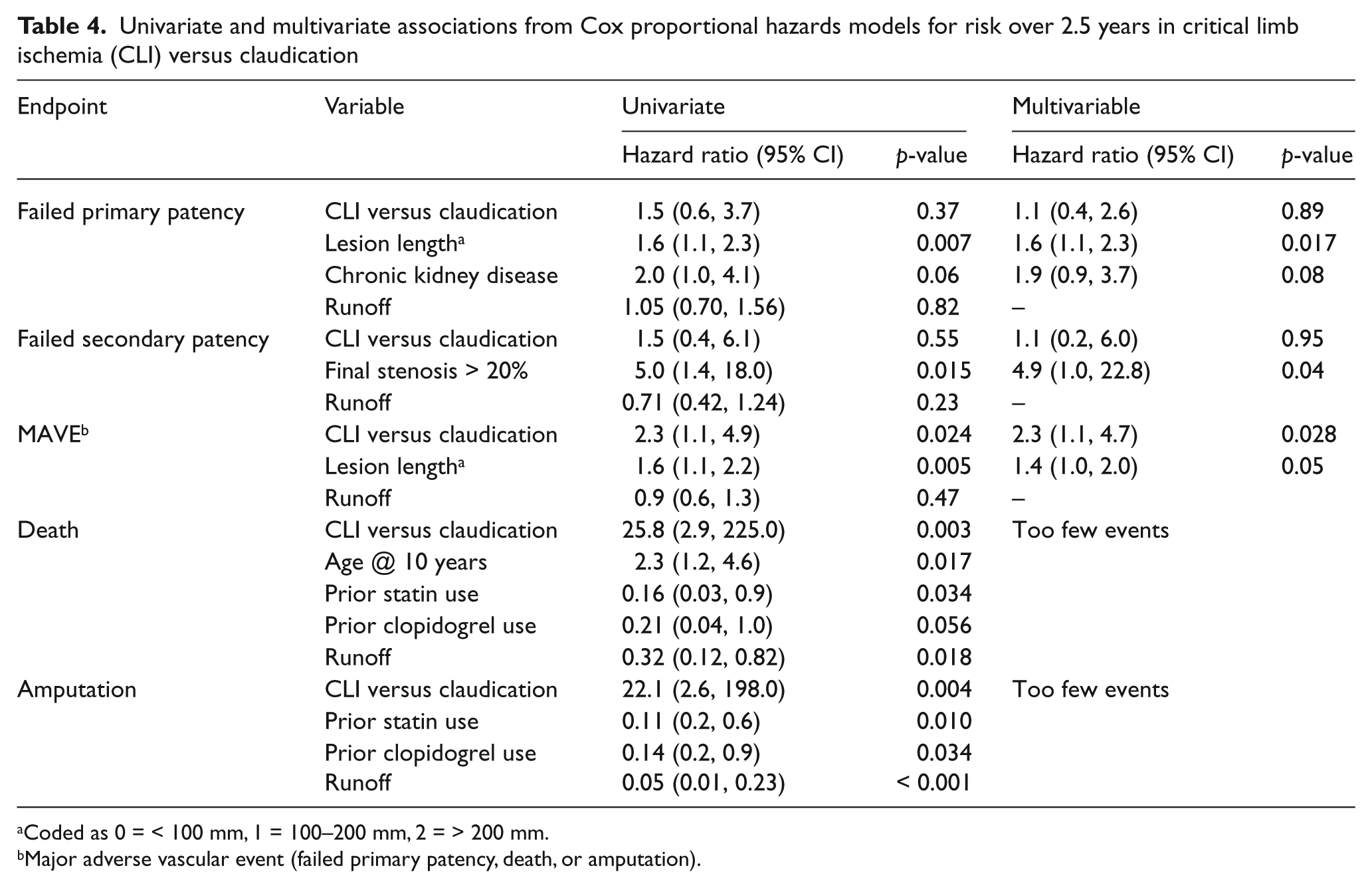
Coded as 0 = < 100 mm, 1 = 100–200 mm, 2 = > 200 mm.
Major adverse vascular event (failed primary patency, death, or amputation).
