
Abstract
Introduction
The aim was to identify whether cardiovascular telerehabilitation programs (CV-T-REHAB) can improve functional capacity, cardiorespiratory fitness and quality of life (QoL) to the same extent of presential rehabilitation (CV-P-REHAB) in older adults, by meta-analysis of previous studies.
Methods
Literature search was conducted in October 2020 in four databases to select controlled trials of CV-T-REHAB effects on functional capacity (six-minute walk test [6MWT]), cardiorespiratory fitness (maximal oxygen consumption [
Results
CV-T-REHAB improved 6MWT (11.14 m [CI95% = 8.03; 14.26], p < 0.001),
Conclusion
CV-T-REHAB improved cardiorespiratory fitness to a level equal to or higher than CV-P-REHAB and improved functional capacity and QoL; being mainly effective for QoL in older adults >65 years. Thus, CV-T-REHAB can be a good alternative, when not the best option and might be considered especially for individuals with limited access to participate in face-to-face programs.
Keywords
Introduction
Cardiovascular diseases have been the main cause of death in the world 1 and rehabilitation to treat patients previously hospitalized for cardiovascular events, such as coronary revascularization, percutaneous angioplasty, aortocoronary bypass, patients diagnosed with atherosclerosis, angina pectoris, myocardial infarction, and hypertension has been recommended by European and North American institutions.2–6 In 1998, the first scientific article on telerehabilitation was published and in recent years, the number of articles on the subject has increased, primarily due to the emerging needs of patients and the development of new information and communication technologies.7,8
Cardiovascular rehabilitation is an essential component of secondary prevention, multifaceted interventions designed to improve physical and social functioning. 2 On the other hand, mobility restrictions and financial constraints for patients to move to a rehabilitation centre, have been the main limitations for maintaining CV-REHAB. 9 In addition, the obligation of social isolation caused by the recent Coronavirus pandemic, made some CV-REHAB programs impossible to be maintained and underscored the urgent need for virtual assistance. 10
In this way, cardiovascular telerehabilitation (CV-T-REHAB) came up as an alternative to presential cardiovascular rehabilitation (CV-P-REHAB). 11 CV-T-REHAB allows contact between the health care professional, usually physical therapists, and patients from different places, connecting in real-time by electronic devices. 12 Despite some evidence of functional capacity and quality of life (QoL) improvements with CV-T-REHAB,13–15 some studies failed to show progresses in some of the same outcomes.16–18 The lack of consensus between studies may primarily be caused by comparison against non-rehabilitation or CV-P-REHAB groups since CV-T-REHAB certainly would be better than no intervention but doubly better than CV-P-REHAB. 19 Also, CV-T-REHAB could be more efficient for physical outcomes rather than psychological or social improvements that would be benefited by human interactions; however, this hypothesis remains unproved. 20 In fact, while a few studies have shown improvements from CV-T-REHAB in cardiorespiratory fitness even when compared to the CV-P-REHAB, some failed to show CV-T-REHAB benefits on QoL even when they were compared to non-rehabilitation control group. Differences in the characteristics of population, interventions and outcomes could determine heterogeneity between studies 18 and need to be properly tested by meta-analysis.
Thus, the present study aims to meta-analyse previous studies in the literature to identify the true effects of CV-T-REHAB when compared to CV-P-REHAB or control group (without rehabilitation) on cardiorespiratory fitness and QoL. The results of this study will be fundamental in designing future cardiovascular rehabilitation programs that will likely take place soon, allowing more patients to maintain their good health and QoL.
Methods
This systematic review was reported according to the recommendations of Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA).
Protocol and registration
The systematic review was submitted to PROSPERO under registration CRD42021250513.
Eligibility criteria
The items of PICOS inclusion criteria were adults (>18 years old) of both sex with any cardiopathy; intervention with a cardiovascular telerehabilitation program; compared to in-person cardiovascular rehabilitation or compared to a no-intervention group; assessing as outcomes the functional capacity by the 6-min walking test (6MWT), the maximum oxygen consumption in a progressive effort test (
Exclusion criteria
Reviews, letters to the editor, case studies, and studies describing methodological protocols without results were excluded. Studies not written in the English language were excluded. Studies that did not have telerehabilitation and studies that did not measure the proposed outcomes, such as functional capacity, cardiorespiratory fitness and quality of life (QoL), were also excluded.
Information sources
The search was performed on MEDLINE/PubMed, Web of Science, Scopus and Cochrane, with the last update in October 2020 and new studies in April 2022.
Search
The combination of synonyms for telerehabilitation, cardiac rehabilitation, virtual rehabilitation, QoL, physical fitness, the targeted outcomes and control trial terms were combined as described in the Supplemental material.
Study selection
Two independent researchers screened the studies according to the protocol description, the conflicts were identified by an automated spreadsheet equation, and they were solved by a third reviewer.
