
Abstract
This study investigates the outcomes of virtual nutritional counseling (VNC) for oncology patients during the Covid-19 pandemic. Our study evaluated the nutritional status data of cancer patients at the baseline and after VNC. An oncology dietitian evaluated the patients by video calling each patient via WhatsApp and sent an individual nutrition diet plan and recommendations via e-mail. Patient-Generated Subjective Global Assessment (PG-SGA) was used as a screening and evaluation tool to assess nutritional status. A total of 157 patients with a mean age of 55.8 ± 14.7 (r = 19–89) were included in the study. Researchers detected at least one nutrition-related sign in 77.7% of patients. After the VNC and based on the final PG-SGA assessments, 62.2% of the patients whose baseline PG-SGA Score-B improved to Score-A, 12.5% with a baseline PG-SGA Score-C improved to Score-A and 54.2% with a baseline Score-C improved to a Score
Introduction
The Covid-19 pandemic had significant implications on the cancer care spectrum for oncology patients at higher risk of morbidity and mortality than the average population. In addition, the expansion of telehealth services, defined as virtual visits with a healthcare professional, caused a paradigm shift in healthcare, including the realm of nutritional diet consultations, which are an integral part of cancer treatment. 1
Telehealth has not reached its full potential due to various barriers such as infrastructure and reimbursement issues, resistance to change, and patient-specific factors such as, but not limited to, user age, education level, and computer literacy.2,3,4 Furthermore, the COVID-19 pandemic highlighted the benefits of telehealth specifically for rural, immobile, and immunocompromised patient populations.5,6 As cancer patients are more susceptible to viral infections due to their immunosuppressive state, dietitians offer medical nutrition therapy to minimize physical contact with patients and mitigate risks during the pandemic. In addition, existing evidence suggests that while telehealth is not an all-encompassing solution, it is proven effective when cancer patients’ access to health care for diagnostics and treatment services is disrupted. 6
Along with ongoing cancer treatments, individual nutritional counseling plays a vital role in managing an oncology patient as a supportive treatment. According to the ESMO clinical practice guidelines published in 2021, the provision of Oral Nutritional Supplementation (ONS) without dietary counseling is inadequate. ESMO advises using ONS along with nutritional diet support under the care and supervision of a professional dietitian. 7
Timely nutritional-behavior change interventions lead to a survival advantage for patients. Thanks to multidisciplinary approaches and recent advancements in oncology treatments, the five-year survival rate for all cancers has increased to approximately 68% in the last decade. 8
The American Cancer Society's nutritional guidelines emphasize the positive association between nutrition awareness and cancer survival. 9 Similarly, The European Society of Clinical Nutrition and Metabolism (ESPEN) guidelines and the American Society for Parenteral and Enteral Nutrition (ASPEN) oncology guidelines highlight the importance of screening for malnutrition and including nutritional interventions in the nutritional care plan for cancer patients.10,11,12,13
Although there are various tests to evaluate the nutritional status of cancer patients, the gold standard test in the evaluation of malnutrition is PG-SGA, which was initially developed by Ottrey et al. in 1995. The PG-SGA consists of information about weight, height, food intake, gastrointestinal symptoms, functional capacity, physical exploration, and the presence of ascites and edema. 14
While telehealth offers a unique opportunity to continue patient care during the Covid-19 pandemic and beyond, there is limited data regarding patients’ interest and ability to participate in telehealth and the impact of telehealth-based nutritional counseling interventions on cancer treatment. This study aims to evaluate the nutritional status improvement in cancer patients who received VNC during the COVID-19 pandemic.
Methods
This descriptive, retrospective study included a convenience sample of 157 cancer patients treated at Acibadem Hospital who received VNC from the same experienced dietitian between April 2020 and March 2022. The same experienced oncology dietitian conducted VNC via video WhatsApp calls to minimize intra-rater reliability. The duration of the first visit was 45 minutes, and the follow-up sessions were scheduled for 30 minutes each. However, we did not limit the number of follow-up sessions. The patients were followed through the VNC program as long as they requested to participate.
The same experienced dietitian discussed the individual nutritional diet plan and recommendations with the patients during the video calls and provided all the information in writing via e-mail after the virtual visit. The content of the diet plan (energy, protein and macro and micro nutrients requirement) was planned in accordance with the recommendations of ESPEN, ASPEN, and ESMO oncology guidelines and American Academy of Nutrition and Dietetics oncology group.
Data collected includes demographic data, patient's comorbidities, body mass index (BMI), reasons for applying to VNC, symptoms at the time of admission, weight loss in kilograms over the last six months, tumor localization and stage, type of cancer treatment, ONS support, and PG-SGA score at baseline and final visit.
The frequency of the sessions was determined according to the nutritional status of patients that were evaluated by dietitian. Patients with malnutrition and multiple nutrition-related side effects were seen at intervals of 10–15 days. But on the other hand, some patients voluntarily terminated the interviews after the first or second session.
Researchers retrospectively evaluated VNC patient outcome data from the hospital's patient registry system (Cerebral). Patients who received enteral and parenteral nutrition, pediatric patients, and those without an official cancer diagnosis were excluded from the study. Acibadem University approved the study, School of Medicine Ethics Committee ATADEK (decision number 2022-08/24). Data were analyzed using SPSS Statistics for Windows, Version 25.0 (IBM Corp., Armonk, NY, USA).
In addition to descriptive statistics (number, percentage, mean, standard deviation, etc.), Pearson Chi-Square with continuity correction and Fisher's Exact Test were used to test associations between categorical variables and to make qualitative comparisons among groups.
McNemar test was used to test the difference in repeated measurements of qualitative data. In addition, multiple Logistic regression analysis helped determine independent factors associated with the presence of malnutrition in patients, and Multinomial Logistic regression analysis was used to determine independent factors associated with weight change in patients. The results were evaluated at the 95% confidence interval and the significance level of P < 0.05.