In multivariable models, primary and secondary patency were similar in limbs with critical limb ischemia and claudication (Table 4). Failed primary patency was more likely with longer lesions and there was a trend for patients with chronic kidney disease to have higher failed primary patency. Only post-procedural stenosis exceeding 20% was a significant factor related to failed secondary patency. In multivariable models, major adverse clinical events remained significantly higher in patients with critical limb ischemia, reflecting the inclusion of death and amputation, which were less common in claudicants. There were too few deaths and amputations to perform a multivariable analysis on these individual endpoints.
Discussion
Critical limb ischemia is usually a consequence of extensive atherosclerosis of the lower extremity arteries, and a break in the integrity of the skin. 1 Contemporary treatment of critical limb ischemia involves either surgical or endovascular revascularization strategies, as medical therapy alone carries a high risk of limb loss. 1 Endovascular therapy for treatment of critical limb ischemia is increasingly the first line of therapy and has several advantages over surgical bypass. These include a less invasive procedure with lower short-term morbidity and mortality, a shorter hospital stay, and lower cost.4–6 However, the durability of percutaneous revascularization may be inferior to surgical bypass.
Patency after revascularization
In the setting of close clinical surveillance for restenosis, we found no difference in primary and secondary patency between percutaneous superficial femoral artery interventions for critical limb ischemia or claudication. Prior reports suggest inferior primary and secondary patency with percutaneous revascularization for critical limb ischemia compared to claudication.7,8 However, these case series are limited by smaller numbers of patients with a mixture of iliac and infra-inguinal disease, 7 and/or shorter (12 months) follow-up.7,8 Our results suggest that the biological response to percutaneous treatments is similar between the two groups and supports increasing trends to endovascular treatment as a first-line therapy for critical limb ischemia. Failed primary patency was higher in longer lesions and greater residual stenosis was associated with failed secondary patency. These factors increase the importance of clinical surveillance for restenosis in patients with critical limb ischemia, as they do for patients with claudication. 2
Major adverse vascular events
This study and others1,9–11 document the higher long-term mortality and amputation risk associated with critical limb ischemia. The increased risk of major adverse vascular events among patients with critical limb ischemia was largely driven by the increased risk of death or amputation, as the patency rates and need for repeat revascularization were similar between the groups. Our long-term mortality rate over 2.5 years was similar to the BASIL trial which randomized 452 patients with critical limb ischemia to bypass surgery or percutaneous revascularization. 6 In that trial only half the patients were alive with either treatment at 4 years. 6 Similar outcomes are reported in several observational studies of bypass surgery for critical limb ischemia with 5-year survival rates of 48–63%.12,13 These studies and our experience highlight the importance of general cardiovascular risk reduction in patients with critical limb ischemia.
As most of the deaths in patients with critical limb ischemia are caused by coronary disease and stroke, the key to improving long-term mortality lies in treating modifiable atherosclerosis risk factors. However, many prior studies show that risk factor modification in patients with critical limb ischemia is suboptimal. In other reports of revascularization for critical limb ischemia, the use of statin therapy ranges from 34% to 46% and antiplatelet therapy ranges from 58% to 80%.6,14,15 In our series, 90% of patients with claudication and 82% of patients with critical limb ischemia were treated with statin therapy and all patients were on at least one antiplatelet agent. Although the number of events was small, prior statin and clopidogrel use in our study was associated with lower mortality and lower amputation rates.
Limitations
Our study is retrospective and included a relatively small number of patients with critical limb ischemia. Although we found no substantial difference in patency and repeat revascularization outcomes between claudication and critical limb ischemia, the hazard ratios were slightly higher with critical limb ischemia, and may be statistically significant with greater numbers of critical limb ischemia patients. Poorer runoff was not associated with patency or revascularization, but was associated with death and amputation. Other studies of critical limb ischemia suggest poorer runoff is associated with worse patency. 16 Our study suggests that poorer tibial and peroneal artery patency is more common in critical limb ischemia and likely reflects more extensive atherosclerosis and worse patient outcomes.
Conclusion
While long-term death and amputation rates are higher in patients with critical limb ischemia compared to claudicants, percutaneous revascularization is associated with similar long-term durability in both groups. Intensive treatment of atherosclerosis risk factors and surveillance for restenosis likely contribute to improving the long-term outcomes with both manifestations of peripheral artery disease.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
The authors have no conflicts of interest to disclose.