
Abstract
Introduction
The COVID-19 pandemic dramatically affected the financial performance of hospitals across the U.S. The prompt availability of telehealth options likely impacted both a hospital's healthcare options and opportunities for revenue in the short-term. The aim of this study was to explore the association between early adoption of telehealth and changes in revenue during the early phase of the pandemic, and to compare whether the results differed between rural and urban hospitals.
Methods
We performed first-difference regressions on a cross-sectional dataset of 1,742 U.S. hospitals. Our dependent variables were percent changes in four categories of revenue between 2019 and 2020: inpatient, outpatient, gross, and net. The adoption of telehealth and remote patient monitoring as of 2019 served as the primary independent variables of interest. We controlled for changes in hospital characteristics from 2019 to 2020, including case mix index and number of employees.
Results
Our results suggest that telehealth adoption prior to the COVID-19 pandemic was associated with significant increases in all four revenue categories from 2019 to 2020, ranging from 1.79% (net patient revenue) to 2.92% (outpatient revenue). However, RPM implementation in 2019 was associated with significant declines in gross patient (0.08%) and outpatient revenue (1.50%). The results were largely similar across rural and urban locations.
Discussion
Adopting telehealth before the onset of COVID-19 helped hospitals increase revenue during the initial phase of the pandemic. Alternatively, implementation of remote patient monitoring was associated with revenue declines, likely due to limited ability for monetization. Whether these relationships have persisted needs further investigation.
Introduction
Proponents of telehealth have long argued that it has the potential to improve health care access and patient experience, while increasing efficiency, reducing costs, and offering revenue opportunities.1–8 Despite evidence supporting telehealth as a potential solution to improve health care access and delivery, the use of telehealth by hospitals was relatively limited prior to the COVID-19 pandemic.9,10 By 2019, physicians reported being optimistic about improvements to practice efficiency due to telehealth, but telehealth adoption and use was growing at a modest rate.11–13
On 31 January 2020, the U.S. Department of Health and Human Services (DHHS) declared a public health emergency in response to COVID-19. As a result, virtually all in-person outpatient visits and elective procedures were cancelled across most of the country, and many hospitals suffered a significant drop in volume.14,15 From the beginning of the outbreak, telehealth was seen as a way to maintain critical access to care while keeping both patient and providers safe from exposure to COVID-19. 16 The emergency declaration was quickly followed by comprehensive changes to telehealth policies by the federal government, private insurers, and state legislators that aimed to broaden telehealth access and use. 17 In particular, the Centers for Medicare and Medicaid Services (CMS) expanded telehealth reimbursement by removing restrictions on “originating sites” (previously limited to clinics, hospitals, and other specific health facilities in rural locations); allowing e-visits and remote evaluation for all patients (instead of only established patients); and expanding the list of Current Procedural Technology (CPT) codes eligible (including 99201–99215 for office/outpatient visits and 99421–99423 for independently billed evaluation and management e-visits).18,19 These changes led to dramatic increases in telehealth use during the early months of the pandemic. 20
The pandemic had important implications for revenue generation by hospitals and practices.21,22 Hospitals across the country turned to telehealth not only to help provide access to health care during the public health emergency, but also to mitigate some of the revenue losses during the COVID-19 pandemic.6,13 Nonetheless, not all hospitals and practices had telehealth capacity prior to the COVID-19 pandemic. We hypothesized that hospitals that adopted telehealth before the COVID-19 emergency declaration were able to respond in a timelier manner to the health emergency and, therefore, experienced smaller decreases in revenue during the early phase of the pandemic compared to the hospitals and practices that did not have telehealth capability prior to 2020.
Before the COVID-19 pandemic there was evidence that telehealth could improve hospital finances.23–25 However, two recent studies suggest a negative relationship between the two, with important rural-urban differences.7,26 The advent of the pandemic and the subsequent exponential increase in telehealth use created a newfound interest in how the technology influenced fiscal outcomes. Several previous studies have examined how telehealth adoption and use influenced hospital revenue changes during the COVID-19 pandemic. However, these studies are either simulations 27 or focus on a particular medical specialty. 4 To our knowledge, this is the first study to use national U.S. hospital-level data to assess the relationship between telehealth adoption prior to the COVID-19 emergency declaration and revenue changes during the initial phase of the pandemic.
