
Abstract
Introduction
The purpose of this study is to show the non-inferiority of the telemedicine therapy versus face-to-face using the exercise therapy of oropharyngeal muscles in 183 patients treated consecutively from 2010 to 2020.
Method
We conducted a retrospective study comparing two dysphagia treatment groups: online versus face-to-face. Patients were distributed in a non-random way but according to patient's preferences. All patients followed the same pathway and were evaluated at the beginning and at the end of the study using the dysphagia outcome and severity scale and the functional oral intake scale. A non-inferiority analysis approximation was done with delta = 1 in both variables.
Results
Within a total of 183 patients, 114 (62.3%) used the online treatment and 69 (37.7%) the face-to-face one. The main cause of dysphagia was neurological in the total sample (60.7%) and within both groups. When we evaluate the clinical response, we find that both groups improved regardless of the type of therapy. The confidence interval of the difference between the beginning and the end of treatment did not reach the inferior limit of the delta defined, therefore supporting the no inferiority of online versus presential.
Discussion
This study shows the no inferiority of the online therapy versus the face-to-face one for the oropharyngeal training of the swallow muscles.
Introduction
Swallowing is a complex sensorimotor sequence that is controlled by cortical, subcortical and brainstem mechanisms that allow a coordinated action of the orofacial, pharyngeal, laryngeal, respiratory and oesophageal muscles. It is a complex motor event with a sequential and ordered activation that is influenced by sensory and cortical stimuli. The sequential muscle activation is not altered in its cranial-caudal progression from the perioral muscles to the cricopharyngeus muscle, which is part of the upper oesophageal sphincter.
When swallowing is impaired due to neurological, head and neck surgery or respiratory diseases amongst others, dysphagia occurs. Oropharyngeal dysphagia is defined as an alteration in the passage of the food bolus from the mouth to the oesophagus. It can occur at any age but its prevalence increases with age.
Oropharyngeal dysphagia affects more than 30% of patients who have suffered a stroke. In Parkinson's disease its prevalence is between 52% and 82%; it is the initial symptom of 60% of patients with amyotrophic lateral sclerosis; it affects 40% of patients with myasthenia gravis, 44% of patients with multiple sclerosis, up to 84% of Alzheimer's disease patients and more than 60% of the elderly institutionalised. Oropharyngeal dysphagia affects up to 80% of patients who have received surgical or radiotherapy treatment for oropharyngeal, laryngeal and maxillofacial area tumours. Furthermore, dysphagia has two major complications: malnutrition and respiratory infection. 1
There are several strategies to treat dysphagia and one of them is the exercise of the oropharyngeal muscles.2–5 The swallowing muscles can atrophy when they are not used in a context of a disease or aging. Geniohyoid muscle atrophy has been associated with aspiration, a mayor complication of dysphagia. 6 Muscle atrophy is reversible with exercise.4,5
Within the dysphagia treatment, the training of the oropharyngeal muscles is a fundamental part of such treatment regardless of the type of oropharyngeal swallowing disorder.
We have been using since 2010 an online program to train the oropharyngeal muscles in the context of treating oropharyngeal dysphagia. The purpose of this study is to show the non-inferiority of the telemedicine training of oropharyngeal muscle versus the traditional face-to-face treatment in 183 patients treated consecutively from 2010 to 2020 by the same speech therapist and using the same protocol.
Method
Study design
After Institutional Review Board approval, we conducted a retrospective study of the dysphagia database of the Physical Medicine and Rehabilitation Department at University Hospital of Sant Pau (Barcelona, Spain) comparing two oropharyngeal dysphagia treatment groups: online versus face-to-face. Patients were distributed according to their preferences in a non-random way. The dysphagia database includes all patients diagnosed by modified barium swallow (MBS) of oropharyngeal dysphagia, who have undergone either online or face-to-face treatment with oropharyngeal exercise from 1 July of 2010 to 31 January of 2020.
