
Abstract
Introduction
This study aimed to identify opportunities for clinical decision support targeting medication safety in remote primary care, by investigating the relationship between clinical workflows, health system priorities, cognitive tasks, and reasoning processes in the context of medicines used in people with chronic kidney disease (CKD).
Methods
This qualitative study involved one-on-one, semistructured interviews. The participants were healthcare professionals employed in a clinical or managerial capacity with clinical work experience in a remote health setting for at least 1 year.
Results
Twenty-five clinicians were interviewed. Of these, four were rural medical practitioners, nine were remote area nurses, eight were Aboriginal health practitioners, and four were pharmacists. Four major themes were identified from the interviews: (1) the need for a clinical decision support system to support a sustainable remote health workforce, as clinicians were “constantly stretched” and problems may “fall through the cracks”; (2) reliance on digital health technologies, as medical staff are often not physically available and clinicians-on-duty usually “flick an email and give a call so that I can actually talk it through to our GP”; (3) knowledge gaps, as “it takes a lot of mental space” to know each patient's renal function and their medication history, and clinicians believe “mistakes can be made”; and (4) multiple risk factors impacting CKD management, including clinical, social and behavioural determinants.
Conclusions
The high prevalence of CKD and reliance on digital health systems in remote primary health settings can make a clinical decision support system valuable for supporting clinicians who may not have extensive experience in managing medicines for people with CKD.
Keywords
Introduction
Medication-related problems are responsible for 72,500 hospital admissions annually across rural and remote Australia, costing $400 million per year. 1 It is estimated that half of the hospital admissions are preventable. 1 A major challenge faced by rural and remote Australians is accessing health services, which leads to an increased burden of disease. The rate of hospitalisation and unintentional medicine-induced deaths in rural and remote Australia is about 2.4 and three times higher, respectively, than in urban Australia. 1 The Australian Commission on Safety and Quality in Health Care, in line with the third World Health Organization (WHO) Global Patient Safety Challenge: Medication Without Harm, aims to minimise preventable medication-related harm by 50% by 2025. 2
Chronic kidney disease (CKD) is a significant health concern in Australia, particularly for Indigenous Australians. 3 Indigenous Australians are twice as likely to have CKD compared with non-Indigenous Australians. 3 The Northern Territory (NT) has the largest proportion of Indigenous residents compared to other Australian States and Territories, with many residing Indigenous persons in rural and remote regions. 4 The hospitalisation rate for patients with CKD is three times higher in remote and rural regions compared with urban areas. 3 In 2017–2019, NT had the highest rate of hospitalisation for CKD (excluding dialysis) for Indigenous Australians (9.3 per 1000), 5 highlighting the need for interventions to support health professionals in their practice in this setting.
Patients with CKD frequently have multiple comorbidities, thus resulting in high levels of medication use. 6 Inappropriate medicine selection and dosing for patients with kidney impairment in primary care is a common preventable cause of emergency department (ED) admission. Reduced kidney function (eGFR < 60 mL/min/m 2 ) has been found to be a significant predictor of readmissions due to adverse drug reactions. 7 An Australian study showed that among patients with poor kidney function at the time of their admission, 16% were on a contraindicated medicine and 21% were on an inappropriate dose, 8 suggesting that interventions aimed at primary care prescribing can significantly reduce ED admissions.
Technological developments may be key in reducing potentially inappropriate medicine use and improving patient safety. A clinical decision support system (CDSS) is an evidence-based intervention to improve patient care. 9 However, its successful implementation in primary care depends on overcoming challenges such as outdated or missing information, 10 interference with clinical workflow, 11 and loss of autonomy. 12 Therefore, a CDSS to prevent inappropriate medicines for patients with kidney impairment, particularly in rural and remote areas, needs to draw information from multiple sources, be flexible, and involve all healthcare professionals in the prescribing-dispensing-administration chain.
The purpose of the current study was to identify opportunities for improvement in the medication management cycle particularly in remote primary health settings by leveraging decision support systems. Clinical workflows, health system priorities, cognitive tasks, and reasoning processes in the context of safely using medicine in people with kidney impairment were explored.
Methods
Study design
This qualitative study involved one-on-one, semistructured interviews (face-to-face or videoconference) with healthcare professionals (rural medical practitioners (RMPs), remote area nurses (RANs), Aboriginal health practitioners (AHPs) and pharmacists) from remote government-run health centres between November 2022 and January 2023. The semistructured interviews consisted of open-ended questions developed by the research team and used as a guide. The participants provided written informed consent prior to being interviewed. This study followed the COnsolidated criteria for REporting Qualitative research (COREQ) guidelines. 13
Participant recruitment
RMPs, RANs, and AHPs were recruited from a health service in Northern Australia. The pharmacists were recruited from pharmacies that provided medicine services to the remote primary healthcare centres of this health service. The participants were recruited using purposive sampling. Recruitment occurred via email invitations to the sites’ managers, who then nominated and identified suitable participants. A follow-up email was sent to the site manager to arrange the interview. Participation was voluntary, and no compensation or reimbursement was given to research participants.