Data collection process
Two independent reviewers extracted data from the studies and analysed the mean and standard deviation (SD) of 6MWT,
Data items
We extracted the following categorical variables for subgroup analysis: sex (men or women), age (<64 years or >65 years), comorbidity (Arterial Hypertension, Coronary artery disease or Heart failure), type of control (CV-P-REHAB or no intervention), type of QoL questionnaires (Short Form 36 [SF-36]; EuroQol 5 Dimensions [EQ5D]; Minnesota Living With Heart Failure Questionnaire [MLHFQ]; Health Disease Health-Related Quality of Life Questionnaire [MacNew]; Health-Related Quality of Life Questionnaire [HRQol]; Dartmouth COOP Functional Health Assessment charts/WONCA [Dartmouth QoL]) type of exercise (aerobic training [AT] or combined training [CT]), and duration of intervention (≤9wk, 12–24wk or ≥24wk).
Risk of bias in individual studies
The PEDro scale was used to identify the quality of primary studies, according to the description of methodological information and the results of each study. 21
Statistical analysis
The three meta-analyses, testing the effects of cardiovascular telerehabilitation on (1) functional capacity (6MWT), (2) cardiorespiratory fitness (
Results
The flow diagram for the studies selection is detailed in Figure 1. Among the 26 studies included, 21 subgroups within studies assessed QoL, 9 assessed 6MWT and 16 assessed
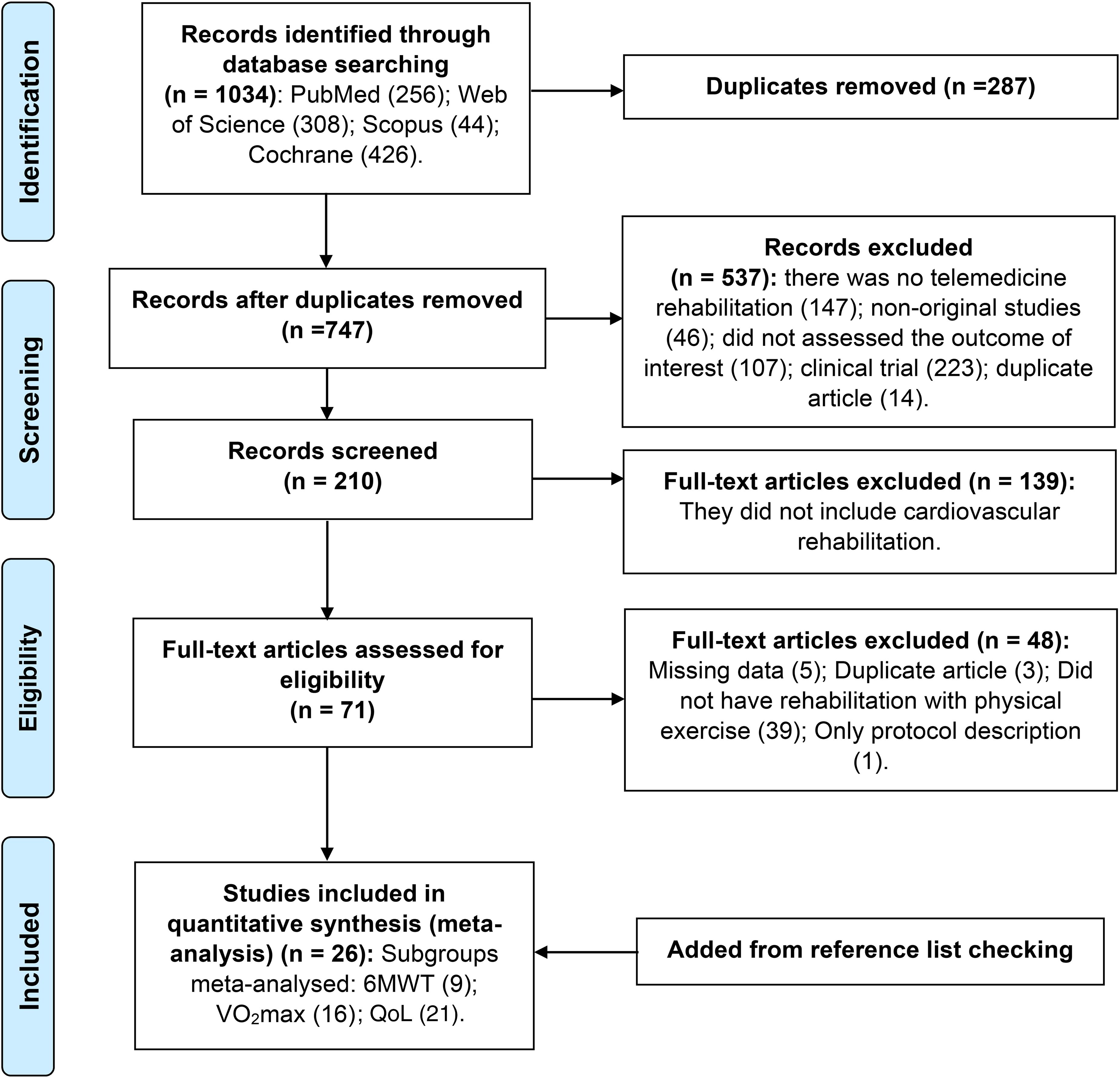
Study selection flowchart.
