
Abstract
Introduction
The global pandemic has raised awareness of the need for alternative ways to deliver care, notably telehealth. Prior to this study, research has been mixed on its effectiveness and impact on downstream utilization, especially for seniors. Our multi-institution study of more than 300,000 telehealth visits for seniors evaluates the clinical outcomes and healthcare utilization for urgent and non-emergent symptoms.
Methods
We conducted a retrospective cohort study from November 2015 to March 2019, leveraging different models of telehealth from three health systems, comparing them to in-person visits for urgent and non-emergent needs of seniors based on International Classification of Diseases, 10th edition diagnoses. The study population was adults aged 60 years or older who had access to telehealth and were affiliated with and resided in the geographic region of the healthcare organization providing telehealth. The primary outcomes of interest were visit resolution and episodes of care for those that required follow-up.
Results
In total, 313,516 telehealth visits were analysed across three healthcare organizations. Telehealth encounters were successful in resolving urgent and non-emergent needs in 84.0–86.7% of cases. When visits required follow-up, over 95% were resolved in less than three visits for both telehealth and in-person cohorts.
Discussion
While in-person visits have traditionally been the gold standard, our results suggest that when deployed within the confines of a patient’s existing primary care and health system provider, telehealth can be an effective alternative to in-person care for urgent and non-emergent needs of seniors without increasing downstream utilization.
Introduction
The quality and cost-effectiveness of telehealth for seniors – adults aged 60 and above – has been heavily debated in addition to being touted as an opportunity to avoid costly Emergency Department (ED) visits within the general population for low acuity or urgent care (UC) needs.1–5 An estimated 30% of all ED visits in the US are for non-urgent conditions, many of which can be addressed through telehealth. 6 The pandemic coupled with the rise of direct-to-consumer (DTC) models of telehealth in recent years, providing on-demand access to online providers, has also accelerated its adoption. 7
While recent COVID-19 events have put telehealth in the national spotlight, research on outcomes and utilization trends remains limited. The results are still mixed as to whether telehealth is effective in reducing downstream utilization (i.e., additional visits, procedures, etc.) One of the only studies addressing this issue found that while telehealth was convenient and increased access, it resulted in increased new utilization and no reduction in overall spending. 8 In particular, Ashwood et al. found that up to 88% of telehealth services were for new utilization, suggesting telehealth led to additional follow-up visits or “episodes of care” with greater number of visits and calling into question its quality and cost-effectiveness. 8 While Ashwood’s study focused on acute respiratory infections for a health maintenance organization in the United States, these findings suggest telehealth services, when delivered in a DTC model, increased utilization.
One area where telehealth may be impactful is in addressing the urgent and non-emergent healthcare needs of seniors. Urgent and non-emergent needs are typically defined as clinical conditions in which a short delay would not increase the likelihood of an adverse outcome (e.g. flu-like symptoms, skin rashes, fever, urinary tract infection (UTI), cough).
Studies have examined the impact of DTC models of telehealth and single-site studies have addressed the impact of telehealth on urgent and non-emergent needs of seniors; yet few, if any, multi-site studies have evaluated common outcomes across distinct telehealth delivery models. Our study aims to address the impact of telehealth services for urgent and non-emergent symptoms for seniors across three healthcare systems.
Methods
Study design
We identified a retrospective cohort with three different health systems in the United States using telehealth to address urgent and non-emergent needs for seniors (as defined in our study as individuals aged 60þ). Two health systems (Kaiser Permanente Southern California and Spectrum Health in Grand Rapids, Michigan) had structured models, providing telehealth services for a set of established conditions as defined by the health system, and one health system (Jefferson Health in Philadelphia, Pennsylvania) utilized an all-calls approach where telehealth services were deployed as an extension of the ED for any condition. Since this was a retrospective study, we examined each health system’s telehealth model as it was designed and staffed. In the Kaiser Permanente model, clinical services were provided by a medical provider (MD) or nurse practitioner (NP), and in the Spectrum Health model, it was provided by an NP or physician assistant (PA). In the all-calls approach, patients called Jefferson Health to request clinical services and were offered a telehealth visit by a physician Doctor of Medicine/Doctor of Osteopathic Medicine (MD/DO) as an alternative to in-person care when appropriate. Each health system utilized different workflows to deploy telehealth services based on their population, with Kaiser Permanente using video, telephone, and E-visits, Spectrum Health utilizing video and E-visits, and Jefferson Health using video visits only (see Figure 1). Our goal was to study the impact of these different delivery models on common clinical outcomesand healthcare utilization across similar cohorts.