Except for the treatment (online vs. face-to-face) all patients had followed the same clinical pathway during a 10-year period: doctor's first evaluation and MBS done the same day; speech therapist evaluation between 4 and 6 weeks after the MBS followed by 13 days of oropharyngeal muscle training either online or presential; speech therapist’s final evaluation and doctor's evaluation with MBS study at the end done in one single appointment between 4 and 6 weeks after the completion of therapy. The MBS is performed by the same physician in all cases.
The reason why we do 13 therapy sessions is because it is being imposed to providers by the contract model with the Catalan Health System. Such a model allows only 15 speech therapy visits that include evaluation and treatment for oropharyngeal dysphagia patients.
Study population. Inclusion and exclusion criteria
One hundred and eighty-three (n = 183) patients were treated consecutively during a 10-year period.
Our study population included adult patients ≥ 18 years old who underwent either online or face-to-face treatment for oropharyngeal dysphagia.
From September 2010 to January 2020, all patients diagnosed with oropharyngeal dysphagia were given the option to do the therapy either online or presential in our Rehabilitation Department.
The online group inclusion criteria were: age ≥ 18 years; to be diagnosed with oropharyngeal dysphagia by MBS evaluation with ≤ 5 level at the Dysphagia Outcome and Severity Scale 7 (DOSS); to have Internet connection at home or use a mobile device to access the network (3-4G) and use email (the patient or their relative caregiver); to sign the consent to accept the photo-video recording of the Rehabilitation Department of our Hospital, and to accept online therapy.
The inclusion criteria for the face-to-face group were: age ≥ 18 years, to be diagnosed with oropharyngeal dysphagia by MBS with ≤ 5 level at the DOSS, 7 to not meet the inclusion criteria for online therapy and to accept conventional face-to-face therapy.
All patients who did not meet any of the inclusion criteria in the online or face-to-face group were excluded.
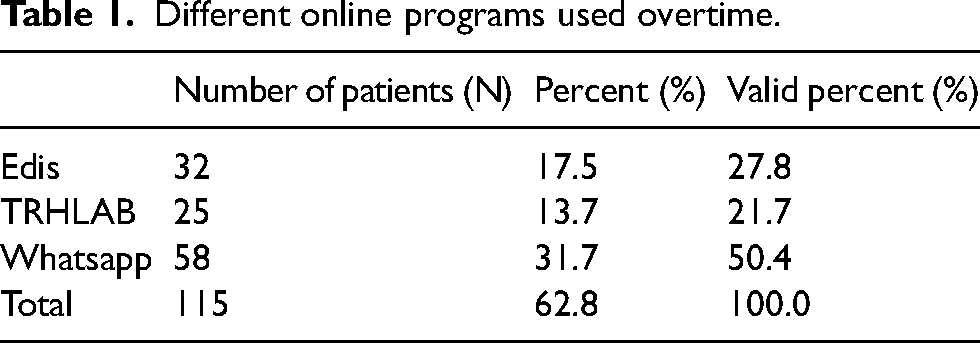
The patients in the online group used different Internet tools over the years. From 2010 to 2012 they used a platform named ‘edis’, from 2012 to 2015 they used a platform named ‘TRHLAB’, and from September 2015 to today oropharyngeal exercises are free of access in YouTube and patients are followed by WhatsApp using a hospital cellular phone. The exercises are available at https://www.youtube.com/channel/UCCrIoHDinvBcF5c_8LcfZ2A. Each patient did a selection of 12–16 of those exercises depending on the clinical and MBS results. The exercise program duration is 45–60 min per day and had to be done with speech therapist supervision during 13 days distributed in 3 consecutive weeks. The follow-up has always been identical and asynchronous: patients recorded videos after looking at the video of the exercise, recorded and sent a video performing the same exercise adding comments and/or questions; the speech therapist evaluated them and sent feedback the following working day.
The patients in the ‘face to face’ group came to our Rehabilitation Department for treatment and used the same exercises recorded for the online group. In addition, they all did 13 therapy sessions with 14–16 exercises per session and during 45–60 min working days during 3 consecutive weeks.