One particularly relevant type of telehealth is remote patient monitoring (RPM), defined as the use of technology to gather physiologic data from patients in one location (e.g., their home) and transmit that data to a health provider in another location (e.g., hospital or doctor's office) for analysis. RPM has been shown to be important for hospitals to monitor discharged COVID-19 patients, but no analysis we are aware of has focused on its financial impact during the pandemic. 28
Methods and approach
Data sources and measures
We matched national hospital-level data on telehealth and RPM adoption in 2019 from the American Hospital Association's (AHA) Annual Survey of Hospitals Information Technology (IT) Supplement with revenue data (2019 and 2020) from the American Hospital Directory (AHD). The product of our data aggregation was a cross-sectional dataset of 1,742 hospitals. About one-third of the hospitals in our sample were rural. A hospital was considered rural if it was in a county with a Rural-Urban Continuum Code (RUCC) greater than or equal to four. These data have been used before to document telehealth adoption and use by academic researchers.5,8,25,29
The independent variables of interest (telehealth and RPM adoption in 2019) were retrieved from the following questions in the AHA IT Supplement (2019): (1) “Does your hospital currently have a computerized system which allows for: Other Functionalities: Telehealth?” and (2) “Does your hospital currently have a computerized system which allows for: Other functionalities: Remote patient monitoring?” These questions measure whether hospitals had Electronic Health Record (EHR) systems with telehealth and remote patient monitoring functionality. For example, large EHR providers like EPIC and Cerner support telehealth and remote patient monitoring capabilities such as patient messaging, uploading images, symptom checkers, home monitoring devices (blood pressure monitors or pulse oximeters), video visits, and screen sharing, amongst others. The benefits of having an EHR system that is linked to telehealth services include prompt verification of eligibility, immediate access to patient's health records, and linkage with insurance information. However not all hospitals have EHRs with these functions.29,30
Four categories of revenue data (inpatient, outpatient, gross and net) in 2019 and 2020 were retrieved from American Hospital Directory (AHD) data. Most hospitals follow fiscal years that end on September 30, thus the FY20 data begins prior to the pandemic (October 2019) and ends six months into it (September 2020). Reported revenues came from annual Medicare Cost Report Worksheets filed by each hospital (and compiled by AHD), and Supplementary File 1 provides data on the specific worksheet and lines used for each revenue category. It is relevant to note that the U.S. Congress gave $175 billion in subsidies to aid hospitals and practices during the COVID-19 emergency as part of the Coronavirus Aid, Relief and Economic Security (CARES) Act and the Health Care Enhancement Act. This aid was not included in our data because hospitals recorded revenue from the relief fund as “other non-operating income.” 31 The revenues examined here represented those received from the delivery of health care services directly to patients.
The variables used as controls were percentage changes in the number of beds, employees, discharges, acute days, and Case Mix Index (CMI) from 2019 to 2020; and general hospital status in 2020. The CMI was obtained by averaging the Medicare Severity Diagnosis–Related Groups (MS-DRGs) weight for all of a hospital's Medicare volume and is indicative of the relative severity of a patient population. Control variables were also retrieved from specific Medicare Cost Report Worksheets compiled by AHD and are detailed in Supplementary File 2.
Analysis
We used linear regression models to examine the relationship between telehealth/RPM adoption before the COVID-19 emergency declaration and revenue changes during the initial phase of the COVID-19 pandemic. Our dependent variables were percentage changes in the four categories of revenue between 2019 and 2020, and telehealth/RPM adoption (in 2019) served as the primary independent variables of interest. To control for revenue changes caused by hospital-specific characteristics, we included a dummy variable for general hospital status (vs. specialty) and changes in the number of beds, discharges, employees, acute days, and CMI from 2019 to 2020.
The resulting models can be considered first-difference regressions where changes in revenue are modeled as responding to changes in hospital characteristics. This technique eliminates bias from time-invariant unobserved factors (such as hospital management skill or ownership status) and from persistent reporting errors. 32 For each dependent variable, we also ran separate regressions for hospitals in rural vs. urban locations to determine whether rural status influenced the relationship between telehealth / RPM adoption (prior to COVID-19) and revenue changes during the COVID-19 pandemic. Important rural-urban differences exist in other telemedicine research.29,30,33,34 Our identification relied on the assumption that changes in hospital revenues not caused by telehealth / RPM adoption were captured by the control variables in our model.
Data limitations
We were limited by the self-reported nature of the AHA IT Supplement survey data, which may introduce some bias. Since self-selection may occur, we followed Parasrampuria and Henry's (2019) suggestion to generalize our results. 35 We used a logistic regression model to predict the likelihood of AHA IT Supplement response as a function of hospital characteristics including size, ownership, type of facility, case mix index, and urban status. Hospital-level weights were derived by the inverse of the predicted likelihood and used in the first-differenced regressions. Supplementary File 3 provides detailed information on the logistic regression model.
Results
We hypothesized that early implementation of telehealth and RPM before the COVID-19 pandemic would allow for quicker response to hospital shutdowns and present revenue-generating opportunities early during the pandemic. Figure 1 provides some preliminary evidence of this: scatterplots of gross revenue changes vs. discharge changes show stronger correlation for hospitals without telehealth (left; r = .49) compared to those with (right; r = .41). Thus, telehealth likely provided more revenue opportunities for hospitals experiencing declines in discharges.
