
Abstract
Past research has examined available literature on electronic mental health interventions for Indigenous youth with mental health concerns. However, as there have recently been increases in both the number of studies examining electronic mental health interventions and the need for such interventions (i.e. during periods of pandemic isolation), the present systematic review aims to provide an updated summary of the available peer-reviewed and grey literature on electronic mental health interventions applicable to Indigenous youth. The purpose of this review is to better understand the processes used for electronic mental health intervention development. Among the 48 studies discussed, smoking cessation and suicide were the most commonly targeted mental health concerns in interventions. Text message and smartphone application (app) interventions were the most frequently used delivery methods. Qualitative, quantitative, and/or mixed outcomes were presented in several studies, while other studies outlined intervention development processes or study protocols, indicating high activity in future electronic mental health intervention research. Among the findings, common facilitators included the use of community-based participatory research approaches, representation of culture, and various methods of motivating participant engagement. Meanwhile, common barriers included the lack of necessary resources and limits on the amount of support that online interventions can provide. Considerations regarding the standards and criteria for the development of future electronic mental health interventions for Indigenous youth are offered and future research directions are discussed.
Keywords
Introduction
Indigenous youth are exposed to many elements that increase their risk for negative mental health outcomes. Colonial legacies (e.g. assimilation, gendered violence, dispossession of land and resources) 1 have historically and continually shaped the lives of Indigenous youth. More broadly, colonialism (i.e. the guiding force that created political and economic inequalities) has been discussed as a social determinant of health that has led to various unjust life situations. 2 For example, Indigenous populations are more likely to experience decreased housing quality, 3 unstable housing, 4 and food security, 5 as well as increased household crowding, 6 poverty, 7 substance use, 8 and sexual violence 9 than non-Indigenous populations. Indigenous youth, specifically, are overrepresented in child protection and youth justice systems and are more likely to experience neglect and abuse, as well as poor outcomes in areas of health, education, and social development, when compared to non-Indigenous youth. 10 As such, Indigenous youth have been noted as constituting a ‘high-risk group’ for emotional and psychological difficulties. 10 With the accumulation and intersection of many of these risk factors, 11 there is a clear need for interventions that specifically support the mental health of Indigenous youth.
Indigenous youth have experienced barriers to mental health care for decades. Barriers to accessing mental health services for Indigenous young people included inconsistent access to mental health services,12,13 lack of awareness of services, 11 and discomfort in seeking help from services due to concerns about confidentiality, shame, fear, language or literacy difficulties, and racism 14 (for a review, see Brown et al. 15 ). Retaining mental health service providers within rural or remote communities is also difficult, 12 and this low retention of staff can then lead to higher caseloads for the remaining staff. 16 As Indigenous communities can be geographically isolated, there are limited options for supervision and training for service providers, which can result in novice practitioners feeling pressured to practice far beyond their capabilities. 17 During the COVID-19 pandemic, populations who are the most vulnerable (i.e. Indigenous youth) were left behind when it came to accessing the rapidly developing, innovative, wellness and self-care virtual services that were being designed to meet the needs of the general population. 18 Conventional mental health supports (i.e. face-to-face care) were also no longer able to meet the increased volume of need for support,19,20 and in many circumstances, in-person support was no longer an option.19,20 Thus, adaptation and transformation of mental health care options were greatly needed, 18 especially for Indigenous youth who had long been facing such barriers to care.
Electronic mental health (e-MH) interventions have been suggested as a method to circumvent health care disparities, including service costs, accessibility, and stigma-related barriers. 21 e-MH refers to mental health services and information that are either delivered or enhanced through the Internet and/or other similar types of technology. 22 A recent meta-analysis found telehealth interventions (including modalities such as video-conferencing and mobile health apps, etc.) to be equally or more clinically effective when compared to usual care. 23 As well, telehealth did not compromise the effectiveness of care when compared to conventional forms of health service delivery. 23 Culturally appropriate care can also be easily integrated into e-MH interventions, 24 making them particularly relevant for use by Indigenous youth who strongly benefit from the inclusion of culture in care. 25 Telehealth has also been found to enhance culturally appropriate care by allowing for care to be provided within supportive environments, such as Indigenous-run primary healthcare programs, instead of within mainstream healthcare programs, and by reducing burdens associated with traveling and dislocating from community and family. 26 As well, literature suggests that young people may be more likely to respond to, and prefer, alternative service delivery strategies offered via e-MH interventions (e.g. video conferencing; and Internet-based applications). 27 In addition to being an option for reducing geographical barriers to care, e-MH interventions may have additional utility as they might help Indigenous youth feel more comfortable and/or motivated to engage in technology-based services.
Some reports have examined the use of e-MH interventions to support the well-being of Indigenous youth during the peak of the COVID-19 pandemic. For example, Walker et al. 28 examined articles identifying existing and expected mental health outcomes associated with COVID-19 for Indigenous young people and found that, while digital technologies can help build strong cultural identity, enhance connections to community, and improve mental, social, and emotional well-being outcomes, there are still great inequities in accessibility to digital technology for Indigenous young people. The authors advocated for more targeted policy and funding to promote Indigenous young people's access to digital well-being services. 28 Relatedly, a review of Strudwick et al. 29 digital interventions to support the mental health of individuals living in Canada during the COVID-19 pandemic briefly highlighted the lack of digital resources available that are specific to Indigenous peoples and communities. 29 These reviews demonstrate the potential of e-MH interventions for Indigenous youth, but also demonstrate some key barriers in terms of intervention accessibility.
Several reviews have been conducted to examine the impact of e-MH interventions for Indigenous populations more broadly,30–35 but there is still a need for more literature pertaining to e-MH services for Indigenous youth specifically, 36 specifically around the facilitators and barriers to e-MH intervention implementation. Recent efforts to summarize the available e-MH services for Indigenous youth thus far have offered preliminary findings but noted that further research is needed to confirm those findings. 37 Povey et al. 38 currently examining more specific aspects of e-MH interventions for Indigenous youth (i.e. best practices for engaging youth in the development and evaluation of e-MH resources), however, an updated review of the broader considerations pertinent to e-MH interventions for Indigenous youth was still needed as (a) the literature on these interventions has increased and (b) the need for these interventions options have also increased throughout the COVID-19 pandemic. As well, as the First Nations Mental Wellness Continuum Framework (FNMWCF) 39 and the Integrated Life Course and Social Determinants Model of Aboriginal Health (ILCSDAH) 40 both highlight the importance of interventions that extend beyond the individual and into the family and community interventions to improve health outcomes, this review will also aim to include e-MH interventions that work to improve outcomes for Indigenous youth via the inclusion of family and community members.
Study purpose
This study aimed to provide an updated systematic review of the literature describing the implementation of e-MH interventions designed for/with Indigenous youth. We sought to capture any new and relevant studies that had been put forth since the previous study 37 and to summarize relevant characteristics, facilitators (i.e. factors that increase intervention development, implementation, and accessibility), and barriers (i.e. factors that decrease intervention development, implementation, and accessibility) of e-MH interventions that were reported. Throughout the Introduction above, various terms related to e-MH interventions (i.e. telehealth and digital technologies) have been/are used interchangeably. Throughout the rest of this article, we try when possible to be consistent with the term “e-MH intervention,” however, we also use language reflected within individual papers (i.e. “mobile interventions” and “web-based programs”). In doing so, we are aiming to provide the best summary possible of available e-MH interventions, regardless of cross-study differences in terminology.
The present study is also process-based rather than outcome-based. More specifically, this systematic review was not conducted to thoroughly review aspects of outcome measures (e.g. efficacy for various outcomes). Instead, only basic counts and descriptions of outcomes are reported, and processes used to develop e-MH interventions for Indigenous youth were the focus, as this type of information would be valuable for future researchers, stakeholders, and/or communities looking to develop or adapt e-MH interventions for their own contexts. With this goal in mind, considerations for standards and criteria that can be used to inform new development e-MH interventions for Indigenous youth were provided based on how often various processes occurred in the literature reviewed and how well they addressed known barriers to intervention.