Characteristics of the studies
The characteristics of the studies included are described in Table 1. Twenty-three studies included both men and women, while three included only men and one included only women. Even though we did not exclude studies with individuals below 50 years old, the lower mean age of the studies included was 54.4 ± 10.9 33 and the studies were clustered according to the mean age of participants for further analysis (<64 years vs ≥65 years). The telerehabilitation programs included AT or CT, lasting from 4 to 48 weeks; their frequency varied from three to seven times per week.
Characteristics of the studies included.
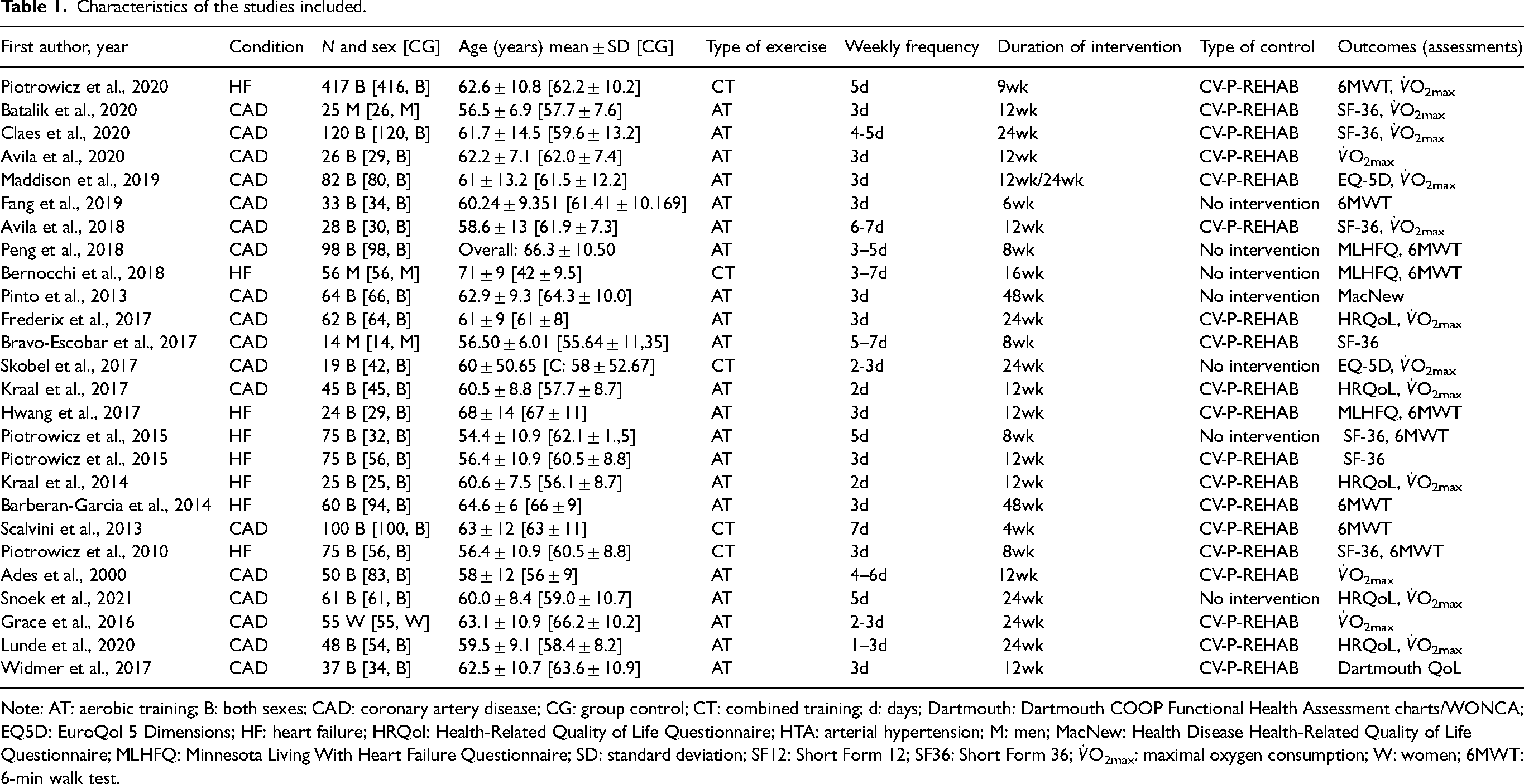
Note: AT: aerobic training; B: both sexes; CAD: coronary artery disease; CG: group control; CT: combined training; d: days; Dartmouth: Dartmouth COOP Functional Health Assessment charts/WONCA; EQ5D: EuroQol 5 Dimensions; HF: heart failure; HRQol: Health-Related Quality of Life Questionnaire; HTA: arterial hypertension; M: men; MacNew: Health Disease Health-Related Quality of Life Questionnaire; MLHFQ: Minnesota Living With Heart Failure Questionnaire; SD: standard deviation; SF12: Short Form 12; SF36: Short Form 36;
Quality of the studies
The quality of the studies ranged from 6 to 8 on the Pedro scale, and the details of their classification can be seen in Table 2.