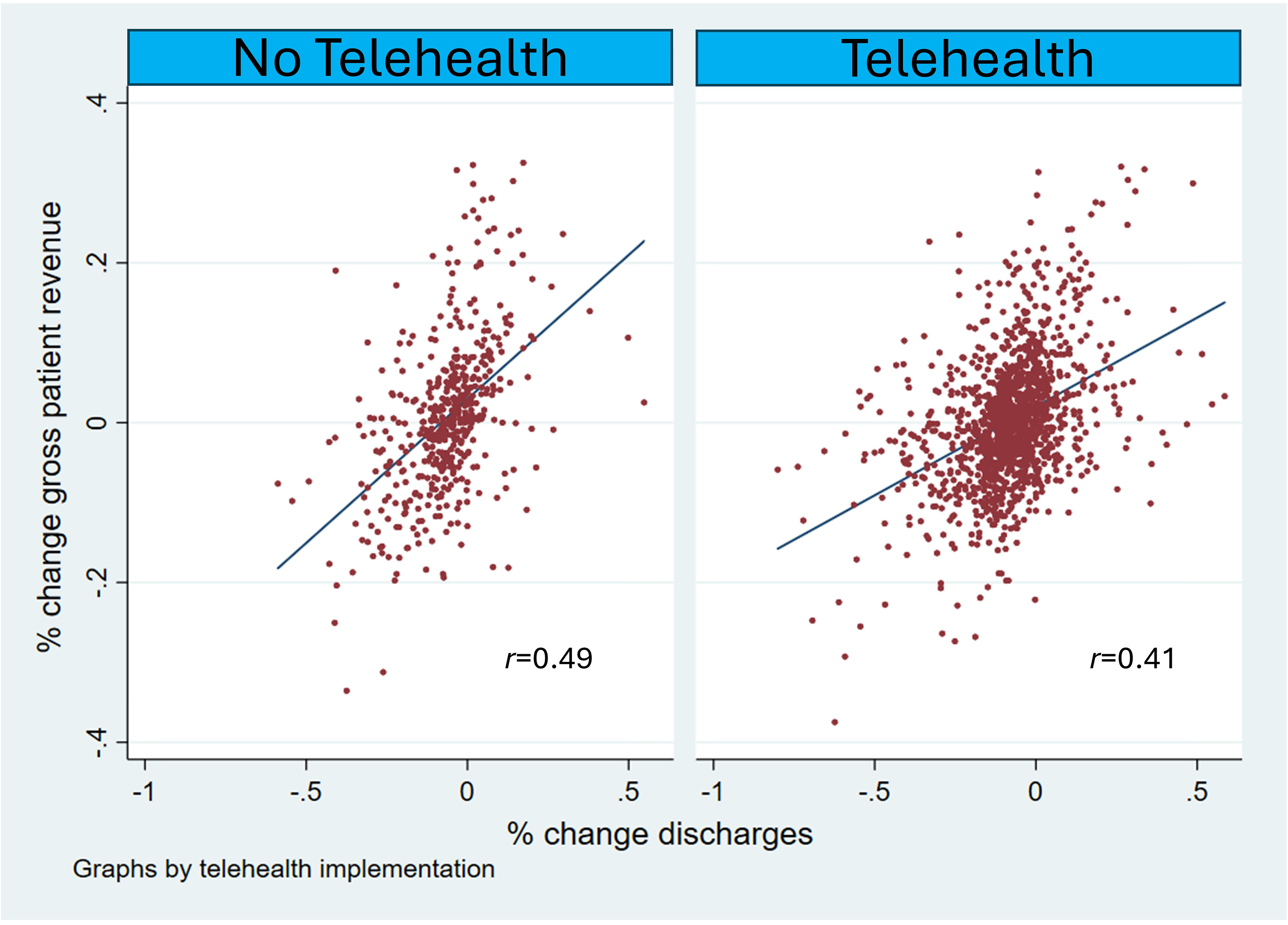
Scatterplots of gross revenue changes (2019–2020) versus discharge changes (2019–2020).
The first panel in Table 1 displays summary statistics on telehealth and RPM adoption for the overall sample and across rural/urban status. Rates of telehealth adoption are similar (around 75%) for hospitals in both geographies as of 2019, but RPM adoption is markedly lower than telehealth adoption as of 2019 (52% in aggregate); this difference is statistically significant at the p < .001 level. The second panel in Table 1 shows the proportion of hospitals with revenue decreases between 2019 and 2020. Roughly half of the hospitals in our dataset report revenue declines over this period; however, a significantly higher proportion of rural hospitals saw losses. Notably, over sixty percent of rural hospitals saw losses in inpatient and net patient (which accounts for bad debts and other adjustments) revenue during this period. Table 1 also demonstrates that rates of telehealth and RPM adoption were not significantly different between rural and urban hospitals in 2019 at the
Summary statistics by rural/urban status – telehealth/remote patient monitoring adoption and revenue data.