Method
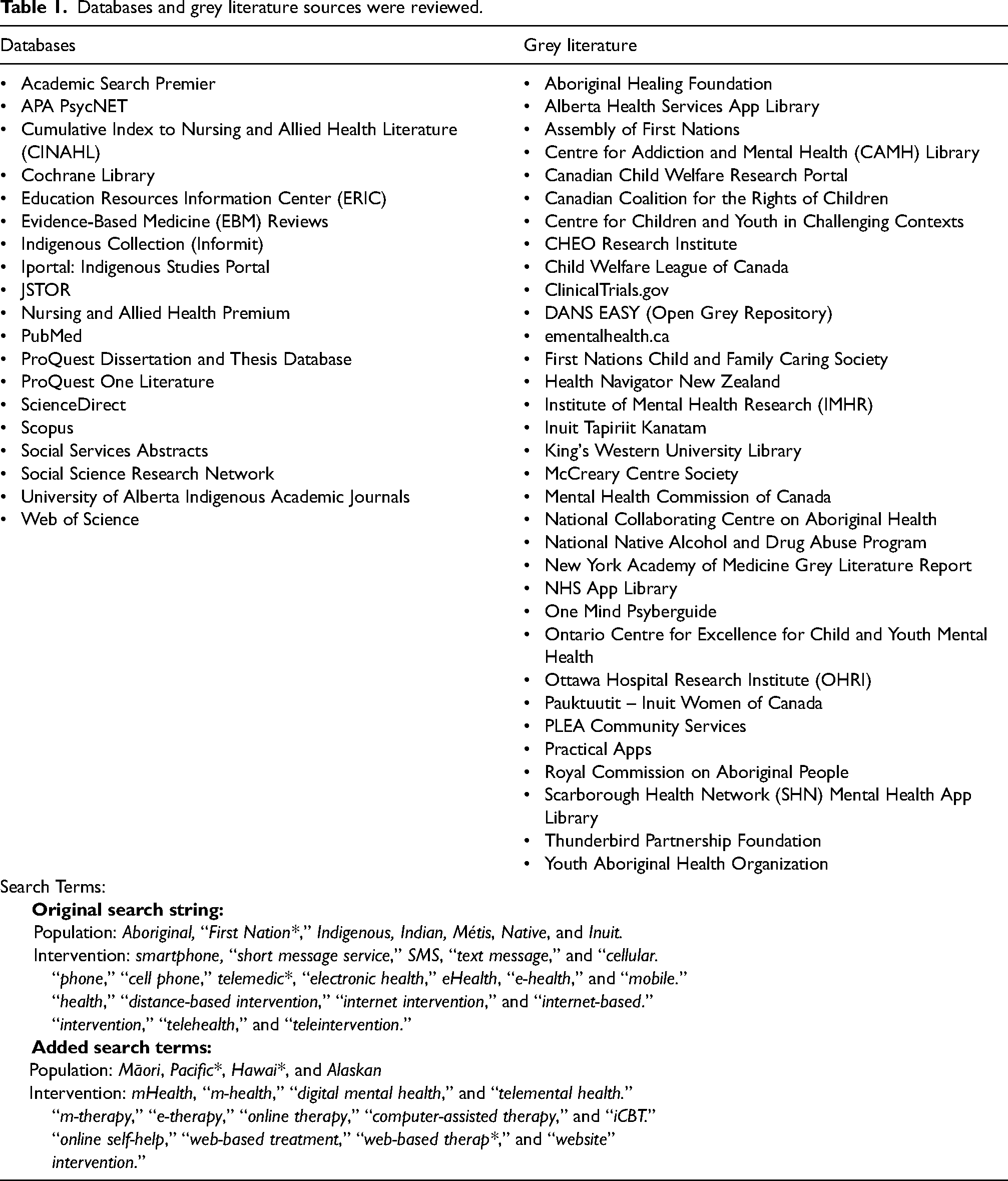
A preliminary review of literature from 19 databases was completed by one reviewer. This review included grey literature and relevant reference lists. Building upon our original search string, 37 we conducted this preliminary review of the literature to identify any new terminology that would support our search aims. Our original search string included 24 terms but was expanded to include additional terms from Povey et al. 38 recently published systematic review protocol, which will examine the various methods used to involve Indigenous youth in the development and evaluation processes of e-MH interventions. 38 These original and additional search terms can be found at the bottom of Table 1. Following this preliminary review, a systematic review of these databases was completed by one author from 29 April 2021 to 25 June 2021, beginning with an initial title and abstract screening, and followed by a full-text review. Table 1 also includes the databases and grey literature sources examined. Figure 1 describes the number of studies included in the final review, in accordance with the most recent Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standards. 41 Tables 2 and 3 include data related to population, intervention, comparisons, and outcomes. Finally, a two-eyed seeing framework was used to interpret the literature, which allowed for standards and criteria to be developed while considering both Indigenous methodologies, ways of knowing, and knowledge, in combination with Western science. 42
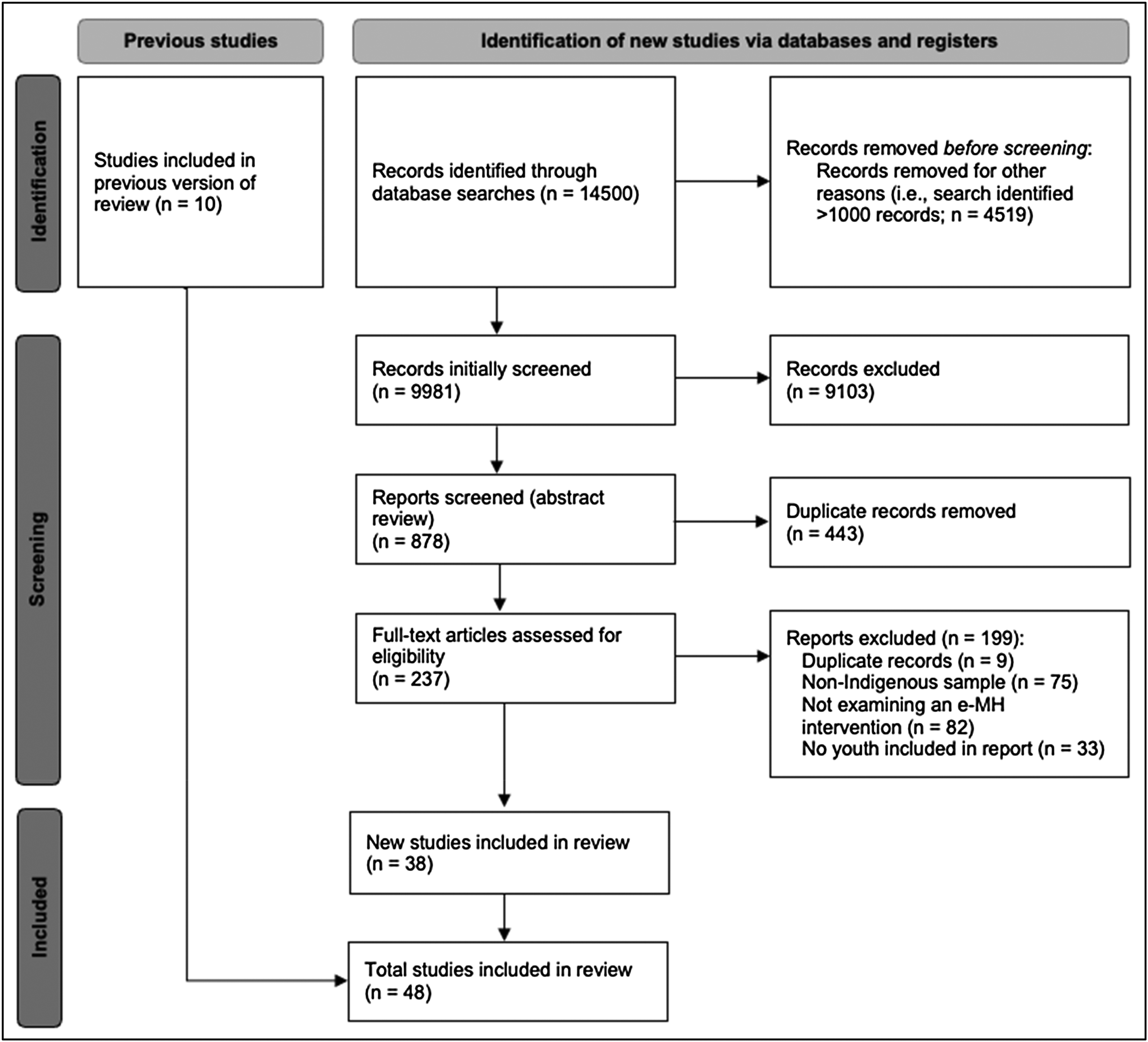
Literature review process via the preferred reporting items for systematic review and meta-analyses (PRISMA) diagram.