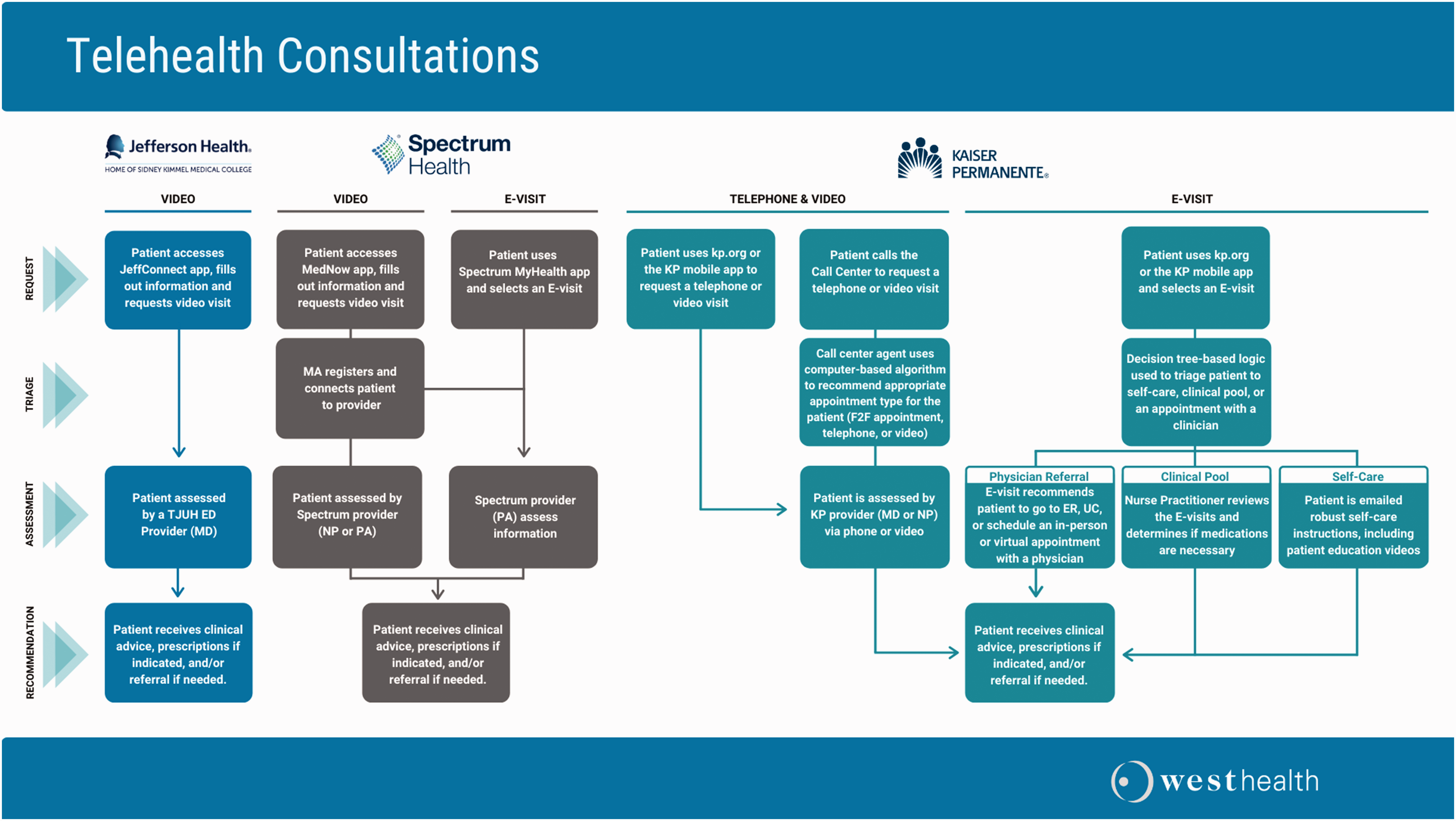
Telehealth consultation workflows.
Inclusion criteria
Across each of the three organizations, we included non-institutionalized ambulatory adults aged 60 years or older who had access to telehealth, were affiliated with the healthcare organization (i.e. established patient), and resided in its geographic region.
Study period and data source
The study period was from November 2015 through March 2019, and captured urgent and non-emergent conditions based on International Classification of Diseases, 10th edition (ICD-10) coding for all patients 60þ years of age and eligible for telehealth. Examples of urgent and non-emergent conditions based on these criteria included upper respiratory infection, skin problems, UTIs, and gastrointestinal problems, to name a few. Data for each of the participating sites originated from electronic health records containing demographic, clinical, and utilization data.
Cohort selection
Data from the three sites were categorized into two cohorts: telehealth and in-person. To be eligible for the telehealth cohort, the initial (index) visit had to be facilitated via telehealth. Subsequent follow-up visits (within 30 days of index visit) may be a combination of telehealth or in-person and still be included in the telehealth cohort.
For the in-person cohort, index visit was defined by an in-person primary care or office visit. Similar to the telehealth cohort, subsequent follow-up visits after index visit (within 30 days of index visit) may be telehealth or in-person and still included in the in-person cohort.
In both cohorts, index visit was defined as the first visit during the study period with no prior visit within 30 days. Furthermore, to be considered for inclusion in both study cohorts, patients were required to have up to one month of data prior to index encounter to capture prior medical history and to ensure cohorts were comparable in demographic and clinical characteristics (see Figure 2).
