
Abstract
Telehealth is an important source of health care during the COVID-19 pandemic. Evidence is scarce regarding disparities in telehealth utilization in the United States. We aimed to investigate the prevalence and factors associated with telehealth utilization among US adults. Our data came from the Health, Ethnicity, and Pandemic Study, a nationally representative survey conducted in October 2020, with 2554 adults ≥ 18 and an oversample of racial/ethnic minorities. Telehealth utilization was measured as self-reported teleconsultation with providers via email, text message, phone, video, and remote patient monitoring during the pandemic. Logistic regressions were performed to examine the association between telehealth use and factors at the individual, household, and community levels. Overall, 43% of the sample reported having used telehealth, representing 114.5 million adults in the nation. East and Southeast Asians used telehealth less than non-Hispanic Whites (OR = 0.5, 95% CI: 0.3–0.8). Being uninsured (compared with private insurance: OR = 0.4, 95% CI: 0.2–0.8), and those with limited broadband coverage in the community (OR = 0.5, 95% CI: 0.3–0.8) were less likely to use telehealth. There is a need to develop and implement more equitable policies and interventions at both the individual and community levels to improve access to telehealth services and reduce related disparities.
Keywords
The COVID-19 pandemic created obstacles (e.g. reduced hospital capacities, social distancing restrictions) for accessing health care. Many health care providers and health systems shifted from the traditional ambulatory in-office care model to a telehealth care model that facilitates remote patient-provider communication,1–5 with support from the US government providing more funding and equipment for telehealth. 6 Telehealth services span a wide range of virtual communication, such as video conferencing, telephone calls, emails, text messages, and remote patient monitoring.1,4,7
The use of telehealth could facilitate health care access for socially or economically disadvantaged populations. 8 However, disparities in telehealth utilization may exist, particularly for individuals who have historically faced an access barrier to telehealth, 9 including those who are ethnic minorities, having low socioeconomic status, being medically vulnerable, having limited technological access, or living in rural areas.7,10 Recent studies have used regional data from a single health system or used non-representative claims data to examine disparities in telehealth access among vulnerable populations.4,7,11 However, evidence on telehealth utilization at the national level is sparse.
This study aims to estimate the national prevalence of telehealth use as well as telehealth use by types of insurance in the United States during the pandemic. In addition, based on the National Institute on Minority Health and Health Disparities Research Framework, 12 this study aims to identify significant factors at the individual level, interpersonal/household level, and neighborhood level associated with telehealth utilization during the COVID-19 pandemic.
Methods
Data and sample
In October 2020, we commissioned the National Opinion Research Center (NORC) at the University of Chicago to conduct a nationally representative survey, the Health, Ethnicity, and Pandemic (HEAP) Study. This survey was designed to understand mental health, lifestyle changes, racial discrimination, financial status, and healthcare utilization in the United States during the pandemic. The sample was randomly selected from the AmeriSpeak Panel using sampling strata including age, gender, race/ethnicity, and educational attainment, following the American Association for Public Opinion Research guidelines. 13 AmeriSpeak is a probability-based panel designed to be representative of the US non-institutionalized population. 13 Additional minority respondents were recruited from Dynata panel participants. Overall, the response rate was 4.2%. Each respondent was given $3 in cash or the equivalent as an incentive to complete the questionnaire. The sample included 2709 adults aged ≥18 years, in which Asians (n = 979) and other minorities were oversampled. We oversampled Asians and other minority groups because the HEAP study aimed to investigate how minorities, especially Asians, experienced racial/ethnic discrimination during the pandemic. The surveys were conducted in English and Spanish. Most respondents participated in the survey online, and respondents with no internet access participated by telephone. It took them 15–20 min each to complete the survey. Poststratification survey weights were constructed to reflect the US adult population profile, adjusting for possible selection bias and nonresponse rate. In the analyses, we excluded those who did not report telehealth use information or covariates in the study and had a final sample of 2554 respondents. The study was approved by the Institutional Review Board at the NORC. 14
Variable measures
The outcome measure was the self-reported utilization of telehealth services (e.g. teleconsultation with health care providers via email, text message, phone, video, and remote patient monitoring) during the COVID-19 pandemic. The original question in the survey was, “Did you receive any telehealth services (e.g. teleconsultation with your care provider via emails, text message, phones, and videos, remote patient monitoring) during the COVID-19 pandemic?” Respondents who answered “Yes” to this question were considered having used telehealth. We also queried participants for delayed or forgone care, including preventive care, mental health care, prescription medicines, dental care, vision care, specialist care, follow-up care, or other medical care due to the pandemic. The original question in the survey was, “Which of the following healthcare have you delayed or forgone due to the COVID-19 pandemic? (Check all that apply). (a) Preventive care including physical examination, flu vaccination, and cancer screening; (b) Mental health care or counseling; (c) Prescription medicines; (d) Dental care; (e) Eyeglasses; (f) Specialist care; (g) Follow-up care; (h) Other medical care; (i) No care delayed.” Respondents can choose more than one option. Those who responded having delayed or forgone any type of care were grouped altogether for a subsample analysis because these respondents may have unmet health care needs.