Databases and grey literature sources were reviewed.
Summary of retrieved articles – directly relevant for youth.

Summary of retrieved articles—not specific to youth, but youth included in the study.

* Note: In the “Population and study location column,” M indicates age mean and SD indicates age standard deviation.
Inclusion criteria
Articles were included in this review if they described any type of e-MH intervention designed to improve the mental wellbeing of Indigenous youth. Articles were also included in this review even if the participants included in the studies were not Indigenous youth, and this was to ensure that we captured e-MH interventions designed to improve the mental wellbeing of Indigenous youth via their support networks (e.g. family members, community members, healthcare workers, etc.), as seen in the FNMWCF 39 and the ILCSDAH 40 discussed above. Articles also had to be available in English and be published between 1 January 2000 and 1 June 2022. Youth was defined as being between 12 and 30 years of age. While Consolidated Standards of Reporting Trials (CONSORT) best practices indicate that only those sources that meet a particular threshold of quality should be evaluated in a systematic review, this was not completed as several studies would have been removed. This is in alignment with a framework by Short et al. 90 ; all studies were included if they met the inclusion criteria.
Results
Study characteristics
Forty-eight articles were included in this review, 38 of which were updated from the previous review. 37 Figure 2 provides a visual of the increase in studies over the past few years. Table 2 describes 30 studies that aimed to support youth/young adults within the defined age range, while Table 3 describes 18 studies that included participants within the defined age range as well as participants older than the defined age range. Throughout each section in the results, studies from Table 2 will be referred to as “youth-specific studies” and studies from Table 3 will be referred to as “broader studies.”
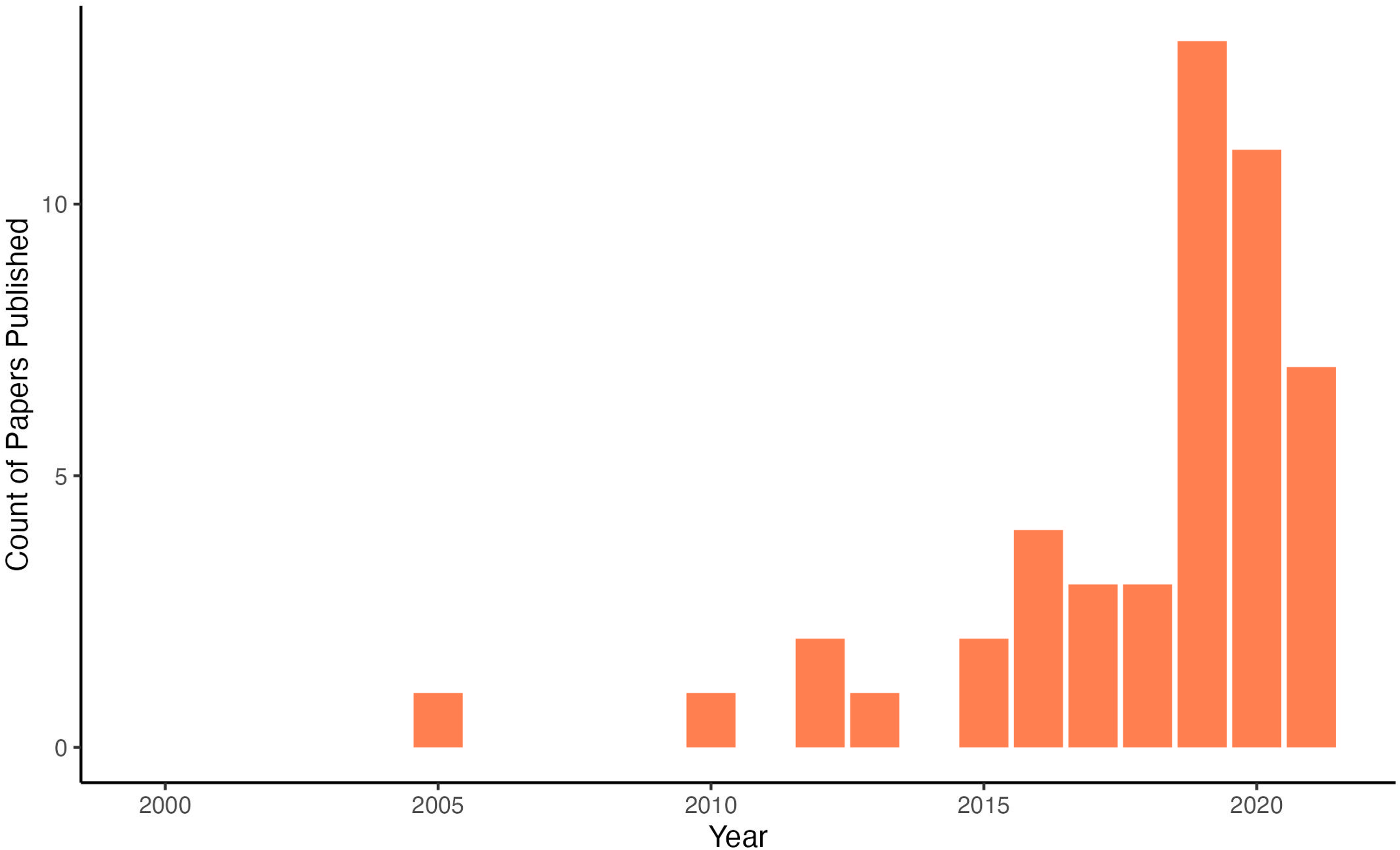
Count of papers published by year.
