
Abstract
Introduction
This study aims to report the effect sizes of telemedicine treatments on the symptom domains of paediatric ADHD.
Methods
In this systematic review and meta-analysis, electronic databases, i.e. PubMed, Scopus, Web of Science and Embase, were searched for articles published up to December 2020. The inclusion criteria were as follows: children or adolescents diagnosed for ADHD or other hyperkinetic disorders; randomized controlled trials (RCTs); efficacy established with parents and teachers or self-rating scales at least for one of the following domains: inattention, cognitive function, hyperactivity, hyperactivity/impulsivity or oppositional behaviours. The risk of bias was assessed using the Cochrane risk of bias tool for RCTs.
Results
From 310 records reduced to 228 after removing duplicates, overall 12 studies were fulfilled our inclusion criteria. They consisted of 708 participants (358 with telemedicine intervention and 350 controls). The telemedicine interventions varied from computerized training programmes with phone calls to videoconferencing programmes, virtual reality classrooms or games. The most applicable method consisted of computerized training programmes with phone calls. Pooling results of all studies with available data on each subscale showed a significant effect of telemedicine on inattention/cognitive function (standardized mean difference (SMD) = 0.26, 95% CI: 0.16, 0.36), hyperactivity/impulsivity (SMD = 0.29, 95% CI: 0.06, 0.52), and oppositional behaviours (SMD = 0.72, 95% CI: 0.24, 1.20) subscales in ADHD. Almost all studies had an overall unclear risk of bias. The source of outcome assessment (parents, teachers or self-report questionnaire) was addressed as a potential confounding factor. In almost all symptom domains, the satisfaction from the treatment was higher in parents than in teachers.
Conclusions
The clinical effects of telemedicine on the treatment of ADHD showed a small effect size for inattention/cognitive function, hyperactivity/impulsivity and oppositional behaviours.
Introduction
Attention deficit hyperactivity disorder (ADHD) is a highly morbid neurobiological disorder and a major public health problem estimated to afflict up to 20% of children. 1 The effects of ADHD on the individual are pervasive, including academic and occupational difficulties,2–7 social skills problems 8 and divorce and separation. 4 Moreover, ADHD is often associated with co-accruing complications including major depression, bipolar disorder, anxiety disorders, antisocial disorders, and criminality,3,6,9 substance abuse,3,5,10–13 traffic accidents,5,7,14,15 posttraumatic stress disorder,3,10,11 and traumatic brain injury.16–18 Furthermore, individuals with ADHD are at higher risk for other comorbidities, including higher rates of hypertension, diabetes, asthma, migraine, epilepsy, obesity and dyslipidemias. 19 Thus, people with ADHD have an increased risk of premature death. 20 At the same time, ADHD is a highly treatable disorder and appropriate treatments can mitigate many of the ADHD-associated adverse outcomes. However, the high prevalence rate of ADHD, poor access to health services (including lack of health insurance), a scarcity of child and adolescent psychiatrists, lack of parental support and education on managing behavioural problems, limited dissemination of evidence-based practices among school professionals and primary care providers (PCPs), also worldwide COVID-19 outbreak and its complications, all contribute to low service utilization rates for childhood behavioural and mental health disorders. Geographic isolation and limited resources that characterize rural communities further complicate the problem of identification and appropriate management for children in rural communities.20–24 It seems that one highly promising approach to solve this problem is through using telemedicine.
There was an emergence of e-terms in the middle and late 1900s with the birth of the Internet. Among these was the term ‘eHealth’ that John Mitchell coined this term back in 1999.25,26 eHealth is an umbrella term covering a wide range of cost-effective and secure health services delivered through various information and communication technologies. 27 Telemedicine has been referred to as the most important revolution in healthcare since the arrival of modern medicine. Despite reporting the effectiveness of telemedicine in the treatment of ADHD in some studies, still there is no comprehensive result about it. It is not clear whether telemedicine is an effective therapy for paediatric ADHD or not, and what are its confounders. The differences in the effect of intervention between various methods of delivery, the frequencies, and duration of treatment sessions, and length of follow-up, as well as the differences between symptom domain outcomes after the intervention, remain to be determined. Therefore, the purpose of this study is to review the effects of telemedicine treatment on the symptom domains of paediatric ADHD.
Methods
Study selection
The protocol of this study was preregistered on the PROSPERO database (CRD42020186330). 28 We searched for studies up to December 2020 in the following databases: Pubmed, Web of Science, Scopus and Embase. It should be acknowledged that we did not limit our search only to purely medical items and we even used hybrid databases. A literature search was conducted to search studies investigating telemedicine in ADHD among children or adolescents under 18 years using combinations of the following keywords: ‘telemedicine’ AND ‘attention deficit hyperactivity disorder’ AND (‘Children’ OR ‘Adolescents’) and their alternative words based on MeSH (Supplemental Table S-1). Our search strategy in different databases is available in Supplemental Table S-2. Moreover, references from relevant articles were evaluated for potentially missed studies. We included data from the end of treatment, and when possible any long-term follow-up. After excluding duplicate publications, two researchers (MB and OY) independently screened abstracts of the retrieved studies to prevent missing studies. Likewise, studies that remained of interest were then screened based on their full text by MB and OY. Two review authors resolved any disagreements through discussion. Disagreements were consulted through discussion with a senior member of the research team (RK).
Studies included in the present meta-analysis and systematic review met the following criteria: (i) having a controlled trial design, (ii) published in peer-reviewed journals in the English or Farsi language, (iii) known cases of paediatric ADHD or other hyperkinetic disorders, (iv) including a clear description of the telemedicine treatment, (v) use of parent, teacher or self-reporting scales as outcome measures, (vi) presenting outcomes in terms of either ADHD symptoms or oppositional defiant disorder/conduct disorder (ODD/CD) symptoms for at least one of the following domains: inattention, cognitive function, hyperactivity, hyperactivity/impulsivity or oppositional behaviours ratings, or (vii) reporting data that allowed calculation of pre- to post-treatment effect sizes, and (viii) sample size larger than 10. Moreover, single-case studies were excluded. When the means (standard deviation, SDs) or odds ratio, 95% confidence interval (OR, 95%CI) from a given study were not available, or it was unclear whether the planned follow-up measurements were published or not, this information was requested by email to the authors. If the authors did not respond or did not provide the missing information, and if there was not sufficient information available based on the publication, the study was excluded from our meta-analysis. Furthermore, studies were screened for duplicate data based on authors, publication year, participant numbers and trial registration number (if available). When possible duplicate data were found, the authors were contacted to clarify whether the data sets were independent or not.