Results
Among the participants, the median age was 55.8 ± 14.7 years (19 to 89 years), and 67.5% were female. According to their BMI scores, 11.5% (n = 18) were in the underweight, 47.8% (n = 75) normal, 26.8% (n = 42) overweight and 14% (n = 22) were in the obese categories.
The primary cancer site distribution is summarized as the following: Non Colorectal Gastrointestinal System Cancer (NCRGIS) in 44 patients (28%), breast in 38 patients (24.2%), lung in 19 patients (12.1%), colorectal in 13 patients (8.3%), head and neck in 14 patients (8.9%), and other locations in 29 patients (18.5%). Among the participants, 45.2% had metastatic cancer at admission, and 41.4% presented with comorbidities. At least one nutrition-related symptom was observed in 77.7% of the patients. The most common symptoms were loss of appetite, constipation, diarrhea, and nausea. The most frequent reason for admission to the VNC program was an issue with weight change during treatment experienced by 53.8% of the patients, followed by 39.5% of patients who needed nutritional support during their chemotherapy or radiotherapy regimen and 5.1% who requested general nutritional support.
During the initial VNC patient intake and evaluation, we determined that 56.1% of the patients experienced weight loss, whereas 19.1% had weight gain. Twenty-one percent of the patients received one session, 43.3% received two, and 35.7% received three or more sessions of nutritional counseling (Table 1).
Nutrition-related characteristics of patients at baseline (before VNC) (n = 157).
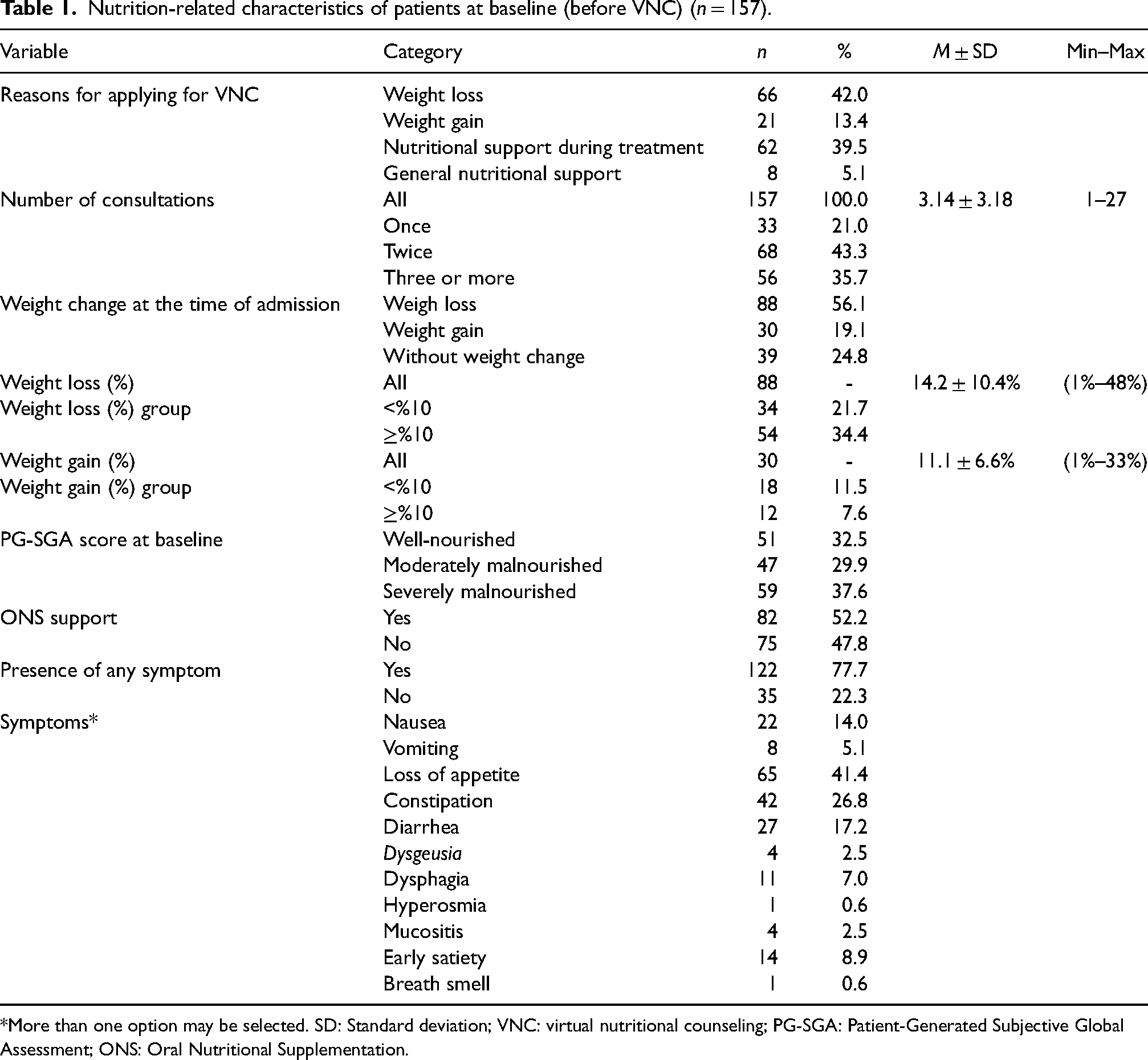
*More than one option may be selected. SD: Standard deviation; VNC: virtual nutritional counseling; PG-SGA: Patient-Generated Subjective Global Assessment; ONS: Oral Nutritional Supplementation.