Participant selection and setting
The eligibility criteria for study participation were healthcare professionals employed in a clinical or managerial capacity and who had clinical work experience in a remote health setting for at least 1 year. Primary care services in remote government-run health centres are mostly staffed by RANs and AHPs, with clinical support from visiting medical and allied health professionals,14,15 although remote government-run health rserving larger populations have residential medical staff. 16 Section 100 (S100) of the National Health Act 1953 allows eligible remote health rto access bulk supplies of Pharmaceutical Benefits Scheme (PBS) medicines with the exception of extemporaneous products, highly specialised drugs, and Schedule 8 medicines from an approved pharmacist (S100 pharmacist). 17 Chronic disease medicines are dispensed by the S100 pharmacy, usually in a dose administration aid (DAA), and supplied to patients by an AHP or RAN. Non-chronic disease medicines are provided in bulk and can be supplied and administered directly to patients without a medical officer, following a protocol approved by the chief health officer (CHO).
Data collection and analysis
The interviews were recorded for verbatim transcription and the duration of each interview was approximately 20–30 min. The interviews were conducted and transcribed by MT with supervision and review by AA. All participants were allocated a case number and transcripts were de-identified. NVivo was used for data management and analysis. All responses were de-identified, but the participant role (RMPs, RANs, AHPs, pharmacists) was maintained for context. Interview transcripts were emailed to research participants for respondent validation. Inductive thematic analysis, as described by Braun and Clarke, 18 was adopted to identify patterns in the data. Relevant segments of text were extracted by MT and reviewed by AA. Initial inductive codes were developed, which were then organised into subthemes. The research team reviewed and reached a consensus for the final themes.
Results
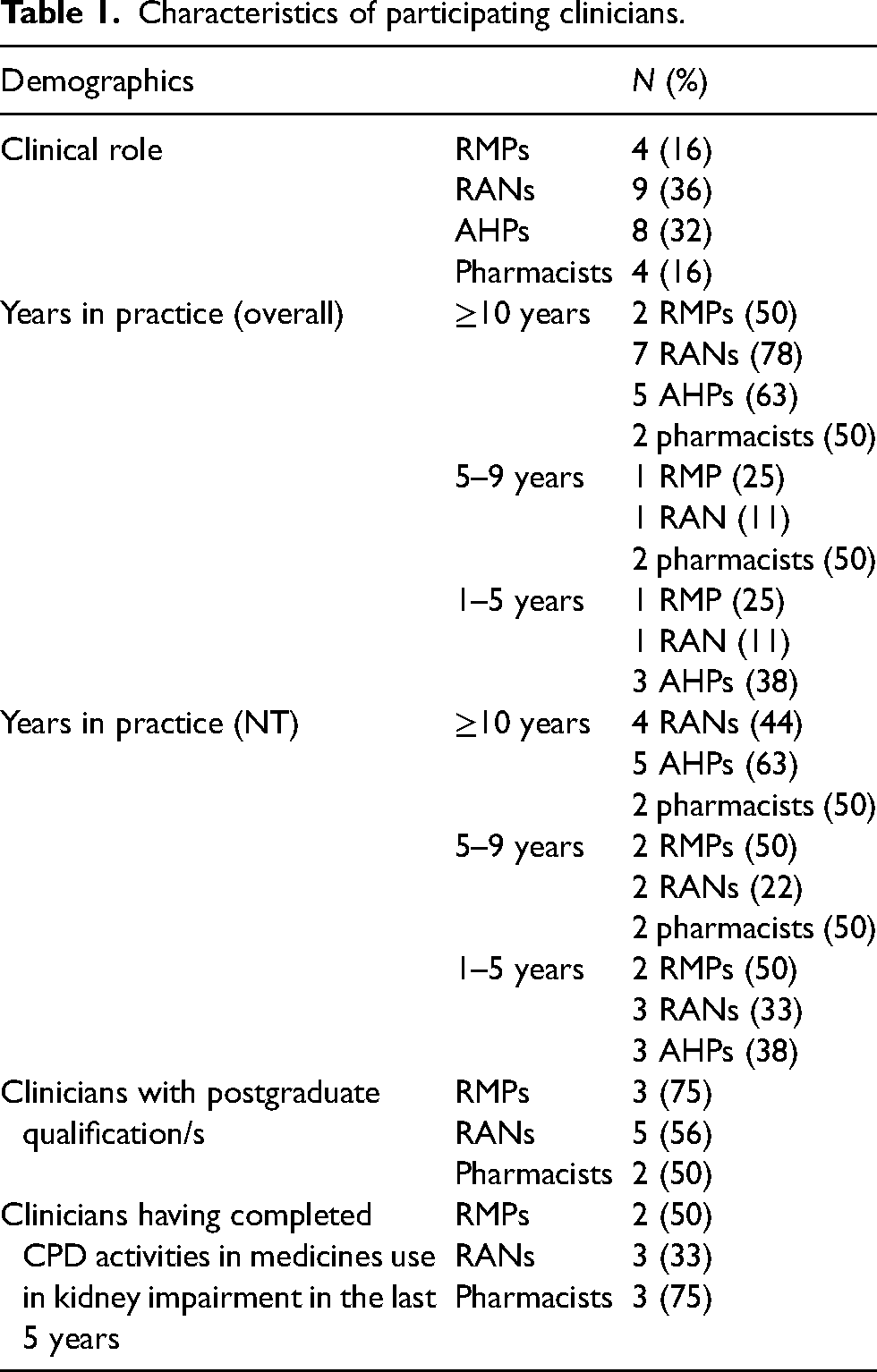
A total of 25 clinicians from four remote primary health centres and three pharmacy services were interviewed; four were RMPs, nine were RANs, eight were AHPs, and four were pharmacists. Most clinicians had been registered for ≥10 years (two RMPs (50%), seven RANs (78%), five AHPs (63%), and two pharmacists (50%)) (Table 1). All RMPs had been practising in NT for less than 10 years. Four RANs (44%) and two pharmacists (50%) had ≥10 years of clinical experience in dispensing for remote health settings while the majority of AHPs (63%) had been practising in NT for ≥10 years. Two RMPs (50%), three RANs (33%), and three pharmacists (75%) had completed continuing professional development (CPD) activities in medicines use in kidney impairment in the last 5 years (Table 1).
