
Abstract
Hypothenar hammer syndrome is an uncommon cause of upper-extremity ischemia that is often overlooked in the absence of a thorough occupational and recreational history. Importantly, it is a reversible cause of hand ischemia that, if missed, can lead to significant morbidity and even amputation. The occupational ramifications and quality of life of those affected can be significant. Its relative rarity, set against the ubiquitous use of the hand as a ‘hammer’ is noteworthy. Several other causes of hand ischemia can present similarly; therefore, consideration of other etiologies must be thoroughly investigated. Key distinguishing clinical features, in addition to a detailed occupational and recreational history, may include characteristic sparing of the thumb, the absence of a hyperemic phase in ‘Raynaud’s phenomenon’, and a positive Allen’s sign. Both non-invasive and invasive diagnostic studies, including bilateral upper-limb segmental pulse volume recordings (PVR), arterial duplex examination, and upper-extremity angiography, are complementary to a thorough history and physical examination. Optimal management strategies are not well defined because of its rarity and resultant lack of quality, evidence-based data. Though most cases can be successfully managed non-operatively, micrographic arterial reconstruction may be limb saving in severe or recalcitrant cases. Newer, experimental strategies including selective sympathetic blockage using botulinum toxin A have been reported in a few recalcitrant cases. The brief case description illustrates the typical presentation and potential treatment strategies employed in a difficult case. A review of relevant literature is also presented.
Keywords
Case report