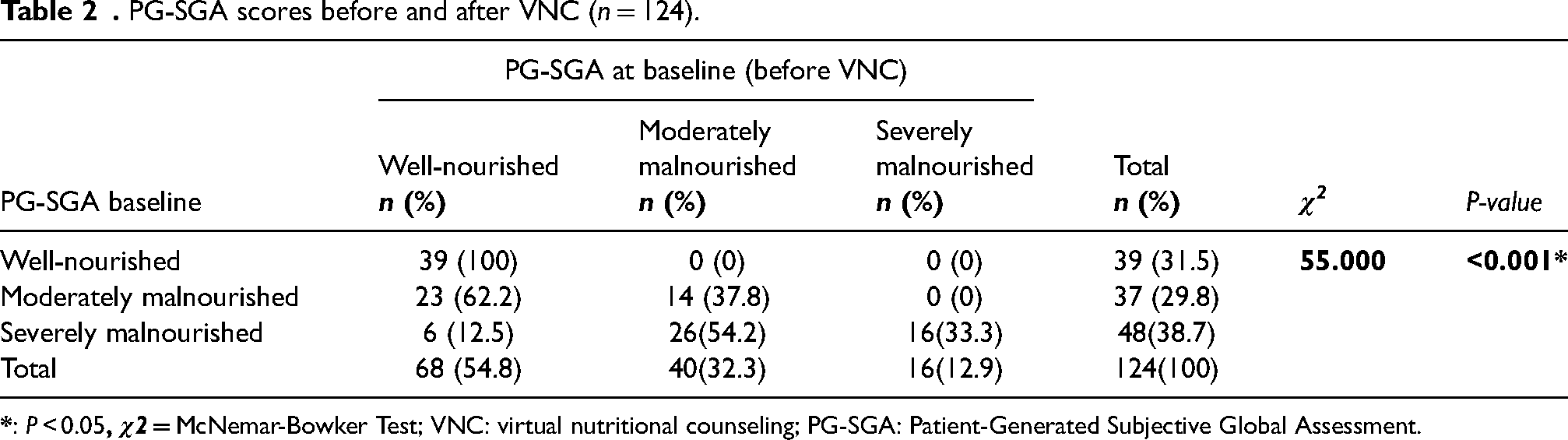
Before VNC, patients were grouped based on their PG-SGA scores: 39 patients (31.5%) were in the well-nourished (PG-SGA-A) group, 37 patients (29.8%) in the moderately malnourished (PG-SGA-B) group and 48 patients (38%) were categorized in the severely malnourished (PG-SGA-C) group.
Based on the comparative analysis performed on 124 patients who had two or more sessions, we did not observe any changes in the nutritional assessment score of 39 patients who were well-nourished before and after the VNC. According to the PG-SGA scores, after the VNC, 62.2% (n = 23) of 37 patients with moderate malnutrition improved to the well-nourished category, and 12.5% (n = 6) of 48 patients with severely malnourished improved to the well-nourished group and 54.2% (n = 26) improved to the moderately malnourished group (χ2 = 55,000, P < 0.001) (Table 2).
When we excluded patients with an initial PG-SGA score of A (n = 39), malnutrition scores for the rest of the patients (n = 85) whose initial scores were B and C improved (P < 0.001) after VNC.