Characteristics of participating clinicians.
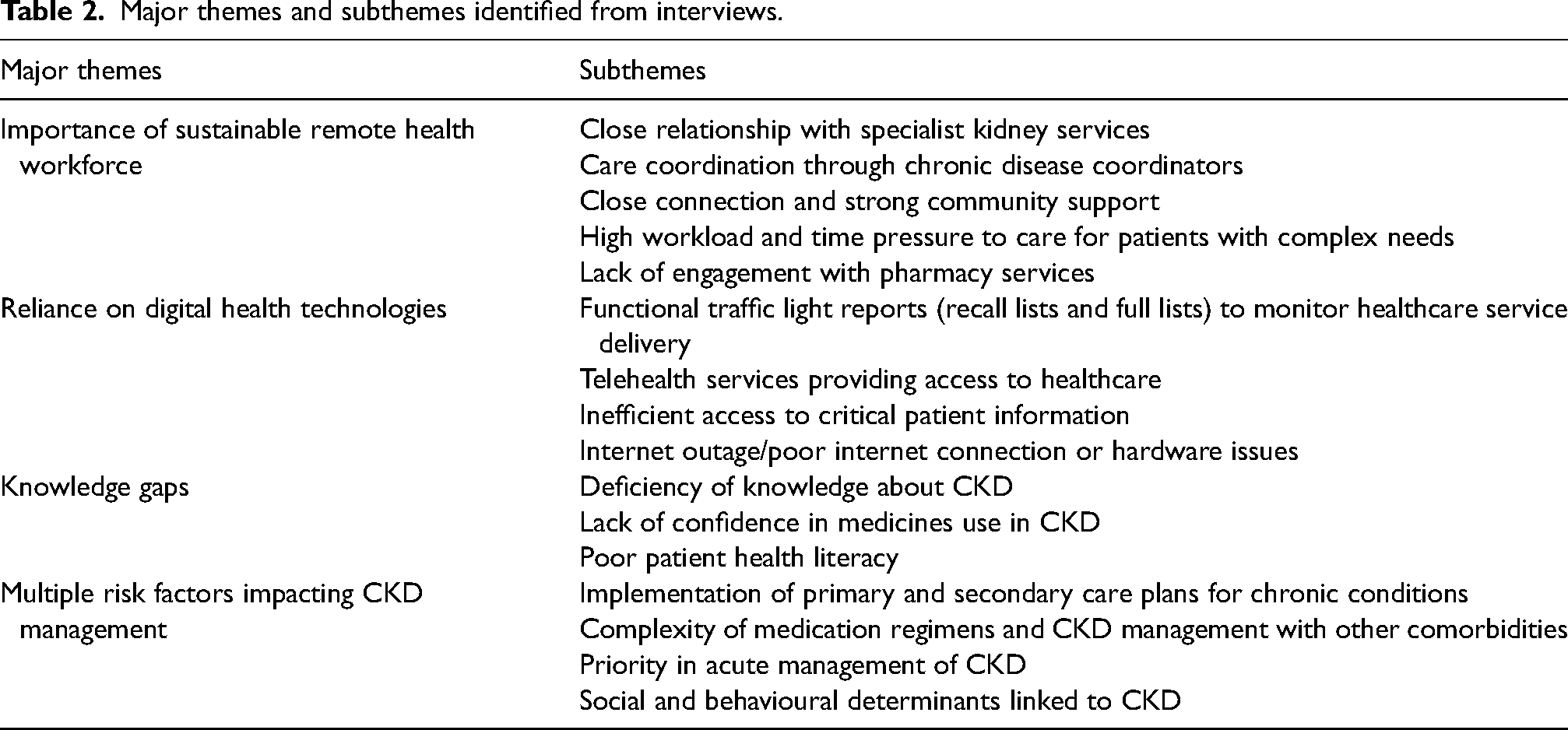
The thematic content analysis of interview transcripts identified four major themes: (1) the importance of a sustainable remote health workforce, (2) reliance on digital health technologies, (3) knowledge gaps, and (4) multiple risk factors impacting CKD management. The themes revealed both individual and systemic strengths and barriers surrounding CKD and medicines management in remote primary care. Emergent subthemes were grouped under relevant major themes (Table 2).