Individual-level factors that may be associated with telehealth use included self-reported age, gender, race/ethnicity, foreign- or native-born, educational attainment, marital status, employment status, primary spoken language, insurance coverage, and self-rated health status. Since we oversampled Asians, race/ethnicity was classified into six groups (non-Hispanic White, non-Hispanic Black, non-Hispanic East and Southeast Asian, other Asians, Hispanic, and other races). The category “East and Southeast Asian” included all respondents who self-identified as Chinese, Japanese, Korean, Burmese, Cambodian, Filipino, Hmong or Miao, Indonesian, and Vietnamese. The “other Asian” category included all respondents who self-identified as Asian Indian, Bangladeshi, Nepalese, Pakistani, and Asians from other countries. Insurance coverage was classified into four categories, including private insurance, Medicaid and other public insurance, Medicare and supplement insurance, and uninsured.
Household-level factors included household income, household size, internet access within the household, and home type (a single-family house, a building with apartments, and a mobile home or a trailer).
Respondents’ self-reported residential locations were linked with county-level measures obtained from the Social Determinants of Health Database compiled by the Agency for Healthcare Research and Quality. 15 The community-level factors included residential regions (New England, Mid-Atlantic, East North Central, West North Central, South Atlantic, East South Central, West South Central, Mountain, and the Pacific), rurality of the county, defined based on the Guidelines for Using Rural-Urban Classification Systems for Community Health Assessment, 16 broadband coverage in the community (< 90% versus ≥ 90%), and perceived racial discrimination in the society. Perceived racial discrimination was assessed using a nine-item Coronavirus Racial Bias Scale discrimination (Cronbach's α = 0.89). The Likert-scale responses to the nine survey questions were summed up, and thus higher score indicated perception of more bias against one's own race and ethnicity. 17
Statistical analyses
All statistical analyses were performed with poststratification weighting to account for the complex sampling methods and nonresponse rate, and thus provided unbiased estimates for the general US adult population. To control for potential sample selection bias in which only those who needed health care responded to the telehealth question, we performed a subsample analysis among those who reported having delayed or forgone care. Characteristics of the study samples who had used or had not used telehealth services during the pandemic were compared using t-test for the perceived racial discrimination score and χ2 tests for all other variables. Multivariable logistic regression models were performed to calculate adjusted odds ratios (OR) for the association of various factors with telehealth use as well as the adjusted prevalence of telehealth use. The significance threshold was 2-tailed, with p < 0.05 considered statistically significant. Stata/MP version 14.2 (StataCorp) was used to conduct the analysis.
Results
Among the 2554 participants, 1047 (42.8%) reported having used telehealth during the pandemic, representing 114.5 million in the nation (Table 1). Among 1632 participants who reported having delayed or forgone care, 749 (47.1%) reported utilizing telehealth during the pandemic. The prevalence of telehealth use was significantly higher among younger adults, females, those working as a paid employee, having insurance coverage, having good health, and those living in a single-family house (Table 1).
Characteristics of the Health, Ethnicity, and Pandemic (HEAP) study sample by use of telehealth services during the COVID-19 pandemic a .