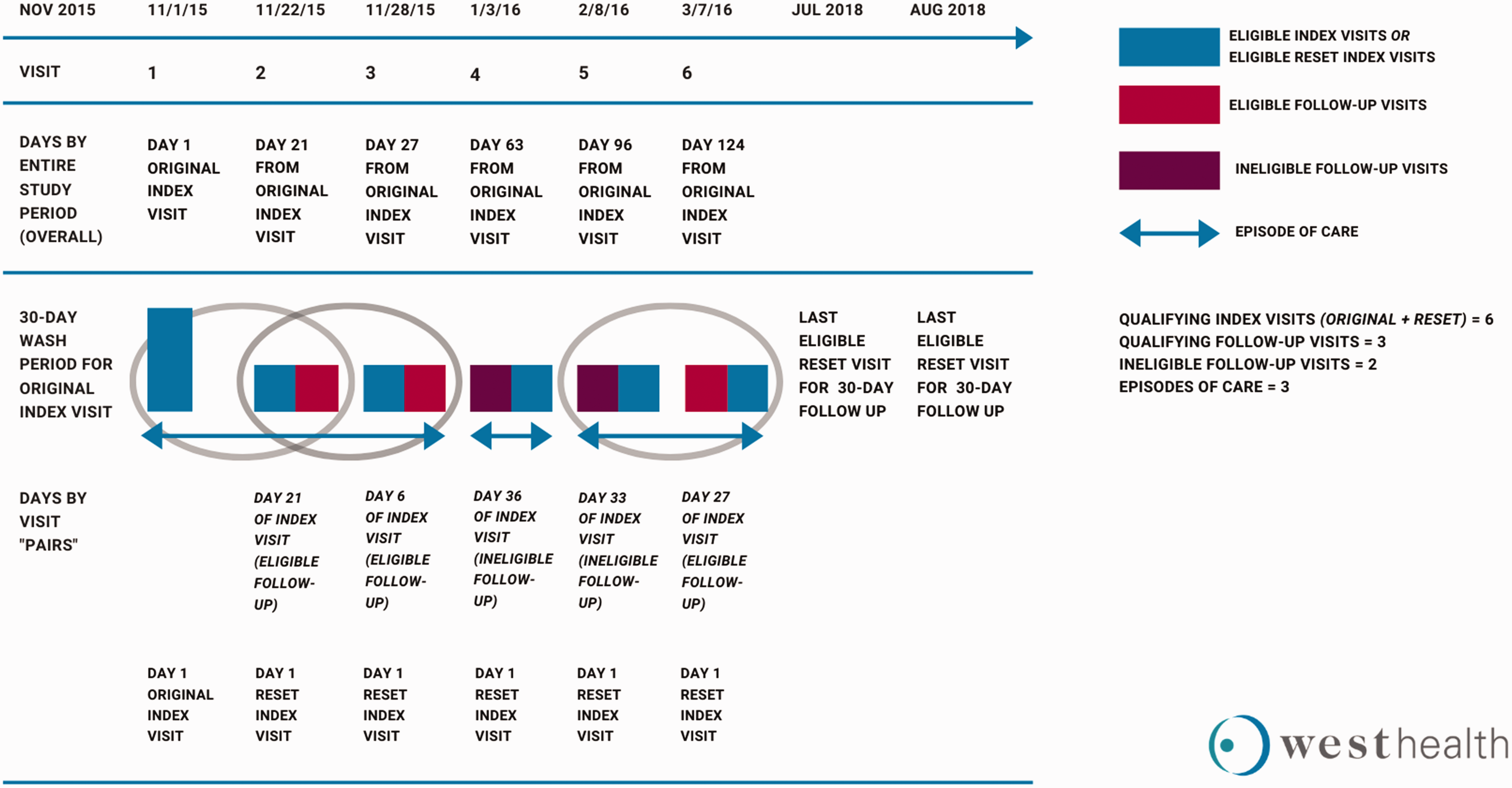
Sample analysis – visit level and episodes of care.
Outcomes
Our primary outcomes of interest were visit resolution and episodes of care. Visit resolution was defined as an index visit with no follow-up within 30 days for the same condition. An episode of care was defined as the number of visits, after the index visit, required to resolve the urgent and non-emergent condition. An episode was considered “complete” once at least 30 days passed before an additional visit (either telehealth or in-person) took place. 9 , 10 To categorize the reason for visit, we utilized diagnosis type based on ICD-10 codes. Visit type was documented by each health system to define whether the visit was conducted in-person or via telehealth.
The diagnosis code for the index visit was used as criteria to determine if subsequent visits were part of the same episode of care.
Additionally, to be consistent with criteria as defined by the Agency for Healthcare Research and Quality, we utilized ED and/or UC visits 30 days following a telehealth visit as a marker for additional utilization. 11
Statistical analysis
Given the different telehealth delivery models across the three organizations, we analysed data from each organization. Furthermore, since the number of tele-health visits was significantly smaller than eligible in-person visits, we utilized a 10:1 ratio of in-person and telehealth visits, consistent with prior research on recommended statistical practice based on simulation studies. 12 In this approach, we randomly selected a matched sample of in-person visits to telehealth visits based on similar demographic and clinical characteristics, ensuring the random sample of in-person visits did not exceed a ratio of 10 in-person visits to one telehealth visit across the study cohorts.
Analysis was conducted with each visit serving as a potential index visit. Visits following an index visit for the same condition within 30 days were flagged as an eligible follow-up visit. Both the telehealth and in-person cohort were matched on clinical and demographic characteristics (e.g. age, race, gender, Charlson Comorbidity Index (CCI)) and a Pearson chi-squared test was conducted on visit resolution to assess significant clinical or demographic differences between the two groups.