Major themes and subthemes identified from interviews.
Major theme 1: Importance of a sustainable remote health workforce
The participants described the importance of a sustainable health workforce on the impact of medication safety in remote primary healthcare. Five subthemes were identified from this major theme (Table 2):
Subtheme 1.1: Close relationship with specialist kidney services
Many participants expressed that they had a close relationship with specialist kidney services, which are based at the tertiary hospital within the Health Service. The service comprises kidney specialists who provide clinical care from acute to community-based care (urban or remote settings). The outpatient model of the service includes outreach services encompassing visits to remote communities and telehealth services. The participants explained that they often consult with the outreach team for specialty advice. Depends what situation is. If we can rectify it, here and now, see what's going on. Otherwise, I'd speak with the renal team because we have a good association with them, having so many renal patients here. (RMP3)
“So, declining renal function…we have a visiting physician and renal doctors that come out here quite regularly. So, if there's any concern, I'll refer to those. Also, usually through…if there's concern, I can call RDH [Royal Darwin Hospital]. There's an outreach renal reg [sic registrar] that you can always talk to. So, if I'm not sure, I'll always ring them and get advice from them as well. (RMP1)
Subtheme 1.2: Care coordination through chronic disease coordinators
The participants have also described the benefits of having an onsite chronic disease coordinator to provide patient education, medication management, and monitoring of symptoms to ensure optimal disease management. […] but on occasions, as I say, we're kind of aware who's at risk and who to watch out for. But that's, again, because we've got a back up of a really good chronic disease nurse. (RMP3)
Subtheme 1.3: Close connection and strong community support
In these discussions, the participants highlighted that they had strong community ties and social support. They reported that they knew their patients well and sometimes provided home visits, especially for those who missed their scheduled appointments. It depends on what the medications are. If it's something that the patient needs, like say it's a once weekly injection or something, then you'd know that they need it. So if they don’t come in then you'd go out and search for them. (RAN2)
We have a doctor twice a week. They [patients] will come back. They're not feeling the best anyway. There's lethargy involved…so, they're generally unwell. We would know them being in a small community. If they're that sick, we will do a DMO consult immediately. (RAN5)
Subtheme 1.4: High workload and time pressure to care for patients with complex needs
The participants cited time constraints due to workload pressures, which resulted in the delivery of shorter patient consultations. They discussed the lack of medical staff and increased demand for health services were difficult for RMPs to provide comprehensive medication reviews for complex patients with CKD. Distractions and interruptions to RMPs, by both staff members and patients, were revealed to be an impending cause for prescribing errors. I think the specific problems with prescribing with renal patients that do come up, you know, with this…hasn't been a timely review, and they need deprescribing because of weight loss or decline in eGFR. Issues do come up often enough, with changes (eGFR, weight, HbA1c, BP, food security, Hb) in CKD3b, 4, 5 patients, of which there are too many in this community. We are constantly stretched and it is easy for problems to ‘fall through the cracks’. (RMP2)
Subtheme 1.5: Lack of engagement with pharmacy services
A few clinicians described the lack of clarity on patient medication adherence. They reported the need for home medicine reviews (HMRs) to be conducted in the community to achieve quality use of medicines. Well, I don't know what they do when they get home because home medication reviews are not done and I think they should be done. So, we can only dispense from their sachet pack or blister pack, and hopefully they take them as well. (RAN5)
They also discussed that there was no communication with how patients were taking their medications and the reasons for nonadherence.
For us, I really want to know whether the person has been taking the medications or not […] yes, you can prescribe, but if you don't know the reason why they're not taking it […]. Maybe he doesn't even want to take it because it's too big, the tablet. Because not all patients will tell you. (PHA2)
During the interviews, it was discovered that there was a lack of awareness of services provided by the S100 pharmacists.