PEDro scale score for the studies included.
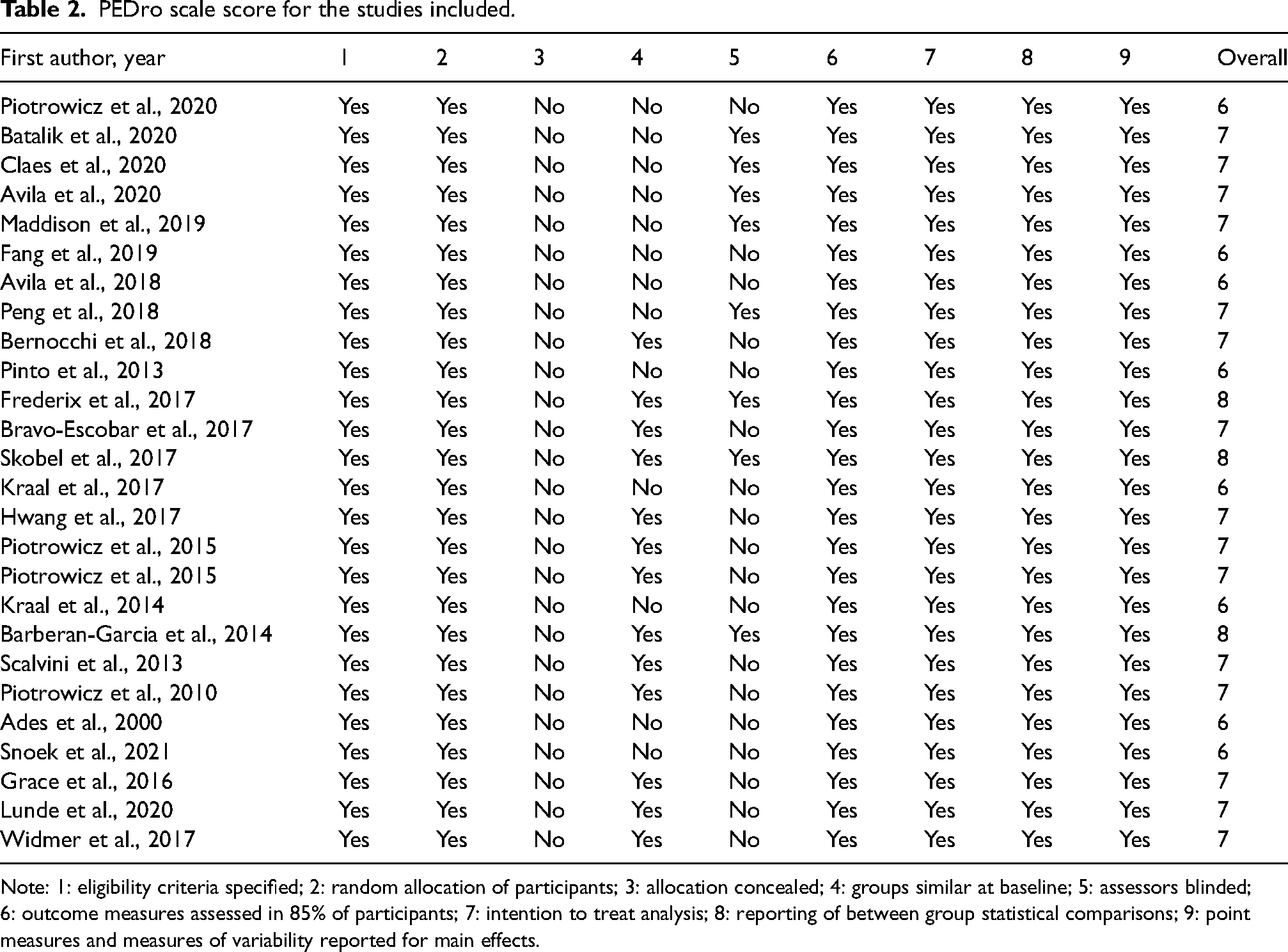
Note: 1: eligibility criteria specified; 2: random allocation of participants; 3: allocation concealed; 4: groups similar at baseline; 5: assessors blinded; 6: outcome measures assessed in 85% of participants; 7: intention to treat analysis; 8: reporting of between group statistical comparisons; 9: point measures and measures of variability reported for main effects.