Descriptive statistics, including frequencies, means, medians, and ranges are reported for each organization to address visit resolution rates and episodes of care. To evaluate differences in number of visits per episode of care we utilized Poisson regression models controlling for covariates including age, gender, race, marital status, and CCI. Due to sample size limitations, only Kaiser Permanente data were analysed using the Poisson regression model. All statistical analyses were conducted using Alteryx™ and RStudio™.
Institutional Review Board approval
All three participating sites applied for and received Institutional Review Board approval through their respective institutions.
Results
Across the three health systems, we examined 313,516 qualifying index visits for telehealth (Kaiser Permanente: 313,241 visits; Jefferson Health: 135 visits; Spectrum Health: 140 visits) (see Table 1). Each of the three sites addressed a variety of urgent and non-emergent clinical conditions, all of which were categorized based on diagnosis-related groups (DRGs). For Kaiser Permanente, telehealth visits fell into 20 predefined clinical conditions, Jefferson Health into eight clinical conditions (which were later categorized according to similar DRGs based on the other sites pre-defined conditions), and Spectrum Health, which fell into 13 pre-defined conditions.
Cohort characteristics.
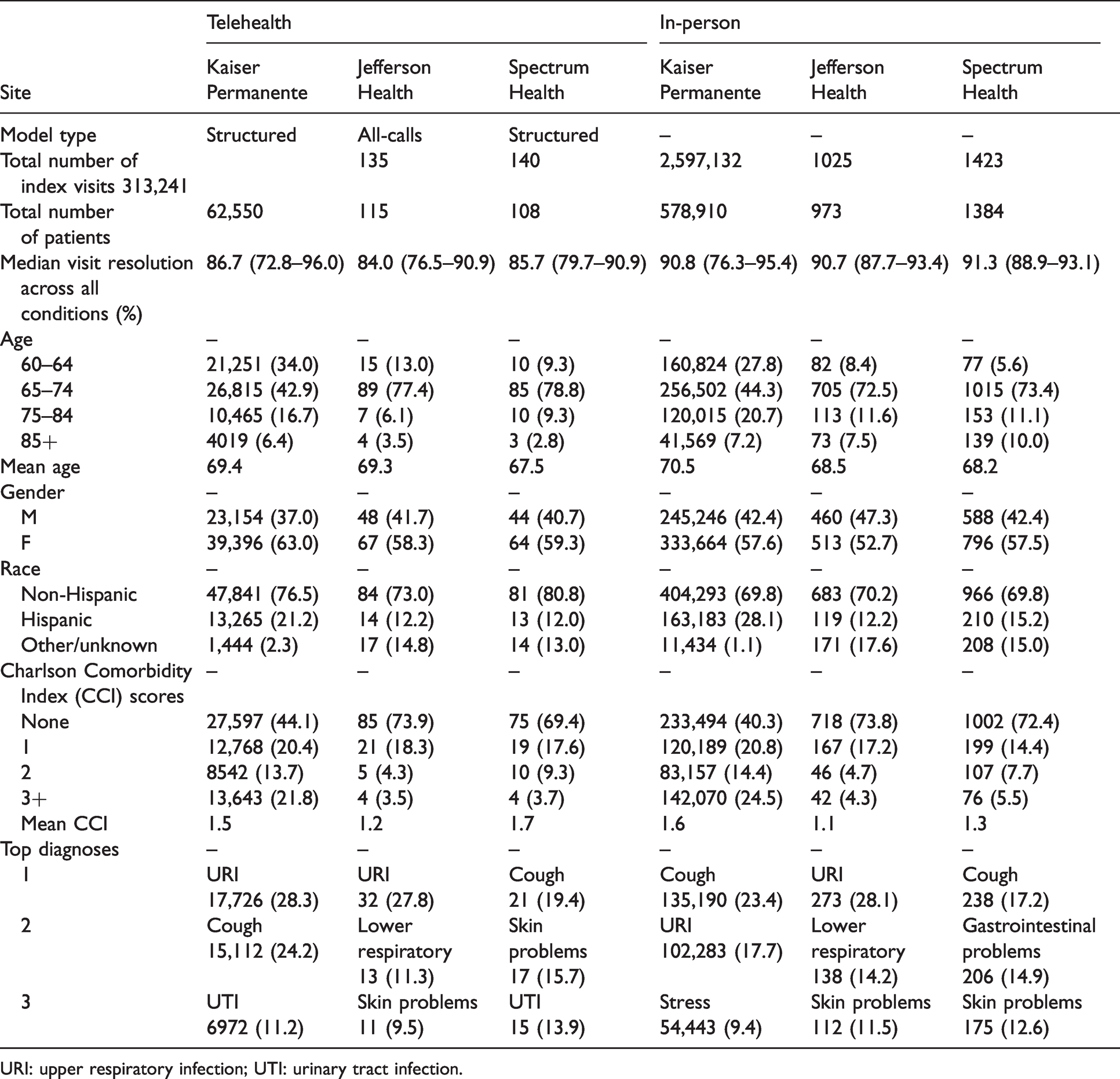
URI: upper respiratory infection; UTI: urinary tract infection.