Mental health concerns targeted
Studies targeted a wide variety of mental health concerns. Several studies targeted more than one mental health outcome so study counts amount to more than the total number of studies initially reported (Figure 3). The mental health concerns examined in these interventions were: alcohol-exposed pregnancies,51,66,78,80 anxiety,60,63,89 coping skills,46,70,84 COVID-19 symptom monitoring, 47 depression,60,63,65,69,89 general health and mental well-being,48,49,55,63,71,77 HIV/STI intervention,53,54,61,72 intimate partner violence,79,87 parenting support, 50 psychological distress,43,53,65,69,89 safe partner relationships, 52 smoking cessation,44,45,59,68,73,75,76,82,83,88 substance abuse/misuse,55,57,62,74,86 and suicide prevention.56,58,64,65,67,69,81,84
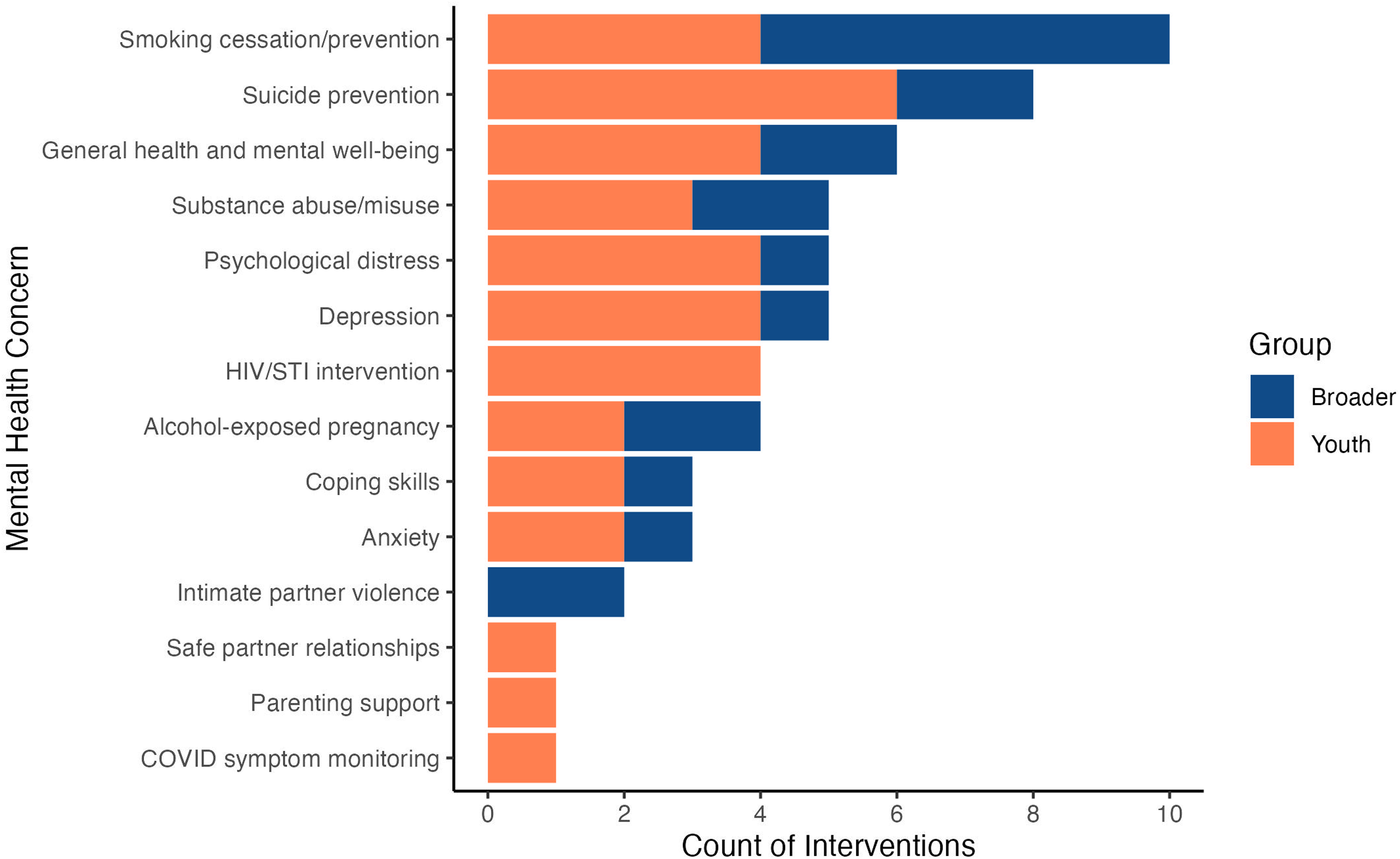
Count of interventions by mental health concerns.
Type of technology used
The type of technology used to deliver each e-MH intervention varied across studies. Several studies relied on more than one type of technology so the breakdowns of these studies in this article total more than the total number of studies reported. Counts of the number of interventions using each type of technology are shown in Figure 4. The types of technology used were: apps,46,48,49,51,52,55,63–65,69,77,83,84,87 networked mobile games, 70 non-specified mobile interventions, 66 non-specified web-based interventions,74,86 online software programs, 60 social media pages,72,88 teleconferencing, 71 text messages,45,47,50,53,54,58,62,67,72,73,75,76,81,82 video-based interventions,61,62 web-based training interventions,43,56,85 web-based zine tools, 68 websites,44,57,59,72,78–80,89 and YouTube channels. 72 Seven interventions used a multi-media-based approach (four in youth-specific studies and three in broader studies), using combinations of the abovementioned delivery modes. Two studies used both text messages and videos,62,67 while others used combinations such as app and text messages, 83 app and website, 49 text messages and telephone counseling, 75 and text messages and websites.60,72 One study paired a FitBit-HR Charge 2 with text messages and web-based programs in their intervention. 60
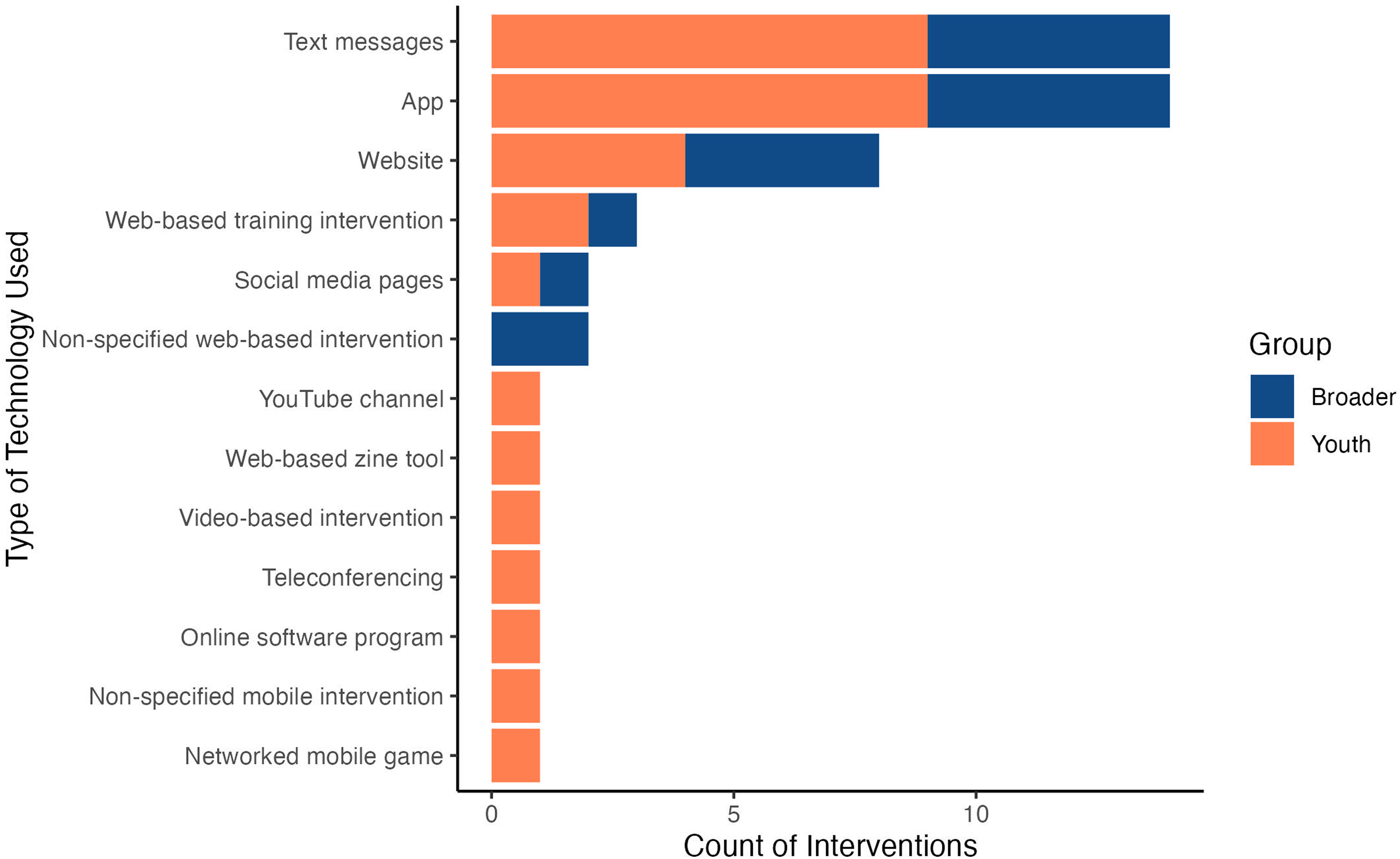
Count of interventions by technology used.