A 51-year-old, right-handed, Caucasian, male factory mechanic with an underlying history of active tobacco abuse, hypertension and hyperlipidemia, awoke with severe, throbbing, left hand pain. His hand felt ‘ice-cold’; ‘like someone pulled my fingernails out’. He denied previous trauma of the involved upper limb or hand. He denied similar past symptomatology. Home medications included zolpidem, simvastatin, losartan, celecoxib, amitriptyline and diltiazem. His work activities were physically demanding, involving heavy use of his hands. He described a history of frequently using his left hand for pounding during previous employment as a farmer. For the previous 6 years, he had been employed as a factory mechanic, requiring less overall use of the left hand as a hammer, though he did still use this technique. Pounding activities using the right hand were much less frequent.
He sought initial evaluation in the emergency department where Raynaud’s phenomenon was suspected and a trial of cilostazol started. Symptoms, however, progressed to dusky, cyanotic-appearing 2nd, 3rd, 4th, and, to a lesser extent, 5th digits (Figure 1) with worsening pain and hypersensitivity. Early signs of tissue loss were noted at the tip of the long finger (Figure 2).
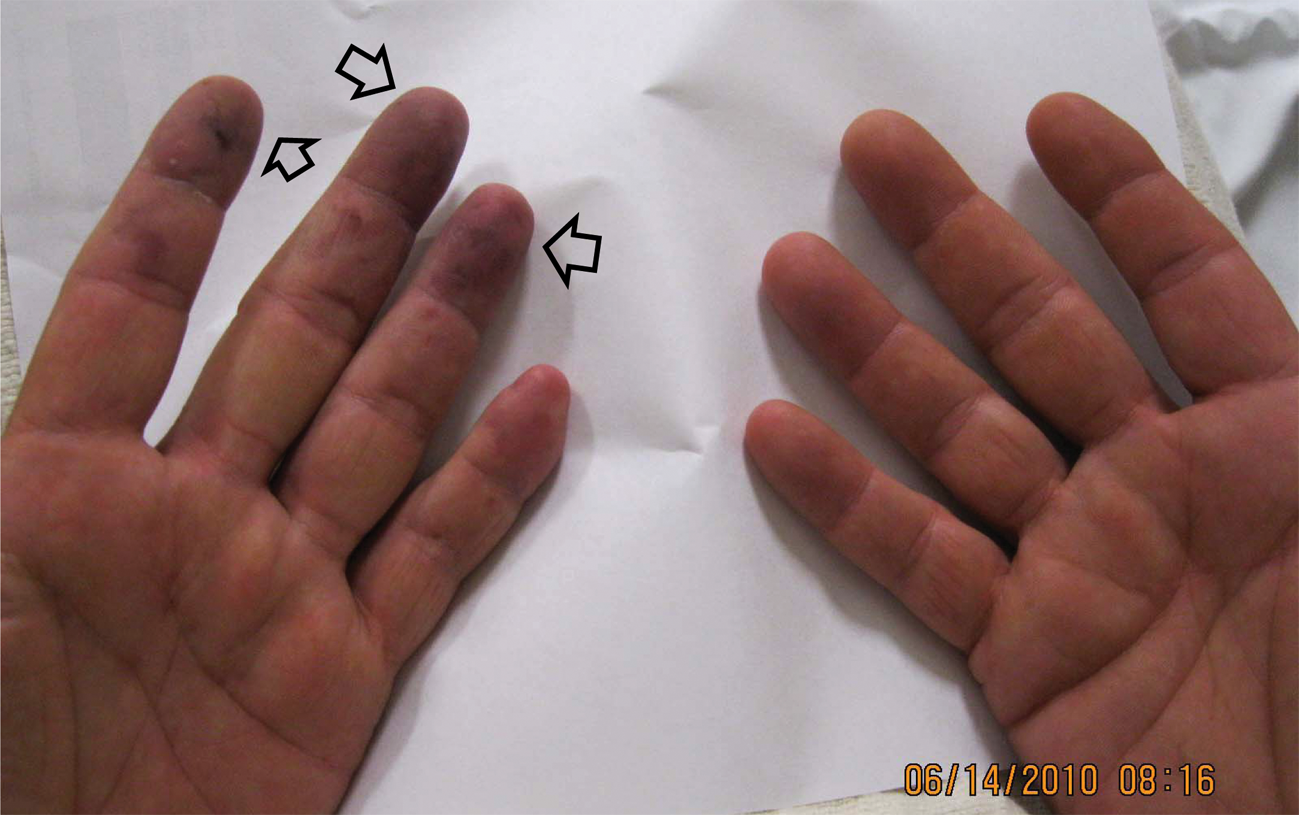
Photographs on initial presentation demonstrating ischemic changes in the tips of the index, middle, and ring fingers (arrows). The findings involving the small finger were more subtle.

Developing ischemic ulceration at the tip of the middle finger (arrows).