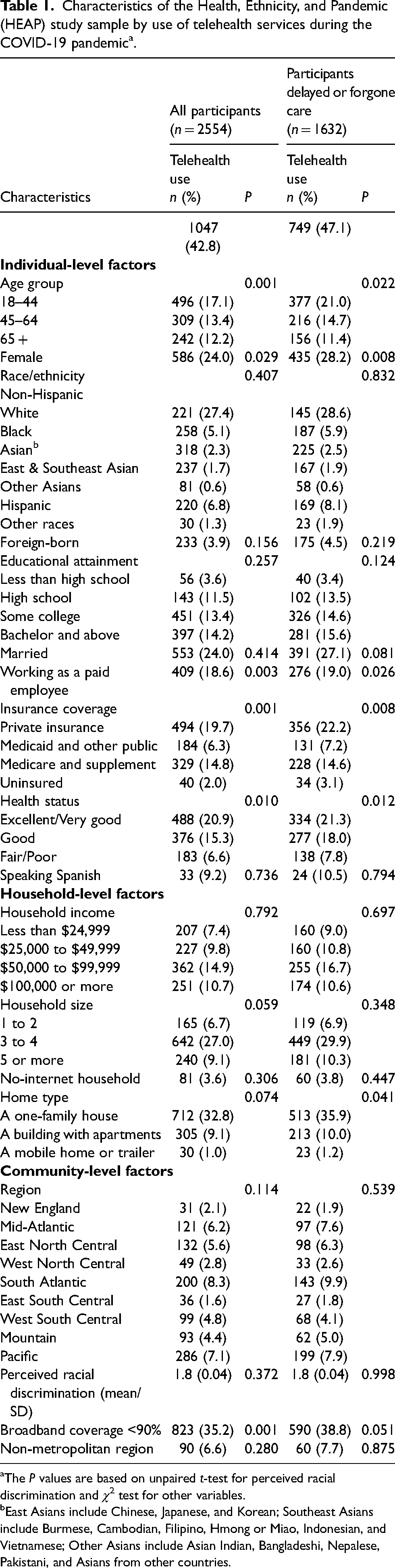
The P values are based on unpaired t-test for perceived racial discrimination and χ2 test for other variables.
East Asians include Chinese, Japanese, and Korean; Southeast Asians include Burmese, Cambodian, Filipino, Hmong or Miao, Indonesian, and Vietnamese; Other Asians include Asian Indian, Bangladeshi, Nepalese, Pakistani, and Asians from other countries.
In the entire sample applying the sampling weights, 46.0% of the respondents who utilized telehealth had private insurance coverage, 34.0% had Medicare coverage, 15% were covered by Medicaid or other public insurance, and 5% were uninsured when they received telehealth services (Figure 1).
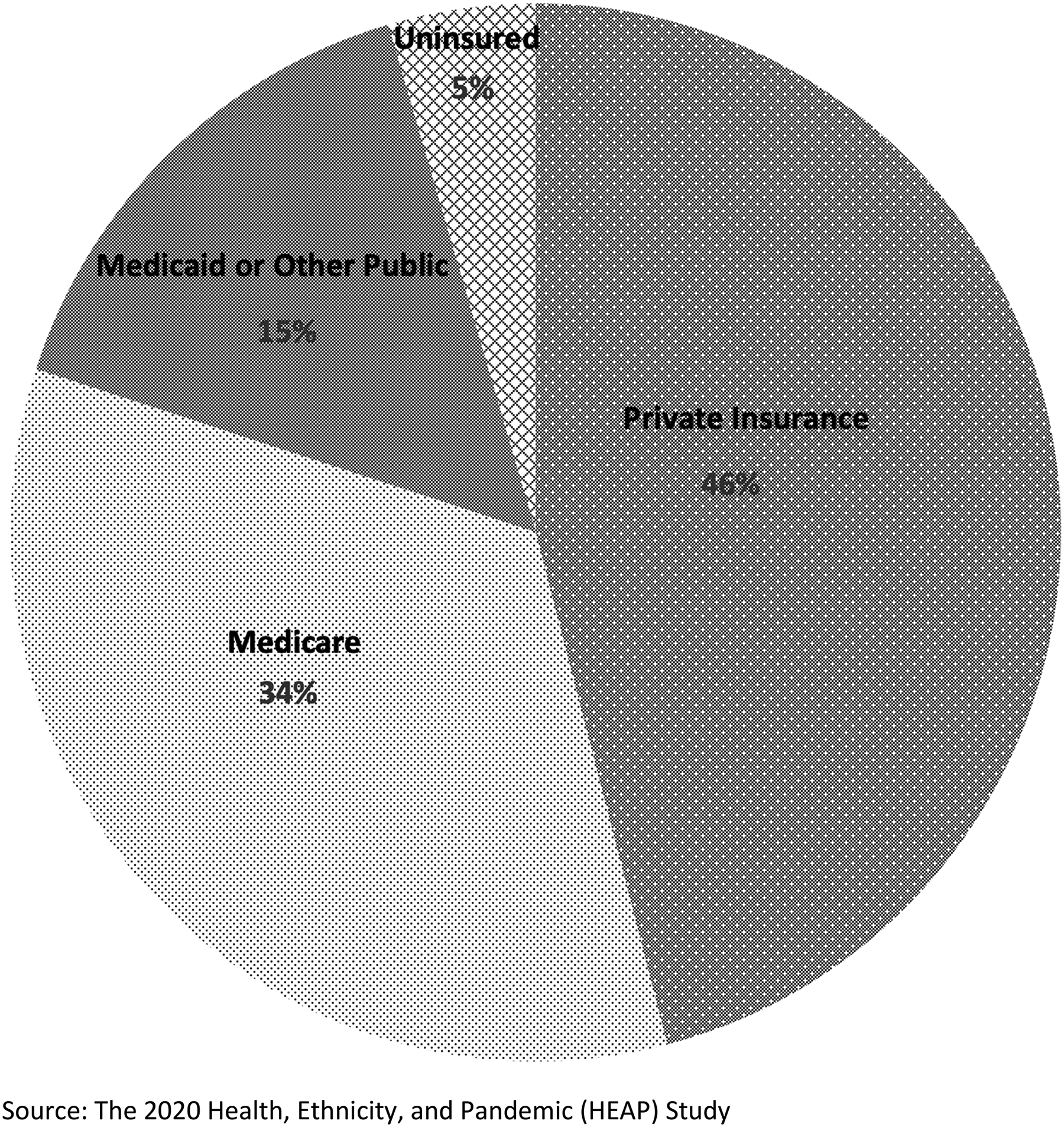
Use of Telehealth by Insurance Status during the Covid-19 Pandemic (n = 2554).
During the COVID-19 pandemic, in the entire sample, non-Hispanic East and Southeast Asians were significantly less likely to have utilized telehealth than non-Hispanic Whites (OR = 0.5, 95% CI: 0.3–0.8) (Table 2). Uninsured individuals were significantly less likely to have utilized telehealth than those covered by private insurance (OR = 0.4, 95% CI: 0.2–0.8). People living in a mobile home or a trailer were associated with a lower likelihood of using telehealth than those living in a single-family house, and the effect size was marginally significant (OR = 0.5, 95% CI: 0.2–1.0). People living in the East South-Central region were significantly less likely to use telehealth than those living in the New England region (OR = 0.4, 95% CI: 0.1–0.9). Those living in a community with < 90% broadband coverage were significantly less likely to utilize telehealth services (OR = 0.5, 95% CI: 0.3–0.8). Notably, although with marginal significance, we found that people who perceived higher racial discrimination (OR = 1.3, 95% CI: 1.0–1.6) were slightly more likely to use telehealth.