Evidence synthesis
Egger tests confirmed the absence of publication bias within the three main meta-analyses (6MWT, t = 1.00 and p = 0.34;
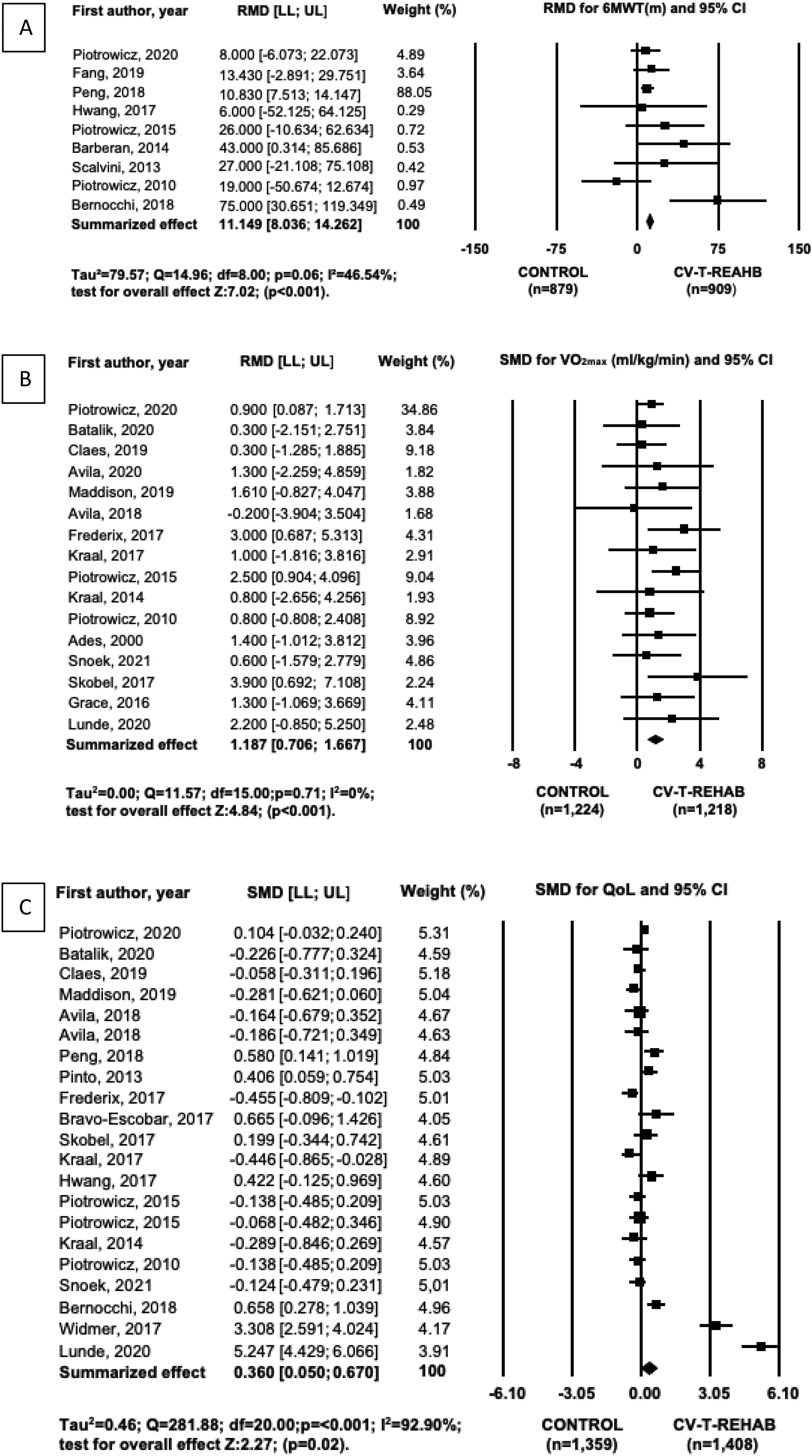
Forest of the effect of telerehabilitation on 6MWT (A),
Subgroup analysis of CV-T-REHAB effects on 6MWT.