Both groups had the recommendation of doing all the exercises trained in therapy every working day until the physiatrist evaluation done between 4 and 6 weeks after completion of the exercise therapy and the final speech therapist's clinical evaluation.
Data collection and analysis
The main outcome measures were: (a) the DOSS 7 that classifies the severity of dysphagia according to the modified swallow evaluation results in a scale graded from 1 to 7, 1 being a severe dysphagia with recommendation of non-oral feeding and 7 a normal swallow with no food restriction per mouth, 6 is a functional swallow and the different levels of dysphagia are from 5 to 1. The scale grading system is based on penetration/aspiration and oropharyngeal residue. (b) The Functional Oral Intake that classifies clinically the type of oral diet the patient is actually taking, it's a 1 to 7 point scale 1 being only tube feed and 7 full oral with no restrictions for any type of solids or liquids. 8
The variables described are median, mean and standard deviation. To evaluate both treatments we calculated the difference between the initial and the final value. Also we calculated the difference of such difference, with a confidence interval of 95%, to be able to evaluate the no inferiority approximation. We have established the delta value for a no inferiority in 1 point for DOSS and FOIS. For the statistical analysis we used the statistical package IBM-SPSS (V26.0).
Results
A total of 183 patients underwent oropharyngeal dysphagia treatment with exercise of swallow muscles. 114 (62.3%) patients did the online treatment and 69 (37.7%) the face-to-face one. The mean age of the total sample was 58.53 years (14–89). Among the online group the mean age was 56.04 years (SD 14.852) and the mean age of the face-to-face group was 64.42 (SD 14.628) Analysing the age with Levine equal variance test (p = 0.539) showed no significant age differences among both groups, even though the online group is younger.
Table 1 summarises the frequencies of the different online programs that we have used thru this 10-year period.
Different online programs used overtime.
There were 108 (59%) men and 75 (41%) women. Within the total of 108 men, 41 (59.4%) choose the face-to-face therapy and 67 (58.8%) choose the online one. Among the 75 women, 28 (40.6%) picked the presential treatment and 47 (41.2%) the online option. Using the Pearson's χ2 test we obtain a p = 0.931 showing no significant differences in sex distribution among the face-to-face and the online group.
The diagnoses were grouped in neurological, structural from otorhinolaryngology surgeries, structural from neurosurgery, pneumological and others. Table 2 summarises the diagnoses and the distribution among presential and online group with a p = 0.069 on the Pearson's χ2 test showing no significant differences in diagnoses among groups.
Medical diagnoses of therapy groups.
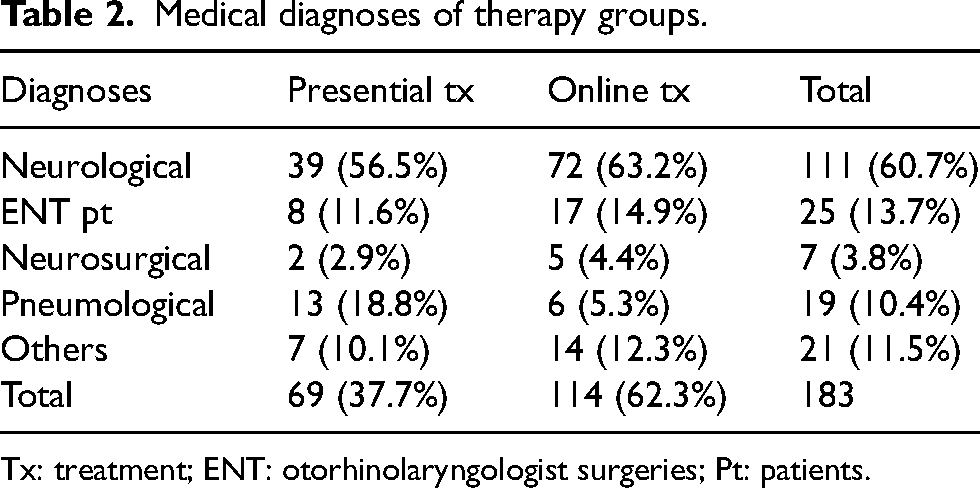
Tx: treatment; ENT: otorhinolaryngologist surgeries; Pt: patients.
