
Abstract
The shortage of Allergy & Immunology providers in the United States restricts access to specialty care. Telemedicine has the potential to expand access beyond physical locations, however, little is known regarding patient preferences for tele-allergy or the ability to successfully manage atopic conditions virtually. This retrospective analysis of a tele-allergy program at the Veterans Health Administration demonstrates that tele-allergy can provide efficient allergy care for veterans, including rural patients, although some reliance on local ancillary services was necessary. A hybrid model of virtual and in-person care is likely needed in Allergy & Immunology to overcome geographical barriers and optimize resource allocation.
Introduction
The Allergy & Immunology physician workforce in the United States is relatively small, with approximately 5,133 active allergists as per the Association of American Medical Colleges 2023 workforce report. 1 Over 30% of allergists currently in practice are aged 65 and older, and there are approximately 160 physicians completing Allergy & Immunology fellowship training each year.1,2 Given these statistics, it is predicted that the Allergy & Immunology physician workforce will continue to decline over the next decade, worsening the current challenges of meeting the demands of an increasing patient population. 3 Telemedicine has the potential to expand care beyond physical locations and close access gaps nationally. Virtual care technology is already existing and has the advantage of fast implementation. In addition, patients have become increasingly telehealth-competent since the start of the COVID-19 pandemic.
Access to care and reducing disparities in healthcare are priorities of the Veterans Health Administration (VHA). In September 2021, the Miami Veterans Affairs (VA) Healthcare System implemented a tele-allergy program for Veterans Integrated Service Networks (VISN) 8, a network of seven facilities located in Florida, South Georgia, and the Caribbean, with the goal of using a digital health strategy to improve outpatient Allergy & Immunology access and continuity of care for veterans with limited in-person options.
Methods
Data collection
This is a retrospective chart review of patients seen by the VA VISN 8 Tele-Allergy program between January 1 and August 31, 2023. Primary interests included proportion of new consults suitable for tele-allergy, patient willingness to receive allergy care via telehealth, proportion of patients transferred to in-person care after virtual evaluation, and proportion of video visits converted to telephone due to technology failure. Patient preference for in-person care, the need for specialized in-person testing and/or treatment, and digital vulnerability were considered potential barriers to tele-allergy. Digital vulnerability was defined as the inability to perform a video telehealth visit due to poor internet access, lack of device, or a patient's technological fluency. Descriptive analytics were performed on Microsoft Excel. Rurality data was provided by the VA Office of Rural Health.
Tele-allergy program overview
Veterans enrolled in a VISN 8 VA facility that lacked an Allergy & Immunology provider (“patient-side” remote site) and required outpatient allergy evaluation and/or treatment were referred to the Tele-Allergy program. The program provided care via synchronous video-to-home telehealth. The tele-allergy providers, including a Board-Certified Allergist & Immunologist and an Allergy & Immunology Advanced Practice Nurse Practitioner, were located at the Bruce W. Carter Miami VA Medical Center (central hub). Video visits were performed using VA Video Connect, a video-based platform that allows providers to interact with patients through their mobile devices or computer. Telephone visits were performed in the event of video technology failure despite troubleshooting efforts. Tele-allergy providers were able to view the patient-side electronic medical record (EMR), prescribe medications, and utilize ancillary services at the patient's local VA facility, such as laboratory services, pulmonary function testing, and radiology services. For patients with rash, tele-dermatology images were obtained in the patient's local VA primary care clinic and were uploaded to the EMR for review prior to consultation.
Allergy skin testing and allergen immunotherapy (AIT) were not available through tele-allergy or at the patient-side VA facility. Patients who required either of these services were referred for in-person care with a local private community allergist through the VA's Community Care Program.
Referral workflow
Tele-allergy consults were initiated in the patient-side facility and submitted as an interfacility consult request. All referrals were reviewed by a tele-allergy provider for appropriateness. Patients referred for rhinitis were required to have a respiratory serum specific IgE panel appropriate for their area or have records of previous allergy skin testing. Depending on the reason for referral, other pre-work such as other labs, pulmonary function testing, and/or imaging may have been requested prior to the initial visit. Consults not suitable for initial evaluation via telehealth were referred to the Community Care program for in-person care. The suitability of a consult for virtual versus in-person care was decided on a case-by-case basis at the discretion of the triaging tele-allergy provider. Patients eligible for telehealth were offered appointments with tele-allergy. Patients who declined telehealth were referred to the Community Care program for in-person care.