But if the patient comes in and says if they are on a higher dose, they'll come and say, ‘Oh, that's making me sick.’ And we send them back to the doctor and they'll lower the dose or put them on something else. Sometimes we call, the renal nurses […]. There's numbers there for special relocation. Can we call the pharmacist? (AHP4)
Out here, I've never really called the pharmacist to talk to them about doses because I think our CARPA protocol is [to do a] medical consult. (RAN4)
Major theme 2: Reliance on digital health technologies
Due to geographical remoteness and isolation, the clinicians discussed that they relied heavily on technologies to provide healthcare services. Four subthemes emerged under this theme (Table 2):
Subtheme 2.1: Functional traffic light reports (recall lists and full lists) to monitor healthcare service delivery
A networked electronic health record was used by the participants in the health centres, which generated regular reports including “recall lists” and “full lists” under the Chronic Conditions Management Model (CCMM) to ensure coordination of care for patients with chronic conditions including CKD. The “recall lists” allowed clinicians to follow up on episodes of care (e.g. regular health assessments and care plans). The “full lists” allowed clinicians to monitor chronic conditions management by detailing relevant information (e.g. care plan reviews, pathology results, and medication use). 19
Many participants discussed utilising these reports as an alert to monitor CKD progression. The daily recall, under the doctor thing. So what I do for our doctors because we don't have full time doctors. I print off two weeks so from today to two weeks ago, specifically Doctor Recalls and then that picks up anyone that's fallen off the system or while the doctors are away and up until today. If they miss out the week before on doctor day, at least we've got, we can pick it up two weeks after that. And that can come up as an alert. (RAN9)
So if someone came in, their eGFR dropped below 30 and that wasn't picked up by the doctor, we also get a traffic light report sent out to us on a monthly, and that will also say on it, ‘eGFR is below 30 but still on metformin’ or something so that is another trigger that I would see or if by chance, the patient came in for check-up and I check their last results and saw that they're still on metformin, I'll phone the doctor then and notify them. (RAN6)
Subtheme 2.2: Telehealth services providing access to healthcare
The participants discussed on utilising telehealth services especially in remote health centres that did not have residential medical staff. It was highlighted that RMPs would often be contacted to provide medical advice for patients seen in the health centres. Well, because we don’t have a GP every day, we only do on doctor days. Usually, I'll flick an email and give a call so that I can actually talk it through to our GP as well as my manager, and talk to the patient about what's happened, you know, these are the contributing factors, what's going on in their life, are they taking their medicines, not taking their meds – why not? How other things are going on, social stuff…funerals…left their meds behind…always a bunch of stuff, it's never one factor. (RAN8)
Subtheme 2.3: Inefficient access to critical patient information
The participants expressed frustrations for not being able to view critical health records quickly, which decreased workflow efficiency and increased the risk of prescribing errors. They highlighted their desire to have easier access to relevant patient information, such as patients’ most recent eGFR or blood pressure, and preferred for these to link to their medications during prescribing. I think just time wise, I think a lot of clinicians are frustrated with the current system. Like you can see how many clicks you need to do to get through something…recalls are…there's like 12 recalls on each patient already. And you're trying to do your job and it's very hard to engage with all of them. I think it would be great if there was something that just…rather than me having to like go look up a patient, go to Results, and then their latest renal function. Instead of having it on the Home Screen or […] where it had your latest eGFR, your latest blood pressure…and if that could talk to the medications that you're prescribing, I think it would be helpful because at the moment it relies on you knowing someone's on metformin…you might be in the clinic for one day every few months or going into another community where you don't know the person. So it takes a lot of mental space to know what people are on and know their renal function, and I think mistakes can be made. (RMP4)
It's hard for me to know which patient has renal impairment because we just receive scripts with…I mean there's no eGFR charted on the prescription itself. (PHA3)
Subtheme 2.4: Internet outage/poor internet connection or hardware issues
The participants required access to a reliable internet connection to provide health services, which presented a challenge during network outages or hardware failures. They reported having to re-enter patient information once they had access to better network services. However, care was still provided for patients that they were familiar with, without needing to refer to their health records. Slow internet. The doctors come out and they struggle to even do their notes. Sometimes they have to take their notes home because our computers are so slow because they can't keep up, it's just too slow. I do find it as a barrier. Sometimes, we have no internet for like three weeks. So we would just go back and document all three weeks’ worth. Like we just won't even see patients…that come in for their tablets, we would give [regular] people their tablets that we knew would need them or just people off the top of our heads that we knew ‘Ah, you need puffers’, we just hand it out. We are time poor, sometimes we get really busy. (RAN9)
Power dropouts, stuff like that…internet dropouts. Just being in remote, being a long way away from people. (RAN3)
Major theme 3: Knowledge gaps
The participants pointed out that there were knowledge deficiencies regarding the management of CKD, particularly with the safe use of medications, for both clinicians and patients. Three subthemes were identified under this major theme (Table 2).