The number of respiratory infections during the year prior to treatment was similar in both groups as is shown in Table 3. There were no respiratory infections reported on any group after completion of treatment.
Respiratory infections prior to treatment.
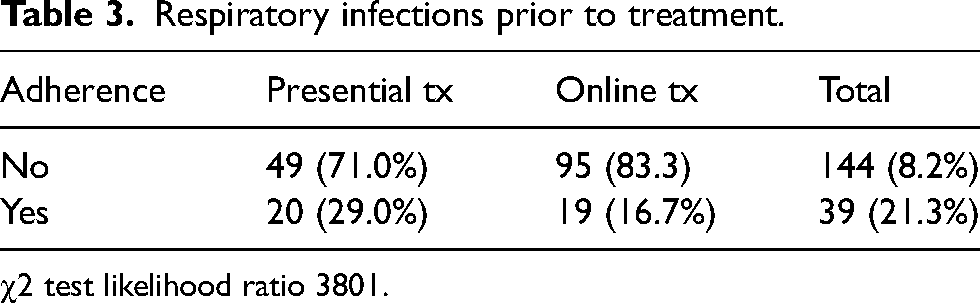
χ2 test likelihood ratio 3801.
The analysis of the face-to-face and the online group according to DOSS and FOIS before starting treatment showed no statistical differences in the DOSS (p = 0.068), but there was statistical difference according to the FOIS (p < 0.001). Table 4 summarises those results.
DOSS and FOIS before treatment.
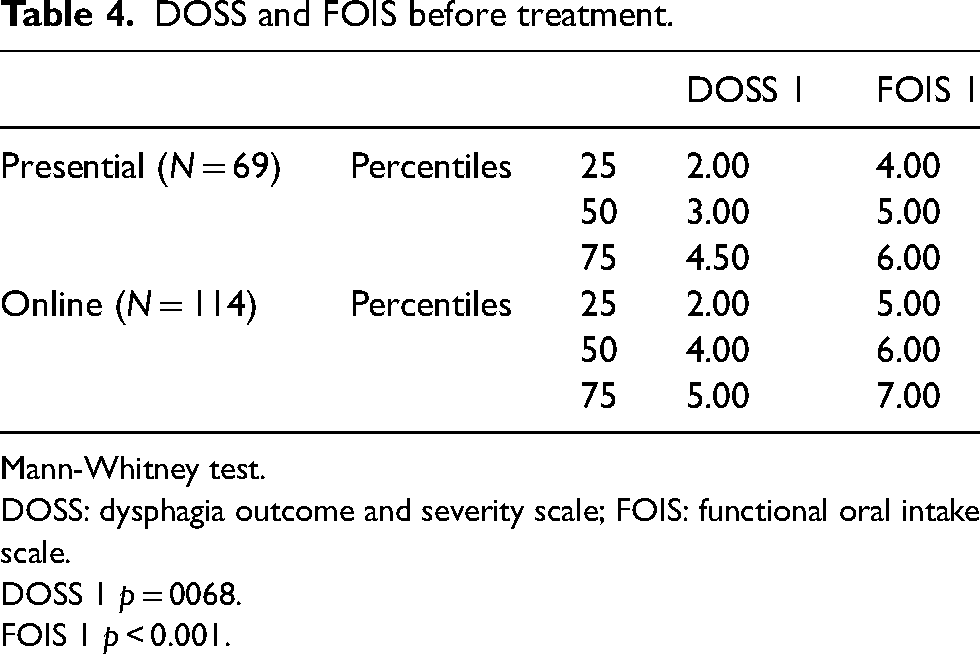
Mann-Whitney test.
DOSS: dysphagia outcome and severity scale; FOIS: functional oral intake scale.
DOSS 1 p = 0068.
FOIS 1 p < 0.001.