Type of research approaches
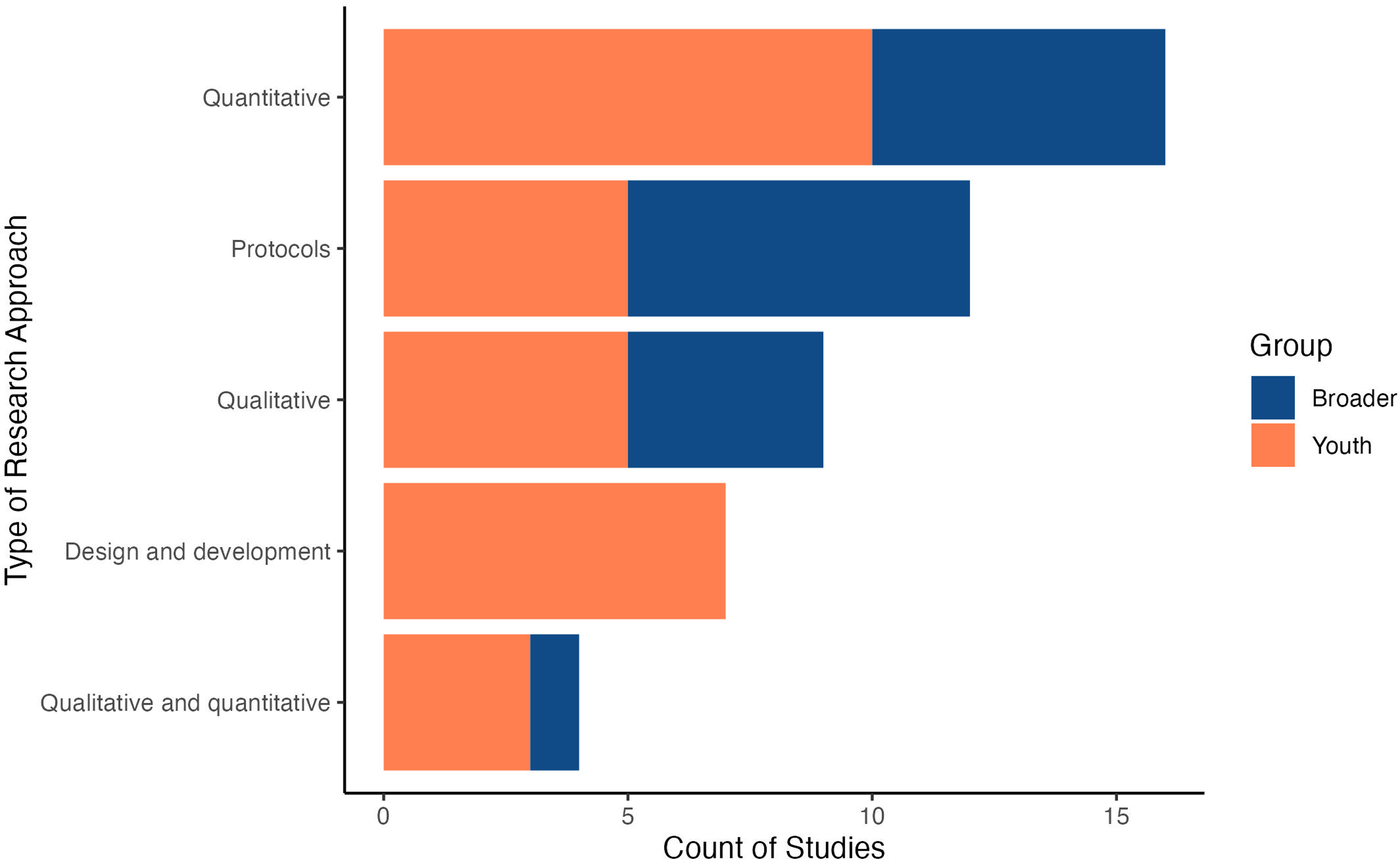
As noted in the “Introduction” section, the aim of this article is not to thoroughly review or evaluate e-MH intervention outcomes (e.g. effectiveness and efficacy). Therefore, only broad categories of research approaches are reported to gain a sense of the type of research occurring within this area. A wide variety of research approaches were used both youth-specific and broader. Figure 5 provides a visual count of studies by reported research approach. Qualitative approaches were reported in five of the 30 total youth-specific studies,50–52,68,71 and in four of the 18 total broader studies,77,78,84,85 and assessed outcomes such as user engagement,50,68 anticipated benefits, 77 and cultural relevance.77,78,84 Quantitative approaches were reported in 10 youth-specific studies43–45,47,48,57,58,65,67,72 and six broader studies49,76,79–81,89 and assessed outcomes such as indicators of psychological distress47,58,65,69 and substance use.44,45,47,57 Some studies reported both qualitative and quantitative approaches (i.e. mixed methods). This occurred in three out of the 30 total youth-specific studies54,56,69 and one of the 18 total broader studies. 83 Other studies reported on the design and development of interventions (rather than reporting qualitative or quantitative approaches) and this occurred for seven out of the 30 total youth-specific studies.38,46,55,59,61,62,70 No broader studies shared the same focus of design and development. The main outcome of these design and development studies was often the developed intervention itself,46,59,61,62,70 in which assessment of intervention effectiveness is currently ongoing. Finally, study protocols were retrieved for five youth-specific studies,53,60,63,64,66 seven broader age-ranged studies,73–75,82,86–88 and described the future assessment of outcomes such as measures of psychological distress53,60,63,64 and substance use.73–75,82,86,88
Count of studies by type of research approach.
Intervention development
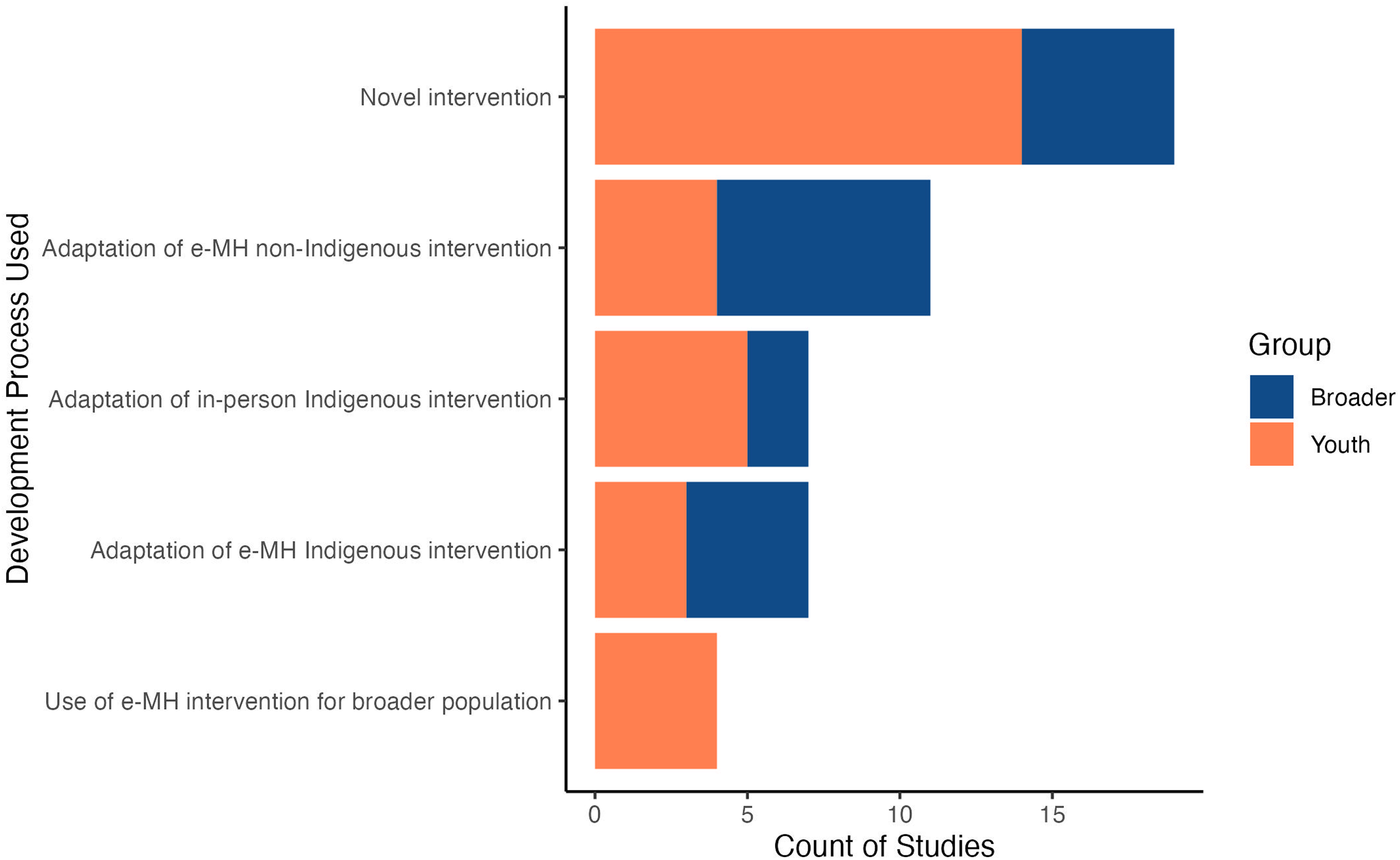
Processes for e-MH intervention development and adaptation also ranged widely. Figure 6 provides a visual count of studies by the development process used. Almost half (n = 14) of the 30 youth-specific studies developed novel e-MH interventions designed specifically for Indigenous youth/young adults,45–48,50,53–56,65,69–72 where as five of the 18 total broader studies developed novel interventions.49,76,86,88,89 In contrast, five of the youth-specific studies51,59,62,66,67 and two broader studies75,77 opted to translate pre-existing in-person interventions developed for Indigenous youth/young adults into e-MH interventions for Indigenous youth/young adults. Four of the youth-specific studies opted to develop e-MH interventions for Indigenous youth/young adults from pre-existing e-MH interventions that had been initially developed for non-Indigenous populations.44,60,61,68 Seven of the broader studies did the same.74,78–81,83,87 Three youth-specific38,58,64 and four of the broader73,82,84,85 studies demonstrated iterative development (i.e. development with several opportunities for feedback from future app users, community members, etc.) by adapting pre-existing e-MH interventions designed specifically for Indigenous youth. One youth-specific study examined a pre-existing e-MH intervention that was not specifically adapted to American Indian/Alaskan Native culture but was designed to aid adults who support youth in multicultural settings. 43 Relatedly, three youth-specific studies described interventions that were co-developed to be inclusive of—but not specifically for—Indigenous youth.52,57,63
Count of studies by development process used.
Reported facilitators to e-MH intervention implementation
Incorporating community-based participatory research approaches
Twenty-eight studies sought participant feedback regarding the design and development of e-MH interventions,38,46,48–53,55,59,61,62,64,65,67,68,70–72,77,78,81–84,86,87,89 through processes such as focus groups,51,59,68,82,87 co-design workshops, 38 and think aloud protocols, in which participants tested interventions while being observed and questioned by the researcher.46,52 As part of the e-MH intervention research approaches, several studies involved many iterative phases that built upon each other in the co-design process.38,46,56,59,61,62,68,72,73,77,82 These processes were used to develop novel interventions46,56,62 and adapt previously existing in-person interventions to e-MH interventions.59,62,77 Iterative processes were also used to consult, review, and revise previously existing e-MH interventions to become more culturally appropriate61,68,72,73,82 or age appropriate 38 for target participants. Some of these studies included software developers 46 and media organizations 62 who supported the development of several drafts of the intervention as well.