Despite equal and symmetric distal pulses, Allen’s maneuver was positive bilaterally. No carotid or subclavian bruits were heard. The remainder of the physical exam was unremarkable. Laboratory studies, including complete blood count, complete metabolic panel, coagulation assays, sedimentation rate and C-reactive protein were all unremarkable. An electrocardiogram showed normal sinus rhythm.
Bilateral upper-limb segmental arterial pressures and waveform analysis were normal with normal radial and ulnar-to-brachial artery indices. However, the digit–brachial index (DBI) of the affected digits suggested severe digital ischemia (Figure 3). Finger photo-plethysmography examination was abnormal in the 2nd through 5th digits (Figure 3). Left upper-extremity angiography revealed normal proximal arterial anatomy to the left wrist. The distal ulnar artery, however, demonstrated significant tortuosity resembling a corkscrew-like configuration (Figure 4). Thrombosis of the digital arteries supplying the affected digits was also noted (Figure 4).
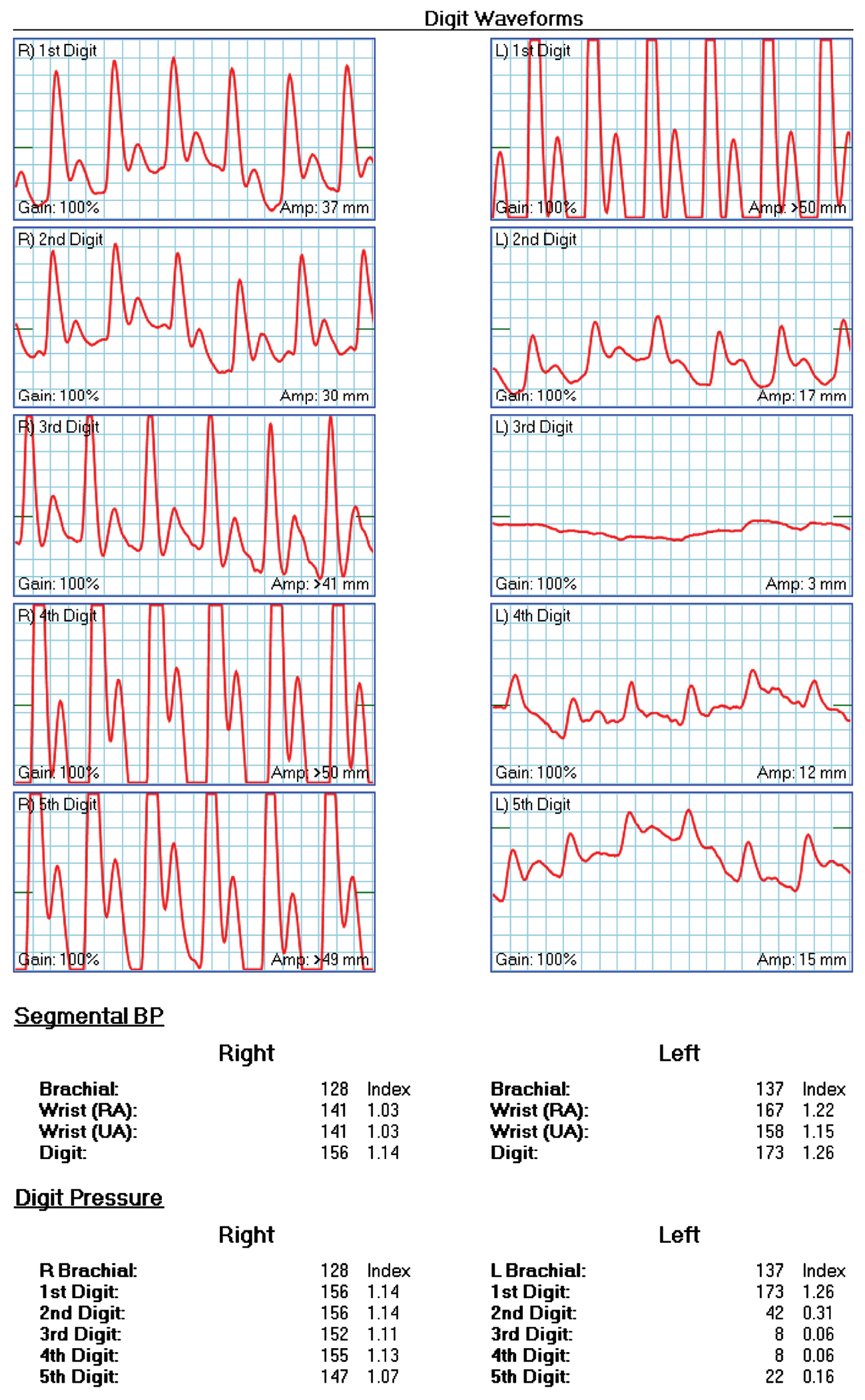
Finger waveforms and pressures showing markedly diminished pressures and waveforms in the index, middle, fourth, and small finger on the left.
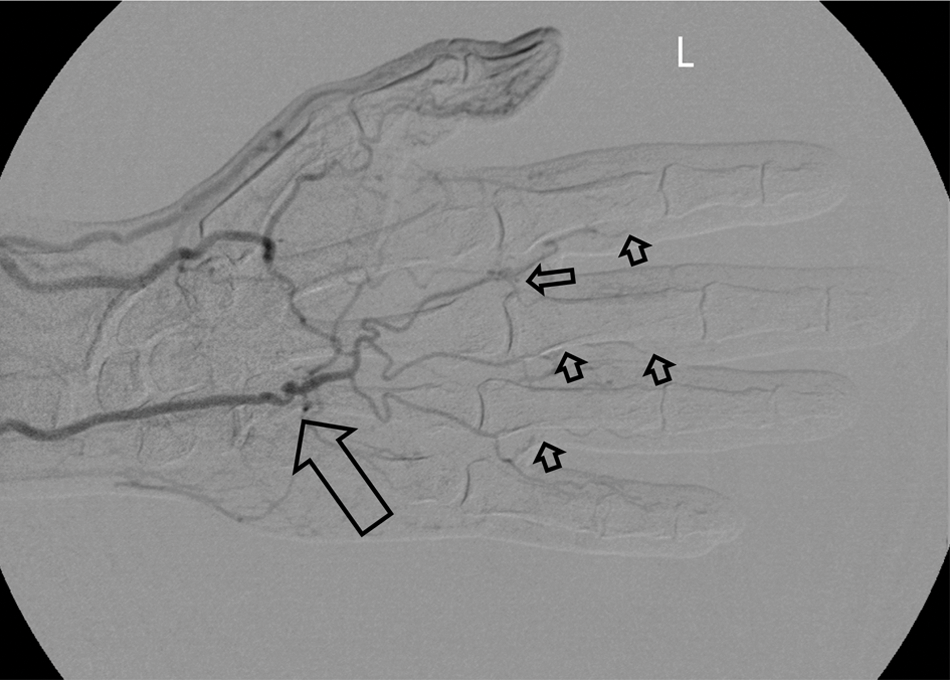
Left hand angiography demonstrating characteristic terminal ulnar artery tortuosity and a corkscrew appearance (large arrow). Proper digital artery occlusions are noted in digits 2–4 (small arrows).
Multi-modality therapy along with local wound care was started. This included an antiplatelet agent, calcium channel blocker, tobacco cessation counseling, hand protection, maintenance of a warm environment, and education on avoidance of further hand trauma. Left stellate ganglionic block was also performed.
Unfortunately, symptoms were progressive with unrelenting pain and frequent nocturnal awaking. At one point, he even requested amputation.