The face-to-face and the online group were analysed according to DOSS and FOIS after completion of the treatment and showed no statistical differences in the DOSS (p = 0.987), or according to the FOIS (p = 0.616). Table 5 summarises those results.
DOSS and FOIS after treatment.
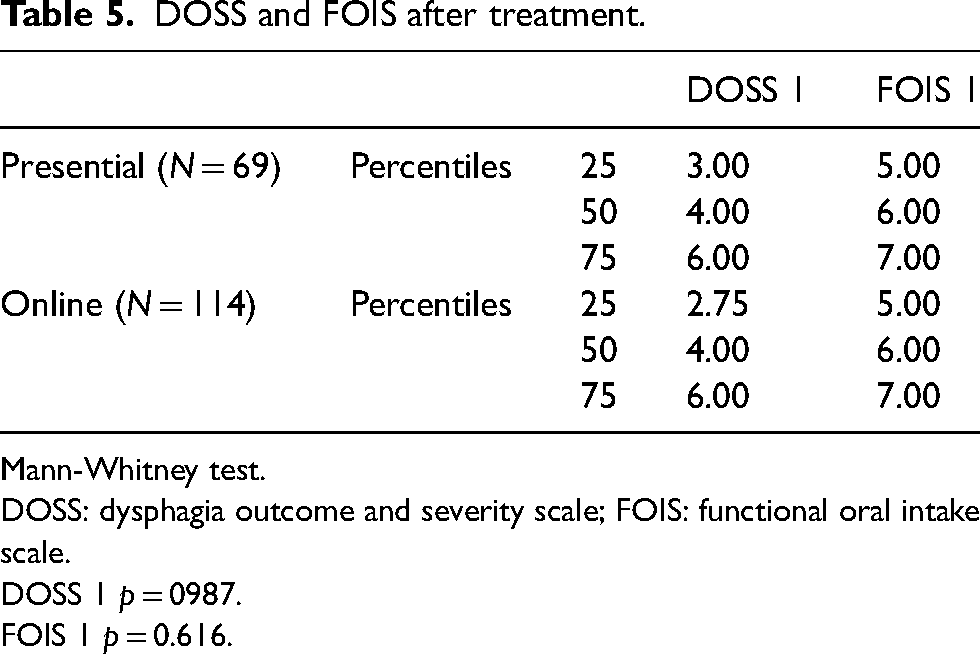
Mann-Whitney test.
DOSS: dysphagia outcome and severity scale; FOIS: functional oral intake scale.
DOSS 1 p = 0987.
FOIS 1 p = 0.616.
All patients, regarding the group, had a MBS and the severity of their oropharyngeal dysphagia was classified according the DOSS. Table 6 summarises de results of the DOSS before the training (DOSS 1) and after the training (DOSS 2) in both groups.
Summary of the results of DOSS 1 and DOSS 2 and median/mean differences.