Subtheme 3.1: Deficiency of knowledge about CKD
Some participants discussed that CKD management was not straightforward and that multiple factors affected the decision-making process, while others believed that clinicians with greater exposure to communities with a high prevalence of CKD were better equipped to identify potential interactions in patients with CKD. I think that renal disease is always a bit fluffy and management of renal conditions, and there were a lot of things that interplay into choices around dosing and while some medication decisions are really cut and dried. I think it would be really good for people to understand that there might be other reasons why choices are being made and to make sure they still use clinical judgment and are able to engage in discussions with prescribers from that perspective […]. (PHA4)
Like I said, there are people that just start here in remote. They don’t really know, they know the basics about renal disease. But when you've been working a while, you see the good and the bad interactions of renal impairment. (RAN5)
Subtheme 3.2: Lack of confidence in medicines use in CKD
Many participants expressed not feeling confident about medication use in patients with CKD and were often contacting their superiors or medical staff for support. I do look at their eGFR but I'll probably have to say I'll do a DMO consult and refer to the doctor like if I'm concern[ed] about if the medications are appropriate I'll talk to the doctor. (RAN4)
[I’d like to] learn more about their [patients] blood results, how to read them and what you can give them or how much. With the renal patients, we can't give them like a lot of ibuprofen or sometimes you can't give them any at all. So like stuff like that. (AHP3)
Subtheme 3.3: Poor patient health literacy
In these discussions, the participants described the struggles some patients experienced with reading medication labels that have resulted in poor adherence. They explained that patients often identified their medications based on physical characteristics such as pill colour. I know a lot of renal patients just have difficulty with reading. They read the medication but I find that a lot that medication colours are changed or renal patients just get confused. I've spoken to one of the pharmacists, I know everything change[s] a lot but I've spoken to someone to stop changing the colours because everyone get confused and they don't want to take it because the colour changed, the name is still the same but the colours, people like to see colours […]. (AHP2)
Major theme 4: Multiple risk factors impacting CKD management
The participants discussed that multiple factors influenced CKD management. Four subthemes emerged from this theme (Table 2):
Subtheme 4.1: Implementation of primary and secondary care plans for chronic conditions
The participants highlighted adopting care plans for assistance in the delivery of healthcare services for individual conditions (e.g. hypertension) or multiple conditions (e.g. hypertension and CKD). They discussed that these care plans involved multidisciplinary care to manage ongoing chronic conditions and ensure patients received relevant medical and pathology tests in a timely manner. Everyone should be on a care plan within community. So if you've got no comorbidities, you're on two-yearly health check. If you've got a risk factor, you go on annual review with risk factors, and a risk factor can just be smoking cigarettes. So, generally almost everybody is on an annual review and then you have your CKD 1–5 care plans, known to high CVR ± CKD ± diabetes and all those. So, depending on that care plan is how frequent they get recall, could be anywhere from six months to three months. (RAN9)
Subtheme 4.2: Complexity of medication regimens and CKD management with other comorbidities
The participants also described the challenges they encountered with polypharmacy in individuals with CKD, further complicated by other conditions such as hypertension and diabetes. They found it difficult to manage complex medication regimens, which were associated with potential drug interactions. […] because sometimes there are too many interactions… there is a lot… they are polypharmacy because most of the time you find that, these renal patients, they have got blood pressure, they've got diabetes, they've got renal…so, the polypharmacy…they've got a lot of medications. That's the only thing that I think, if to manage all these conditions that they have…is hard. I think that's the only thing, really, I see when I look at the renal patients. (RAN7)
Subtheme 4.3: Priority in the acute management of CKD
The clinicians discussed that they lacked time to review all health issues in a clinic visit. Priority was given to any “red flags” on pathology results or symptom-related patient presentation. The most common trigger was declining kidney function or acute kidney injury (AKI). Acute kidney injury…often that's not even with medications. I mean, it's dehydration, you know, someone comes in unwell. I usually make sure if there's a risk of renal function and if someone's dehydrated, we do a UEC [Urea, Electrolytes and Creatinine test] at that stage. So, we can see, and often we can pick up an acute kidney injury. Well, my concerns are that…we do see a lot of that. And so, it's not really a flag, unless we look at a patient clinically. So, I'm very unlikely to give NSAIDs if the patient's dehydrated and requiring…or if they're sick. (RMP3)
If I see something obvious in front of me, like say somebody is not on any renal medications and see a decline in their renal function, you would then refer them on to the GP or if something has changed or it's clear that the medications that they're on are not working for them anymore, then you would refer them for a medication review. (RAN2)
Subtheme 4.4: Social and behavioural determinants linked to CKD
The participants highlighted the contributing factors many patients exhibited that affected CKD progression. They expressed concern that there were social risk factors, such as food insecurity, and behavioural risk factors, such as high mobility, tobacco use, alcohol consumption, and poor diet, which affected treatment outcomes. The participants also discussed that CKD management was sometimes complicated by poor patient adherence to treatment and care. But chronic disease, CKD all that, there are three chances and then we'll try three times and then it's up to them to come in when they're ready. So say, somebody's due for their renal bloods, then today it would have come up on their Recall, they don't come in today, we'll try again tomorrow and we'll try again Thursday and if that's it, then they just pick it up the next time they come in. (RAN9)
Generally, if it's somebody that doesn't come in, you'd put in Recalls, saying their medications due or make sure patients get their medications every 2 weeks or whatever, so you note it so you don't forget. (RAN2)
Discussion
This research investigated the relationship between clinical workflows, health system priorities, cognitive tasks, and reasoning processes in the context of medicines used in people with CKD to identify opportunities for improvement with a CDSS. Exploration of the complex relationships between workflow, team interaction, and cognitive processes revealed gaps and opportunities that can benefit from decision support technologies. The interviews revealed positive connections and engagement between clinicians and community members, which is crucial for recognising patients at risk and ensuring active involvement in healthcare initiatives. However, participants also highlighted heavy workloads and knowledge gaps that have resulted in delays in conducting comprehensive medication reviews for patients with kidney disorders. Effective remote primary care for patients with CKD requires a multidisciplinary team approach, and digital technologies should complement, not replace, practice. The themes identified in this study showed that the use of a CDSS may be beneficial due to lack of staff retention (major theme 1), knowledge gaps (major theme 3), and the complex nature of CKD itself (major theme 4). Major theme 2 showed that clinicians are already utilising technologies to provide healthcare service delivery in clinical practice. Therefore, this study showed that implementing a medication-related CDSS into current electronic medical records could improve medical decisions without significantly impacting workflows (Figure 1).