Arterial flow pump and selective peri-arterial sympathetic blockade with botulinum toxin A injections were trialed but were also unsuccessful. Because of progressive symptoms, repeat bilateral upper-extremity angiography was done. Findings were essentially unchanged, although interestingly they did show similar distal ulnar artery findings on the asymptomatic right side as well (Figure 5). Deep palmar arch collaterals, however, were more robust on the uninvolved side. Intra-arterial vasodilators did not change angiographic findings. Ultimately, he required left distal ulnar artery resection and end-to-end anastomosis. Intraoperative findings demonstrated a thickened and pale-appearing segment just distal to the pisiform interposed by normal-appearing vessels both proximally and distally. Histology demonstrated medial hypertrophy and fibrosis.
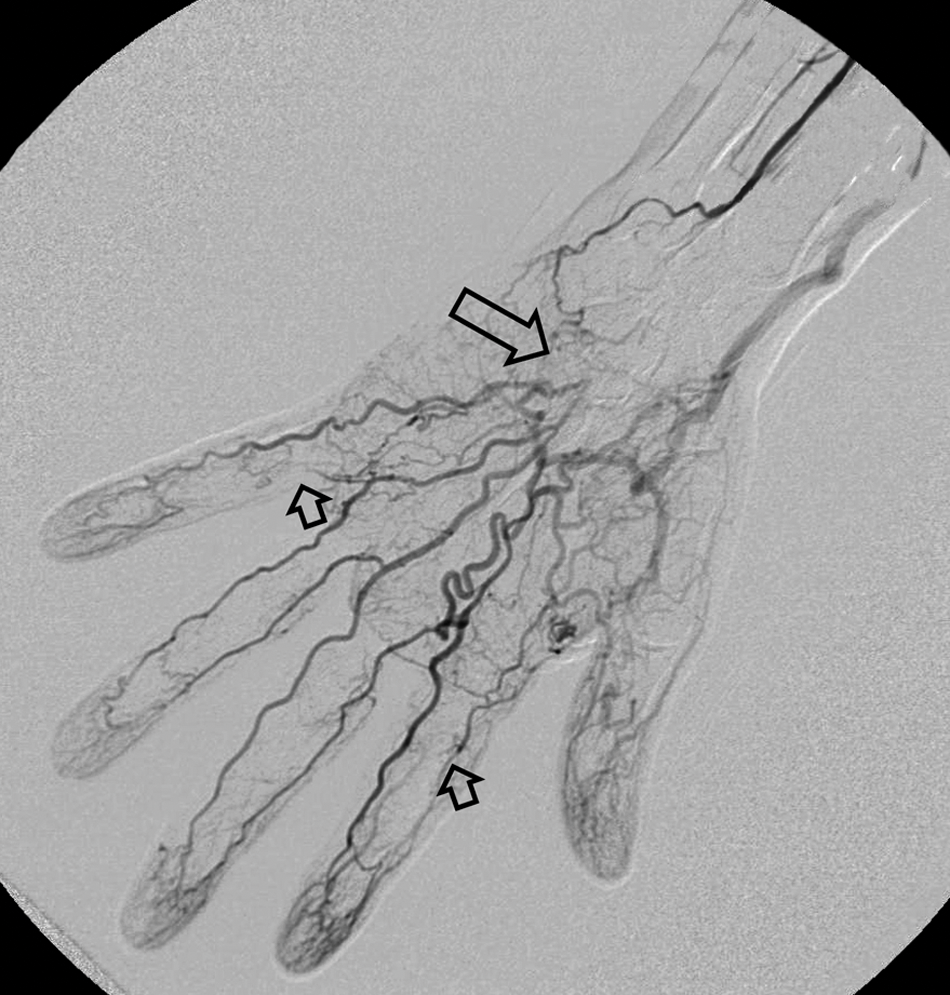
Right (asymptomatic) hand angiogram demonstrating occlusion of the distal ulnar artery (large arrow) with an incomplete superficial palmar arch. Occlusions were noted on the radial aspect of the 5th and index finger proper digital arteries (small arrows). Findings did not change following intra-arterial nitroglycerin. Allen’s sign was positive on this side.
His postoperative course was unremarkable noting improved ‘warmth’ in the involved digits almost immediately. Over the next several months, he made regular progress on range of motion and strength with the assistance of hand therapy. Bedside Doppler evaluation demonstrated a consistently strong triphasic signal over the operative ulnar arterial segment. Within 2 months, the areas of fingertip necrosis had completely resolved and he returned to restricted work activities. At 6 months, he demonstrated full recovery of finger and wrist range of motion, a well-healed surgical scar, and had returned to unrestricted work. His only sequela was mild numbness over the tip of the middle finger in the area of previous ulceration. He was repeatedly advised not to use either hand as a hammer and to avoid vibration exposure.
