
Abstract
Introduction
Videoconferencing circumvents various physical and financial barriers associated with in-person care. Given this technology's potential benefits and timely nature, we conducted a systematic review to understand how videoconferencing for chronic obstructive pulmonary disease (COPD) follow-up care affects patient-related outcomes.
Methods
We included primary research evaluating the use of bidirectional videoconferencing for COPD patient follow-up. The outcomes of interest were resource utilization, mortality, lifestyle factors, patient satisfaction, barriers, and feasibility. We searched MEDLINE, EMBASE, EBM Reviews, and CINAHL databases for articles published from January 1, 2010, to August 2, 2021. Relevant information was extracted and presented descriptively and common themes and patterns were identified. The risk of bias for each study was assessed using design-specific validated tools.
Results
We included 39 studies of 18,194 patients (22 quantitative, 12 qualitative, and 5 mixed methods). The included studies were grouped by type of intervention; 18 studies explored videoconferencing for exercise, 19 explored videoconferencing for clinical assessment/monitoring, and 2 examined videoconferencing for education. Generally, videoconferencing was associated with high levels of patient satisfaction. There were mixed results in terms of its effects on resource utilization and lifestyle-related factors. Additionally, 12 studies were at high risk of bias, indicating that these results should be interpreted with caution.
Conclusions
The videoconferencing interventions resulted in high levels of patient satisfaction, despite facing technological issues. Overall, more research is needed to better understand the effects of videoconferencing interventions on resource utilization and other patient outcomes, quantifying their advantages over in-person care.
Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of global morbidity and mortality, accounting for 3.2 million deaths worldwide in 2019.1–3 Furthermore, the European COPD Audit found a 90-day all-cause readmission rate of 35.1%. 4 In the United States, an analysis of Medicare claims data identified a 30-day all-cause readmission rate of 20.2%. 5 Researchers and policymakers have recently begun using telehealth, technology-based medical services where distance is a factor, 6 for COPD management.7,8 Common applications of telehealth in COPD management include the monitoring of vital signs, patient education and self-management sessions, and pulmonary rehabilitation (PR) (i.e., supervised exercise and education sessions). 8 These technologies have the potential to benefit patients who experience barriers in access to care, 9 including rural,10,11 elderly,11,12 and Indigenous populations. 13
Videoconferencing, a division of telehealth, provides bidirectional synchronous communication between providers and patients. It offers the benefits of face-to-face contact while circumventing various physical and financial barriers to accessing in-person care. Videoconferencing has also been associated with high levels of patient satisfaction.14–16 Despite its advantages, this technology has not yet been widely implemented.
Several systematic reviews have summarized the effects of telehealth interventions on COPD management. However, few included videoconferencing-specific search terms or inclusion criteria.7,8,17–21 To our knowledge, Almojaibel 22 is the only systematic review to have focused specifically on videoconferencing. The review identified seven studies that evaluated the use of PR videoconferencing services for COPD patients. These interventions were well-accepted by patients, and no safety concerns were reported. This review specifically focused on PR-based interventions and only included literature published prior to 2015. To our knowledge, no reviews have assessed videoconferencing interventions focused on patient education, clinical assessment, or monitoring. Additionally, over recent years the context of the COVID-19 pandemic has further increased the popularity of telehealth for facilitating remote care,23–25 highlighting the need to understand the effectiveness of these technologies.
We conducted a systematic review to investigate how providing videoconferencing for COPD patient follow-up affects patient-related outcomes including resource utilization, mortality, lifestyle factors, satisfaction, barriers, and feasibility. Understanding these relationships will help inform recommendations for future research and practice.
Methods
Study design and eligibility criteria
A systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Checklist. 26 There is no published protocol associated with this review; all pertinent methodological details are available in the present manuscript and its supplement. This review included English-language primary research studies (clinical trials, quality improvement studies, and observational studies) with an available full text. The population of interest was adult patients (>18 years) with a confirmed COPD diagnosis. The target intervention was any form of videoconferencing, defined as a method of distance bidirectional face-to-face contact using telecommunication technologies. 27 Studies that did not include videoconferencing as the primary intervention were excluded. Our primary outcome was resource utilization, defined as all clinical-related visits following the intervention start date (hospital admissions and readmissions, emergency department visits, outpatient visits, exacerbations, and length of stay). Secondary outcomes included mortality, lifestyle factors, patient satisfaction, barriers, and feasibility. Table A1 contains the detailed eligibility criteria.
Search strategy
We systematically searched MEDLINE, EMBASE, EBM Reviews, and CINAHL electronic databases. The initial search was conducted on August 3, 2020, and it was subsequently updated on August 2, 2021 (Table A2). We only considered studies published after 2010 because prior studies would likely differ in terms of technology and clinical contexts.