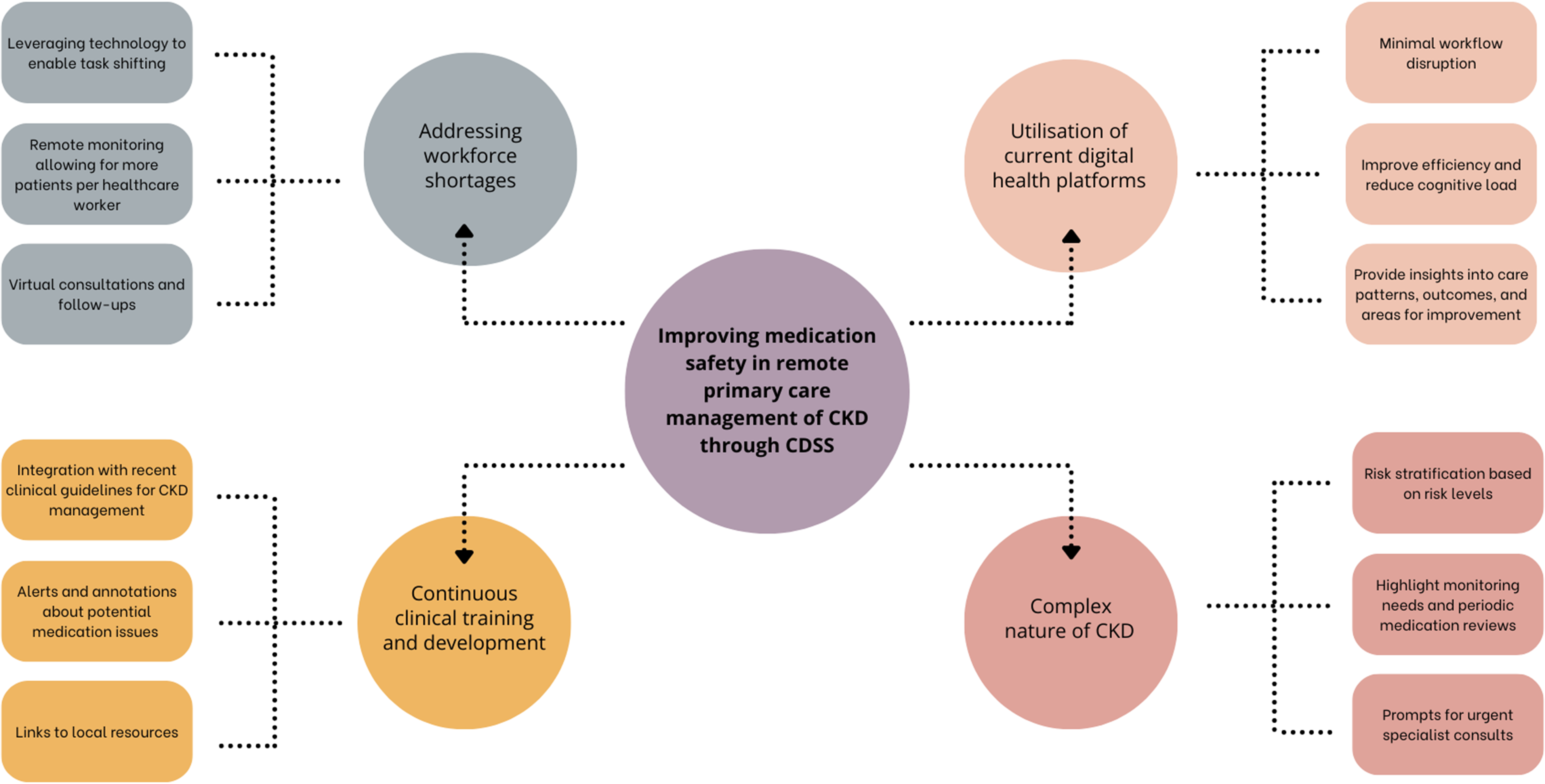
Improving medication safety in remote primary care management of CKD through CDSS.
Enablers to facilitate medication safety in CKD
There were several strengths within the current system highlighted by participants. Many participants reported having a close association with specialist kidney services, which were used as a referral point for kidney-related concerns. Strong collaborative care between primary care providers and kidney specialists has been shown to reduce the risk of complications and improve patient outcomes.20,21 The participants have also highlighted the advantages of chronic disease coordinators within primary care settings, which have been shown to improve chronic disease management.22–25 They work closely with other healthcare providers to ensure coordination of care, prevent medication errors, and reduce healthcare costs, especially for patients with CKD who often require ongoing care and support.