We observed a statistically significant difference in malnutrition before and after VNC based on the patient's age, BMI, primary cancer site, metastasis, comorbidity, radiotherapy, and hormone therapy status (P < 0.05) (see Table 3). The presence of severely or moderately malnourished was statistically significantly higher in patients over 60 years of age, with normal or low BMI, tumor localization in the lower and upper GIS, metastatic cancer, comorbidities, and absence of radiotherapy and hormone therapy treatment (P < 0.05) (Table 3).
Presence of malnutrition before and after VNC according to patient characteristics.
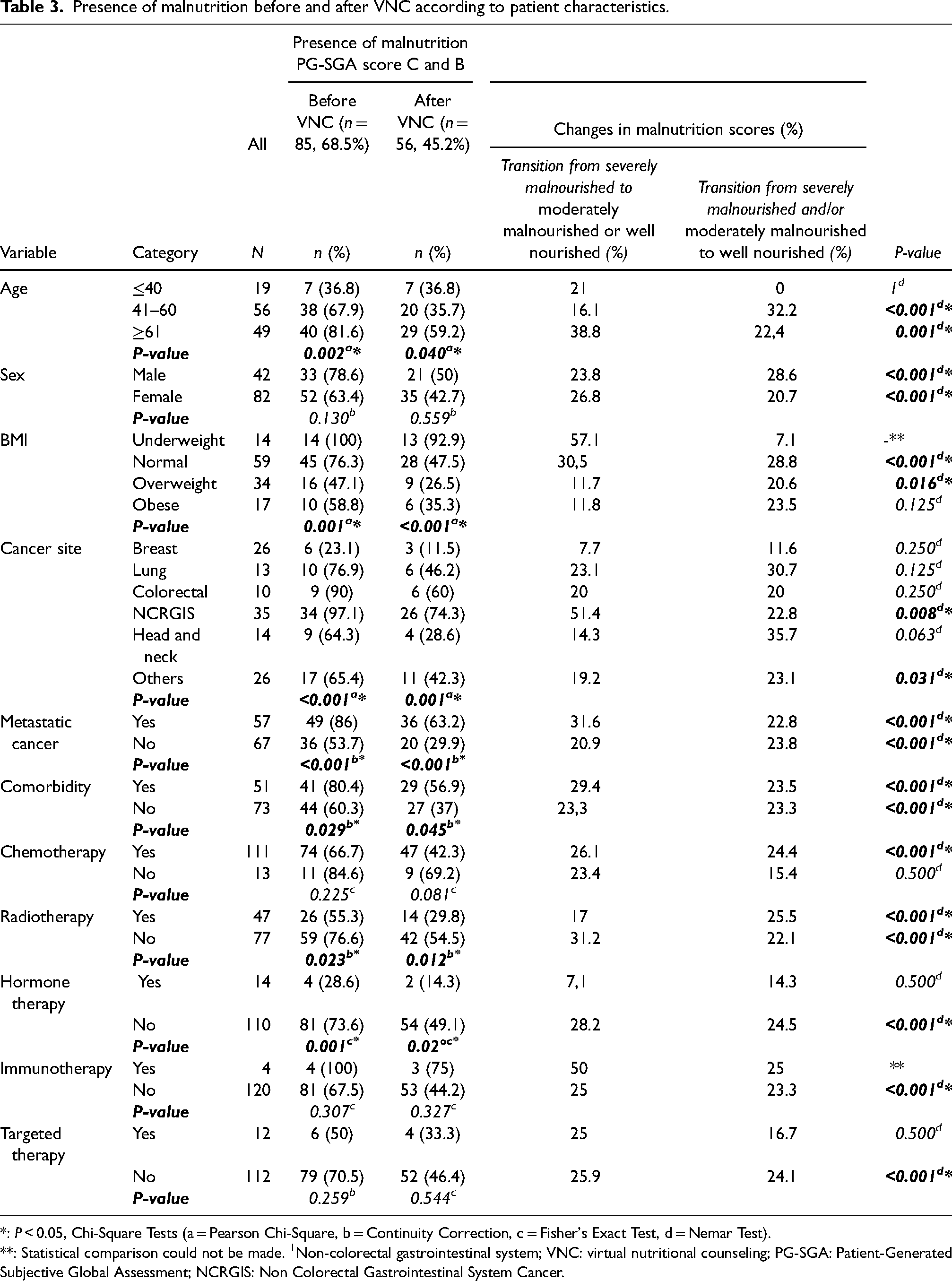
*: P < 0.05, Chi-Square Tests (a = Pearson Chi-Square, b = Continuity Correction, c = Fisher's Exact Test, d = Nemar Test).
**: Statistical comparison could not be made. 1Non-colorectal gastrointestinal system; VNC: virtual nutritional counseling; PG-SGA: Patient-Generated Subjective Global Assessment; NCRGIS: Non Colorectal Gastrointestinal System Cancer.
Presence of Malnutrition Before and After VNC According to Nutrition-Related Characteristics of Patients.
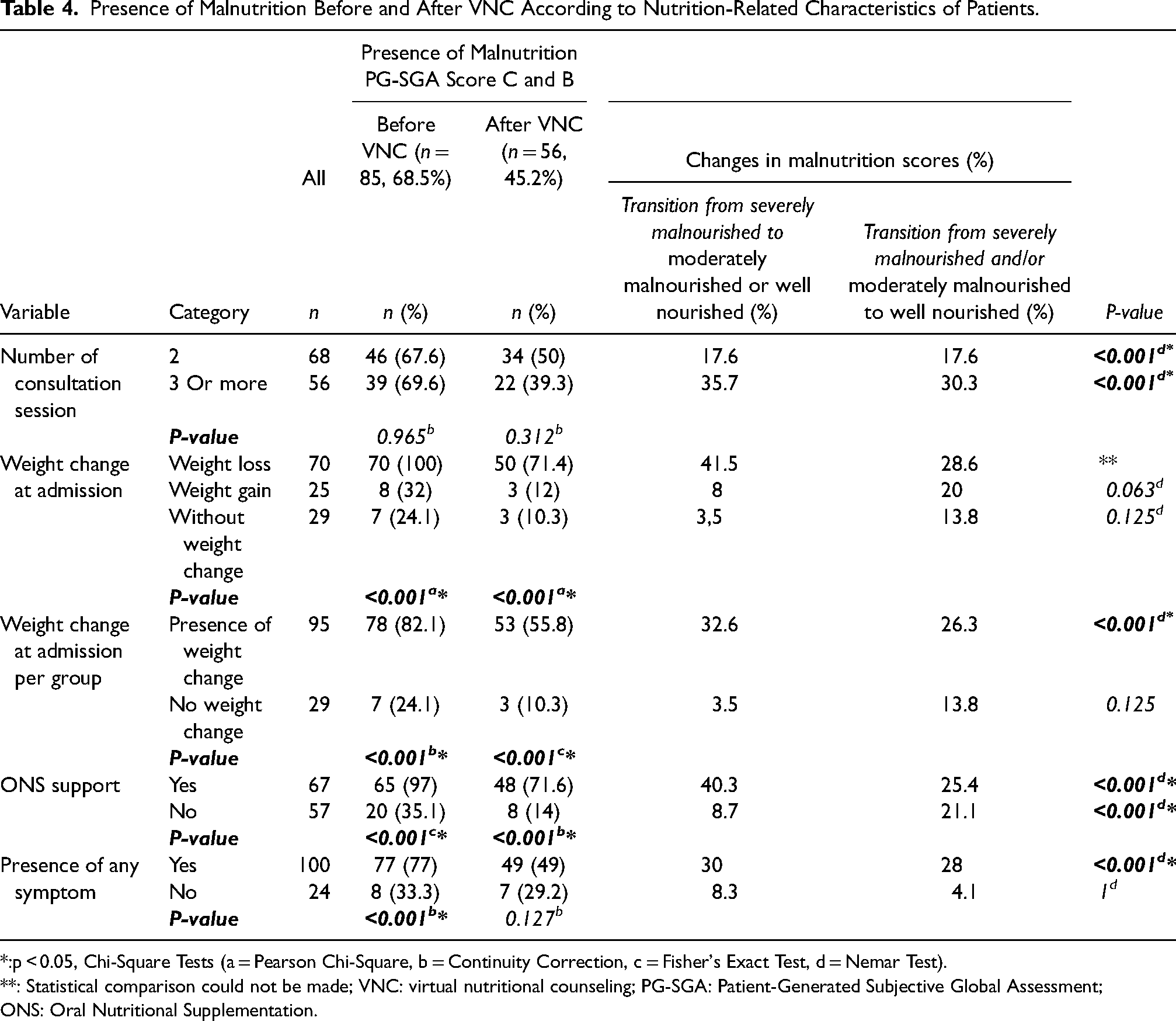
*:p < 0.05, Chi-Square Tests (a = Pearson Chi-Square, b = Continuity Correction, c = Fisher's Exact Test, d = Nemar Test).