Visit resolution
Across all three sites telehealth index encounters were successful at resolving urgent and non-emergent needs, as median visit resolution ranged from 84.0% to 86.7% (see Table 1).
At Kaiser Permanente, median visit resolution was achieved across 20 urgent and non-emergent conditions at a rate of 86.7% (72.8–96.0%) compared to an in- person visit resolution of 90.8% (76.3–95.4%) (see Table 1). We found the highest resolution rates for chills, allergy, muscle spasms, and vaginal discharge/itch, all of which were resolved on initial visit at least 90% of the time (See Supplemental Table 1). Results were similar to the in-person cohort where these conditions were also resolved at least 90% of the time.
The clinical condition with the highest degree of difference between the two cohorts was for headache/migraine, where median in-person visits were resolved 90.9% of the time compared to 77.7% in the telehealth cohort (See Supplemental Table 1).
Jefferson Health had a total of 135 eligible telehealth visits within the study period and 1025 eligible in-person index visits across eight different conditions. For Jefferson Health, median visit resolution for telehealth visits was 84.0% (76.5–90.9) across all urgent and non-emergent conditions (see Table 1). This was less than the cohort of in-person visits, where median visit resolution was 90.7% (87.7–93.4) across the same conditions (See Supplemental Table 2).
The greatest difference between the in-person and telehealth cohort for Jefferson Health was for gastrointestinal disorders, where median visit resolution in the telehealth cohort was 69.2% compared to 90.6% for in-person (See Supplemental Table 2). Across six of eight clinical conditions, in-person index visits were more likely to result in visit resolution than telehealth, although it should be noted that when telehealth was associated with higher visit resolution (skin/subcutaneous and other conditions), sample sizes were too small to draw firm conclusions.
Spectrum Health deployed telehealth services across 13 different clinical conditions with a total of 140 eligible telehealth visits included in our telehealth cohort and 1423 included in the eligible in-person cohort. In this model, telehealth median visit resolution was 85.7% (79.7–90.9) across all urgent and non-emergent conditions (see Table 1). These results are similar to the cohort of in-person visits where the median visit resolution rate was 91.3% (88.9–93.1).
For Spectrum Health, median visit resolution was highest for vaginitis, oral pain, and UTIs within the tele-health cohort (See Supplemental Table 3. Similarly, the highest resolution rates within the in-person cohorts were for UTI, oral pain, and upper respiratory infections. In all but two of 13 clinical conditions (vaginitis and oral pain), visit resolution rates were slightly higher for in-person than tele-health, although it should be noted that where telehealth was associated with higher resolution rates, sample sizes were too small to draw reasonable conclusions (See Supplemental Table 3).
Episodes of care – descriptive