Participants also discussed that they had developed and maintained rapport with their patients. They were more likely to be familiar with their patients’ medications and medical history, which enabled active follow-up with patients who missed appointments or did not follow through on recommended care. Moreover, AHPs played a crucial role in delivering culturally safe healthcare, which increased patient trust and engagement, particularly for those who may otherwise not seek care due to cultural and social beliefs. Multiple studies have shown the need for AHPs or Aboriginal health workers (AHWs) to work in partnership with patients and non-Indigenous health professionals to facilitate better access to health services and treatment acceptance in the community.26,27
Digitally enabled models of care for remote communities have also improved processes for clinicians to deliver health services efficiently. The CCMM, which was developed and built into the electronic medical record, enabled patients to receive appropriate and timely care, even if they were in a remote location. This included functional traffic light reports and care plans for individual and combined chronic diseases. This model, using technology, streamlined communication, reduced administrative burden, and improved access to patient information, which allowed clinicians to monitor process and outcome measures and take actions to ensure better patient outcomes.
Key issues and digital solutions to improve medication safety in CKD
The participants also underlined numerous challenges during these discussions. They reported staff shortages and low workforce retention, which resulted in increased workload pressure. It was also revealed that there was a lack of awareness of services provided by pharmacists, which resulted in poor access to pharmacist advice and medication management reviews. RANs and AHPs may have been trained to rely primarily on medical staff for medication information, rather than pharmacists, due to limited accessibility. Increasing the use of telepharmacy services may be an effective strategy to address this issue in remote areas, where there is a lack of onsite pharmacists. 28 Medication reviews and counselling with patients through telepharmacy may help ensure patients receive proper management of their medications and bridge the gap in access to pharmacy services in remote areas.29–31 The current HMR model in Australia may also not be financially viable and sustainable. It impacts credentialed pharmacists to effectively service remote communities due to limited funding and reimbursement options for travel expenses, accommodation, and time commitments.
Clinicians have expressed knowledge gaps as a barrier to optimal medication management surrounding CKD and the need for education programmes for primary care providers in delivering health promotion, disease prevention, and treatment. The participants also reported the complexities in managing polypharmacy in patients with CKD and other comorbid conditions, which can increase the risk of medication-related complications. Perceived poor medication adherence among people living in remote communities was also reported to be a challenge, which may be due to low health literacy, 32 language barriers,33,34 or cross-cultural misunderstandings in healthcare.35–37
During these interviews, the participants highlighted that inefficient access to critical patient information was a barrier to providing effective and efficient care for patients. Several clinicians described needing to navigate through multiple screens or complete numerous steps in order to access relevant information. Moreover, information silos that exist across different service providers, particularly in remote areas where prescribers are geographically distant from pharmacies, were highlighted as an issue. Patient laboratory results (e.g. eGFR) were not commonly included in prescriptions, and pharmacists were required to obtain these values from a different system to the dispensing software, which significantly impacted workflow. Hence, pharmacists may not be aware of a change in a patient's kidney function which may lead to potential dispensing errors. Additionally, a few participants underlined that their communities had poor broadband connectivity. The inequitable access to internet connectivity may hinder timely access to vital patient information and remote consultations, potentially affecting patient health outcomes.38–40
Limitations and future approaches
This study had a small sample size and was limited to one geographic region in Northern Australia. There was more participation from RANs and AHPs than RMPs and pharmacists; however, this was reflective of the higher proportion of these professions in the remote workforce. Recruitment of RMPs and pharmacists was challenging due to time constraints and lack of availability. Moreover, this study only focused on government-run remote primary health centres. Therefore, these findings may not be generalisable to non-governmental organisations. Our results suggest that interventions aimed at improving the flow of information between different healthcare providers are particularly important in remote health settings where communication and coordination between providers are more challenging due to geographic distance and limited resources. CDSS implementation may be an effective approach by providing relevant information at the point of care, especially for complex patients such as those with CKD. Studies have shown that CDSSs may have potential by providing real-time recommendations for medication selections and dosage adjustments based on patients’ kidney function. 41 However, careful execution is required to ensure minimal workflow interference and alert fatigue.42,43 Future research could benefit from investigating how CDSS can be better integrated across different health platforms to facilitate seamless sharing and utilisation of real-time patient data in diverse healthcare settings. More studies are also required to explore how healthcare professionals engage with CDSSs, with an emphasis on enhancing the user interface's usability, which could reduce the potential for user error.
Conclusion
Due to the high prevalence of CKD, a decentralised clinical workforce, and reliance on digital health systems in day-to-day care clinical service practices, interoperability of a CDSS with existing electronic systems may be beneficial in improving medication management for patients with CKD in remote primary care. The findings from this study will facilitate the integration of workflow considerations into the design and implementation of a medication-related CDSS to improve prescribing and dispensing practices for patients with kidney impairment.
Footnotes
Acknowledgements
The authors would like to thank all RMPs, AHPs, RANs, and pharmacists who generously gave up their time to participate in this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethics approval was granted by the Human Research Ethics Committee of the NT Department of Health and Menzies School of Health Research (HREC 2022–4403). Governance approval was granted from each study site (EFILE 2022/22911).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Digital Health CRC Limited (“DHCRC”). DHCRC is funded under the Australian Commonwealth's Cooperative Research Centres (CRC) Program. Work undertaken by S.E.R. is with the financial support of the Cancer Council's Beat Cancer Project on behalf of its donors, the State Government through the Department of Health, and the Australian Government through the Medical Research Future Fund.
Data availability statement
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.