Data extraction/outcome measures
Data were first extracted by MB and checked by MY. Included studies were entered into a pre-piloted form for assessment of study quality and evidence synthesis. The following items were extracted from the included studies: publication date, country, population (number, and age), ADHD subtype, type of telemedicine treatment, medication use, method of delivery of telemedicine treatments, frequencies and durations of treatment sessions, outcome measures (at least in one the following symptom domains: (1) Inattention/cognitive function, (2) Hyperactivity/impulsivity, (3) oppositional behaviours), outcome measurement source and tool (assessed from parent, teacher or self-reporting scales with a validated ADHD rating scale (e.g. Diagnostic and statistical manual of mental disorders, 4th and 5th edition (DSM-IV and V) rating scale,29,30 Conners, 31 disruptive behaviour disorder (DBD) rating scales, 32 Vanderbilt ADHD rating scales (VADRS), 33 ADHD rating scales, 4th edition (ADHD-RS-IV), 34 strengths and weaknesses of attention deficit/hyperactivity symptoms and normal behaviours (SWAN) rating scale, 35 child behaviour checklist (CBCL), 36 etc.), comorbidities and time points of outcome measures. These variables were used as treatment endpoints at post-treatment and follow-up relative to baseline values.
Statistical analysis
Treatment effects were determined using standardized mean difference (SMD). They were calculated from the difference between the change scores divided by the pooled baseline standard deviation using the Hedges’ method and improvement rates using the Chinn formula.37,38 Data from intent-to-treat (ITT) analyses were preferred to data from modified-ITT or per-protocol (PP) analyses. Individual study weights were calculated as the inverse of the variance. Weighted averages and 95% CIs are pooled using the random-effects model. The I2 statistic (percentage of the total variation across studies due to heterogeneity) was calculated to determine the between-study statistical heterogeneity. Subgroup analyses across levels of qualitative confounders were conducted to explain some potential sources of heterogeneity. We also conducted a meta-regression analysis, using the metareg command in STATA, 39 to assess the association of SMDs with treatment duration/n. session and mean age of participants. Publication bias was assessed with Trim and fill plot, Egger's and Begg's tests.40,41 Statistical analysis was performed using STATA version 13 (StataCorp LP) software. Two-tailed significant probability was considered <0.05.
Quality assessment
The risk of bias was assessed using the Cochrane risk of bias tool for randomized controlled trials. It was structured into a fixed set of domains of bias, focusing on different aspects of trial design, conduct and reporting. Within each domain, a series of questions ‘signalling questions’ aimed to elicit information about features of the trial that are relevant to the risk of bias. Bias was assessed as a judgment (high, low or unclear) for individual elements from five domains (selection, performance, attrition, reporting and other). 42 Two researchers (MB and OY) independently assessed each study for quality. Any discrepancies were assessed by a third reviewer (MY) when necessary.
We also assessed the quality of included studies using the Critical Appraisal Skills Programme (CASP) checklist for randomized controlled trials. This checklist consists of 4 sections with 11 questions with ‘Yes/No/Can't tell’ answers. 43
Results
A total of 310 records were identified and reduced to 228 after removing duplicates. After screening and the application of the eligibility criteria, 12 articles44–55 met the inclusion criteria for at least one of the parameters and conditions resulting in 12 studies in the telemedicine arm and 10 studies in the control arm. Sibley et al. 47 and Lim et al. 46 had no control arm in their studies. Figure 1 presents the flow diagram of included and excluded articles of our review according to the preferred reporting items for systematic reviews and meta-analyses (PRISMA).
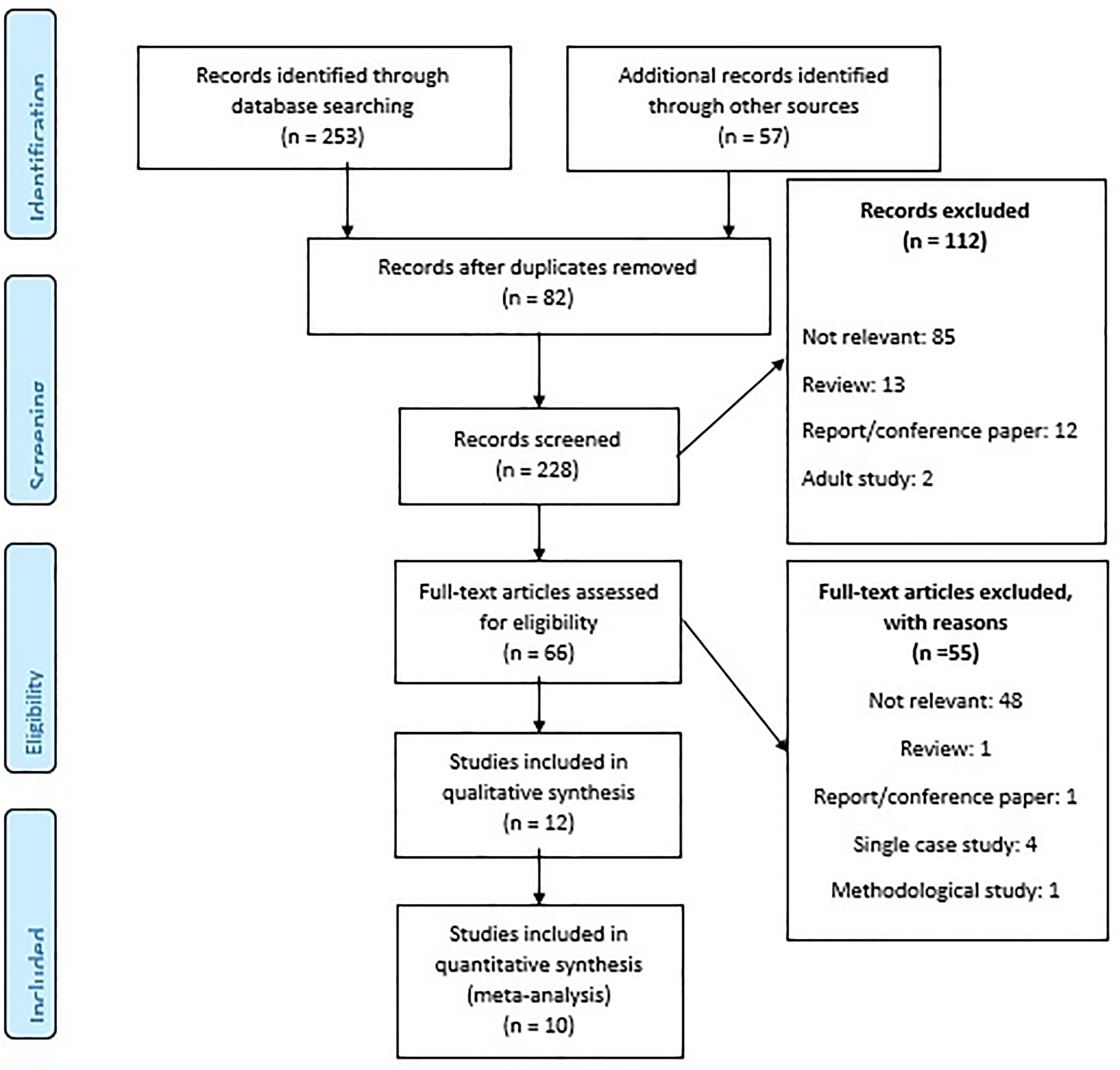
PRISMA flow diagram.