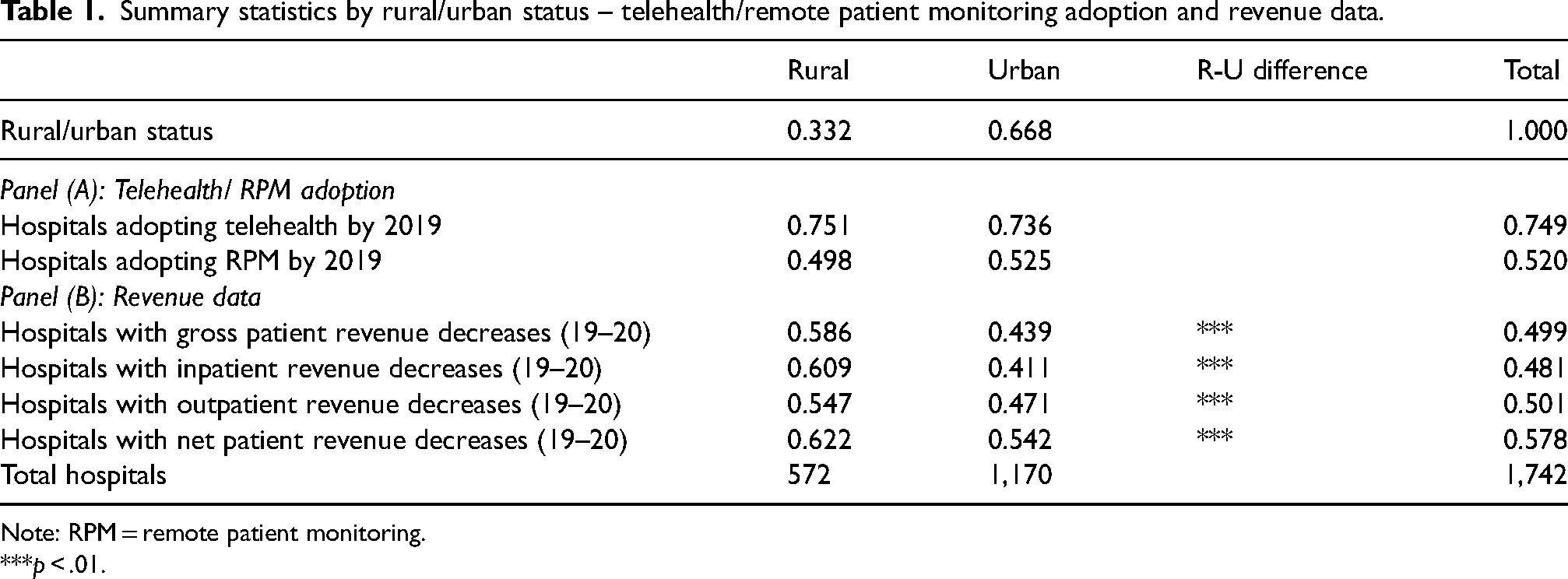
Note: RPM = remote patient monitoring.
***p < .01.
Table 2 shows summary statistics for hospital characteristics. As expected, CMI, the number of beds, employees, discharges, and acute days are significantly larger for urban hospitals. Table 2 also demonstrates that a greater proportion of rural hospitals (97%) are general facilities when compared to their urban counterparts (75%). This is expected given that most specialty hospitals are located in more urban locations. 36 Rural hospitals experienced significantly larger declines in the number of beds, employees, discharges, and acute days during the initial phase of the pandemic. For instance, acute day losses and total employee decreases were twice as large for rural hospitals as for urban hospitals (−8% vs. −4%, and −2% vs. −1%, respectively).
Summary statistics by rural/urban status – hospital characteristics.
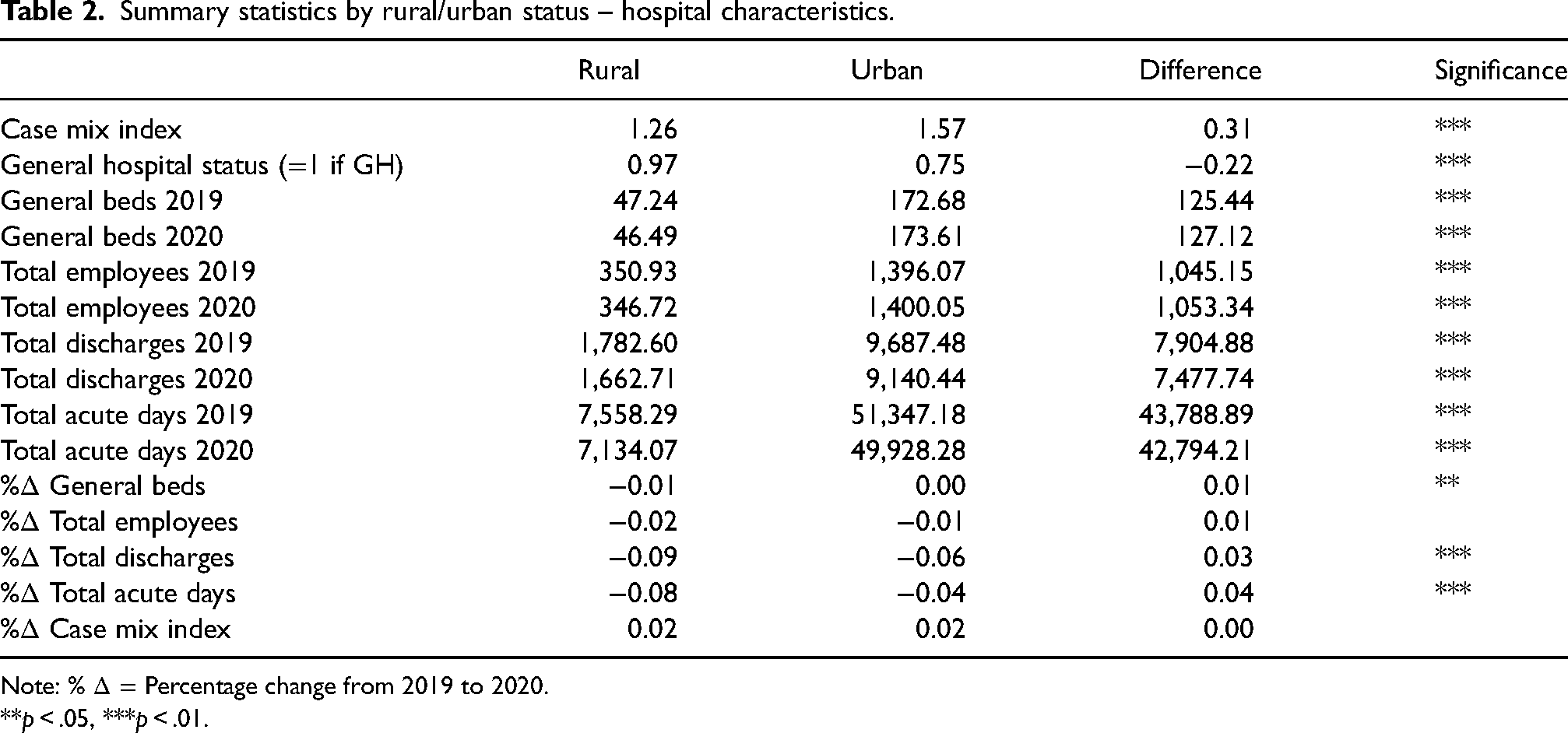
Note: %