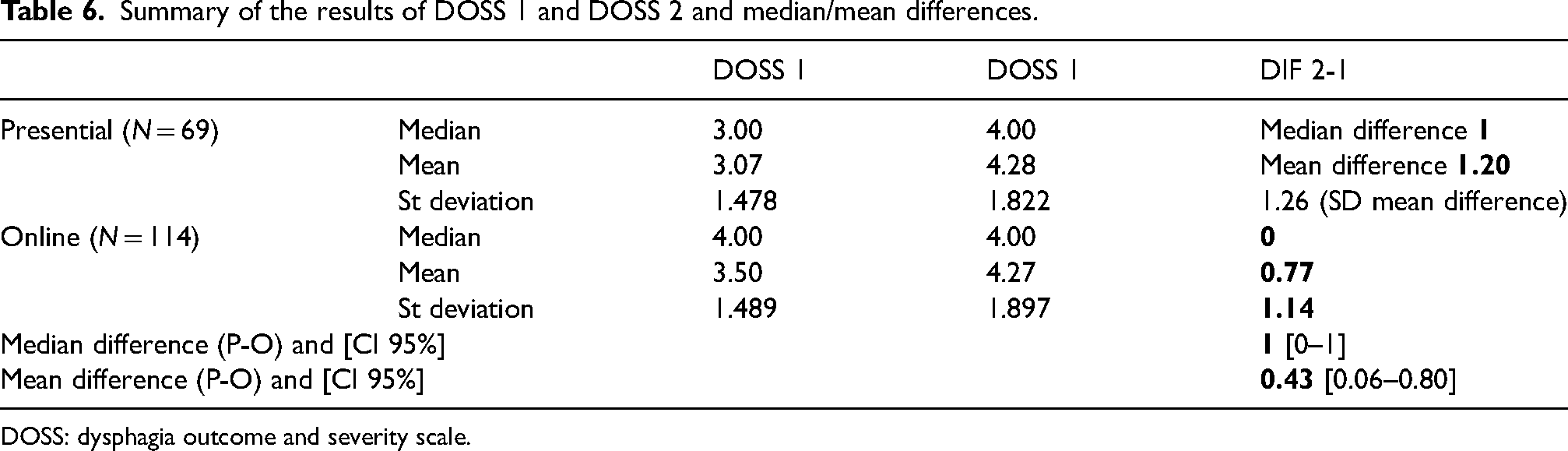
DOSS: dysphagia outcome and severity scale.
The intake of food per mouth was assessed in all patients using the FOIS. Table 7 summarises de results of the FOIS done before the training (FOIS 1) and after the training (FOIS 2) in both groups.
Summary of the results of functional oral intake scale (FOIS 1) and FOIS 2 and median/mean differences.
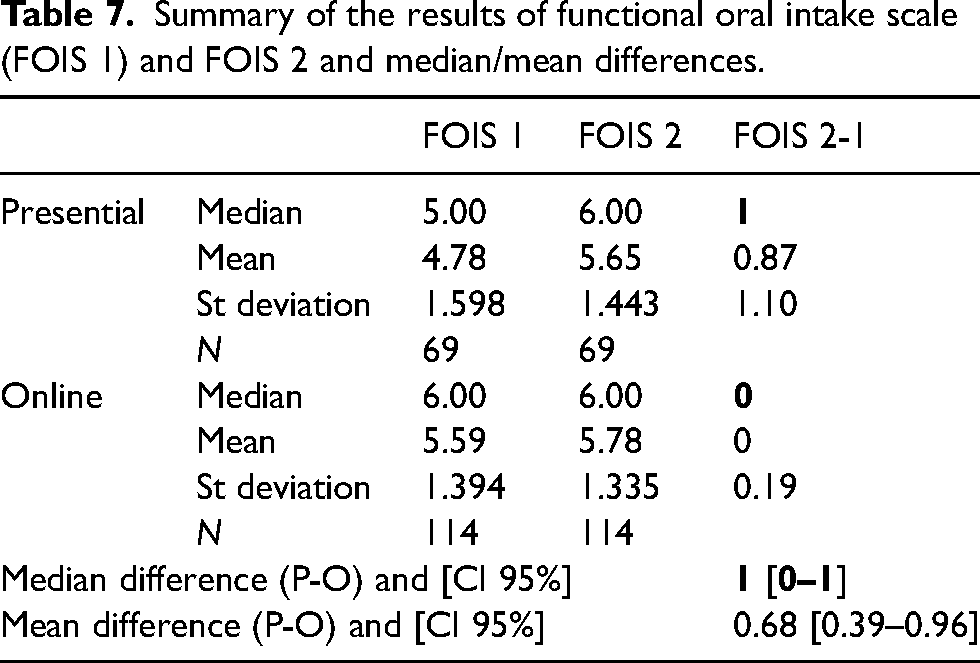
When we evaluate the clinical response by evaluating the median of the change between the beginning and the end of the variables FOIS and DOSS, and we calculate a CI 95% of the difference between the medians of this change [0–1] with the minimum delta of 1 point between groups, we can assume that online treatment is not inferior that the face-to-face one. Tables 6 and 7 show those calculations.