Results
Consult triage and patient preferences
There were 636 new patient consult requests during the review period. The referral patient population was 76% urban and 24% rural. Eighteen consults (2.8%) were not suitable for initial evaluation via telehealth and were forwarded for in-person care for the following reasons: specific drug allergy skin testing (5 patients); food allergy skin testing (5 patients); AIT (4 patients); atopy patch testing (1 patient); aeroallergen skin testing (1 patient); and rash requiring in-person skin exam (1 patient). Six-hundred and eighteen consults (97%) were suitable for initial evaluation via telehealth. Of these, 517 patients were successfully contacted. Eighty-one patients (16%) refused telehealth due to preference for in-person care (77 patients, 95%) or digital vulnerability (4 patients, 5%).
Clinical encounters
There were 845 tele-allergy visits for 581 unique patients (439 new, 142 previously established) during the review period. Most patients were male (71%). The average age was 52.5 years with an interquartile range (IQR) of 21 years. The most common primary diagnosis at initial consultation was rhinitis (259 patients, 59%), however, a variety of primary diagnoses were seen (Table 1). Thirty-three visits (4%) were converted to telephone due to technology failure despite troubleshooting efforts. Among patients who experienced a technology failure, the average age was 53.6 years with an IQR of 31 years.
Primary diagnosis of new patients at initial consult visit.
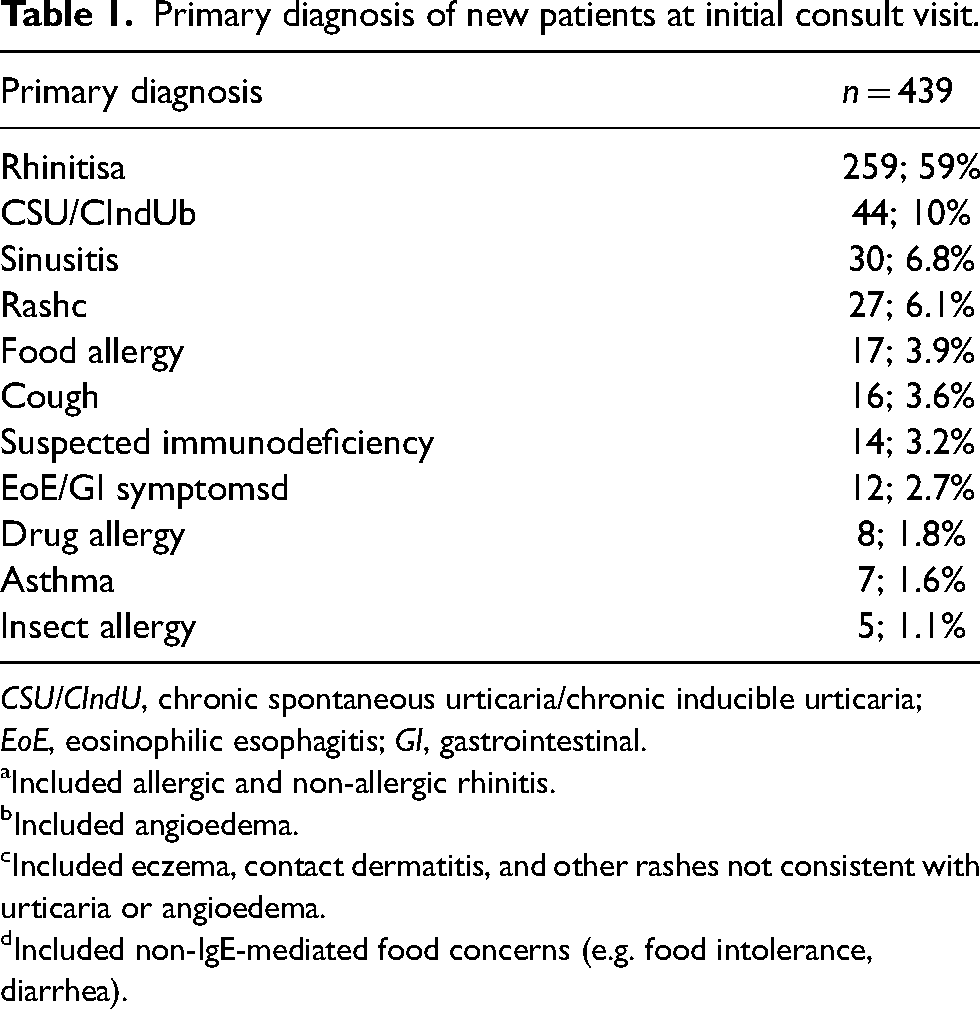
CSU/CIndU, chronic spontaneous urticaria/chronic inducible urticaria; EoE, eosinophilic esophagitis; GI, gastrointestinal.