Several types of participant groups (e.g. stakeholders and individuals with experience working with AI/AN youth 51 ; expert reference groups such as service providers 77 ; community advisory boards 70 and groups 86 ) were included in the co-design process. Longer lengths of the research projects (e.g. two years, 81 three years, 61 and five years 62 ) were highlighted by researchers to allow for the incorporation of a wide array of perspectives and experiences in the intervention design process. 61 Studies varied in the levels of involvement of participants throughout the study with this process ranging from communities electing to participate in all stages of the study 49 to others who were only involved in some stages. This level of involvement was also dependent on client variables, such as the level of preparedness to provide critical feedback. 46
Several studies also noted the importance of establishing and preserving relationships with partnering communities.50,53,65,67,70–72 Researchers noted that these partnerships were key to project success 50 and provided opportunities to demonstrate relational accountability with participants and with governing leadership to make research relevant to the communities represented. 53 These partnerships enabled engagement through well-established communication channels, 67 multimedia health resources, 72 and local partner organizations. 65
Incorporating culture into intervention presentation, content, and study design
Researchers from one study included in this review noted that the “one size fits all” approach is not as effective as approaches that are more culturally matched to their audiences. 68 Thirty-three studies included in this review described efforts to provide culturally-appropriate interventions for their participants.38,45,46,48–52,55,59,61,62,64,67,68,70,72–82,84–89 Some interventions described the inclusion of cultural representation in language and visual aspects of the intervention. For example, culturally relevant text messages,45,67,72,73,76,81,82 and the inclusion of culturally relevant language more broadly51,62,67,68,70,77,78,84,88 (e.g. through culturally relevant video and auditory components59,68,84) were noted. Cultural representation via visual aesthetic choices was also incorporated,46,77,78,84 with a few studies including Indigenous media experts, (e.g. a Native-owned film crew Sky Bear Media 62 ; Indigenous actors 86 ; Indigenous artists64,86; Indigenous graphic designers 64 ) to support participant engagement.
On a more conceptual level, several studies noted the importance of incorporating cultural values48–50,59,67,70,77 and cultural norms67,80 into interventions. Participants in one study requested that intervention videos not include “romanticized Native imagery,” and instead situations that are relatable to them (e.g. familiar scene locations, and characters that American Indian youth would typically turn to for help 61 ). Authors also concluded that the inclusion of Indigenous frameworks in interventions (e.g. Kaupapa Māori model of interaction 52 ; Two-Eyed Seeing Framework 55 ; and Cultural Variance Framework 88 ) were associated with improved user engagement, as was the inclusion of narratives/storytelling86,88 and holistic approaches that examined social determinants of Indigenous health.54,55,67,88
Beyond intervention content, studies also included culturally tailored aspects in their research design. For example, some studies incorporated culturally tailored assessments (e.g. quizzes, 59 survey items, 76 and overall study measures 87 ), while others included a comparison arm in the design that was culturally tailored, 59 or used culturally relevant frameworks while conducting study analyses. 45 Another study noted cultural considerations in terms of compensation for participants and highlighted their efforts to indigenize the process of accessing federal grant funds for their project (e.g. ensuring that incentive relevance was not questioned at the institutional level; ensuring incentives were received before participation). 55
Enhancing participant engagement
Studies outlined several targeted recruitment methods to support engagement (e.g. via Māori radio station advertising 45 ; via e-Newsletters, listservs, conferences, print postcards, tribal epidemiological centers, websites, Native social media influencers, and Native student centers at schools and universities 67 ). The use of interfaces that youth were familiar with, such as social media platforms (e.g. Instagram, Snapchat, or TikTok)38,46,67,88 and/or web-based-platforms previously used for online classes 59 was also reported to facilitate youth engagement.
Methods of incentivization
Several types of incentivization strategies (e.g. access to a mobile phone and cellular plan 53 ; access to additional computer time 44 ; and gift cards or monetary reimbursements67,72,86) were used to support engagement. Access to requested therapy (e.g. nicotine replacement therapies) and facilitator support were also offered. 59 With respect to randomized control trial designs, making the intervention be made available to all clients interested in the service, rather than just to those who were randomly allocated to the intervention arm was suggested as well. 83 For example, one study found the use of a pre-randomized controlled design (i.e. Zelen design) to minimize false hopes, resentment, and contamination in the control group participants. 53 The Zelen pre-randomization design method allowed participants to initially consent to providing observational data and then provided them with an opportunity later for further consent if they were pre-randomized to receive the intervention.