We also studied the adherence to oropharyngeal exercise. We consider adherence that the patient exercised on a daily bases while was followed by the speech therapist. After completion of the 13 therapy sessions online or face-to-face, the patient had to continue 5 days per week until the MBS was done 4–6 weeks later. The results are summarised in Table 8, and shown no differences.
Adherence to oropharyngeal exercise.
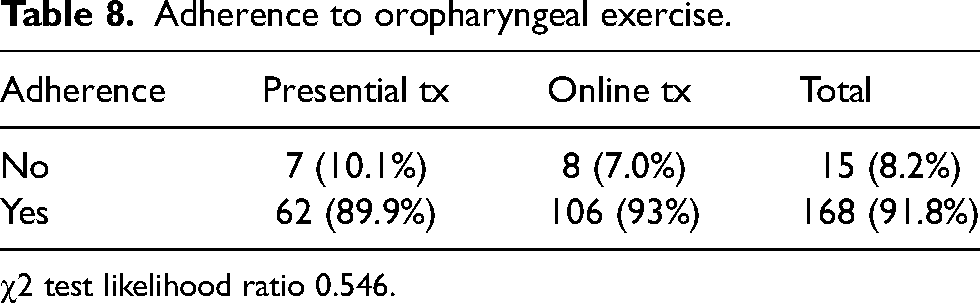
χ2 test likelihood ratio 0.546.
Discussion
There are an emerging number of telerehabilitation studies on dysphasic patients.9–14 However, this study is the first one that compares online and face-to-face care reporting swallowing outcomes and/or swallowing improvements, which are both essential to verify the effectiveness of a treatment. The randomised control trial of Wall et al. 15 studied adherence to a prophylactic swallowing exercise protocol, and if clinical and demographic factors influence adherence but it does not report swallowing outcomes and/or improvements.
In our study, the baseline characteristics of the face-to-face and online group are comparable in terms of: cause of the swallowing disorder, initial severity of their oropharyngeal swallow according to the Dysphagia Outcome and Severity Scale (which rates the modified barium swallow evaluation) and comparable respiratory infections prior to therapy. The FOIS evaluation showed that the online group had taken a less restricted oral diet at the beginning of the program probably because this group was younger and did not have any prior recommendation about it. After performing the therapy, both groups improve, even though there is a slight better improvement in the presential group, when is calculated the confidence interval of the improvement between the two therapies the limit value does not overpass the level of delta defined as no inferiority for both variables DOSS and FOIS. The slight better improvement of the presential group could be secondary to daily therapy encourage of face-to-face therapy.
We think that the improvement of both groups is based on that they used the same series of oropharyngeal exercises with the same intensity, and had the exact same medical and therapeutic evaluation protocol. The adherence to therapy in both groups is also equivalent.
A limitation of our study is that was not designed as a randomised control trial. The patients decided which modality of treatment they preferred according to their technological possibilities. Our study shows the digital gap in relation to age. Our face-to-face group had a mean age of 64.42 years and the online group was 56.04. In Europe, 83% of its population uses the Internet and this increases to 96% for the youth (15–24 year old individuals). 16 In the age group from 55 to 74 years, only 46% are Internet users, according to Seybert 2013 study. Almost all our patients are within that age group but the online group was 8 years younger.
In addition, there are some other limitations as the type of outcome used (DOSS) in a 10-year period.
Conclusion
In the last years telerehabilitation is becoming an alternative to face-to-face therapy in speech and language therapy, which has been examined by several studies.3,11 Specifically, telemedicine offers a possibility to increase access to clinical rehabilitation medicine services and to guarantee adequate services to people with swallowing disorders. Face-to-face therapy has always been considered the ‘gold standard’ of care, and our study, even though is not a randomised control trial, shows that the outcomes of online therapy are not inferior to the face-to face one evaluated with the DOSS and the FOIS. Our results contribute to the endorsement of the online therapy.
Further studies should be done to define the additional benefits and risks eventually associated with the telerehabilitation of oropharyngeal dysphagia.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.