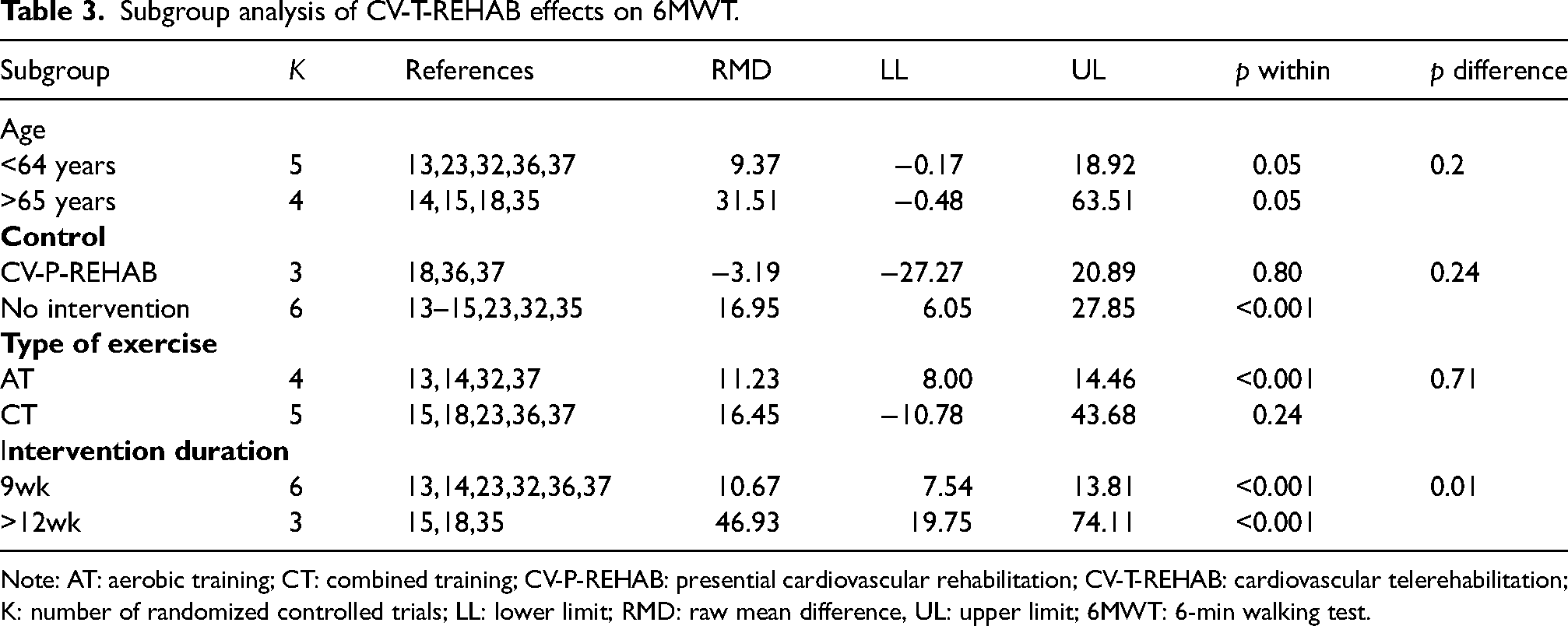
Note: AT: aerobic training; CT: combined training; CV-P-REHAB: presential cardiovascular rehabilitation; CV-T-REHAB: cardiovascular telerehabilitation; K: number of randomized controlled trials; LL: lower limit; RMD: raw mean difference, UL: upper limit; 6MWT: 6-min walking test.
The effect of CV-T-REHAB on improving cardiorespiratory fitness was also significant (Figure 2(b)) and consistent across studies (I2 = 0%). Furthermore, CV-T-REHAB led to significant increments in comparison to no intervention and, in comparison, within CV-P-REHAB (Table 4). Both AT and CT were effective to improve the
Subgroup analysis of CV-T-REHAB effects on
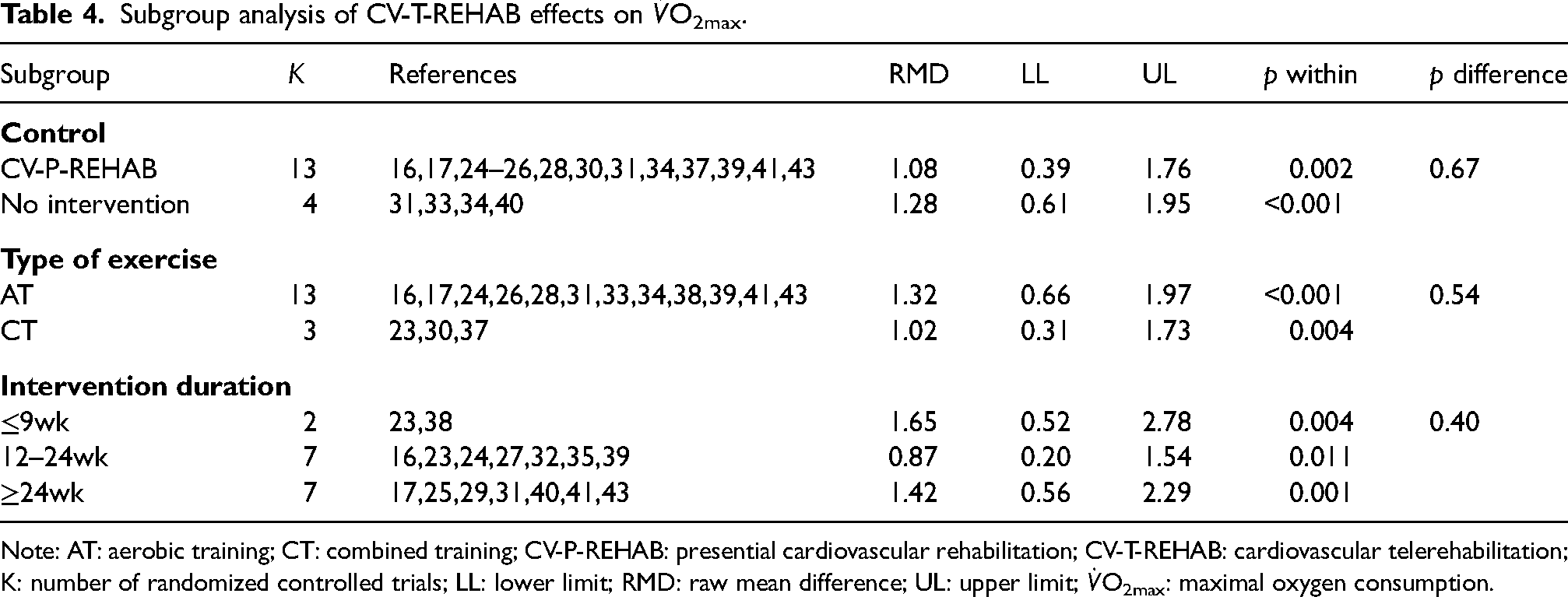
Note: AT: aerobic training; CT: combined training; CV-P-REHAB: presential cardiovascular rehabilitation; CV-T-REHAB: cardiovascular telerehabilitation; K: number of randomized controlled trials; LL: lower limit; RMD: raw mean difference; UL: upper limit;
Figure 2(c) shows a significant effect of CV-T-REHAB on QoL; however, the analysis was significant heterogeneous and had high inconsistency across studies (I2 = 92.90%). Subgroup analysis (Table 5) showed a significant increase for some QoL assessments such as MLHFQ, MacNew and Dartmouth; and for the subgroup of older adults above 65 years (including all types of QoL instruments). Interestingly, CV-T-REHAB did not improve QoL when compared to CV-P-REAHB. Duration of intervention did not influence QoL outcomes.
Subgroup analysis of CV-T-REHAB effects on QoL.
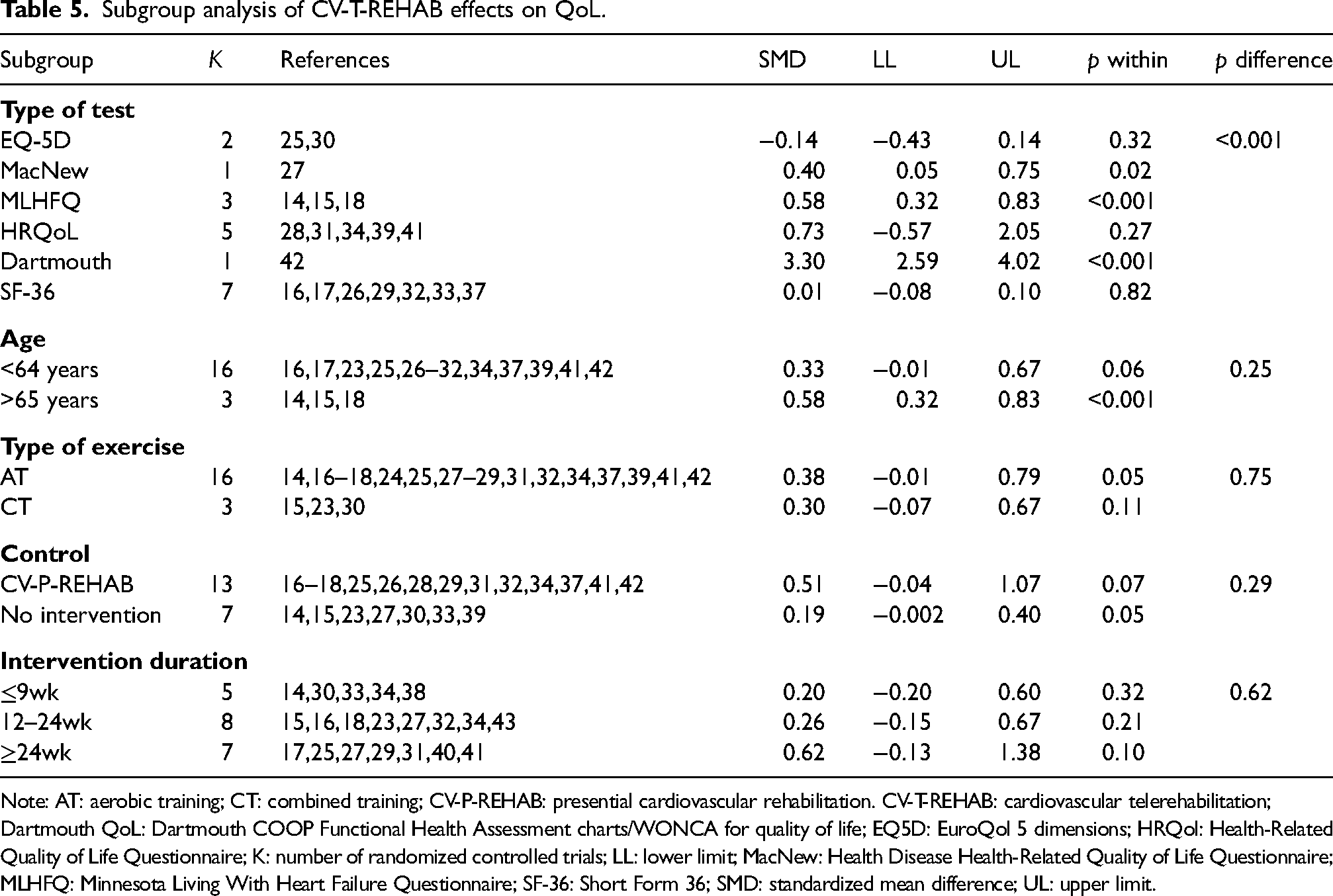
Note: AT: aerobic training; CT: combined training; CV-P-REHAB: presential cardiovascular rehabilitation. CV-T-REHAB: cardiovascular telerehabilitation; Dartmouth QoL: Dartmouth COOP Functional Health Assessment charts/WONCA for quality of life; EQ5D: EuroQol 5 dimensions; HRQol: Health-Related Quality of Life Questionnaire; K: number of randomized controlled trials; LL: lower limit; MacNew: Health Disease Health-Related Quality of Life Questionnaire; MLHFQ: Minnesota Living With Heart Failure Questionnaire; SF-36: Short Form 36; SMD: standardized mean difference; UL: upper limit.