**: Statistical comparison could not be made; VNC: virtual nutritional counseling; PG-SGA: Patient-Generated Subjective Global Assessment; ONS: Oral Nutritional Supplementation.
The highest rate of change from severely malnourished to moderately or well-nourished group after VNC was within the NCRGIS patients, whose rate of improvement in nutritional status was 51.4% (P = 0.008). After VNC, 31.6% of patients with metastasis categorized in the severely malnourished group improved to moderately malnourished or well-nourished, and the results were statistically significant (P < 0.001).
We determined that 30.5% of the patients who were severely malnourished at admission in the normal BMI category improved to the moderately malnourished or well-nourished category. In addition, 28.8% of the patients who were moderately and severely malnourished at admission who were in the normal BMI category improved to the well-nourished class after VNC. The results were statistically significant (P < 0.001). The rate of transition to moderately malnourished and well-nourished among patients who were severely malnourished and who received chemotherapy was determined to be 26.1%, and the difference was statistically significant (P < 0.001). All patients who reported weight loss at admission were categorized as category C or B according to their PG-SGA assessment. At the time of entry, 42 patients had more than 10% weight loss, and 28 patients had less than 10% weight loss.
The presence of severely or moderately malnourished patients was statistically significantly higher in patients with weight change at admission, those who received ONS support, and those who presented with symptoms (P < 0.05). When evaluated according to the number of VNC sessions, there was a 17.6% improvement in the presence of severely and moderately malnourished patients who received two VNC sessions. In patients who received three or more sessions, the transition rate from severely malnourished to the moderately malnourished or well-nourished category was 35.7%, and the rate of improvement from moderately and severely malnourished to the well-nourished category was 30.3% (P < 0.001).
The counseling program's median length was 21 (7–728) days. The median program length for those whose PG-SGA scores did not change after VNC was 18 days (7–728) for those in the well-nourished, 18.5 days (7–340) in the moderately malnourished group, and 16 (8–286) days in the severely malnourished group, respectively. The median online counseling length for patients whose initial PG-SGA score C (n = 32) improved to A (n = 6, 4.8%) and B (n = 26, 21%) after VNC was 123 days (31–567) and 26.5 days (9–270), respectively. The median online counseling length for those with an initial PG SGA score of B (n = 23) that improved to A (n = 23, 18.5%) after counseling was 30 (7–585) days. The group with the highest median length of counseling had an initial PG-SGA score of C (severely malnourished), which improved to score A after VNC.