**p < .05, ***p < .01.
Supplementary File 4 discusses tests for the primary assumptions of multivariate regression (heteroskedasticity, normality of residuals, linearity, and multicollinearity). It also provides evidence that endogeneity is not problematic for inpatient, gross patient, and net revenue, but may be for outpatient revenue. The models generally appear to be well-specified.
Table 3 displays results for percent changes in gross and net patient revenue, while Table 4 looks at percent changes for inpatient and outpatient revenue. Across all models, we found that increases in the number of employees and discharges were associated with increases in all revenue categories, as expected. Increases in CMI were associated with increases in gross patient and inpatient revenue, but not outpatient. A higher CMI indicates that a hospital treats more complex patients, and procedures that are more complex typically generate more revenue. 37 Increases in the number of acute days were associated with significant increases in gross, net, and inpatient revenue increases, but were not associated with significant changes in outpatient revenue. This is a reasonable finding since changes in patient length of stay should affect inpatient – but not outpatient – revenues. We also found that general hospital status was associated with decreases in gross, net, and inpatient revenue, but slight increases in outpatient revenue. This is again intuitive given that specialty hospitals may select the most profitable patients and because of the increase in ambulatory surgery centers (which focus on outpatient procedures) for general hospitals. 38 These results suggest that the models behaved according to economic theory, with all control variables having the expected signs.
Multivariate analysis of gross patient/net patient revenue changes during the COVID-19 pandemic (from 2019 to 2020) and telehealth/remote patient monitoring adoption before the COVID-19 pandemic (in 2019).
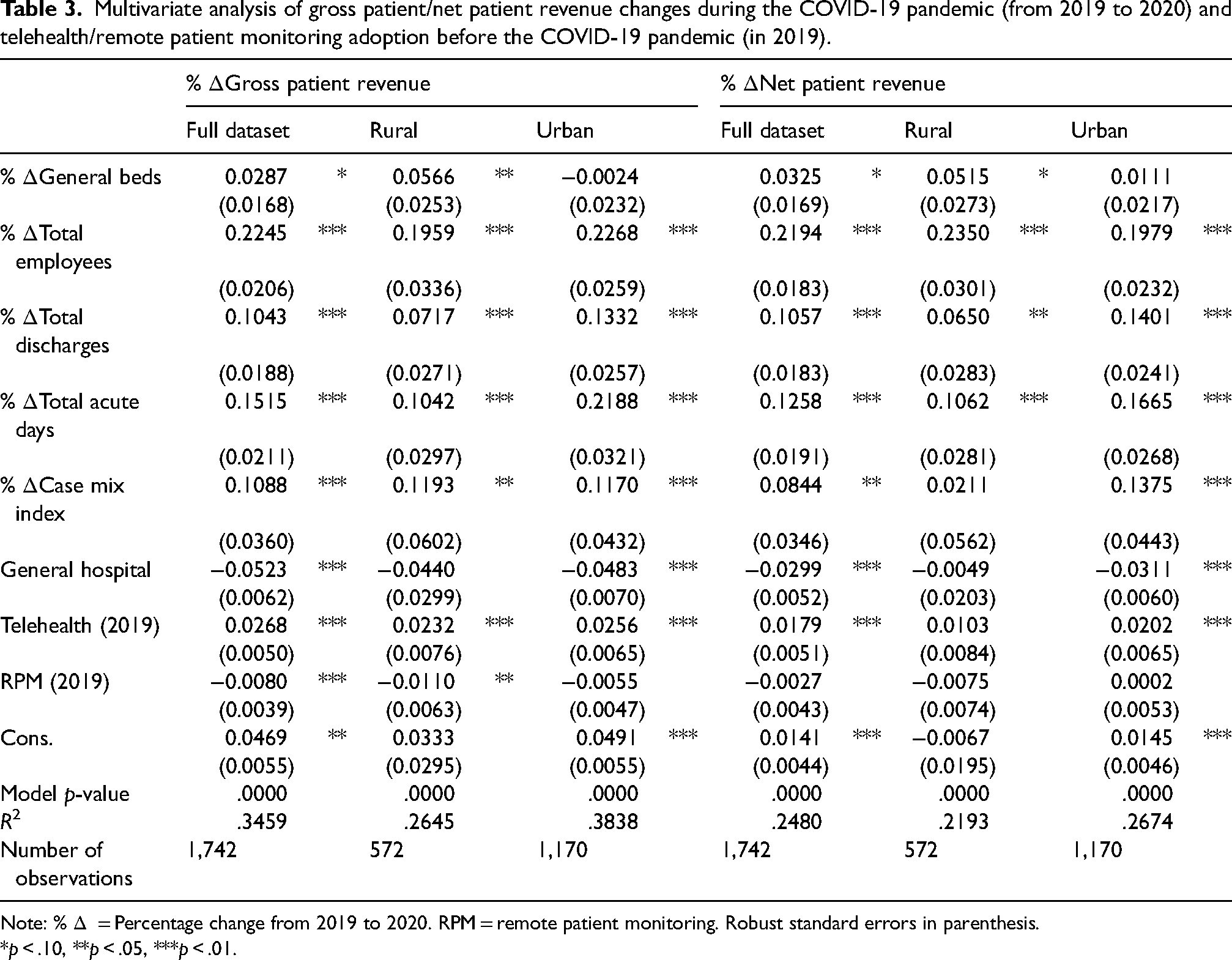
Note: %
*p < .10, **p < .05, ***p < .01.
Multivariate analysis of inpatient/outpatient revenue changes during the COVID-19 pandemic (from 2019 to 2020) and telehealth/remote patient monitoring adoption before the COVID-19 pandemic (in 2019).
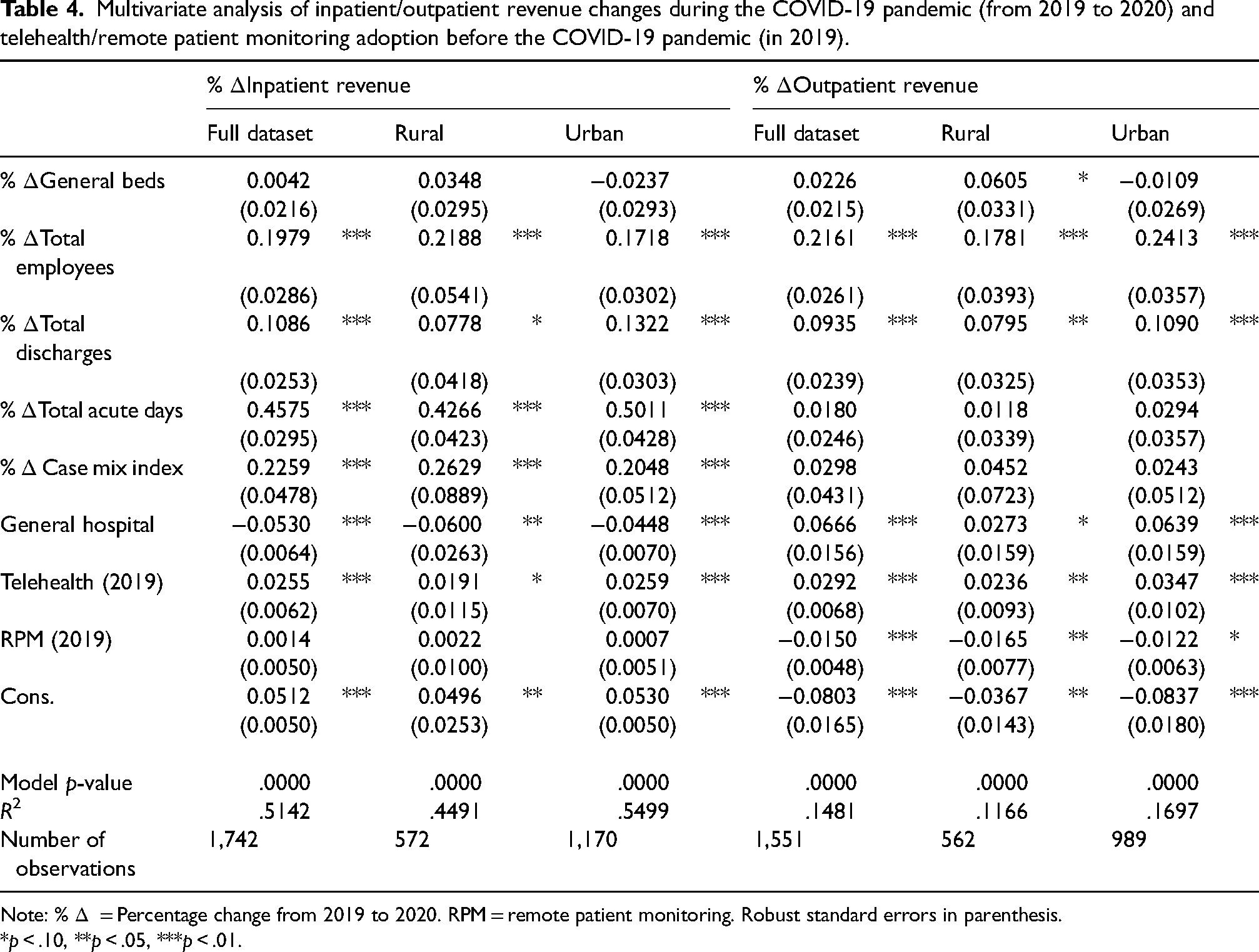
Note: %
*p < .10, **p < .05, ***p < .01.