Enabling participant autonomy
Interventions that provided participants with opportunities for choice and autonomy also appeared to support participant engagement. One study highlighted that participants were interested in being able to define their own problems and solutions while using an app, 84 while another highlighted the fact that their app did not provide opportunities for personalization as a limitation. 46 Other studies found that the use of open-ended sharing allowed for participants to set their own health and well-being priorities, and to engage at their own comfort levels.53,54 Methodologies that honored participant expertise also supported participant autonomy. For example, one study noted that including Indigenous youth throughout the research process as citizen scientists was a key component for facilitating empowerment, 55 while other studies discussed involving young participants as researchers and viewing their role as content experts,50,62 which provides participants with further autonomy during intervention development.
Functional considerations
App use was supported by easy sign-up processes 52 and clear navigation52,84 within apps. Customization of content (e.g. interactive videos) 59 and of problems/solutions to work on 84 were also identified as functional considerations that facilitated greater ownership and engagement with app interventions in future iterations of the technology. For text message-based interventions, several studies provided recommendations for message interactivity and frequency.49,67,83 Recommendations included requiring more active engagement from users, 49 using open-ended weekly text messages, 53 using a “Call to Action” within text messages, 67 allowing for open-ended sharing options,75,76 encouraging anonymous use,38,84,86 and using a high message frequency. 83
Developing interventions for those who support youth
Other studies examined interventions that could improve mental health support systems more broadly by increasing support and facilitating skill-building for “natural helpers” (i.e. peers, parents, and trusted adults) within communities. 38 Online role-play training simulations were used to increase participants' capacity to support youth in psychological distress. 61 Several interventions also noted providing training and support for mental health workers,61,71,77,85 which supported the iterative design process during intervention development 61 and raised awareness of validated electronic mental health tools that are responsive for target communities. 85 Additional interventions were used to support frontline workers while in session, 77 and to support the development of practitioner knowledge and skill via professional-to-professional case consultation. 71
Reported barriers to eHealth implementation
Limited or lack of resources
Funding
Having access to adequate financial resources was described as a barrier to intervention success.43,62,83,85 Limited resources were reported to hinder an iterative design process 62 and lead to changes in the intervention's focus, target population, and intervention strategy over time. 62 While interventions can be sustainable once developed, unanticipated costs associated with development (e.g. conducting needs analysis, receiving ongoing feedback from subject matter experts and end users, conducting beta testing) 43 also hindered study success.
Access
Several other studies noted access to technology as a limiting factor.38,49,53–55,67,68,70,76,84,85 Access to the required technological devices68,84,85 (e.g. mobile phones 54 or devices with proper storage capacity for the intervention 49 ) was a noted barrier, as was the fragility of devices used. 77 Access to technology was noted as a reason that participants decided to opt into a study 76 and loss of access to technology was a reason that participants opted out. 67 One 62 study found that, while several participants in this study did not own a phone, the majority of participants felt that having a mobile phone would be helpful as it would support their access to resources beyond just the presented intervention (i.e. access to health care; access to emotional, mental, and spiritual forms of support during crisis; access to emergency text alerts, such as those for shelter opening during extreme weather or for notifications of “bad batch” incidents; and access to opportunities for privacy). 54 The authors noted that this lack of phone ownership must be understood within the context of colonization and the intersectional barriers that it has caused (e.g. substance use, poverty, and incarceration). 54
Difficulty connecting to the Internet or having access to data was also a barrier,38,49,54,55,59,77,83–85 particularly in rural and remote areas.55,59,77 High costs and existing debt with service providers were reported to prevent participants from maintaining regular cellular connectivity.53,84 Suggestions for navigating these barriers included providing mobile data plans for youth, 55 providing a free, one-time download for required apps,53,64,84 and engaging with community organizations that may already have access to the internet (e.g. schools). 55
Intervention scope
e-MH interventions alone may not be sufficient to holistically address user needs,38,49,52,69,77,83,84 and could be used in conjunction with other services or supports,49,52,83,84 particularly for those with co-morbid or complex mental health needs. Some participants expressed concerns regarding the extent of support that can be obtained from a single app in scenarios where more intensive supports are needed (e.g. ongoing patterns of family violence 52 ) or where mental health concerns are caused by broader historical factors, such as colonization. 84 In one study, individual-focused apps promoting behavioral change had relatively small effects at the population level, suggesting that such options may have a low impact (irrespective of the degree of participation from the target population) in the absence of structural interventions. 49
Technological competence, youth safety, and literacy
Information technology (IT) literacy levels 85 and technical skill gaps 52 challenged e-MH intervention use, while support articles 52 and extensive training with the app 83 were reported to encourage use. Parents reported concerns maintaining youth safety in an online environment, relating to cyberbullying and inappropriate content or advice on unmonitored boards. 52 Similarly, addressing aspects of confidentiality, anonymity, and privacy were reported to help maximize engagement. 71 Literacy and language differences were identified as barriers to intervention use by participants, 84 while lack of knowledge regarding e-MH interventions (e.g. understanding effectiveness and applicability of resources for specific target populations) was identified as a barrier by healthcare workers. 85
Discussion
The aim of this review was to provide an updated summary of the literature on e-MH interventions for Indigenous youth conducted to date. This review shows an increase within this research area as evidenced by the jump from 10 studies previously 37 to 48 studies presently. This increase brings the need for reflection on facilitators and barriers to implementation processes of e-MH interventions, and for the creation of standards/criteria considerations to support future development.
The most common mental health concerns targeted in studies in this review were smoking cessation and suicide prevention. Text messages, apps, and websites were the most frequently reported types of technology used. Quantitative outcomes were reported most often (i.e. within 16 studies), contrasting the reporting of quantitative outcomes in the previous report (i.e. within three studies). 37 This review also found more protocol/proposal reports than our previous (12 vs. 2, respectively), supporting the conclusion that the number of studies within this research area is expanding. The inclusion of the “design and development” study outcome category can similarly be taken as evidence for a growing area of research. The most common process for developing an intervention was to create a novel intervention, however, additional development methods were used, such as developing e-MH interventions from previously existing in person interventions for Indigenous youth. Iterative development (i.e. working group consultations, community engagement in treatment adaptations, etc.) was also commonly used, and was noted to be beneficial as it allows for cumulative and targeted efforts to meet the needs of the Indigenous youth the interventions are designed to serve.
Several facilitators were noted to support e-MH intervention development and implementation. Incorporating community-based participatory research approaches throughout was found to be important; namely, including participants in the co-design process,38,46,48–53,55,59,61,62,64,65,67,68,70–72,77,78,81–84,86,87,89 ensuring opportunity for an iterative co-design process,38,46,56,59,61,62,68,72,73,77,82 and maintaining close partnerships with communities50,53,65,67,70–72 were commonly noted features of research designs that supported successful intervention development. Representation of culture was also important to ensure that the e-MH interventions were culturally matched to their Indigenous youth users.38,45,46,48–52,55,59,61,62,64,67,68,70,72–82,84–89 This occurred in both surface-level details of the interventions, such as in the language used and images included, and in the deeper level details of the intervention, such as the cultural contexts and values communicated. Including aspects of culture throughout various points in the research design process (e.g. culturally appropriate incentives, assessments, and comparison study arms) also facilitated intervention development.45,55,59,76,87
Various methods of motivating participant engagement, such as the use of targeted recruitment methods (e.g. radio station advertisements, word of mouth, and positive-toned Facebook Ads), modern communication mediums (e.g. familiar social networks such as Instagram or TikTok, familiar school websites), and aspects that support participant autonomy (e.g. opportunities for personalization, open-ended sharing, and sharing of participant expertise) also supported intervention development. Functional considerations relating to accessibility (e.g. easy-to-use methods for app navigation and customization) and level of required interactivity (e.g. bi-directional and dynamic messaging) within the e-MH intervention platforms were also important factors considered throughout the development process. Finally, the development of support for those who support Indigenous youth (e.g. community members and primary care providers) was also a reported facilitator.38,43,61,71,77,85 This style of approach is valuable because it extends beyond the individual user of e-MH intervention and provides resources that can be used to support Indigenous youth from a community level.