The rate of transition from severely malnourished to moderately malnourished or well-nourished category was 40.3% and from moderately and severely malnourished to well-nourished was 25.4% in patients who received ONS support. The results were statistically significant (P < 0.001).
The transition rate from severely malnourished to the moderately malnourished or well-nourished category was 30% in patients with any nutrition-related symptoms. When the moderately and severely malnourished groups were evaluated together, we found the transition to the well-nourished category to be 28% of patients with any nutrition-related symptoms. The results were evaluated as statistically significant (P < 0.001; Table 4).
Based on the multiple logistic regression analysis, the independent factors that increase the presence of malnutrition in patients were determined from the available data: BMI (OR = 0.83, CI = 0.71–0.97, P = 0.016), cancer localization in a site other than breast (OR = 19.40, CI = 1.92–196.52, P = 0.012), presence of metastatic cancer (OR = 11.80, CI = 1.76–78.95, P = 0.011), weight change at the time of admission (OR = 64.57, CI = 8.08–516.02, P≤0.001) and the presence of any nutrition-related symptom (OR = 35.40, 4.19–299.37, P = 0.001) (Table 5).
Independent factors associated with the presence of malnutrition before VNC (multivariate logistic regression analysis results).
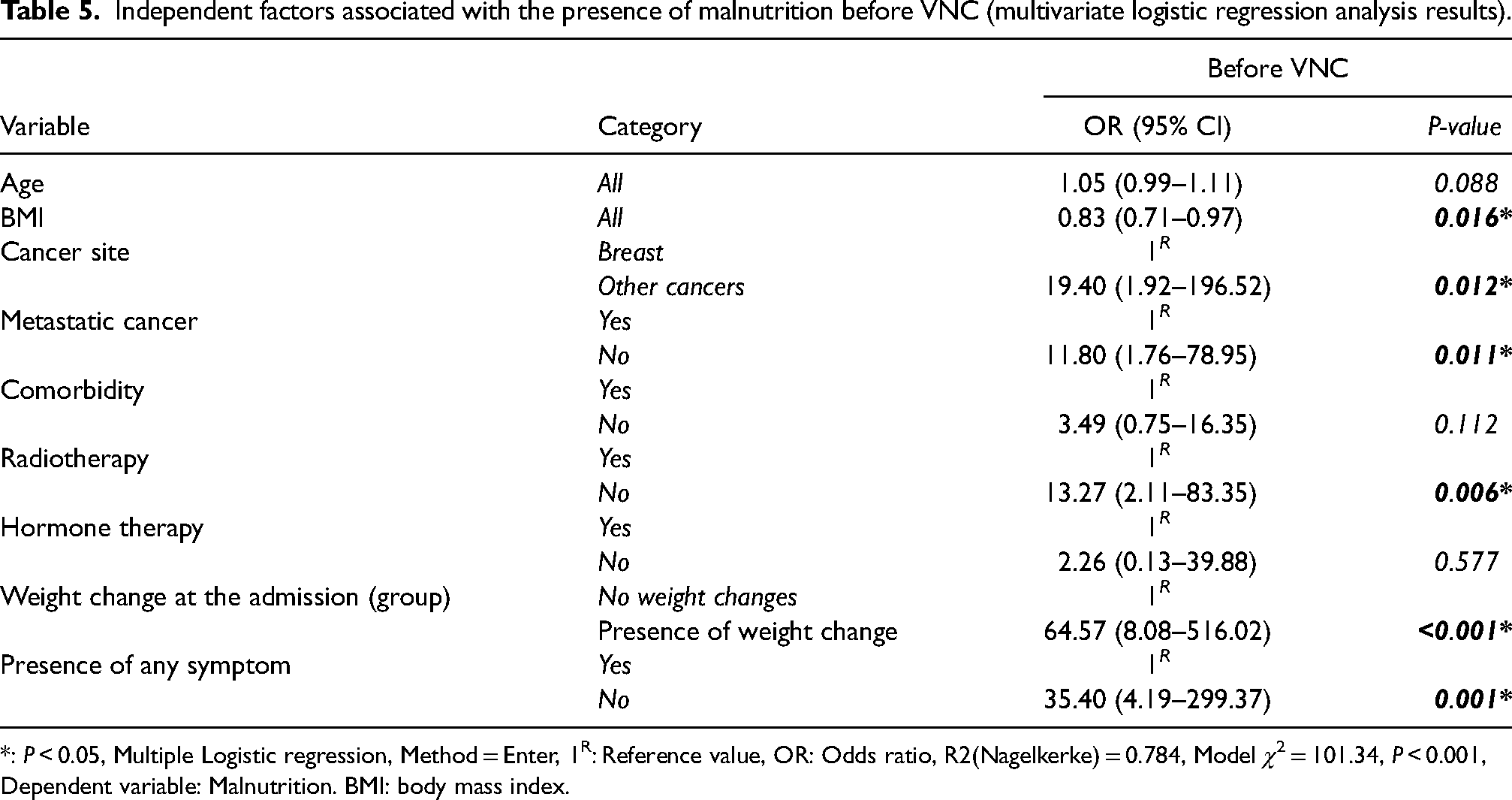
*: P < 0.05, Multiple Logistic regression, Method = Enter, 1R: Reference value, OR: Odds ratio, R2(Nagelkerke) = 0.784, Model χ2 = 101.34, P < 0.001, Dependent variable: Malnutrition. BMI: body mass index.
In patients without weight change at admission, the factors that increased weight loss were the GIS tumor site (OR = 12.27, CI = 1.36–110.83, P = 0.026) and the presence of symptoms (OR = 26.42, CI = 5.48–127.46, P < 0.001).
When weight loss is evaluated according to tumor localization, the risk of weight loss are 12.3 times higher in the GIS cancer group compared to the breast cancer group. The development of nutrition-related symptoms increased the odds of weight loss up to 26.4 times compared to the group of patients who did not experience any symptoms (Table 6).
Independent factors associated with weight change.
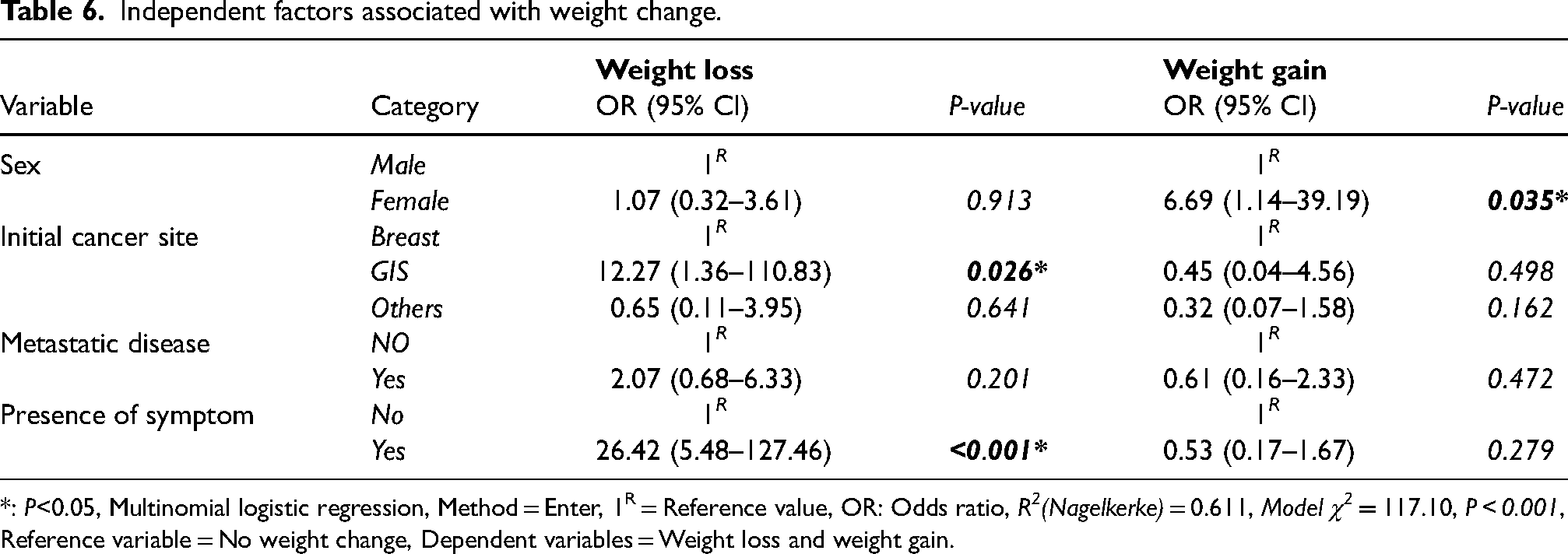
*: P<0.05, Multinomial logistic regression, Method = Enter, 1R = Reference value, OR: Odds ratio, R2(Nagelkerke) = 0.611, Model χ2 = 117.10, P < 0.001, Reference variable = No weight change, Dependent variables = Weight loss and weight gain.