Moving to the variables of interest, telehealth adoption prior to the COVID-19 emergency declaration was associated with significant increases in all four types of revenue for our full dataset. The associated coefficients imply that, on average, hospitals with prior telehealth functionality in their EHR observed increases in revenue ranging from 1.79% (net patient revenue) to 2.92% (outpatient revenue) between 2019 to 2020. However, contrary to our expectations, RPM implementation was significantly associated with decreases in gross patient and outpatient revenue from 2019 to 2020. The coefficients imply that hospitals with RPM in place by 2019 saw a 0.08% decrease in gross patient revenue and a 1.50% decrease in outpatient revenue between 2019 and 2020. RPM implementation was not associated with significant changes in inpatient or net patient revenue.
Results across rural/urban locations
Tables 3 and 4 also show that early telehealth adoption was associated with significant increases in gross and outpatient revenue from 2019 to 2020 for both rural and urban hospitals, as hypothesized. However, for inpatient and net patient revenue changes, telehealth implementation was only associated with significant changes for urban (and not rural) hospitals. A test of differences between the estimated coefficients for rural and urban hospitals returns no evidence that any telehealth coefficients were different across geographies (Supplementary File 5). This implies that the lack of significance of the estimated telehealth coefficients for rural hospitals was likely due to imprecise estimation (i.e., larger variance) associated with the smaller rural hospital sample size.
We further found that RPM implementation prior to the COVID-19 pandemic was associated with decreases in gross and outpatient revenue from 2019 to 2020 across both rural and urban hospitals. However, the negative relationships were only significant for rural hospitals. This is a striking finding suggesting that early RPM capability led to revenue losses in rural facilities, perhaps due to an inability to monetize RPM follow-up visits and not capturing the in-person visits that would have likely occurred without RPM. Supplementary File 5 again demonstrates that the estimated coefficients for RPM implementation are not significantly different for rural and urban hospitals, although the statistical significance is stronger in rural locations. These opposing findings for telehealth and RPM are intriguing and worthy of additional research.
Discussion
The results suggest that telehealth adoption prior to the onset of COVID-19 was associated with significant increases in inpatient, outpatient, gross and net patient revenue during the initial phase of the pandemic. The largest association is found with outpatient revenue (2.92%, p < .01); however, endogeneity concerns suggest that this may not depict a causal relationship. The finding that inpatient revenue was positively associated with prior telehealth adoption is somewhat surprising, since the COVID-19 expansion of telehealth was largely focused on outpatient services. However, other studies have argued that elements like “virtual rounding” or remote supervision make telehealth useful in inpatient settings. 39 Contrary to our expectations, RPM implementation prior to the COVID-19 emergency declaration was associated with gross patient and outpatient revenue decreases from 2019 to 2020.
The results largely hold across rural and urban hospitals. However, the lack of association between telehealth and inpatient revenue in rural facilities gives credence to the idea that only more urban hospitals were poised to implement telehealth opportunities in inpatient settings7,39 Alternatively, we find that RPM adoption was associated with significant decreases in outpatient and gross patient revenue from 2019 to 2020, and that this was driven by rural facilities. These losses are important and suggest that hospitals did not quickly find a way to monetize the RPM interactions that took place immediately after the COVID-19 pandemic began. One recent report documented that roughly one-fourth of all states still do not have Medicaid reimbursement for RPM. 40 This likely contributed to the reduction in revenue for hospitals with RPM capability during the pandemic.
Our findings are relevant for policy discussion as telehealth usage continues to grow and evolve. Strong continued uptake, changing consumer and provider perceptions, and changes in the regulatory environment during the COVID-19 pandemic have contributed to telehealth use rates never seen before. 20 However, although the COVID-19 pandemic demonstrated the relevance and the potential of telehealth, there is still some uncertainty regarding the long-term financial benefits of telehealth adoption. Our study adds to the literature on the links between telehealth and hospital financial outcomes, and supports the claims of telehealth advocates that telehealth can be a tool for hospitals and practices aiming to improve their finances.23,24,41–43 Alternatively, our results suggest that RPM adoption was associated with revenue losses. This result was driven by rural hospitals, where RPM has been hypothesized as an important contributor to overcoming distance challenges. 44 The results here suggest that pushing for private and public insurance to reimburse for RPM interactions is an important policy consideration for hospital proponents – particularly those advocating for rural facilities such as the National Rural Health Association.