Differences in telehealth utilization by demographic characteristics and social determinants of health in the Health, Ethnicity, and Pandemic (HEAP) study sample a .
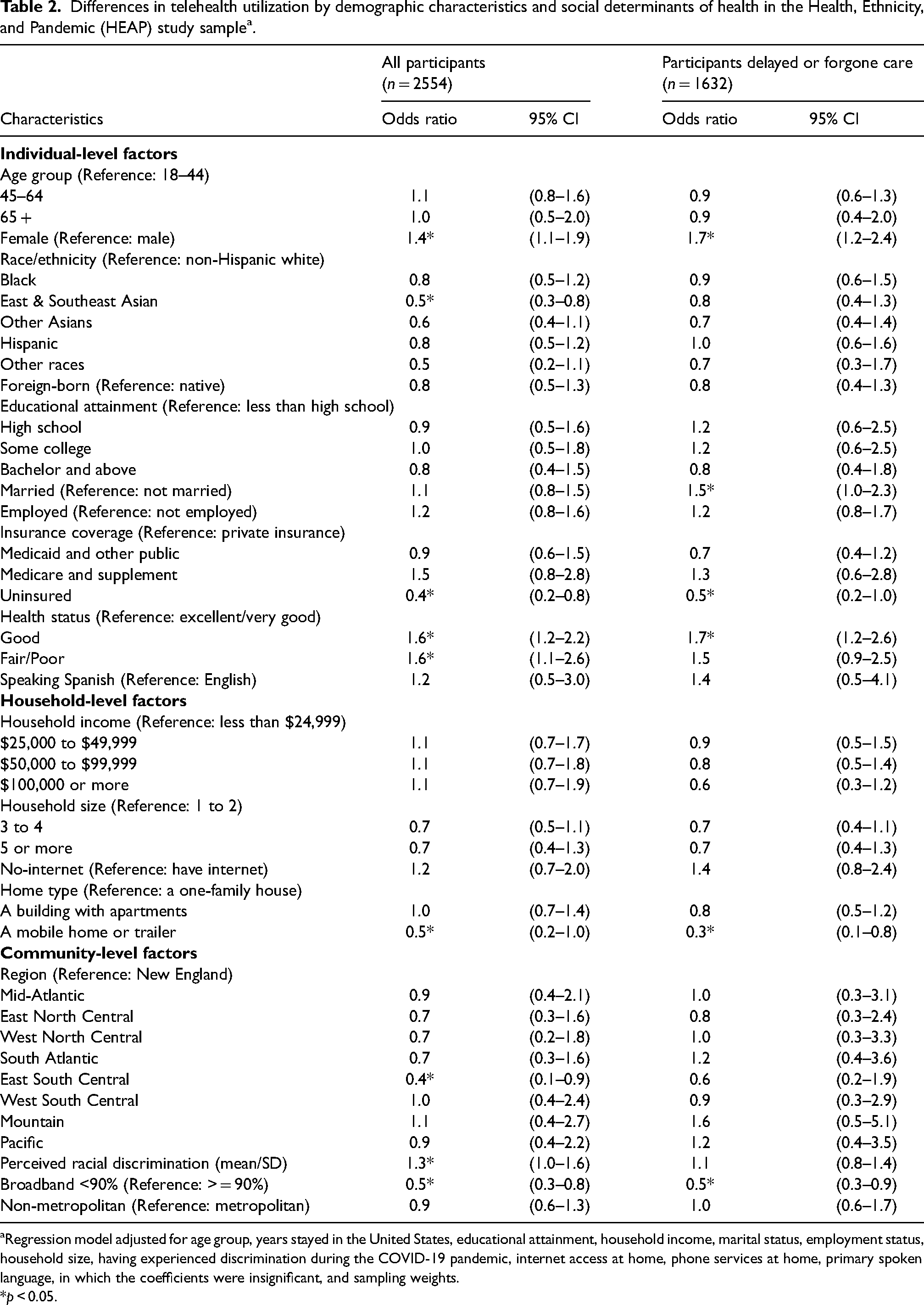
Regression model adjusted for age group, years stayed in the United States, educational attainment, household income, marital status, employment status, household size, having experienced discrimination during the COVID-19 pandemic, internet access at home, phone services at home, primary spoken language, in which the coefficients were insignificant, and sampling weights.
*p < 0.05.
In the subsample analysis, among people who delayed or foregone health care due to the pandemic, those being uninsured, compared with those covered by private insurance, were marginally-significantly associated with a lower likelihood of using telehealth services (OR = 0.5, 95% CI: 0.2–1.0). However, the association was attenuated, and the OR remained marginally significant. In addition, people living in a mobile home, or a trailer as compared to living in a single-family house were less likely to use telehealth (OR = 0.3, 95% CI: 0.1–0.8). Finally, people living in a community with limited broadband coverage (OR = 0.5, 95% CI: 0.3–0.9) were significantly associated with a lower likelihood of telehealth use (Table 2).
Discussion