Introduction and underlying pathophysiology
Hand and finger arterial flow can be compromised by repetitive blunt trauma to the terminal ulnar artery as its position becomes somewhat fixed just as it emerges from Guyon’s canal and runs superficially across the hypothenar musculature (Figure 6). 1 Compression from repetitive use of the hypothenar eminence as a ‘hammer’ can lead to an ‘anvil’ effect, with the vulnerable ulnar artery crushed against the ‘hook’ of the hamate bone (Figure 5). Conn et al., in recognizing this mechanism, astutely coined the term ‘hypothenar hammer syndrome’ (HHS). 2 The syndrome is more commonly seen in carpenters, butchers, mechanics, and others who commonly substitute their hand as a hammer. It has also been well described in several sports and hobbies. Although more commonly occurring in the setting of repetitive micro-trauma, it may occur following a single severe blow to the hypothenar eminence. Undoubtedly, HHS has been around for centuries; however, its original description dates back to the 1930s when its description, histopathology, and surgical management were described by Von Rosen. 3 Guttani may have described the syndrome as early as 1884. 4
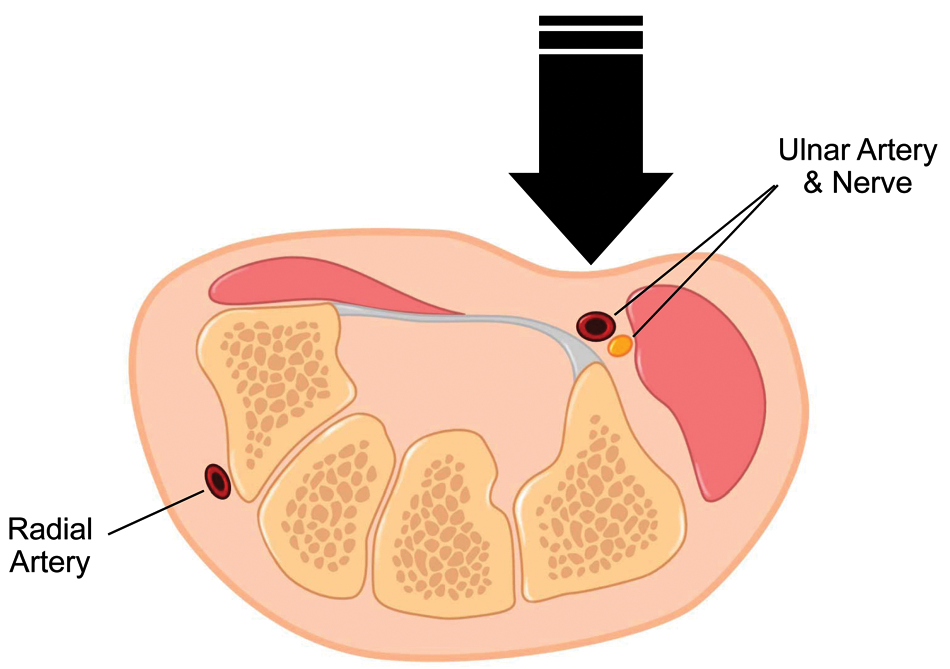
Axial anatomy demonstrating the vulnerable position of the ulnar artery and accompanying nerve (sensory portion) situated just over the hook of the hamate with relatively little superficial protection.
HHS pathophysiology has been theorized to begin with initial vasospasm, eventually leading to intimal hyperplasia and disruption of the internal elastic lamina. 5 The damage can initiate platelet aggregation and encourage thrombus formation at the site of injury. 6 Further, depending on the extent of arterial wall damage, it may lead to aneurysm (true or false), though this occurs much less frequently.5,6 Intra-aneurysmal thrombus formation with subsequent distal embolization often develops in the setting of ulnar artery aneurysm. 6 Additionally, thrombus at the original site of injury, if extensive, may cause reflex vasospasm of surrounding vasculature, further limiting digital perfusion. 5 Finally, vascular trauma to the adventitial layer can cause thickening and fibrosis, ultimately leading to extrinsic scarring and subsequent arterial occlusion. 1
Incidence
HHS incidence is difficult to characterize because of frequent under-recognition but is generally thought to be quite rare. The largest cohort, reported by Ferris et al., found 22 cases among 1300 patients referred to a tertiary vascular center with hand ischemia. 7 A French study found 47 cases among 4148 consecutive patients referred for evaluation of Raynaud’s phenomenon. 8 These studies suggest an incidence of 1.1–1.3% in a group specifically referred to specialty centers for hand ischemia. In the general population, therefore, the prevalence is likely less than 1%.
It is unclear why the incidence of HHS is so rare when a relatively large segment of the population uses their hand in a repetitive fashion. Possible explanations include anatomical variability, subclinical disease, and underlying abnormal arterial histology. These factors may also explain the widely varied presentation ranging from asymptomatic to tissue gangrene. A closer look at these explanations follows.