As an empirical study, our analysis has important limitations. First, we defined telehealth and RPM adoption as whether these features were available in the facility's EHR. We had limited insight into more precise metrics of telehealth abilities or usage. In particular, interactions that took place on third-party applications such as Zoom would not require EHR interoperability. Data on specific telehealth and RPM functionality and usage could better inform its effects on hospital revenue. Further, the analysis looked only at one-year changes and additional work is needed to assess whether these relationships have continued in a post-COVID environment. Although the first-difference approach cannot make a strictly causal argument, reverse causality is less of a concern given the results of our endogeneity tests.
Conclusions
This study offers national-level evidence that prior hospital adoption of telehealth and RPM capability were associated with revenue changes during the early phase of the COVID-19 pandemic. Our results support the hypothesis that telehealth adoption by 2019 allowed hospitals to respond in a timelier manner to the health emergency and potentially suffer less severe revenue losses during the initial months of the pandemic. However, contrary to our expectations, remote patient monitoring adoption was associated with meaningful revenue decreases. These distinct differences suggest that additional research should delve into specific telehealth modalities (real-time, store-and-forward, RPM, mobile health) and whether these trends persist in the post-pandemic period.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X241298989 - Supplemental material for Early adoption of telehealth/remote patient monitoring and hospital revenue changes during COVID-19
Supplemental material, sj-docx-1-jtt-10.1177_1357633X241298989 for Early adoption of telehealth/remote patient monitoring and hospital revenue changes during COVID-19 by Claudia A Rhoades, Brian E Whitacre and Alison F Davis in Journal of Telemedicine and Telecare
Supplemental Material
sj-docx-2-jtt-10.1177_1357633X241298989 - Supplemental material for Early adoption of telehealth/remote patient monitoring and hospital revenue changes during COVID-19
Supplemental material, sj-docx-2-jtt-10.1177_1357633X241298989 for Early adoption of telehealth/remote patient monitoring and hospital revenue changes during COVID-19 by Claudia A Rhoades, Brian E Whitacre and Alison F Davis in Journal of Telemedicine and Telecare
Supplemental Material
sj-docx-3-jtt-10.1177_1357633X241298989 - Supplemental material for Early adoption of telehealth/remote patient monitoring and hospital revenue changes during COVID-19
Supplemental material, sj-docx-3-jtt-10.1177_1357633X241298989 for Early adoption of telehealth/remote patient monitoring and hospital revenue changes during COVID-19 by Claudia A Rhoades, Brian E Whitacre and Alison F Davis in Journal of Telemedicine and Telecare
Supplemental Material
sj-docx-4-jtt-10.1177_1357633X241298989 - Supplemental material for Early adoption of telehealth/remote patient monitoring and hospital revenue changes during COVID-19
Supplemental material, sj-docx-4-jtt-10.1177_1357633X241298989 for Early adoption of telehealth/remote patient monitoring and hospital revenue changes during COVID-19 by Claudia A Rhoades, Brian E Whitacre and Alison F Davis in Journal of Telemedicine and Telecare
Supplemental Material
sj-docx-5-jtt-10.1177_1357633X241298989 - Supplemental material for Early adoption of telehealth/remote patient monitoring and hospital revenue changes during COVID-19
Supplemental material, sj-docx-5-jtt-10.1177_1357633X241298989 for Early adoption of telehealth/remote patient monitoring and hospital revenue changes during COVID-19 by Claudia A Rhoades, Brian E Whitacre and Alison F Davis in Journal of Telemedicine and Telecare
Footnotes
Acknowledgements
The information, conclusions, and opinions expressed in this article are those of the authors and no endorsement by FORHP, HRSA, HHS, Oklahoma State University or University of Kentucky is intended or should be inferred.
Availability of data and materials
The data underlying this study are not publicly available. Restrictions apply to the availability of these data which were used under license for the current study from the American Hospital Association (AHA) and the American Hospital Directory (AHD). Data are, however, available from the authors upon reasonable request and with permission of the American Hospital Association (AHA) and the American Hospital Directory (AHD). No administrative permissions were required to access the data used in this study.
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
Our research did not require Institutional Review Board (IRB) approval as it did not involve human participants. The data used in this study was not anonymized before its use as the data did not involve human participants, only financial and health IT hospital-level data.
Ethical approval
This study uses only secondary data and does not require Institutional Review Board approval.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Federal Office of Rural Health Policy (FORHP), Health Resources and Services Administration (HRSA), U.S. Department of Health and Human Services (HHS) under cooperative agreement # U1ZRH33331-02-01.
Data availability statement
Our final dataset includes proprietary data from the American Hospital Directory (AHD) and cannot be made publicly available. We will make our code available upon publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.