When there was no weight change at admission, the female gender was linked to weight gain (OR = 6.69, CI = 1.14–39.19, P = 0.035). We determined that being of female gender increased the risk of weight gain 6.7 times compared to male gender (Table 6).
Discussion
Pandemics present challenges to healthcare delivery. Though telehealth will not solve all the challenges faced during this time, it facilitates increased access to health care. 15 A systematic review evaluating the importance of telehealth and nutritional support in the first year of the Covid-19 pandemic investigated dietitians’ use of telehealth services and barriers to implementation. The review argues that telehealth will not only keep patients and healthcare providers safe but will also allow continuity in health care. In certain situations, telehealth can improve health care delivery beyond the standard of care. 16 The same article states, “Perhaps one of the most intuitive first steps in using telehealth are to transform existing outpatient one-on-one visits to telehealth visits with a registered dietitian nutritionist.” Several studies exploring telehealth's impact on chronic disease management found that nutrition-related interventions were successful.17,18,19
World Health Organization and the American Telemedicine Association define telehealth (or telemedicine) as the use of electronic communication and information technologies in the remote delivery of clinical services.16,20 Tele-oncology is the application of telemedicine to oncology to improve cancer treatment. 21 Cancer patients are immuno-compromised, and this population's early recognition of nutritional problems is the primary driver of appropriate dietary management. Timely nutritional-behavioral interventions positively affect prognosis. The malnutrition accompanying cancer has well-known adverse effects related to toxicity and response to cancer treatment, quality of life, and prognosis. 22
A recent review reported that during the pre-COVID-19 pandemic, a nutritional assessment was provided to only 30 to 70% of cancer patients at risk of malnutrition, and roughly half of those who underwent nutritional examination obtained the appropriate level of nutritional support. 23
Although VNC has become popular in certain countries during the pandemic, it is not used routinely in most parts of the world due to issues with access to technology. 24 The difficulty in accessing healthcare during the quarantine period led to the expanded use of virtual services, including nutritional consultations by dietitians for oncology patients. Several studies highlight the contributions of VNC to proper patient management.25,26
To our knowledge, our study is the first in the literature to explore the effects of VNC in the nutritional evaluation of cancer patients. Our results illustrated a statistically significant improvement in malnutrition scores of patients after VNC. As highlighted in ESPEN, ASPEN, and ESMO oncology and nutrition guidelines, individual nutritional counseling and nutritional follow-up of oncology patients are essential steps to increase the success in the treatment of malnutrition.7,10,11,12,13
Each follow-up visit lasted up to 45 minutes including intake, evaluation of nutritional status, creation of an individual nutrition plan, and a nutritional education held via WhatsApp with the participation of the oncology dietitian, the patient, and the patient's relatives. The dietitian shares an individual nutrition plan and recommendations with each patient via e-mail and answered questions via WhatsApp in between sessions, which were carried at 1-, 2- or 3-week intervals.
A dietitian conducted all virtual visits via secure and encrypted WhatsApp video calls. WhatsApp is a free mobile application that contributes to approximately 20% of the time spent on smartphones. 27 Instant messaging systems facilitate effective communication among patients, caregivers, and clinicians, providing an enhanced care experience. 28 However, more studies are needed to assess the effectiveness of instant messaging in oncology care, and our study may be able to fill this gap.
Several studies conducted on web-based and WhatsApp platforms support our findings. For example, a scoping review in Indonesia that investigated the use of mobile apps in the management of palliative care at home reported that mobile apps could improve care delivery, primarily by increasing the knowledge of the patient's caregivers. 29 A Canadian descriptive, exploratory, proof-of-concept study that evaluates the effectiveness of telehealth in guiding caregivers and nurses in providing palliative care to people with cancer in rural and remote areas 30 confirms the above findings. Finally, in a study with 212 patients, researchers demonstrated that WhatsApp was successfully used in remote hematuria assessment and reduced unnecessary service costs within cases of mild clinical significance. 31
In addition, Snoswell et al. 32 reported that “The clinical effectiveness of telehealth seems apparent for clinical services such as stroke management, blood pressure control, mental health support, pain management, blood glucose reduction and diagnostic services involving dermatological (skin cancer) and ophthalmic (glaucoma) conditions.”
In our study, 59.1% of cancer patients who applied for VNC reported weight loss at admission. Weight loss is one of the most common symptoms in cancer patients. In 2011, Fearon et al. suggested using weight loss percentage to develop the most accepted framework for diagnosing cancer cachexia. 33 Similarly, the Global Leadership Initiative on Malnutrition (GLIM) evaluates nutritional status based on the percentage of weight loss as a determining criterion for the severity of malnutrition. 34 Newer evaluation criteria also advise the addition of direct muscle mass measurement, as cancer cachexia may co-occur with obesity, edema, and large tumors may mask weight loss. 35
In a virtual assessment, it is possible to monitor weight changes, the percentage of weight loss, and calf circumference. In addition, VNC leverages a validated nutritional assessment tool such as PG-SGA to evaluate nutritional status. However, VNC also presents weaknesses: one cannot use Bioelectrical Impedance Analysis to monitor body composition or measurements such as skinfold thickness or hand grip strength.