Data extraction
Search results were aggregated and duplicates were removed using the Covidence platform. 28 Title/abstract screening was performed by two independent reviewers (MB and IS) to identify eligible articles, which were subsequently assessed for eligibility at the full-text level. Conflicts were resolved through consensus and, when needed, a third arbitrator (DTW).
Detailed information on the location, design, population, baseline characteristics, intervention, control, and outcomes was extracted by one reviewer and a random 10% sample was validated by a second reviewer for accuracy. We captured all qualitative and quantitative outcomes that aligned with our eligibility criteria and presented the findings descriptively using frequency counts and tables.
The included studies were grouped and presented by intervention domain based on how videoconferencing was used: exercise-based interventions, clinical assessment and monitoring interventions, and education interventions (Table 1). Within each domain, we presented outcomes in the following categories: quantitative, qualitative, and patient satisfaction and barriers (both qualitative and quantitative; combined due to the similar nature of these outcomes). All outcomes of interest were presented in the supplemental tables. In the main text, an abbreviated version of the tables was presented. To create the abbreviated tables, the overall themes for qualitative results were presented and a hierarchy was used for each quantitative outcome category, based on clinical relevance and frequency of outcome reporting (Table A3).
Videoconferencing domain definitions and examples
Risk of bias assessment
Risk of bias assessments were preformed independently by two reviewers (MB and IS) and, when needed, a third arbitrator (MJ). Randomized controlled trials (RCTs) were assessed using the Cochrane Risk of Bias Tool. 29 Non-randomized interventional studies were assessed using the Risk Of Bias In Non-randomized Studies – of Interventions (ROBINS-I) tool. 30 Observational studies were assessed using the Newcastle–Ottawa Scale. 31 Qualitative studies were assessed using the Critical Appraisal Skills Programme (CASP). 32 Based on the guidance of Long et al., 33 we identified CASP items one (research aims), three (design), eight (data analysis), and nine (statement of findings) as most relevant to our research question.
Results
The literature search identified 1334 records. Thirty-nine studies were included in the final synthesis (22 quantitative, 12 qualitative, and 5 mixed methods; Figure 1). Although some studies, such as Hoaas et al. 34 and Kooij et al., 35 appeared to meet our inclusion criteria, they were excluded because videoconferencing was not the main intervention component.
Study PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram.
Twelve of the included studies were RCTs, 9 were pre-post-intervention studies, 4 were non-randomized trials, 2 were retrospective cohort studies, and 12 were qualitative studies (Table 2, Table A4). The sample sizes ranged from n = 6 36 to n = 11,303, 37 and most (74%) had a sample size of 100 or less. Twenty-two studies were conducted in Denmark, six in Norway, five in the United States, two each in Australia and Canada, and one each in the Netherlands and South Korea. Length of study follow-up ranged from 7 days 38 to 5 years. 37
Summary of the study design characteristics and risk of bias for all included studies (n = 39).
*Compared same sample before/after intervention; **Results presented for COPD subgroup only, ***No control group.
Note: Outcome sample sizes are equal to sample sizes at baseline unless otherwise specified.
d: day; F/U: follow-up; HRB: high risk of bias; LRB: low risk of bias; mo: month; nRCT: non-randomized controlled trial; OT: occupational therapist; PC: prospective cohort; PR: pulmonary rehabilitation; PT: physiotherapist; RC: retrospective cohort; RCT: randomized controlled trial; UC: usual care; wk: week.
Risk of bias
Twelve RCTs were assessed for risk of bias using the Cochrane Risk of Bias tool; nine were deemed low risk (LRB) and three were deemed high risk (HRB) (Table 2, Table A5). Using the ROBINS-I scale, we evaluated the risk of bias for 13 non-randomized interventional/observational studies (Table 2, Table A6). One study was deemed low risk (LRB), six moderate risk (LRB), five serious risk (HRB), and one critical risk (HRB). Two cohort studies were assessed using the Newcastle–Ottawa scale, both of which were low risk (LRB; Table 2, Table A7). Twelve studies were appraised using the CASP qualitative checklist; nine were considered low risk (LRB) and three high risk (HRB; Table 2, Table A8).
Domain 1 – exercise-based interventions with videoconferencing
Quantitative outcomes
Thirteen studies (10 quantitative and 3 mixed methods) presented quantitative outcomes for exercise-based videoconferencing interventions (Table 3; Table A9).39–51 All included some form of group-based or individually tailored exercise. Most also included educational40,41,43,44,46–48 and/or symptom telemonitoring39,42,44,46,50,51 components. The exercise programs ranged from 3 weeks 47 to 24 months, 50 with most lasting 8–10 weeks.39,41–44,46,48,49 Three studies were RCTs.41,43,49
Summary of key outcomes for the n = 27 studies reporting quantitative outcomes.