Discussion
The main findings of the present study were the efficacy of CV-T-REHAB improving functional capacity (6MWT) and QoL, and improving
Regarding functional capacity, CV-T-REHAB improved 6MWT to the same extent as CV-P-REHAB and significantly higher than the control with no interventions. This effect was observed for both aging groups (<64 years and >65 years), and the different duration of interventions (9 weeks and >12 weeks), although only for AT rather than CT.
Whether the studies that used only 6MWT included the most diseased patients that were not able to perform a
Although an increase in maximal cardiorespiratory fitness (
The CV-T-REHAB was also enough to improve QoL, however the effect of CV-T-REHAB on QoL was inconsistent across studies. The improvement in QoL was seem in some questionnaires but not all. We attribute these differences to the different questionnaire scales that may remain difficult to compare even though we applied standardized analysis (SMD effects).
The increase in QoL with CV-T-REHAB was higher for patients above 65 years old than the younger ones. We suggest that whether this is true, CV-T-REHAB could be an even better alternative to older patients with physical and health limitations (e.g.: sarcopenia, pain, osteoarthritis, urinary incontinence, uncontrolled blood pressure) and need to overcome more barriers to be at rehabilitation centres. However, it is noteworthy that not all older adults have the required skills or access to handle certain technological devices, 46 and thus, telerehabilitation should be used to complement the existing services rather than replace them.41,48
Study limitation
The main limitation of our meta-analyses was the significant heterogeneity, suggesting confounding factors’ influence on the benefits of CV-T-REHAB on QoL. Even for the meta-analyses with non-significant heterogeneity, subgroup analyses were performed to identify any source of confounding factors. Although we raised some candidates to explain heterogeneity between studies, there were still a few heterogeneous subgroups remaining, in which future confounding factors need to be identified.