Anatomical variation of the arterial hand supply has been well characterized. Coleman and Anson, in the early 1960s, detailed several variations of the distal hand arterial supply. 9 The superficial palmar arch, supplied principally by the ulnar artery, is the main blood supply for most of the fingers. 10 In contrast to the deep palmer arch, the superficial palmar arch displays much greater anatomical variability and is often incomplete. Further, its completion on the radial side is often diminutive or absent. The superficial palmer arch arises entirely from the ulnar artery 37% of the time. 11 Finally, the ulnar artery’s location in relation to the hamate bone is somewhat variable and not always positioned directly over the ‘hook’ of the hamate.
Subclinical disease has been demonstrated by Little and Ferguson’s work in the early 1970s. 12 They showed that 62% of motor vehicle mechanics regularly use the hand as a hammer. Although none had symptoms, 14% had subclinical distal or terminal ulnar artery occlusion based on Allen’s test and Doppler ultrasound. 12
Finally, work by Ferris et al. prospectively assessing unilateral hand ischemia in over 1300 patients identified 21 with HHS. Although all underwent angiography of the involved extremity, 13 had bilateral angiography. Strikingly, 12 of 13 (92%) showed similar abnormalities in the asymptomatic ulnar artery. 7 Unfortunately, other large series of HHS are rare and those that have reported on angiographic findings employed only unilateral angiography. 8 Hammond et al. described angiographic ulnar artery irregularity and ectasia 2 years prior to new onset unilateral finger ischemia. 13 Angiography found a thrombosed palmar ulnar artery in the previously described abnormal ulnar artery. 13
Histopathological examination of resected ulnar arteries has demonstrated hyperplastic proliferation of the intima or media and disruption of the internal elastic lamina suggestive of fibromuscular dysplasia. 7 Based on these findings, it has been suggested that an underlying intrinsic arterial abnormality subjected to repetitive trauma could result in clinical HHS. 7 This case lends credence to the theory of an underlying histological defect given the angiographic evidence of bilateral ulnar artery occlusion (Figure 5). It also demonstrates the interplay of how hand dominance and differences in collateral flow can affect clinical presentation, with our patient being asymptomatic on the right side.
Diagnosis and differential considerations
Arriving at the diagnosis of HHS first mandates a high clinical index of suspicion and a complete history and physical, with special emphasis on a detailed occupational and recreational history. It is not uncommon for the diagnosis to be delayed; sometimes with severe consequences. 6 Detailed information on specific job and recreational activities and hand dominance in the performance of these activities is invaluable in providing clinical clues to the diagnosis.
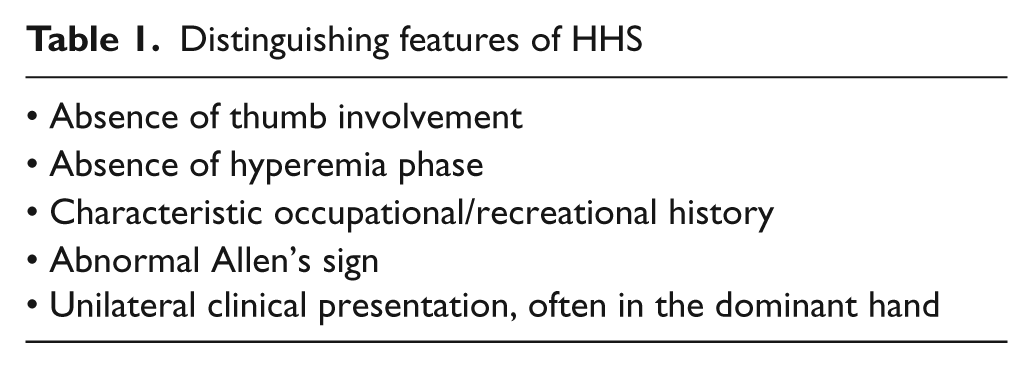
The differential considerations for upper-extremity ischemia, although quite broad, can be narrowed by a detailed history and physical examination. Approximately 50% of hand ischemia can be localized to a proximal embolic source. 14 Embolization from the heart, aortic arch, or proximal upper-limb arteries should always be considered. Specific examples include atrial fibrillation-induced intra-cardiac emboli, mycotic emboli in the setting of endocarditis, and subclavian artery aneurysm from thoracic outlet syndrome. More distal, small vessel processes have been described and include secondary Raynaud’s phenomenon resulting from scleroderma, systemic lupus erythematosis, or rheumatic disease. Thromboangiitis obliterans (TAO) or Buerger’s disease can share several features of HHS such as distal digital ulcerations, cold sensitivity, and abnormal Allen’s test along with corkscrew-like vessel changes on angiography. 15 However, unlike HHS, TAO presents more symmetrically, often with lower extremity involvement. Further, multiple extremity involvement is common. Initial symptoms characteristically start with claudication (often in the arch of the foot) and may progress to distal ischemia and ulceration. 15 Often, ischemic ulcers will already be there upon presentation. 15 Table 1 summarizes the major distinguishing characteristics found in HHS.