Study characteristics
Table 1 provides an overview of the study characteristics and outcome measures. Sample sizes ranged between 19 54 and 223; 52 five studies had a sample size of at least 50.44,48,49,52,55 The studies represent 708 children (358 telemedicine intervention, 350 controls). The age range was between 5 and 17 years. Most studies have focused on school-aged children. The exception was the study of Dupaul et al. 50 that was conducted among 3–6-year-old children. All studies were conducted in developed countries (United States, Singapore, Sweden, Netherland and Canada) and more than half of them were conducted in the United States.44,47,48,50,52–54
Characteristics of included studies.
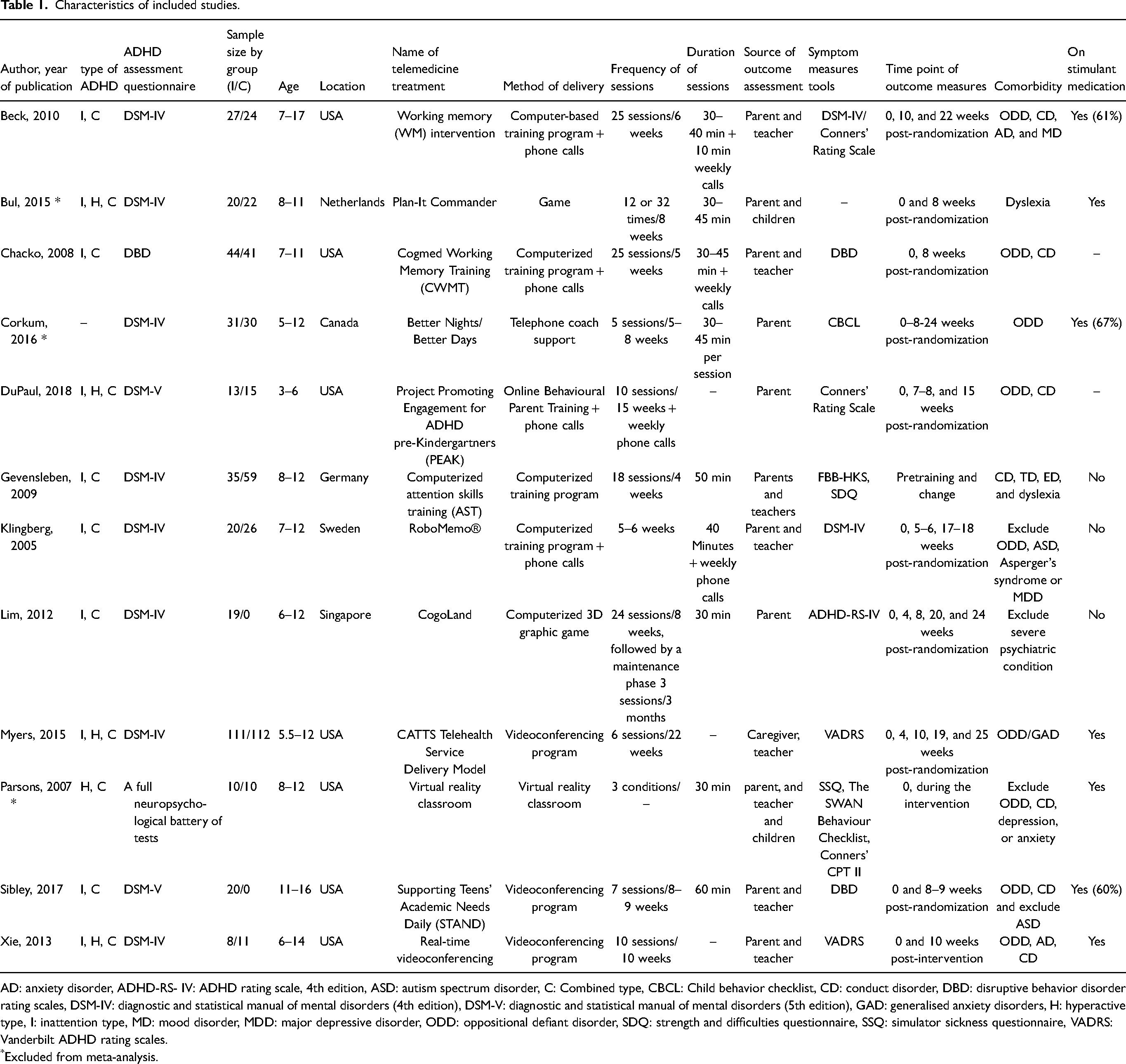
AD: anxiety disorder, ADHD-RS- IV: ADHD rating scale, 4th edition, ASD: autism spectrum disorder, C: Combined type, CBCL: Child behavior checklist, CD: conduct disorder, DBD: disruptive behavior disorder rating scales, DSM-IV: diagnostic and statistical manual of mental disorders (4th edition), DSM-V: diagnostic and statistical manual of mental disorders (5th edition), GAD: generalised anxiety disorders, H: hyperactive type, I: inattention type, MD: mood disorder, MDD: major depressive disorder, ODD: oppositional defiant disorder, SDQ: strength and difficulties questionnaire, SSQ: simulator sickness questionnaire, VADRS: Vanderbilt ADHD rating scales.
*Excluded from meta-analysis.
Method of delivery
As presented in Table 1, overall five methods of delivery for telemedicine intervention have been performed in clinical trials, the most applicable method consisted of computerized training programmes with phone calls.44,48,50,51 Following these programmes, videoconferencing programmes were also considered more frequently than other methods in telemedicine interventions in paediatric ADHD.47,52,54 Only one study had used a virtual reality classroom. 53
Intervention and study outcomes
In most studies, the ADHD assessment tool for the diagnosis was DSM-IV or V. Exceptions were the studies of Parsons et al. 53 and Chacko et al. 48 In all studies, the duration of each session was <1 h. The longest follow-up was 25 months in Myers et al.’s study. 52 Overall, nine studies reported other comorbidities such as oppositional defiant disorder (ODD), conduct disorder (CD), generalized anxiety disorder (GAD), etc. Exceptions were the studies of Klingberg et al., 51 Lim et al., 46 and Parson et al. 53 that excluded some psychological comorbidities.