Unfortunately, some subgroup analyses were not possible due to the original heterogeneity within studies such as the inclusion of participants from different sexes, lack of information regarding the exercise protocols and adherence to each intervention.
Conclusion
The cardiovascular telerehabilitation programs were not just efficient in improving functional capacity by 6MWT and QoL but also better than in-person programs to improve cardiorespiratory fitness, assessed by
Because cardiovascular telerehabilitation with CT did not improve functional capacity, there is still a need to improve the telerehabilitation protocols to make it enough for all the benefits the CV patients demand. The longest interventions herein tested one year of rehabilitation. Still, not many studies tested these long-lasting effects, so future studies must continuous to explore how long the benefits can be maintained and develop strategies to keep the patients engaged in their rehabilitation. At last, since the telerehabilitation effectiveness for patients with CV disease is now confirmed, future studies need to compare types of protocols that will increase its effectiveness and ensure long-lasting benefits.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X221137626 - Supplemental material for Cardiovascular telerehabilitation improves functional capacity, cardiorespiratory fitness and quality of life in older adults: A systematic review and meta-analysis
Supplemental material, sj-docx-1-jtt-10.1177_1357633X221137626 for Cardiovascular telerehabilitation improves functional capacity, cardiorespiratory fitness and quality of life in older adults: A systematic review and meta-analysis by Diego Nacarato, Amanda V Sardeli, Lilian O Mariano and Mara Patrícia T Chacon-Mikahil in Journal of Telemedicine and Telecare
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.