Note: For feasibility, lifestyle, patient satisfaction, and barrier outcomes, when multiple time points were recorded, we reported the longest available follow-up. Significant findings are noted in bold. See Table A3 for the hierarchy used to select relevant outcomes for this summary table.
AECOPD: acute exacerbation of chronic obstructive pulmonary disease; BCKQ: Bristol COPD Knowledge Questionnaire; C: control group; CAT: COPD Assessment Test; CCQ: Clinical COPD Questionnaire; CI: confidence interval; COPD: chronic obstructive pulmonary disease; CRQ: Chronic Respiratory disease Questionnaire; CSES: COPD Self-Efficacy Scale; d: day; ECOPD: exacerbation of chronic obstructive pulmonary disease; FEV1: forced expiratory volume in 1 s; I: intervention group; IQR: interquartile range; MD: mean difference; mo: month; NIV: non-invasive ventilation; OR: odds ratio; PR: pulmonary rehabilitation; PT: physiotherapist; RC: retrospective cohort; RCT: randomized controlled trial; SD: standard deviation; SEM: standard error of the mean; SGRQ: St George's Respiratory Questionnaire; SUS: System Usability Scale; VAS: Visual Analog Scale; VVL: visual verbal learning; wk: week.
Five studies compared resource utilization outcomes between groups and the results were varied. In a matched comparison of patients receiving PR via videoconference versus those receiving the standard of care (no PR), Bhatt et al. 40 (LRB) reported a significant reduction in 30-day all-cause and acute exacerbation of COPD (AECOPD) readmissions (readmission rate in PR via videoconferencing vs. standard of care for all-cause: 6.2% vs. 18.1%, p = 0.013 and for AECOPD: 3.8% vs. 11.9%, p = 0.040). In a comparison of PR via videoconference and conventional PR, Hansen et al. 43 (LRB) found no significant difference in COPD-related hospitalizations after the intervention period (p = 0.77) or the 22-week follow-up (p = 0.97).
Three studies reported cost-related feasibility outcomes.39,47,51 A 3-week study of physiotherapist training plus occupational therapist counseling in Denmark found that total expenditures cost up to €956 per patient (LRB). 47 In a pre-post evaluation of a telerehabilitation program, Zanaboni and colleagues 51 (LRB) reported a 27% reduction in 6-month COPD-related hospital costs compared to the 6 months before the program (p = 0.50).
The exercise-based interventions were largely successful in improving lifestyle-related outcomes. An RCT conducted by Hansen et al. 43 (LRB) identified significant improvements on the Hospital Anxiety and Depression Scale among those receiving videoconference-based PR compared to those receiving conventional PR (10-week change from baseline adjusted difference [conventional videoconference] on anxiety scale: 1.2, 95% confidence interval [CI] 0.2–2.3, p < 0.05, depression scale: 0.9, 95% CI 0.1–1.7, p < 0.05). Another RCT, Tsai et al. 49 (LRB), reported similar improvements among those receiving videoconferencing versus usual care. Burkow and colleagues 39 (LRB) reported significantly better health-related quality of life (HRQoL) as measured by St George's Respiratory Questionnaire at post-intervention compared to baseline (mean change score pre to post: −6.53, 95% CI −12.68 to −0.38, p = 0.04). However, some studies found null or negative results in terms of lifestyle outcomes (e.g., Godtfredsen et al., 41 Hansen et al., 43 and Stickland et al. 48 ).
To summarize, while no overwhelming evidence was found in support of exercise-based videoconferencing, we observed promising improvements in lifestyle outcomes. The majority of rehabilitation studies had a significant improvement in this category (n = 7/12). The one study that looked at a yoga intervention also found a significant improvement in one or more lifestyle factors (Table 4).
Summary of outcomes for all included quantitative studies (n = 27).