We categorized symptom domains into three subgroupings: inattention/cognitive function subscale scores (N = 9), hyperactivity/impulsivity subscale scores (N = 7), and oppositional behaviours subscale scores (N = 5). As these varying N's indicated, most studies did not provide information on all of these scores. Data were not available on symptom domains in terms of our classification, for participants of the studies of Bul et al., 45 Corkum et al., 49 and Parson et al. 53 Thus, we included these studies only in our systematic review. Seven studies reported the medication treatment of participants before or within the period of the intervention.44,45,47,49,52–54
Quality assessment
Table 2 shows the risk of bias assessment of the included studies. Following the results of the Cochran Risk of Bias tool, almost all studies had an overall unclear or high risk of bias (Table 2). We also assessed the quality of included studies using CASP for randomized clinical trials. All results have supplied in Supplemental Table S-3.
Quality assessment of included studies.
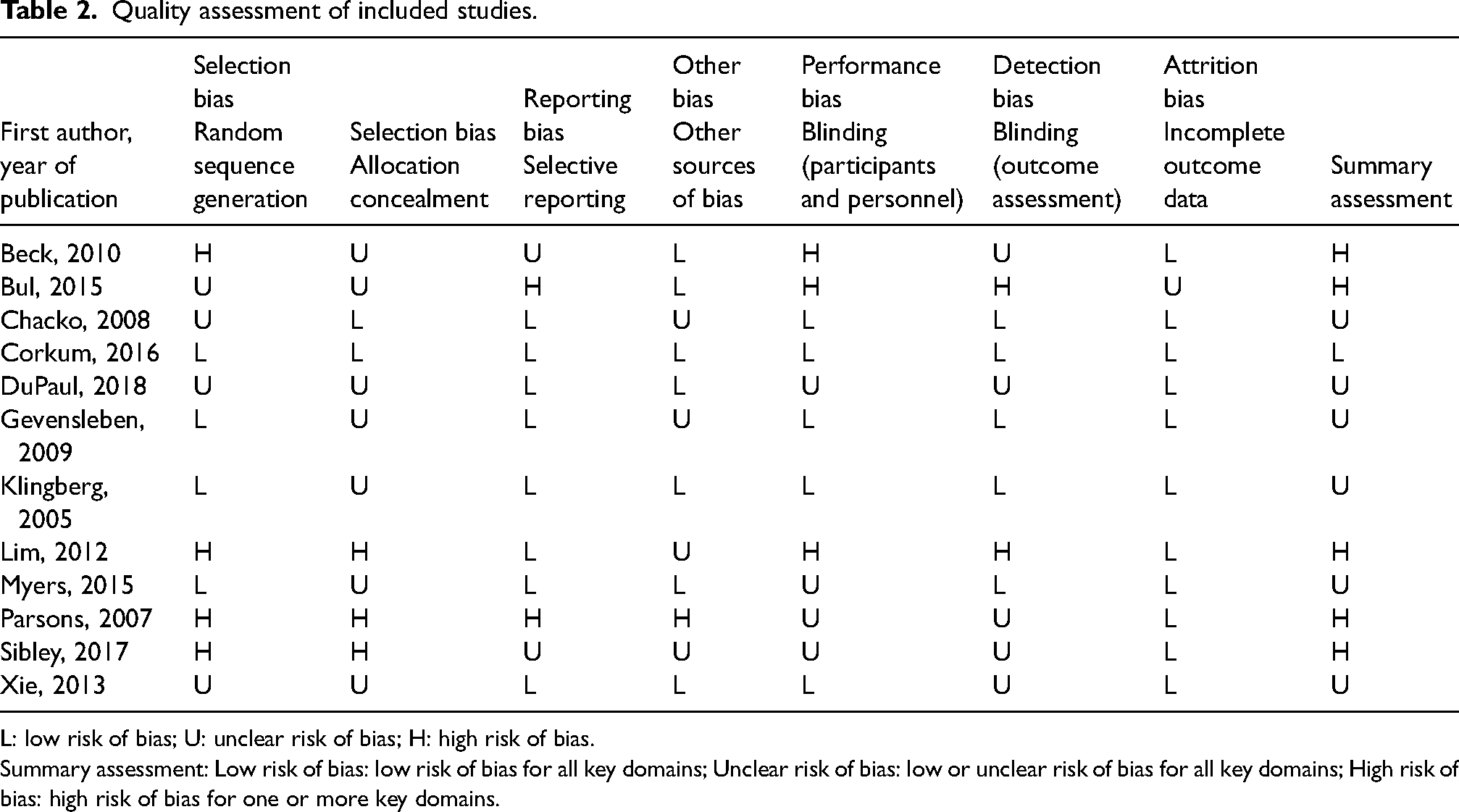
L: low risk of bias; U: unclear risk of bias; H: high risk of bias.
Summary assessment: Low risk of bias: low risk of bias for all key domains; Unclear risk of bias: low or unclear risk of bias for all key domains; High risk of bias: high risk of bias for one or more key domains.
Meta-analysis
Inattention/cognitive function
In total, nine studies had investigated the effect of telemedicine on inattention and cognitive function subscale during the periods of follow-up.44,46–48,50–52,54,55 Forest plots of SMDs and pooled effect sizes are illustrated in Figure 2. The pooling results of all studies showed a significant effect of telemedicine on reducing cognitive and inattention problems (SMD = 0.46, 95% CI: 0.21, 0.71, I2 = 68.90%). In a subgroup analysis to describe the potential source of heterogeneity, after discarding the pre−post RCTs (Lim et al., 46 Gevensleben et al., 55 and Sibley et al. 47 ) from meta-analysis, pooled SMD changed to 0.26 (95% CI: 0.16, 0.36, I2 = 0.0%, N = 6). Teachers were less satisfied with treatment compared to parents (0.26 vs. 0.27). Among the studies with participants on other medications, the effect of combination therapy was stronger than solely telemedicine intervention (0.27 vs. 0.23). High-quality studies graded by the Cochran tool showed more strength effect of telemedicine on inattention problems compared to studies with low or unclear bias (Table 3).