aIncluded allergic and non-allergic rhinitis.
bIncluded angioedema.
cIncluded eczema, contact dermatitis, and other rashes not consistent with urticaria or angioedema.
dIncluded non-IgE-mediated food concerns (e.g. food intolerance, diarrhea).
Transfers to in-person care
Fifty-two virtual patients (9%) were subsequently transferred to in-person care based on best medical interest and shared decision making between the patient and the tele-allergy provider. Thirty-eight patients (73%) were transferred to start treatment with AIT. Fourteen patients (27%) were transferred for allergy skin testing. There were no patient requests to transfer due to dissatisfaction with telemedicine.
Discussion
Strategies to close gaps in access to Allergy & Immunology care are needed. We found that most veterans in VA's VISN 8 (84%) were comfortable with telemedicine and were receptive to a digital health strategy for their allergy care. Technology failure impacted 4% of video visits, while only 0.5% of patients declined due to digital barriers, despite a 24% rural population. While patient satisfaction surveys were not performed, it is notable that no patients requested transfer to in-person care due to dissatisfaction with telemedicine.
Several studies have demonstrated the utility of telemedicine in managing asthma. 4 However, there is limited data on its use for evaluating and managing other conditions commonly treated in Allergy & Immunology. 5 In our program, most patients were referred for chronic rhinitis, though a wide variety of atopic conditions were also evaluated and managed. Like others, we observed that only a small percentage of patients were referred primarily for asthma. 5 Nevertheless, 22% of our cohort had asthma managed as a secondary diagnosis (data not shown).
Most referrals were suitable for initial evaluation via telemedicine. In 2016, Waibel reported that 24% of established tele-allergy patients were subsequently recommended for an in-person visit. 5 In contrast, we observed that only 9% of virtual patients required in-person care. However, our program utilized ancillary services at local VA facilities to ensure accurate diagnosis and effective treatment guidance, making it not completely virtual. These ancillary services, though, are considered routine in many healthcare systems and are widely accessible. A key limitation to fully virtual allergy care is the need for specialized therapies and testing that require in-person visits. Among our tele-allergy patients who needed in-person care, the most common reason was AIT. To enhance the reach and efficiency of tele-allergy services, efforts should focus on expanding local support for AIT clinics.
Overall, our findings demonstrate that tele-allergy can effectively address access gaps and provides a model for increasing specialty care accessibility for patients with limited in-person options. A hybrid model of virtual and in-person care is likely needed to create the best overall outcomes in Allergy & Immunology. Further studies are needed to assess the broad applicability of our findings, evaluate the long-term clinical outcomes of tele-allergy, measure patient satisfaction, and identify ways to enhance tele-allergy for delivering value-based care.
Footnotes
Acknowledgements
The authors would like to thank the Bruce W. Carter Miami VA leadership and the VISN 8 Specialty Care Integrated Clinical Community for their continued support of tele-allergy.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Ethics Committee of the Bruce W. Carter Miami VA Medical Center waived the need for ethics approval and patient consent for the collection, analysis and publication of the retrospectively obtained and anonymized data for this non-interventional study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.