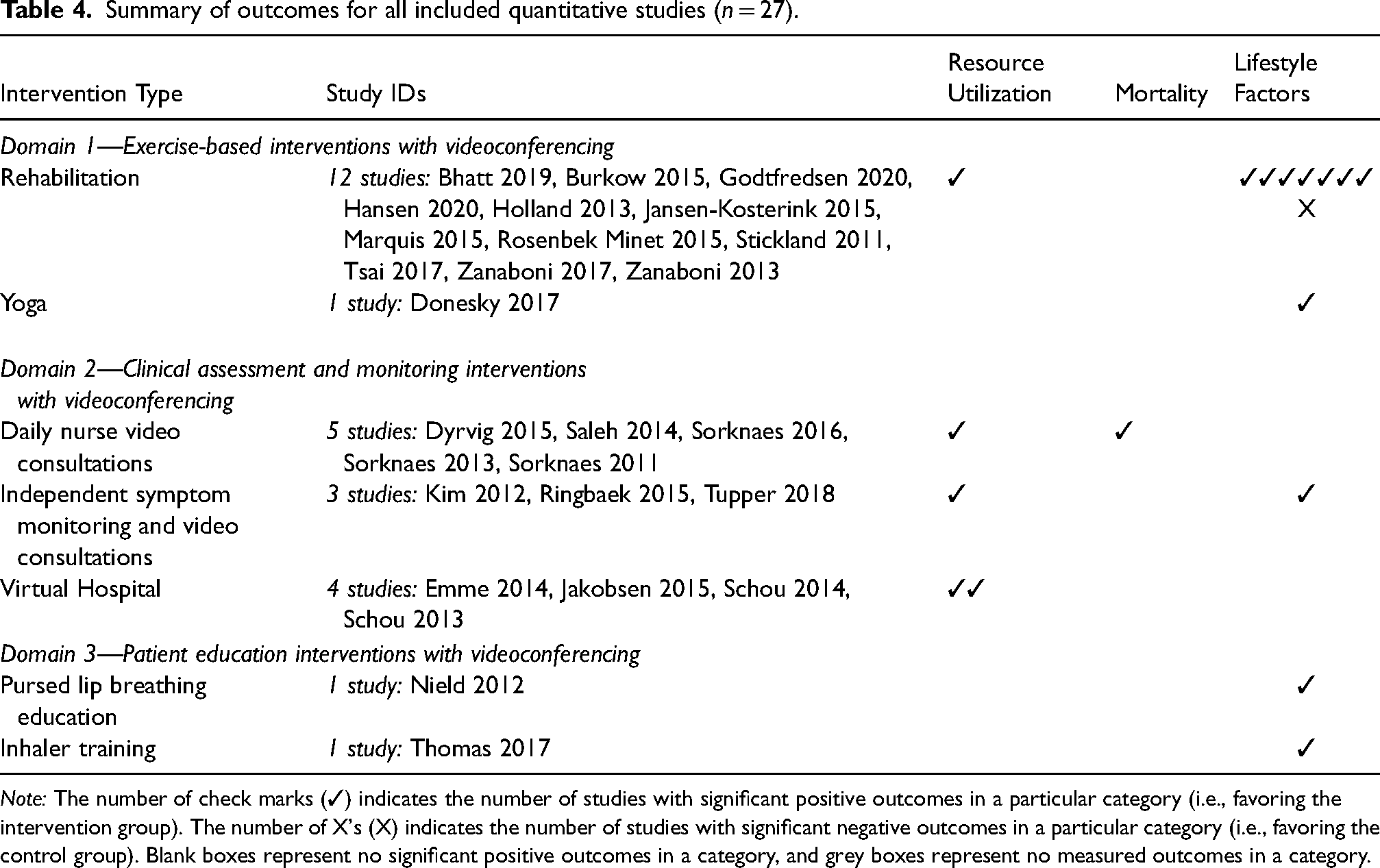
Note: The number of check marks (✓) indicates the number of studies with significant positive outcomes in a particular category (i.e., favoring the intervention group). The number of X's (X) indicates the number of studies with significant negative outcomes in a particular category (i.e., favoring the control group). Blank boxes represent no significant positive outcomes in a category, and grey boxes represent no measured outcomes in a category.
Qualitative outcomes
Five studies presented qualitative outcomes (four qualitative and one mixed method; Table 5, Table A10).39,52–55 Among these studies, two main themes were identified. The first theme was patient experience living with COPD (n = 4 studies).52–55 Most patients agreed that videoconferencing interventions improved feelings of support, increased disease knowledge, coping ability, and accessibility to healthcare professionals and provided reassurance, greater clinical insight, and opportunities to participate actively in care.
Summary of key outcomes for the n = 13 studies reporting the main qualitative themes.