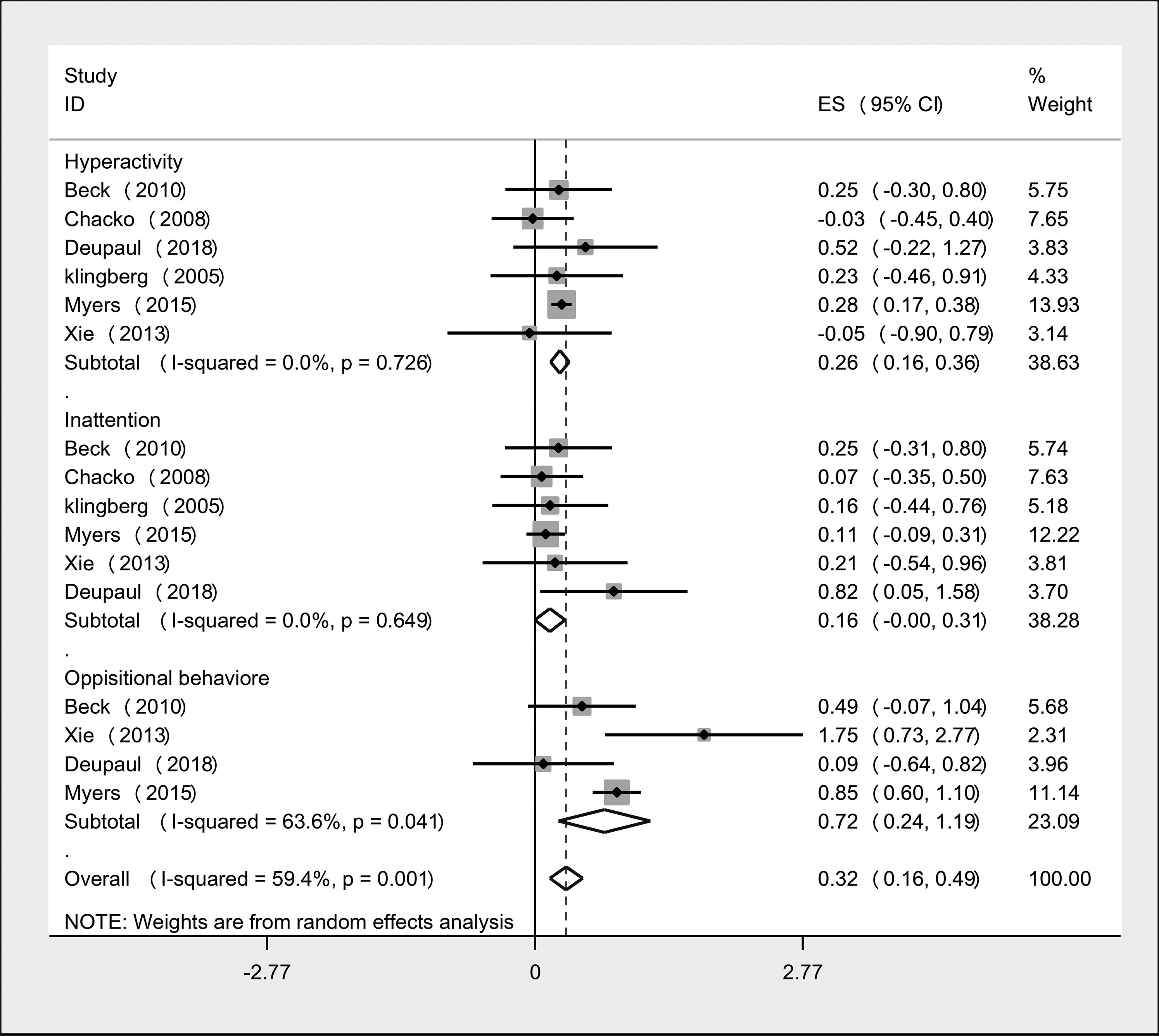
Forest plot of within-group analysis for inattention, hyperactivity, and oppositional behaviour parameter.
Analysis of the effect of type of study, medication use, study design, rater and clinical trial reporting quality on the efficacy of telemedicine in children and adolescents with Attention deficit hyperactivity disorder (ADHD).
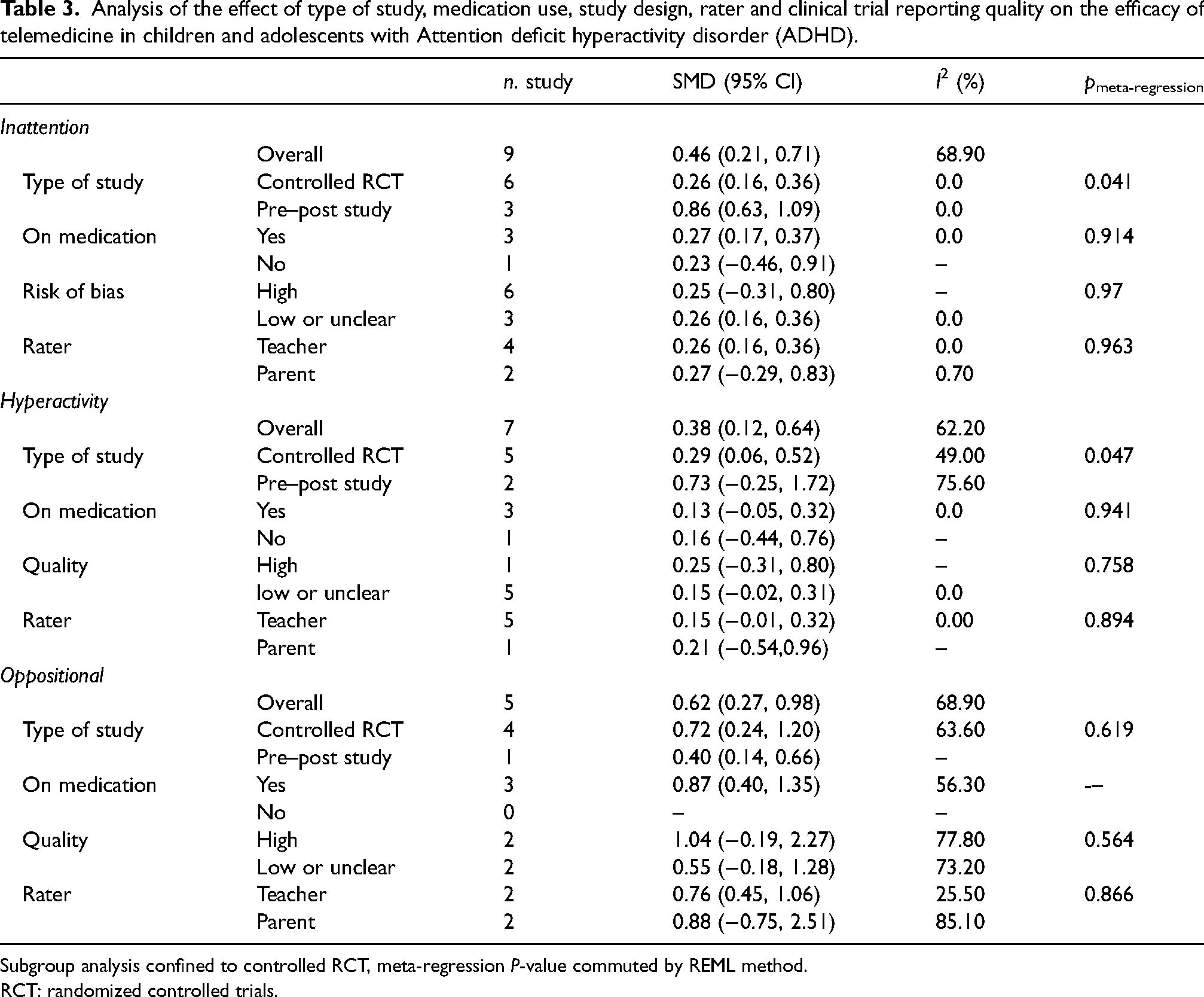
Subgroup analysis confined to controlled RCT, meta-regression P-value commuted by REML method.