Several barriers were also noted to hinder e-MH intervention development and implementation. Notably, several studies reported having limited access to the resources necessary to conduct their research.38,43,49,53–55,62,67,68,70,76,83–85 Insufficient financial resources were commonly reported, as well as insufficient access to the required technological devices and connection services (e.g. cellular networks and Wi-Fi networks). To bypass these barriers, researchers suggested creating apps that only require one-time downloads. Another broad category of barriers found was the limit to the amount of support that can be provided by online interventions.38,49,52,69,77,83,84 This limitation was prominent for youth with more severe mental health concerns, suggesting the need for these types of supports to be used in tandem with in-person care. Indigenous youth using e-MH interventions face challenges that are far beyond the scope of a single app (e.g. intergenerational trauma and reconnection to culture) and thus, these supports must be provided in tandem with policies and programs that will also support structural and system-level change. Finally, additional barriers identified included low levels of both IT and general literacy,49,52,83–85 as well as aspects of the research designs used (e.g. small samples and short trial durations), which should also be considered when developing and implementing future e-MH interventions.
Future directions
Standards and criteria considerations for future development of e-MH interventions for Indigenous youth
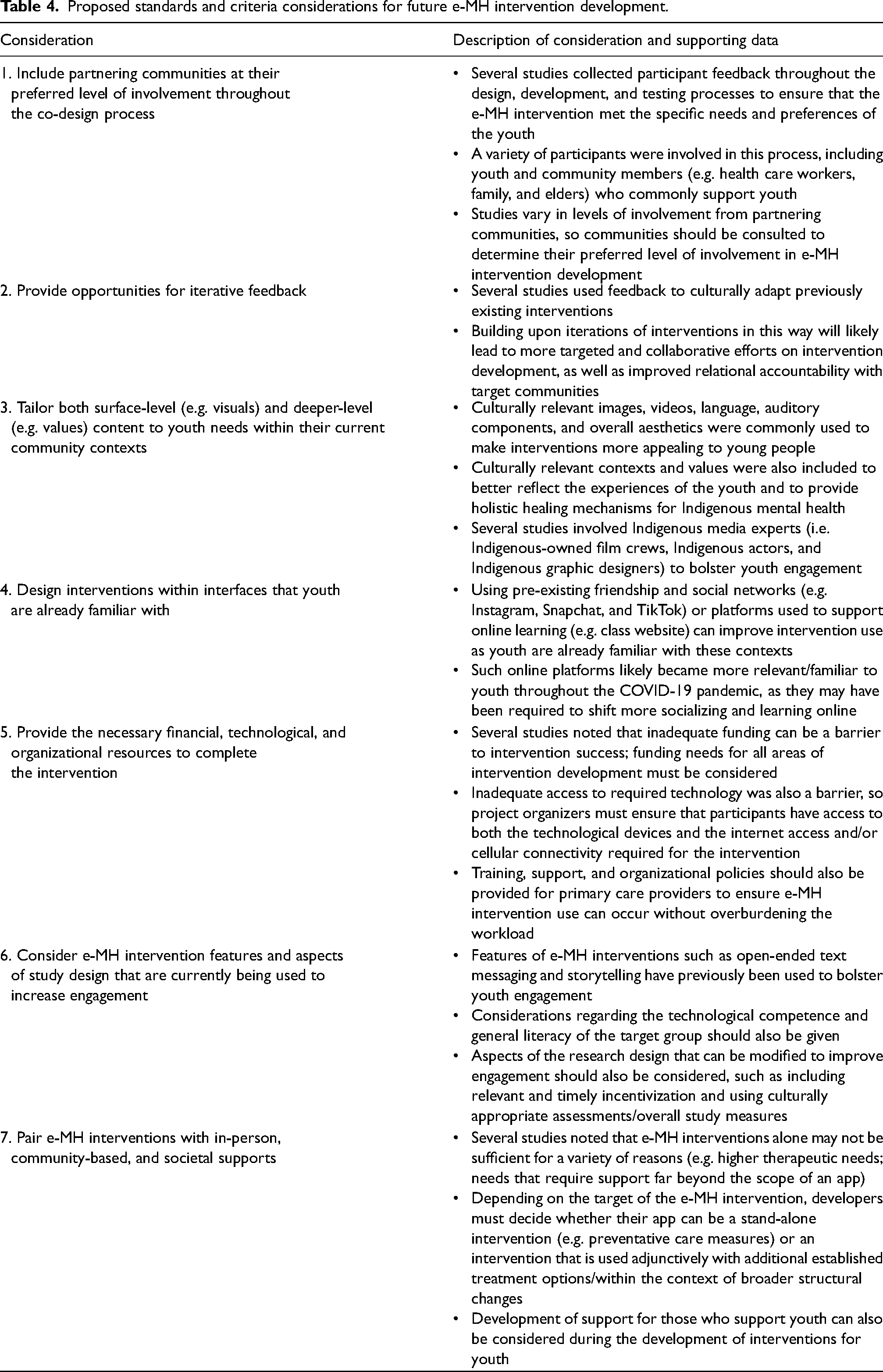
Beyond summarizing study characteristics, facilitators, and barriers, the final purpose of this updated systematic review was to provide considerations for standards and criteria that can be used to inform the processes for e-MH intervention development. The practices that occurred most often in the literature were considered in tandem with the known facilitators and barriers for Indigenous youth accessing e-MH care to generate tangible suggestions for those looking to develop e-MH interventions in the future. The findings of this review are bolstered by several of the recommendations from the previous review. 37 Our seven considerations for standards and criteria of e-MH intervention development from this review are presented in Table 4.
Proposed standards and criteria considerations for future e-MH intervention development.
Future reviews needed
To better understand the types of e-MH research that are currently ongoing and if the field is growing (i.e. via the availability of protocol studies), the categories of outcomes within studies were briefly summarized. Future systematic reviews should further examine specific e-MH intervention outcomes to better understand the effectiveness of these methods. Specifically, reviewers could examine e-MH intervention effectiveness for apps designed to promote overall well-being among Indigenous youth, which may promote Indigenous views of holistic wellness. Additional review topics within the realm of e-MH interventions may examine which modalities best support user engagement, why developers opt to create novel interventions vs. adapting previously existing ones, and which factors best facilitate the integration of e-MH intervention with additional interpersonal and societal supports.
Conclusion
There has been an increase in published studies and protocols for eMH interventions used to support the mental wellness of Indigenous youth since our previous examination. 37 As this research becomes more available, there is a greater need for further summarizing of the types of concerns targeted, technology used, outcomes reported, and processes included for development. Consideration must also be given to the factors that are known to help or hinder youth engagement with these e-MH interventions, and these facilitators and barriers should be addressed in iterative rounds of collaborative research to ensure the specific mental health needs of the targeted population are met. To help meet these needs, we have provided seven considerations relevant to future research examining e-MH interventions designed to support Indigenous youth, which build upon those provided by Toombs et al. 37 Future research should continue to support the iterative development of e-MH interventions and should aim to fill gaps that currently exist within this area.
Footnotes
Acknowledgements
This article was supported by the Thunderbird Partnership Foundation. This article summarizes a report written for and with Thunderbird Partnership Foundation to summarize recent research developments and processes regarding available digital mental health interventions for Indigenous youth. The authors are grateful for the guidance, comments, and feedback provided by members of the Thunderbird Partnership Foundation during the drafting of this report.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CJM's participation in this project was partially supported by the Canada Research Chairs Program, grant number CRC-2019-00069 and by the Canada Foundation for Innovation (grant number 33721). ET's participation in this project was partially supported by a Canadian Institutes of Health Research (CIHR) Banting Postdoctoral Fellowship (grant number 454119). LJH, ET, JL, KRK, and CH's participation in this project was supported by funding from the Thunderbird Partnership Foundation.
Data availability statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.