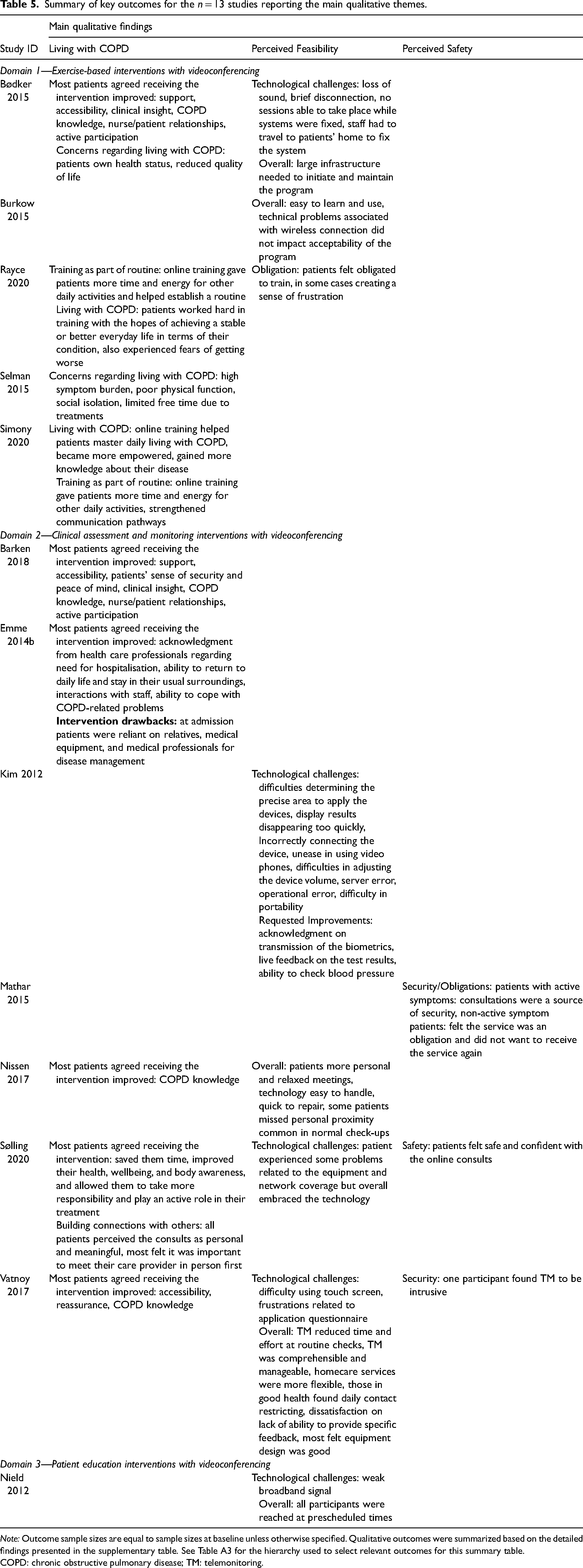
Note: Outcome sample sizes are equal to sample sizes at baseline unless otherwise specified. Qualitative outcomes were summarized based on the detailed findings presented in the supplementary table. See Table A3 for the hierarchy used to select relevant outcomes for this summary table.
COPD: chronic obstructive pulmonary disease; TM: telemonitoring.
The second theme was the perceived usability and technological feasibility of the videoconferencing interventions (n = 3 studies).39,52,53 The findings within this theme were varied. For example, one study reported that the participants found the equipment user-friendly (LRB). 39 However, two studies noted a variety of technological challenges including connection problems and loss of sound,39,52 and another reported that patients found the videoconferencing intervention to be an obligation (LRB). 53
Patient satisfaction and barriers to use
Twelve studies reported patient satisfaction outcomes (two qualitative, seven quantitative, and three mixed methods; Table 6, Table A11).39,40,42,43,45–47,49,51,54,56 Patient satisfaction was consistently high. Qualitative evidence suggested that the videoconferencing programs were well received and that patients felt they experienced positive health changes as a result of the intervention.39,47,51,54 Quantitatively, Burkow and colleagues 39 (LRB) reported a mean System Usability Scale score of 94.4/100 for the videoconferencing users. Several studies reported technology issues as a barrier to the use of videoconferencing. For example, Donesky et al. 42 (HRB) found that just 23% (n = 7) of their sessions occurred without technical issues.
Summary of key outcomes for the studies reporting on patient satisfaction and/or barriers to use (n = 11 studies reporting qualitative outcomes, n = 15 studies reporting quantitative outcomes).