RCT: randomized controlled trials.
Table 4 shows the meta-regression of study-specific SMDs with the mean age and the treatment duration. There was no statistically significant association between participants' mean age, treatment duration, and the number of sessions. This result may arise from the adequate length of treatment among all included studies or the small number of studies in the regression model.
Meta-regression analysis of the efficacy of telemedicine for Attention deficit hyperactivity disorder (ADHD).
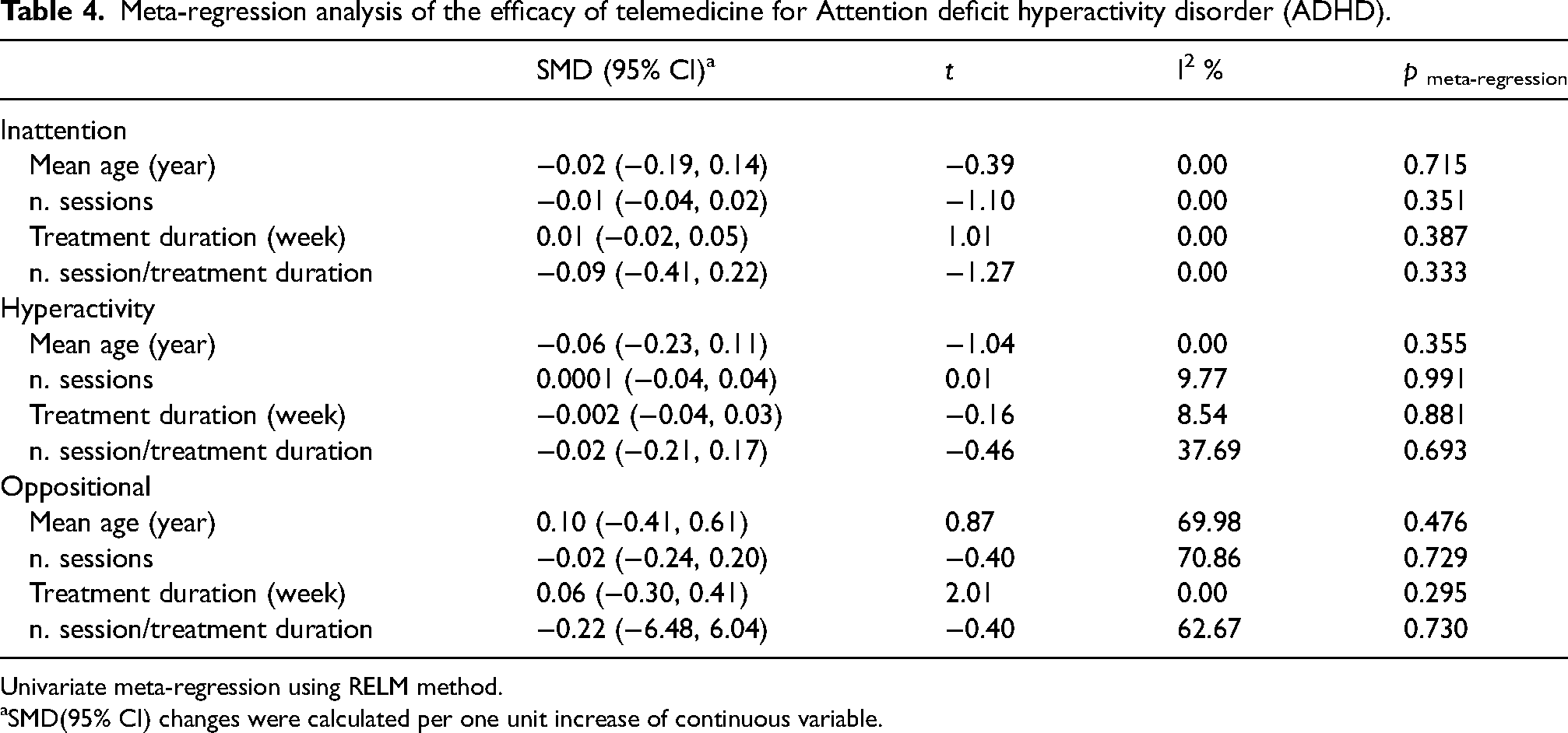
Univariate meta-regression using RELM method.
SMD(95% CI) changes were calculated per one unit increase of continuous variable.
There was no evidence of publication bias (Begg's p = 0.216, Eggers’p = 0.332). Likewise, the Trim and Fill plot showed no evidence of publication bias (Figure 3).
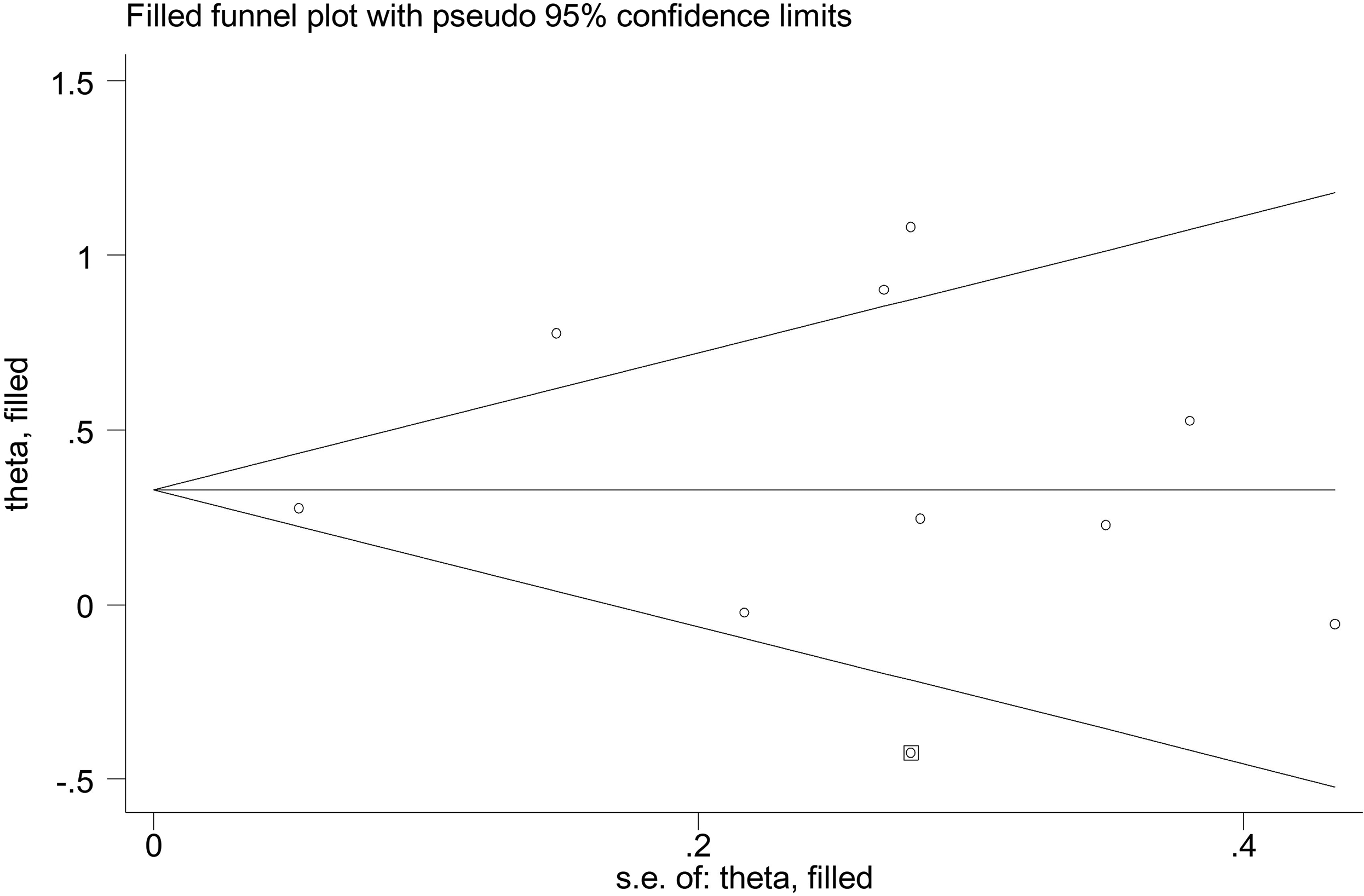
Funnel plot; efficacy of telemedicine on inattention/cognition symptom domain plotted against its standard error of the mean.