For visits that were not resolved in a single visit, we also examined subsequent follow-up visits or “episodes of care” to understand the number of visits required to achieve resolution (see Table 2) Generally, across all three participating organizations, only a small proportion of eligible visits required follow-up (12.9%, 16.0%, and 14.0%, respectively) and when follow-up did occur, mean episodes of care. for the telehealth cohort comprised 2.42 (2.15–2.85), 2.50 (2.11–2.73), and 2.39 (2.08–2.65) visits, respectively, across each of the three sites. In all three organizations, episodes of care that started with an index telehealth visit required additional follow-up visits to achieve resolution than the in-person cohort; however, differences between the two cohorts in frequency were less than half a visit.
Episodes of care (EOC).
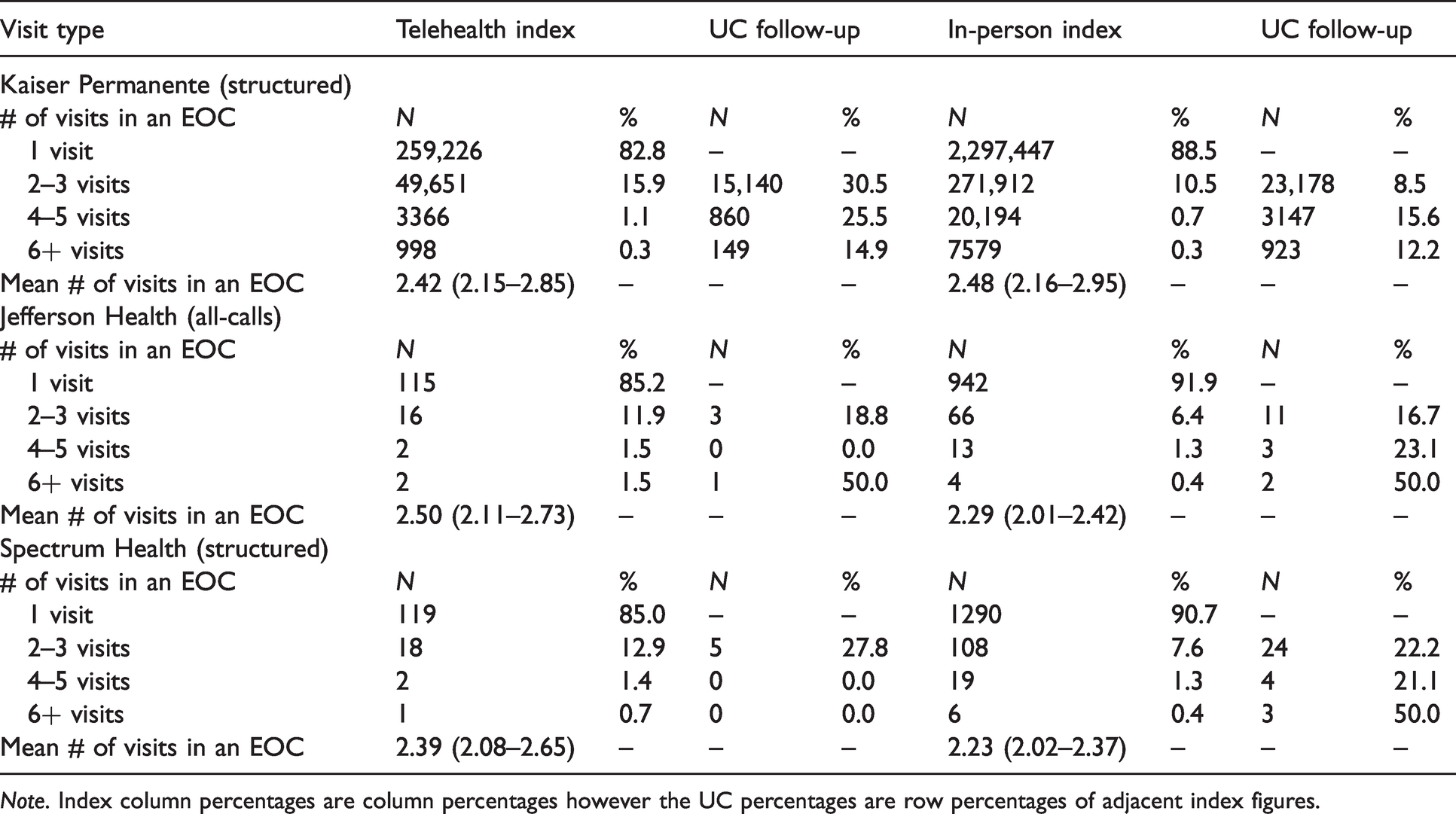
Note. Index column percentages are column percentages however the UC percentages are row percentages of adjacent index figures.
For Kaiser Permanente, 17.2% of index telehealth visits across all 20 clinical conditions required additional follow-up to achieve resolution. Depending on clinical condition, mean episode of care was 2.42 (±1.36) visits compared to 2.48 (±1.36) visits for the in- person cohort. No clinical conditions had a mean episode of care that comprised more than three visits (see Table 2). Mean episodes of care for back pain, head-ache/migraine, anxiety, and stress all required 2.5 visits per episode (See Supplemental Table 1). ED visits within 30 days of an index visit were similar to the in-person visits, with an average frequency of 1.17 visits, and telehealth, with an average frequency of 1.18 visits.
For Jefferson Health, 14.8% of index telehealth visits required additional follow-up and a mean episode of care of 2.50 (±0.26) visits compared to 2.29 (±0.09) visits for the in-person cohort. Of the eight clinical categories that required additional follow-up visits, gastrointestinal disorders, upper respiratory infections, and influenzarequired greater than 2.5 visits (See Supplemental Table 2). Across all eight clinical conditions, index telehealth encounters had similar numbers of visits to achieve resolution compared to in-person.
For Spectrum Health, 15.0% of index telehealth visits required additional follow-up, with the mean episode of care being 2.39 (±0.24) visits compared to 2.23 (±0.13) visits for the in-person cohort. Of the 13 clinical conditions, episodes of care had the most number of visits for allergies, musculoskeletal, and gastrointestinal problems (See Supplemental Table 3). Furthermore, index telehealth encounters had a similar frequency of visits to achieve resolution compared to in-person index visits.
Episodes of care – Poisson regression
Due to sample size limitations, only Kaiser Permanente had sufficient data to evaluate the frequency of episodes of care across different urgent and non-emergent conditions. In six of the 18 clinical areas, we found significant differences between the telehealth and in-person cohort where episodes of care starting with a telehealth visit required more visits to achieve resolution (head-ache/migraine, fatigue, back pain, sinus, constipation, and diarrhoea) (See Supplemental Table 1). The most notable difference was for headache/migraine, where episodes of care starting with a telehealth visit took 16% greater number of visits to achieve resolution (Coef. = 0.846, 95% confidence interval (CI) 0.708–0.984; p < .001) (see Table 3).
Poisson model (Kaiser Permanente only).