Distinguishing features of HHS
Other diverse causes of small vessel disease or vasospasm include dysproteinemia, cryoglobulinemia, myeloproliferative disorders, malignancy, and frostbite. 14 In general, systemic processes tend to present bilaterally whereas HHS is more typically unilateral. 1 Finally, attributing distal upper-extremity ischemia to isolated ulnar artery atherosclerosis should be cautioned as this finding is quite uncommon and debatable in the literature. 16
The Hand Arm Vibration syndrome (HAVS) is particularly difficult to distinguish from HHS in that both have typical occupational exposure with similar symptoms. HAVS is a more general disease process, typically involving nerves and muscles in addition to arterial structures. Moreover, HHS can be seen concomitantly in those with HAVS. Kaji et al. found that 24 of 293 subjects with HAVS also had HHS. 17 Whereas HAVS typically presents with classical Raynaud’s phenomenon, those with HHS almost invariably will not exhibit the hyperemic phase and often (but not always) will have positive Allen’s sign. 11 Those with vibration-induced HHS do not have ulnar artery aneurysm and typically report a long history of vibration exposure. 17 HHS spares the thumb whereas HAVS can affect any digit. 6 Finally, the natural history of symptom progression is helpful. HAVS symptoms usually start in the digit bearing the brunt of the vibration exposure (most often the little finger) and, over time, spread medially to involve other fingers. 11
HHS can cause ulnar artery aneurysm but is only found in a minority of cases. Therefore, other causes of aneurysm should be considered. Other known causes of isolated ulnar artery aneurysm include congenital, mycotic, and penetrating trauma. 11
Imaging modalities in the diagnosis of HHS
Diagnostic studies complement the complete history and physical exam with non-invasive assessment followed by confirmatory angiography in most cases. As illustrated in our case, non-invasive digital photo-plethysmography and segmental/digital pressures (Figure 3) can assist in quantifying the degree of digital ischemia and localize the area of obstruction. Arterial duplex imaging is useful in identifying the precise location and etiology of the ischemia, especially in the case of aneurysms.5,14 Magnetic resonance imaging (MRI) has shown good correlation with angiography and can also better assess surrounding soft tissue structures which may be clinically pertinent. 1 In five HHS patients, magnetic resonance angiography (MRA) was diagnostic in all cases showing detailed images, including embolic obstructions as distal as the common digital arteries. 18 Although distal digital occlusion remained challenging with MRA, bilateral comparison proved helpful in determining pathology from vessel variants. 18 Multi-slice computed tomographic angiography (CTA) has also shown comparable diagnostic accuracy, offering the added advantage of ruling out underlying bony abnormalities in select cases. 19 Bilateral catheter-based angiography, including proximal vasculature along with magnified views of distal hand vasculature, remains the gold standard for complete and detailed assessment of hand ischemia. Unlike CTA or MRA, angiography can provide detailed arterial anatomy in the rather complex and variable hand vasculature, which is often helpful in surgical planning. 10 Regardless of the imaging modality, it is important to thoroughly assess the proximal segments in order to not miss a proximal source of obstruction or embolization. 14
Arteriographic findings in HHS commonly show alternating areas of stenosis and ectasia (corkscrew) of the palmer ulnar artery (Figure 4). Tortuosity and redundancy have also been described. Abrupt occlusion of the common and proper digital arteries are also typical findings. Less commonly, palmar (or distal ulnar) artery aneurysm is seen.
Arteriographic classification of HHS has been reported, although this was done in a group with vibration-induced HHS. 17 It is unclear whether classification of arteriographic findings influences therapeutic approach.
Clinical manifestations
The presenting symptoms of HHS are classically very similar to our case. Based on natural history studies, the typical patient is a 40-year-old male smoker with a several year history of repetitive hand trauma.7,8 Over 90% of the time, the dominant hand is affected. 8 The long finger is most frequently affected followed by the ring and small finger. 7 The mean duration of symptoms prior to diagnosis was 2.5 months in one study, highlighting its initial under-recognition. 8
Invariably, patients complain of pain, pallor, cyanosis, coolness, and color changes in the involved digits with characteristic sparing of the thumb. The degree of ischemia can range from mild color changes to frank ischemic ulceration and gangrene. Paresthesia, hypothenar tenderness, and hand hypersensitivity (especially to cold) have been reported and likely relate to the close approximation of the sensory portion of the ulnar nerve and artery through Guyan’s canal (Figure 5). Pulsatile mass over the hypothenar eminence has been reported in cases of ulnar artery aneurysm.20,21 In addition to digital ischemia, another key physical exam finding may be a positive Allen’s sign. In order to avoid a false–positive result, avoidance of finger and wrist hyperextension should be emphasized. Further, a negative Allen’s test does not rule out HHS. Kaji’s data showed that 14% of individuals with HHS had a negative Allen’s test. 17
Management of HHS
Optimal treatment is not known in this syndrome. Given its rarity, there are no prospective randomized trials comparing medical, surgical, or interventional treatments. Most treatment data are derived from small retrospective case series. Acuteness of symptom onset, degree of ischemia, type of underlying ulnar artery pathology (thrombosis versus aneurysm) and status of collaterals all carry weight when determining the optimal approach. Most authors suggest a more aggressive, interventional approach in acute, limb-threatening ischemia. Inadequate response after multi-modality medical therapy can also be an indication for invasive intervention. Those with competitive sport-induced HHS may be able to return to their sport faster with surgery. Finally, surgical repair for aneurysm formation is favored.