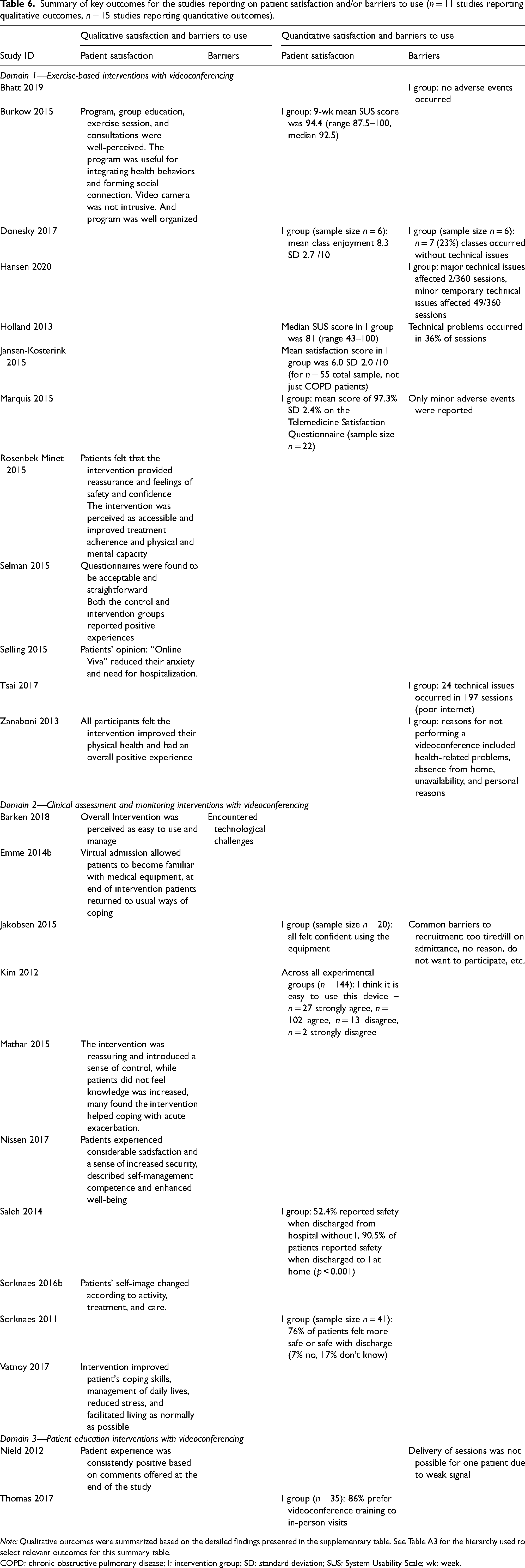
Note: Qualitative outcomes were summarized based on the detailed findings presented in the supplementary table. See Table A3 for the hierarchy used to select relevant outcomes for this summary table.
COPD: chronic obstructive pulmonary disease; I: intervention group; SD: standard deviation; SUS: System Usability Scale; wk: week.
Domain 2—Clinical assessment and monitoring interventions with videoconferencing
Quantitative outcomes
Twelve studies (11 quantitative and 1 mixed method) presented quantitative outcomes for clinical assessment/monitoring videoconferencing interventions (Table 3; Table A9).37,57–67 Four studies evaluated a virtual hospital intervention where patients received home treatment using telemedical equipment.57,58,62,63 Five studies provided daily nurse video consultations.37,60,64–66 Three studies tested a combination of independent symptom telemonitoring and video consultations.59,61,67
Findings were mixed in terms of resource utilization. One study reported an increased rate of readmissions among their videoconference intervention group (42-day all-cause readmissions in videoconferencing vs. usual care: odds ratio 3.18, 95% CI 2.40–4.22, p < 0.0001) 37 (LRB) and the remaining six reported non-significant results.58,60,61,64–66 However, the clinical assessment and monitoring interventions showed promise in reducing patient length of stay.58,60 In addition, among patients on long-term oxygen therapy, Ringbaek et al. 61 (LRB) reported significantly fewer 6-month respiratory-related outpatient clinic visits among the group receiving telemonitoring plus video consults compared to usual care (video consults: mean 1.34 visits vs. usual care mean 1.41 visits, p < 0.001).
In an RCT by Sorknaes et al. 65 (LRB), each patient was expected to receive between 5 and 9 nurse video consultations and received a mean of 6.6 (range 0–9). In Saleh et al.'s60 pre-post study (HRB), patients were expected to receive at least 10 nurse video consultations and received a median of 10 (IQR 9–11).
To summarize, while the clinical assessment and monitoring interventions were feasible, the majority of outcomes in all categories were non-significant (Table 4). Half (n = 2/4) of the studies examining virtual hospitals reported significant positive findings for resource utilization. This proportion was greater than that of the studies examining daily nurse video consultations (n = 1/5) or independent symptom monitoring with video consultations (n = 1/3), which reported positive significant findings for resource utilization (Table 4).
Qualitative outcomes
Seven studies presented qualitative outcomes and three main themes were identified (six qualitative and one mixed method; Table 5, Table A10).36,57,59,68–71 The first theme was patient perspectives on living with COPD (n = 5 studies).57,68–71 All studies found that patients perceived improvements in their ability to live with COPD related to the videoconferencing intervention. Areas of benefit included increased feelings of support, ability to cope with COPD, COPD knowledge, and access to care.