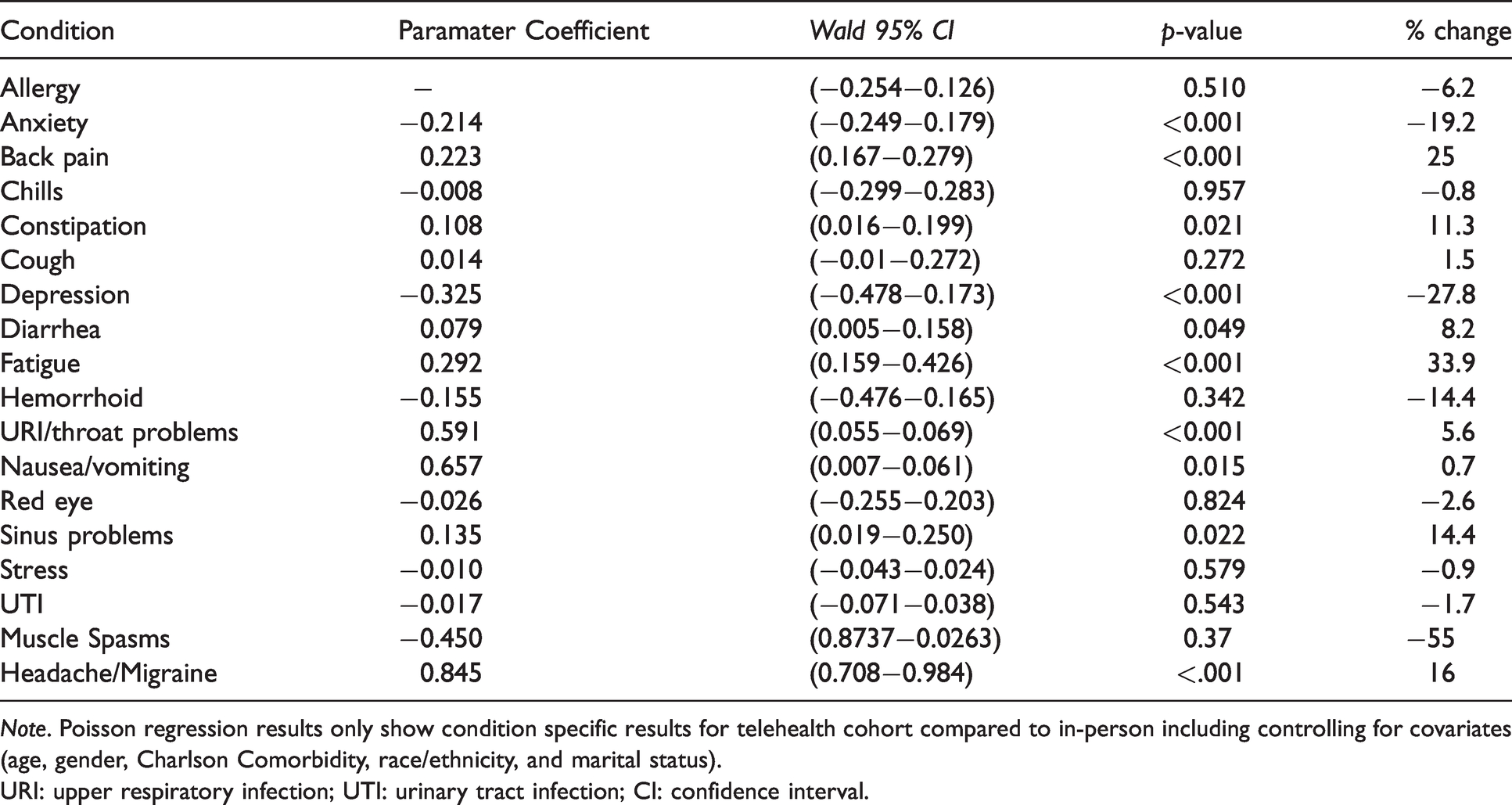
Note. Poisson regression results only show condition specific results for telehealth cohort compared to in-person including controlling for covariates (age, gender, Charlson Comorbidity, race/ethnicity, and marital status).
URI: upper respiratory infection; UTI: urinary tract infection; CI: confidence interval.
Alternatively, in four clinical conditions, our results indicate that when starting with a telehealth index visit, episodes of care were meaningfully shorter in frequency (anxiety, depression, nausea/vomiting, and muscle spasms). The most notable difference was for muscle spasms, where episodes of care starting with telehealth had 55% lesser number of visits to achieve resolution (Coef. = –0.45, 95% CI 0.8737–0.0263; p = .037) (See Table 3) than the in-person cohort. In all other eight clinical categories, differences in the frequency of episodes of care did not vary after controlling for age, gender, diagnosis, and comorbidity.
Discussion
Our results demonstrate that telehealth index visits were successful at resolving urgent, non-emergent needs between 84.0% and 86.7% of the time across three different organizations deploying three different models of telehealth. While the median rate of visit resolution for telehealth visits was lower than clinically comparable in-person visits, telehealth was effective in resolving urgent, non-emergent conditions a high percentage of the time.
We studied the number of visits in an episode of care to resolve urgent and non-emergent conditions when follow-up visits were warranted. The number of visits within an episode of care was largely similar to an in-person cohort. In our study, even when differences were present, they were marginal, and visits that required additional follow-up were resolved in a similar number of visits regardless of whether care was initiated via telehealth or in-person. Our findings suggest downstream utilization rates are similar between telehealth and in-person cohorts for urgent and non-emergent conditions among the senior population. This is in contrast to prior research where telehealth has been associated with increased utilization.8,13 However, our study focused on the senior population cared for by a healthcare system as opposed to prior studies that examined episodic utilization rates by younger or middle-aged adults, who historically have been the highest users of telehealth.
Where is telehealth most effective and how?