Hyperactivity/impulsivity
Overall, seven studies investigated the effect of telemedicine on hyperactivity/impulsivity during the follow-up period.44,46,48,50–52,54
The Forest plot of SMDs and pooled effect size are illustrated in Figure 2. Pooling results of all studies showed significant effect of telemedicine on reducing hyperactivity/impulsivity in total (N = 7, SMD = 0.38, 95% CI: 0.12, 0.64, I2 = 62.20%) and according to controlled RCTs (N = 5, SMD = 0.29, 95%CI: 0.06, 0.52, I2 = 49.0%).
The effect size for those that were not under medication (SMD = 0.16, 95% CI: (−0.44, 0.76) was larger than medication users (SMD = 0.13, 95% CI: (−0.05, 0.32). The effect of telemedicine in reducing hyperactivity was greater when it was rated by the parents compared to the teachers (0.21 vs. 0.15) (Table 3). Moreover, there was no evidence of publication bias (Begg's p = 1.0, Egger's p = 0.392) (Figure 4).
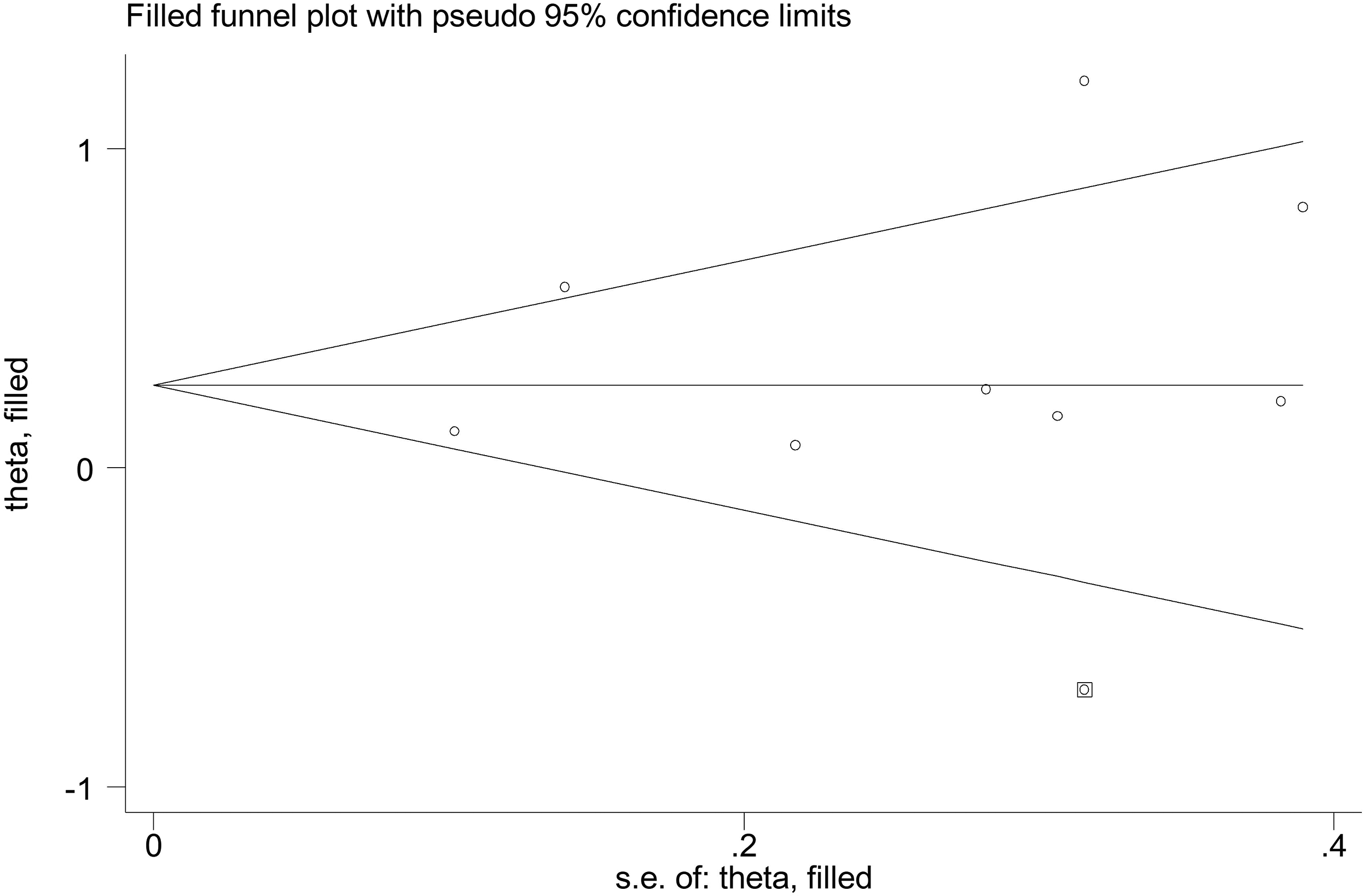
Funnel plot; efficacy of telemedicine for hyperactivity/impulsivity plotted against its standard error of the mean.