Our multiple logistic regression analysis showed that the factors that affected weight loss were the tumor location in the gastrointestinal system and the development of nutrition-related symptoms. In the literature, cachexia varies according to tumor type, with incidence over 80% in gastric or pancreatic cancers; approximately in half of the patients with lung, prostate, or colon cancer, and about 40% of patients with breast, advanced head, and neck cancers and certain leukemias. 35
According to our multiple regression analysis, BMI, cancer localization in a site other than the breast, metastatic cancer, weight change at admission, and any nutrition-related symptoms appeared as independent factors that increased the risk of malnutrition. Cancer cachexia evaluation criteria and current literature support our data.7,10,32,33,35 Our results also showed that the risk of weight loss increased 12.3 times in patients with GIS tumors. Nausea, vomiting, diarrhea, constipation, and loss of appetite are the most common nutritional symptoms during cancer treatment. These symptoms increase the risk of malnutrition and weight loss.7,10,32,33,36 In our study, the risk of weight loss increased 26.4 times in patients with nutrition-related symptoms. The presence of weight loss, loss of appetite, and malnutrition increase the necessity of using ONS in the individual nutrition plan.
In a meta-analysis of postoperative patients diagnosed with upper gastrointestinal cancer, researchers concluded that home enteral nutritional support resulted in a significantly higher quality of life, better body weight change, and higher albumin and pre-albumin levels compared to an oral diet. 37 In another study on cachexia and pancreatic cancer, investigators concluded that enteral nutrition support positively affects weight gain. 38
Our study initiated ONS in 52.2% of the patients in the program, of whom 97% had been moderately or severely malnourished at baseline. In the ONS personal nutrition plan, the dietitian defined the dose and timing of the recommended products. In addition, the dietitian informed the patients verbally and in writing on how to use the recommended ONS product, such as consumption time, dose, the temperature of the product, method of preparation, etc.
A recent randomized study reported that in post-discharge patients at nutritional risk following colorectal cancer surgery, using ONS may reduce skeletal muscle loss and prevalence of sarcopenia, as well as improve chemotherapy tolerance, compared to dietary advice alone. 39 Routine assessment of nutritional status and appropriate nutritional intervention are essential to reduce the adverse effects of malnutrition on the quality of life and survival of patients. In addition, nutritional homeostasis without anorexia or cachexia can optimize resistance to the side effects of anticancer therapy. 40
Early nutritional support in oncology patients has a positive effect on clinical outcomes. ONS helps increase calorie and protein intake and is beneficial in patients with increased energy requirements to improve results. It also helps with appetite loss during pre-cancer treatments to reduce side effects. 41 In our study, malnutrition rates improved in 40.3% of the patients who received both VNC and ONS aligned with ESMO and ESPEN guidelines.
Our study presents some limitations, such as selection bias. Our sample contains only volunteers, which limits the generalizability of our results as systematic differences may arise between those who volunteer and those who decline or do not respond to invitations or if the VNC was held mandatory. Also, we did not evaluate our patients’ education level, health literacy, and internet literacy.
The ability of patients and their caregivers to use online messaging applications such as WhatsApp are essential factors for the success of any VNC implementation. Almost all patients in the study could make calls on their mobile phones except for a few who needed assistance from others. The use of popular and well-known applications such as WhatsApp may have been instrumental in patients’ compliance with the program.
WhatsApp is one of the frequently used application in Turkey and all of the patients in our study were using WhatsApp and there were not any reported problem related to difficulty in access or using of the application in patients .On the other hand using other telemedicine apps in our country are not as common as WhatsApp. 42 In this topic Smith et al. 3 reported that “Enabling more equitable access to telehealth requires improvements in digital health literacy, workforce training in clinical telehealth, co-design of new telehealth-enabled models of care, change management, advocacy for culturally appropriate services, and sustainable funding models.”
The transition from severely malnourished to moderately malnourished or well-nourished category was 35.7% in patients who received three or more sessions of VNC. These results were statistically significant compared to the group that received less than three sessions. There is no consensus in the literature regarding the frequency of nutritional evaluation or the number of interval sessions. 23 Our results may contribute to the limited data on this subject and guide future studies regarding the frequency of nutritional monitoring for cancer patients. In addition, future research that compares face-to-face nutritional consulting to VNC via randomized controlled trials may provide information on the efficacy of VNC.
In the future, expanding messaging applications like WhatsApp in telehealth delivery may positively affect program sustainability and success. With the rapid onset of the pandemic, VNC was created to address the gaps in care, and this rapid transformation presented both challenges and opportunities. Our results showed that VNC enhanced the nutrition status of 69.4% of cancer patients who experienced malnutrition.
Healthcare providers may continue to use VNC as an alternative solution for the benefit of patients, specifically for centers without an oncology dietitian, by tapping into the resources of more extensive facilities. VNC can be an alternative option for patients who do not want to come to the hospital except for critical situations and may result in time and cost savings in some instances. Video visits wherein family members participate in a patient-centered care model are practical and can be leveraged for the success of future VNC programs. However, audio and video technologies may be shortcomings, such as connection problems or user experience.
Although there are barriers to VNC implementations, the importance of nutritional support as a distinguishing feature of good clinical practices in oncology treatment is emphasized more and more every day, and scientific evidence highlights the need to focus on multimodal cancer care.
With telehealth-based virtual nutrition consultancy, messaging applications such as WhatsApp and upcoming innovations will facilitate more accessible communication in the future. As a result, VNC, which started with the Covid-19 pandemic, will continue to be used more effectively in our daily practice.
Footnotes
Author Contributions
Dilşat Baş: writing-original draft preparation and software, investigation, and visualization; Özlem Sönmez: conceptualization, writing-original draft preparation, and software, critical reviewing and editing the final version of the manuscript, assessing study eligibility and conducting quality assessments, supervision, critical reviewing, and editing the final version of the manuscript. Elif Sitare Koç and Özde Melisa Celayir: assessing study eligibility and conducting quality. Ladan Hajhamidiasl and Ebru Tontaş: critical reviewing and editing the final version of the manuscript.
Ethics
The study was found suitable for medical ethics by the Medical Research Evaluation Board (ATADEK) of Acıbadem Mehmet Ali Aydınlar University, and approval from the Ethics Committee was taken.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.