The second theme was the perceived feasibility and usability of the videoconferencing interventions (n = 4 studies).59,69–71 Three studies reported that patients had positive feelings towards the technology. Video consults were found to reduce the time and effort of routine follow-up checks; the technology was easy to handle and problems that did occur did not change the overall acceptance of the programs.69–71 Three studies reported technological challenges.59,70,71
The final theme was perceived safety (n = 3 studies).36,70,71 Two opposing views stood out within this theme. Sølling et al. 70 (LRB) and Mathar et al. 36 (HRB) found that patients with active symptoms felt the videoconferencing intervention was a source of safety and security. Conversely, Mathar et al. 36 (HRB) reported that patients without active symptoms found the intervention to be an obligation.
Patient satisfaction and barriers to use
Ten studies reported patient satisfaction outcomes (six qualitative, three quantitative, and one mixed method; Table 6, Table A11).36,38,58–60,66,68,69,71,72 All studies reporting qualitative outcomes found that patients were considerably satisfied. The interventions were seen as reassuring and allowed patients to continue with their daily lives. This was supported by quantitative measures. For example, 95% of patients receiving daily nurse teleconsultations recommended this as a replacement for standard care (LRB). 66 Technological challenges were a barrier to the telemonitoring intervention in Barken et al. 68 (LRB).
Domain 3—Patient education interventions with videoconferencing
Quantitative outcomes
Two studies evaluated quantitative outcomes for educational videoconferencing interventions (Table 3, Table A9).73,74 Nield et al. 73 (HRB) conducted a mixed methods RCT of video-based weekly pursed lips breathing education sessions. After 4 weeks, the videoconferencing group reported significantly higher social and emotional support compared to the control group receiving a single in-person education session and brochure (mean social support score: Skype 74.1 standard error (SE) 6.6 vs. control 51.6 SE 7.2, p = 0.02; mean emotional support score: Skype 33.8 SE 2.8 vs. control 23.5 SE 3.0, p = 0.02); however, these differences were attenuated by the end of 12-week study (social p = 0.12, emotional p = 0.14). Thomas et al. 74 (LRB) conducted a quantitative pre-post study of monthly inhaler training sessions via videoconference. The authors reported significant improvements in the Chronic Respiratory Disease Questionnaire subscales from baseline to follow-up (dyspnea +0.3 points, fatigue +0.6 points, emotional +0.5 points, mastery +0.7 points; all p ≤ 0.01).
Overall, very few studies examined patient education interventions with videoconferencing (Table 4). Although promising findings were observed for lifestyle factors in both studies (n = 1 pursed lip breathing education intervention, n = 1 inhaler training intervention), further examination is required.
Qualitative outcomes
One study examined qualitative outcomes (HRB) (Table 5, Table A10). They found that despite weak broadband signals, all participants completed their sessions at the prescheduled time. 73
Patient satisfaction and barriers to use
Both studies reported patient satisfaction outcomes (one quantitative and one mixed methods; Table 6, Table A11). Thomas et al. 74 (LRB) found that 86% of patients preferred videoconference training over in-person training. Similarly, Neild et al. 73 found patients were highly satisfied with the intervention and reported few technical problems (HRB).
Summary of qualitative themes
Three common themes emerged across the intervention domains, reported by 13 of the 17 qualitative and mixed methods studies (Table 5, Table A10). Firstly, patients agreed that videoconferencing interventions improved life with COPD by providing increased support, accessibility, and COPD knowledge. Secondly, patient perceptions of the feasibility of videoconferencing were cautiously optimistic, with positive feedback balanced almost equally by varying levels of technological challenges. Finally, due to conflicting findings among the small number of studies that reported on patient-perceived safety, no conclusions could be drawn. The remaining four studies reported patient satisfaction and barrier qualitative outcomes only.
Discussion
This systematic review summarizes recent evidence on videoconferencing for COPD follow-up care. We identified 39 studies exploring videoconferencing in the context of exercise, clinical assessment/monitoring, and education. Overall, videoconferencing interventions were well-received by patients and showed improvements in resource utilization and lifestyle-related outcomes in certain settings. However, we also identified potential issues regarding technological feasibility.
This review found that some videoconferencing interventions reduced resource utilization while others did not. Several studies comparing video-based care to its in-person equivalent found null effects in terms of resource utilization (e.g., virtual hospital care, 58 virtual PR, 43 and telemonitoring 61 ), indicating that in these settings videoconferencing may be as equally effective as in-person care. Given that videoconferencing reduces common barriers to in-person care (e.g., access to transportation, travel time),10,75 it may be advantageous for COPD patient follow-up. Future research should focus on better understanding the effects of these types of videoconferencing interventions on clinical outcomes and quantifying their advantages over in-person care. However, we also acknowledge there were few significant differences in resource utilization within studies comparing videoconferencing interventions to standard care.60,64–66 This observation may in part be due to heterogeneity in the definition of standard care.