Oppositional behaviour
Five studies investigated the effect of telemedicine on defiant or oppositional behaviour during the months of follow-up.44,50,52,54,55
The Forest plot of SMDs and pooled effect size was illustrated in Figure 2. Pooling results of studies showed a significant effect of telemedicine on reducing oppositional behaviours totally (N = 5, SMD = 0.62, 95% CI: 0.27, 0.98, I2 = 68.90%) and according to controlled RCTs (N = 4, SMD = 0.72, 95% CI: 0.24, 1.20, I2 = 63.60%). In addition, there was no evidence of publication bias (Begg's p = 1.0, Egger's p = 0.884).
Discussion
The appropriateness of implementing telemedicine is often poorly informed or uninformed. Thus, there is a need for a high-quality evidence-based result to support the sustainable integration of telemedicine into routine clinical care. 56 This meta-analysis aimed to investigate the effects of telemedicine on various ADHD symptom domains of current literature to inform future research. The focus in telemedicine research emerges to have changed from technical-related applications to clinical use and evaluation. 57 While there are several studies on technical-related applications of telemedicine in ADHD children,58–62 this trend has been changed towards a patient- and illness-centred focus especially in RCTs. This review found that the most common telemedicine intervention in ADHD children was computerized training programmes with phone calls; however, the trends in eHealth are changing rapidly toward mobile applications, which would influence future study designs. 63
Consistent with previous reviews of a similar nature, pooling results of all studies that had available data on each subscale showed the significant effect of telemedicine on inattention/cognitive function, hyperactivity/impulsivity and oppositional behaviours subscales in children and adolescents with ADHD, although most of the included studies in this review were small. We must also consider that almost all studies used parent and teacher questionnaires instead of therapist assessments, except Myers et al. 52 which introduced bias in our review.
While combination therapy showed better improvements versus telemedicine intervention in the inattention subscale, telemedicine intervention solely, represented better improvements in the hyperactivity subscale. This difference might reflect the difference in the nature of symptom domains, even types of ADHD (inattention, hyperactivity or combined) or types of medications in children. This finding needs to be more investigated in future studies. On the other hand, we should consider that most of the studies in our meta-analysis employing a combined treatment first used optimal dosing procedures and then added telemedicine interventions, limiting the room for further improvement. Although more evidence is needed to show the specific effect of telemedicine on the treatment of children and adolescents with ADHD, it seems that it could be solely an effective intervention for treatment without other medications, especially in hyperactivity symptoms. Furthermore, a combination of telemedicine interventions with other non-pharmacological treatments might reveal some new points of view in the treatment of ADHD specifically in inattention symptoms.
In almost all symptom domains, parents were more satisfied with the treatment compared to teachers. Since the informant agreement on ratings of ADHD symptoms has been low, it is an important issue in ADHD research.64,65 While a recent study indicated that parents were as sensitive as teachers to detect changes in ADHD symptoms, 66 some authors suggest that parent's ratings are less informative for assessing ADHD symptoms than teachers' ratings. 67 Some other studies on the efficacy of short-acting methylphenidate found higher effect sizes for teachers than for parents on rating scales, which is not surprising since short-acting methylphenidate often does not cover home situations.68,69 Our results found larger effect sizes for parents than teachers with telemedicine treatment on all outcome domains. If we assumed that parents were as sensitive as teachers to detect changes in ADHD symptoms, this result might be hypothesized that a combination of stimulant therapy and telehealth interventions could cover both home and school situations in school-aged children with ADHD; however, more evidence is needed to support this hypothesis.
There was no statistically significant association between participants' mean age and reduction in symptom domains of ADHD. However, this finding needs to be viewed with caution due to the small number of studies in different subscales.
It has been suggested that the effectiveness of psychosocial treatments depends on the duration of treatment.70,71 However, in our meta-analysis, there was no statistically significant association between treatment duration and improvement in the symptom domains. This result may arise from the short duration of interventions as the length of interventions varied between 5 and 22 weeks in included studies.
Due to the small number of trials and the diversity of interventions, it is difficult to draw definite conclusions about the effectiveness of telemedicine. Furthermore, all included trials were conducted in developed countries, affecting the applicability of the results in developing countries and highlighting a gap in the current knowledge. Moreover, trials eligible for subgroup meta-analysis were relatively low, limiting statistical power. On the other hand, as most included studies were RCTs, there was a low risk of bias for participant randomization. However, selection bias could not be avoided as only two studies achieved sufficient allocation concealment. Besides, only five studies achieved participant blinding, and blinding of treatment conditions was not possible in more than half the studies (Table 2). Although the studies had different outcome measures that constrained meta-analysis, overall findings support telemedicine use for a relatively mild improvement in ADHD outcomes.
Strengths and limitations
The studies examined in our meta-analysis often suffered from low statistical power because of the small sample size as well as multiple scattered outcome measures and variation in time points. Meta-analysis enhances the power by combining the results of all underpowered studies and therefore yields statistically better-informed conclusions. This study includes literature available from interdisciplinary databases. While some previous systematic reviews have been focused on non-medical libraries entirely. 72 Besides, we extracted quantitative data on symptom domains and conducted a meta-analysis on them. However, some previous studies have been focused on qualitative data.72–74 Since the control groups encountered in our literature retrieval were very different with variation from intervention control, attention control to waitlist control), the control groups were incomparable and it would have yielded results that would have been difficult to interpret, if not misleading.
Conclusions
This meta-analysis showed a small effect size of telemedicine in the treatment of ADHD for inattention/cognitive function, hyperactivity/impulsivity and oppositional behaviours. Although teachers were less satisfied with treatment compared to parents, we found no statistically significant association between other factors including participants' mean age, treatment duration and the number of sessions. Further high-quality RCTs are needed to clarify the combination effect of telemedicine as an alternative intervention with other pharmacological or non-pharmacological interventions. In addition, assessing other potential confounding factors and challenges of home-based or school-based eHealth interventions may be promising.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X211045186 - Supplemental material for A meta-analysis on the effect of telemedicine on the management of attention deficit and hyperactivity disorder in children and adolescents
Supplemental material, sj-docx-1-jtt-10.1177_1357633X211045186 for A meta-analysis on the effect of telemedicine on the management of attention deficit and hyperactivity disorder in children and adolescents by Maryam Bemanalizadeh, Maryam Yazdi, Omid Yaghini, and Roya Kelishadi in Journal of Telemedicine and Telecare
Footnotes
Acknowledgements
The authors are very grateful to the Research Institute for Primordial Prevention of Non-Communicable Disease staff for their kind support
Authors’ contribution
RK, MB and OY have contributed to the design of the work, systematic search and screening, data extraction, drafting and the final revision of the manuscript. MY has contributed to data extraction, data analysis, interpretation and drafting of the article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Isfahan University of Medical Sciences.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.