The COVID-19 pandemic has significantly increased the use of telehealth services. This study demonstrated significant disparities in telehealth services among racial and ethnic minorities, particularly East and Southeast Asians. Asian American communities, especially East and Southeast Asians, have been subjected to increased rates of discrimination and hate crimes,18,19 in addition to the health and healthcare challenges faced by all Americans during the pandemic. The escalation in racism can lead to a decrease in seeking medical services for fear of bias and discrimination from medical professionals. 20 Asian Americans have been reported pre-pandemic to have underutilized health care, in particular mental health care due to cultural background, perceived racial discrimination and language barriers. 21 The same racial/ethnic group may also have underused telehealth care during the pandemic, posing a potential long-term health risk. The significant association between perceived racism and higher odds of telehealth utilization, as reflected by our study, underscores the need to address racism as a factor affecting health care access. A recent study documented significantly lower telehealth utilization rates for Black and Hispanic patients, elderly patients, as well as those living outside of metropolitan areas before the pandemic. 22 However, our study did not find that the elderly population, rural population, or Blacks or Hispanics were less likely to use telemedicine amidst the pandemic. 23 Due to budget constraint, we were not able to oversample other underserved groups such as rural population, elderly patients with chronic conditions, and undocumented immigrants, which may explain why we did not observe disparities in telehealth use among these groups in our study.