We found that videoconferencing interventions were associated with high levels of patient satisfaction. Videoconferencing allowed patients to participate in their own care, improved the relationship between patients and providers, and gave greater clinical insight. These findings are consistent with the existing literature; a recent review of reviews examining videoconferencing among patients with long-term conditions reported that despite finding no concrete evidence for or against improvements in clinical outcomes, patient satisfaction was high. 76
Our review identified technological issues as the main barrier to the use of videoconferencing. Although videoconferencing can improve access to care among those who live in rural areas or have limited mobility, 10 it is important to consider that some of these populations may lack access to the internet and/or videoconferencing devices or may lack skills in navigating this technology. For example, inexperience with technology and lack of caregiver support may contribute to lower uptake of videoconferencing among older adults.77,78 Lower income and racialized populations experience a disproportionate lack of access to the internet and videoconferencing devices.79,80 Several studies in our review excluded participants based on their lack of internet access39,42,51 or lack of technology skills, 67 which may have limited the generalizability of their samples to the aforementioned populations.
Importantly, internet coverage and access to videoconferencing-enabled devices have been steadily improving among rural and low-income populations over recent years. 81 In cases of inaccessibility, satellite care sites can also provide access to videoconferencing technologies with greatly reduced travel times.82–84 In addition, various other solutions can be applied to improve access to videoconferencing within hard-to-reach populations. For example, mobile-friendly platforms may provide greater ease of use for patients who only have access to the internet through a mobile phone. 85 Subsidizing the costs of technology may also support access. 85 Ultimately, increasing access to videoconferencing will allow patients to develop the knowledge and skills to manage their condition without the need to travel to a care center. 86
Overall, the exercise-based interventions were successful in improving lifestyle-related outcomes such as anxiety and depression and, in some cases, HRQoL. This aligns with the work of Almojaibel, 22 which identified positive trends in exercise capacity, dyspnea, HRQoL, and sense of social support among COPD patients receiving video-based PR. One possible mechanism supporting this effect may be the association between technology use and increased self-efficacy through the development of positive emotional functioning, coping, and self-management skills.49,87,88 In turn, this may contribute to improvements in mental health and HRQoL.89,90
Strengths and limitations
Our review has a number of strengths. Firstly, we examined a novel topic that has the potential to impact policy and practice, particularly given the ongoing COVID-19 pandemic. Restricting to studies from the past 11 years allowed us to present the current state of videoconferencing in COPD follow-up care. Further, this review captured quantitative, qualitative, and mixed methods studies, creating a comprehensive picture of the literature. Lastly, a bias assessment was performed using a validated risk of bias tools,29–32 allowing us to identify studies at high risk of bias and consider their findings accordingly.
Our review also had several weaknesses we would like to acknowledge. For feasibility reasons, our search was limited to English-language peer-reviewed studies, which may introduce publication bias. Only two studies explored videoconferencing for education, limiting our ability to draw conclusions within this domain. More generally, a high level of heterogeneity in study design, outcomes, and quality made it difficult to compare studies. In the future, the use of standardized outcome measures may improve comparability. Lastly, 12 of 39 (31%) included studies were at a high risk of bias, limiting our ability to draw accurate conclusions. However, this may be due, in part, to the use of the Cochrane Risk of Bias tool to assess bias in RCTs. This tool penalizes studies that are unable to blind participants, such as the studies included in this review, resulting in a higher assessed bias.
Conclusion
The COVID-19 pandemic has increased the need for remote patient-care strategies such as videoconferencing, which enables real-time face-to-face communication with patients. Our review identified three domains of videoconferencing interventions for COPD follow-up care: exercise-based, clinical assessment and monitoring, and education. Despite encountering technological issues, patients using videoconferencing interventions reported consistently high levels of satisfaction and improved perceptions of living with their condition. In addition, some studies found no significant difference in healthcare resource utilization when comparing videoconference-based care to an in-person equivalent. This suggests that in some cases, videoconferencing may be as effective as in-person care. Additional promising findings were seen for lifestyle outcomes within exercise-based studies. Going forward, additional high-quality research is needed to better understand these potential effects and to make further comparisons with in-person equivalents.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X231158140 - Supplemental material for Videoconferencing interventions and COPD patient outcomes: A systematic review
Supplemental material, sj-docx-1-jtt-10.1177_1357633X231158140 for Videoconferencing interventions and COPD patient outcomes: A systematic review by Meghan Bowman, Matthew Jalink, Isobel Sharpe, Siddhartha Srivastava and Don Thiwanka Wijeratne in Journal of Telemedicine and Telecare
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Southeastern Ontario Academic Medical Organization (SEAMO) Innovation Grant (Don Thiwanka Wijeratne, Siddhartha Srivastava); Don Thiwanka Wijeratne received funding from Ontario Drug Policy Research Network and Canadian Institute of Health Research, Cardiovascular Network.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.