Regardless of the specific therapy pursued, some general principles universally apply to all those with HHS. Patient education on hand protection, maintenance of a warm environment, and avoidance of exacerbating activities form the foundation of care. Tobacco cessation cannot be overemphasized. Adjunctive medications and specialized smoking cessation counseling should be aggressively pursued. It has been shown that those who continue to smoke consistently fail both conservative and operative care. 8 Our case demonstrates how challenging smoking cessation can be. Our patient continued to smoke even after successful operative arterial reconstruction.
Many modalities are aimed at improving distal blood flow. Simply maintaining a warm environment will avoid cold-induced vasospasm. Sympathetic nerve ablation via cervical block has not been favored in the few studies that have examined this. 22 Anticoagulation with heparin or Coumadin has been helpful in case reports, though the most appropriate setting is unclear. Most surgeons advocate post-reconstructive anticoagulation for a period of time. Rheostatic therapy has been mentioned in case reports and was trialed in our case without effect. Antiplatelet and vasodilator therapy is initiated in a majority of cases despite the lack of data on efficacy. Intra-arterial thrombolysis offers the theoretical advantage of disintegration of distal embolic events unreachable by classical surgical thrombectomy. 23 Thrombolysis has been described as a primary modality and as adjunctive treatment with various surgical approaches. Thrombolysis may be beneficial early on, when thrombus is unorganized but seems to be less effective in atheroemboli and organized thrombus. In four patients with HHS treated with primary intra-arterial thrombolysis, three had clinical improvement despite inconsistent angiographic results. 22 Major bleeding did not occur and surgery could be safely performed after intra-arterial thrombolysis. 22
Surgery consists mainly of three approaches: ligation of the diseased ulnar artery, direct end-to-end anastomosis, or vascular reconstruction with vein interposition graft. Ligation, performed to prevent further thromboembolism, requires proven adequate collateral circulation and some have used a DBI of 0.7 as the cut point in determining simple ligation versus surgical reconstruction. 24 Although the nutritional benefits of revascularization would seem obvious, Lifchez’s retrospective data suggest a more complex pathophysiology. 25 In a group of 14 patients treated with surgical reconstruction, late postoperative occlusion rates were greater than 40%. Paradoxically, however, digital arterial flow (quantified by DBI) was significantly better in those with late postoperative occlusion. Further, there was a trend toward better functional status in those with late postoperative occlusion. It was postulated that reconstruction allowed sufficient time for adequate collateral flow development.
Intermittent pneumatic compression (IPC) has been investigated in severe lower extremity PAD where revascularization options have been exhausted. It has been shown to improve vascular perfusion, increase healing rates, and result in limb salvage in those patients with no reconstructive options. 26 It is unclear, however, if these outcomes can be extrapolated to the unique pathophysiology of HHS. In our case, it is difficult to determine whether IPC was effective as compliance was not well documented. Subjectively, there was no substantial improvement.
Botulinum toxin A (Botox) has been shown to alleviate ischemic pain and promote ischemic ulcer healing in Raynaud’s phenomenon. Several retrospective trials over the past 7 years have evaluated the effects of Botox in Raynaud’s (primary and secondary) phenomenon.27–29 Although we attempted Botox injections in our patient, it should be emphasized that most studies examining the efficacy of Botox in hand ischemia excluded those with arterial obstruction.
Conclusion
HHS should be suspected when hand ischemia occurs in those who repeatedly use their hand as a hammer, either at work or play. Immediate definitive testing should be aggressively pursued as early diagnosis allows for more effective therapeutic options. Delayed diagnosis, as in most conditions, can have morbid consequences. A multidisciplinary, team approach is encouraged. Several basic principles apply to all cases including behavioral modification, hand protection, and smoking cessation. Optimal therapy, particularly the indications and timing of surgery, remains debated in the literature.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
None declared.