The literature revolving around telehealth expansion throughout the COVID-19 pandemic focused on social determinants of health and various disparities that create barriers to access.9,24,25 Studies found that mental health and private facilities were more equipped to handle the increase in demand for telehealth than primary care clinics and public facilities but still struggled with addressing the disparities within vulnerable populations.9,24 Our findings were consistent with the literature in that social determinants of health, such as being uninsured or underinsured, limited broadband coverage, and poor housing conditions, 26 constitute important barriers to telemedicine use.3,27 These relationships hold true even among people who already delayed or forgone care due to the COVID-19 pandemic. Governmental policies at the local, state, and national levels and health care institutions should begin addressing these resource disparities to improve both in-person and telehealth care. 24
Consistent with the literature documenting the salient role socioeconomic resources play in contributing to the utilization of telehealth services, 2 our study also found that economically disadvantaged populations were less likely to use telehealth services during the pandemic. For example, those uninsured, living in a mobile home or a trailer, and those living in the East South-Central region (Alabama, Kentucky, Mississippi, and Tennessee) were identified as less likely to use telehealth. The Mississippi Delta Region had been identified as the country's “least connected” area. 28 The geographic disparity observed in this study reinforces the importance of strengthening telehealth infrastructure in those states.
The Biden Administration has passed an infrastructure bill through the US Congress, which will expand high-speed broadband access across the country. Rural communities will benefit most from this plan that will provide 35% of rural Americans with access to affordable and reliable broadband. 29
Finally, consistent with a recent study, we found that women were more likely to utilize telehealth services compared to men during the pandemic,11,30 a gender pattern that could be of concern since men are at elevated risk for both COVID-19 mortality and certain pandemic-elevated health challenges such as opioid overdose.31–33 Healthcare professionals who plan to maintain or expand telehealth services (e.g. payers, hospitals, governments, etc.) should be aware of the gender differences in utilizing telehealth care.
There were several limitations in this study. First, the study used data from a cross-sectional survey, as such limited in inferring causal relationships. Second, recall biases and measurement errors may exist, given the self-reporting nature. Third, the telehealth use question could not differentiate telehealth due to lack of need or barriers to access, although we controlled for self-rated health status. In addition, the HEAP study did not ask respondents the specific type of telehealth services (i.e. phone-based, internet-based, video-based, or others) they received and did not collect information on respondents’ insurance plans and diseases; as such, the study was limited in a more in-depth understanding of the factors that influenced the utilization of different types of telehealth services. Fourth, the survey was only available in English and Spanish, which may not include certain minority groups who have issues accessing the internet and/or have language barriers (e.g. Asian respondents who speak an Asian language), compromising the generalizability of our study. Lastly, there may be unmeasured confounding factors, such as access to medical providers and whether local clinics or hospitals were closed because of the pandemic. Despite these limitations, this study is among the first to assess disparities in telehealth use across the United States by factors at the individual, household, and community levels, and, thus, would shed light on the barriers in expanding telehealth and inform the future design of more effective policies and interventions.
In summary, stark disparities exist in the utilization of telehealth services in the United States during the COVID-19 pandemic among socially disadvantaged populations such as East and Southeast Asians, uninsured populations, people living in the East South-Central region with limited broadband coverage, and people living in mobile homes. During the COVID-19 pandemic, the accessibility of telehealth services is crucial to many Americans. 34 There is a need to develop and implement more equitable policies and interventions at both the individual and community levels to improve access to telehealth services and reduce related disparities.35,36 When considering pandemic relief packages, policymakers should recognize the necessity to expand telehealth services to reach underserved populations who face various challenges in accessing needed healthcare services.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding support for the “Health, Ethnicity, and Pandemic” survey comes from The Center for Reducing Health Disparities at University of Nebraska Medical Center (Principal Investigator: Dr Dejun Su), The Chinese Economists Society (Co-Principal Investigator: Dr Zhuo Chen), and Calvin J. Li Memorial Foundation (Co-Principal Investigator: Dr Hongmei Li).