Our findings across three different organizations suggest telehealth is being most commonly deployed and utilized by seniors for upper respiratory infections, UTIs, and skin conditions, all of which were resolved at least 80% of the time with only one visit. These findings are particularly relevant given that the COVID-19 pandemic has increased the deployment of telehealth across the country.14–16
In addition, we also conducted secondary descriptive analyses and found differences based on the modality in which telehealth was deployed. One health system that utilized multiple different modalities found that for conditions such as eye infections, skin conditions, and allergies, telephone was equally as effective at achieving resolution as video. In this regard, organizations that wish to introduce or expand telehealth services for seniors may first consider conditions such as respiratory infections, UTI, and skin conditions, and, depending on clinical condition, consider starting with telephone as an initial modality.
Who administers telehealth?
Taken together, our findings suggest that while tele-health may not always be as effective at resolving urgent and non-emergent conditions as in-person, it is successful the majority of the time, even when follow-up visits are warranted. There are some notable differences that should be pointed out between our findings and prior research. 8 , 17 , 18 Perhaps the most significant, as mentioned above, was that in our study we focused on the impact of telehealth administered by a health system with established patients and its own provider network. This is in contrast to prior research which focused on the DTC approach where telehealth services were delivered by an online provider group independent of the patient’s primary care team or local health system. 8 While common, there have been questions raised as to the quality of care in these more independent provider and consumer-focused models, potentially due to the increased likelihood of fragmented, episodic care. For example, lack of access to the patient’s health records and past medical history may result in different recommendations between an independent provider and an established provider.
In our study, within each of the three organizations, telehealth services were facilitated by a provider affiliated with the health system, so they had access to the patient’s health record and past medical history. In this regard, providers had access to the same resources, documentation, and treatment options as those in an in-person setting, all of which are especially important during a pandemic.
Cost implications
While it is well known that the cost of a telehealth visit is a fraction of the cost of an in-person visit, 13 the challenge has always been if cost savings come at the expense of quality, utilization, and access. In our study, even in cases where the number of follow-up visits to achieve resolution was higher in the telehealth cohort, differences were relatively modest. Generally, we found differences in episodes of care were less than half a visit across each organization. Considering prior research estimates that telehealth visits costs less than a physician office visit, 19 our findings also suggest that for certain symptoms as defined in our study, telehealth is a lower cost alternative that does not compromise quality.
Specific relevance to older adults
Finally, the issue of access should be considered given the patient population in our study. Aging in place is not only preferred by the majority of seniors 20 but also has practical implications, especially during a pandemic where seniors are at higher risk for severe outcomes. COVID-19 has led to delays or cancellation of many non-essential in-person clinical services for seniors and coupled with concerns over visiting an ED due to potential COVID-19 exposure, telehealth has emerged as a critical tool in ensuring senior healthcare needs are being met.
Even before COVID-19, many seniors faced practical challenges, such as transportation, which has prevented them from keeping follow-up appointments, or in some cases visiting a provider at all. Alternative delivery models, like telehealth, remain our most promising option. Coupled with the fact that the ED is not an ideal clinical setting for seniors, telehealth may be one of our best alternatives to help address urgent and non-emergent conditions for seniors.
Limitations
Several limitations of our work are worth noting. This study focused on outcomes related to resolution of urgent and non-emergent conditions, and the premise that if a patient did not see a provider within 30 days of initial visit, the condition was resolved. Additionally, we did not look at severity of conditions and given the variability that is likely to exist between the same two clinical cases, the number of visits for the same condition to achieve resolution is likely to vary. Furthermore, we focused on visit resolution based on an acute single condition as opposed to overall utilization related to seniors with chronic conditions. Similarly, based on the symptom, 30 days may not always be an adequate window of time to schedule a follow-up visit, as in some cases it may be preferred and entirely appropriate to follow-up after 30þ days to assess treatment. This may be the case, especially for seniors where resolution of acute conditions may be longer based on medical as well as social factors. Episodes of care or number of visits is only a single marker as to whether clinical quality of care was delivered, as a routine follow-up compared to follow-up for re-examination serve two different purposes.
We also recognize that sample size was much smaller in two of our three participating organizations following inclusion of our eligibility criteria. Given our focus on seniors, the population of seniors utilizing telehealth that met inclusion criteria may have resulted in selection bias towards seniors who were already well connected to their health system’s providers and more likely to resolve acute conditions.
Conclusions
While the potential for telehealth has been discussed for years and widespread adoption has remained slow, the current COVID-19 pandemic has led to an unprecedented increase in telehealth utilization. Our findings across three different organizations indicate that when deployed within a health system for established patients, telehealth services are effective in addressing urgent and non-emergent healthcare needs of seniors between 84.0% to 87.7% of the time without additional follow-up. Even when visits require additional follow-up, the number of visits to achieve resolution were only marginally higher than in-person. While in-person visits have traditionally been the gold standard, our results suggest that when deployed within the confines of a senior’s existing primary care and health system provider, telehealth is an effective alternative to in-person care to address acute unplanned needs without increasing downstream utilization. This may especially be the case in common conditions found in older adults such as upper respiratory conditions, UTI, and dermatologic needs. Our findings are especially relevant as health systems seek to expand the scope and scale of their telehealth strategies in response to the COVID-19 pandemic and an increased preference by seniors for telehealth services.
Footnotes
Acknowledgements
The co-authors would like to thank Virginia Suarez, West Health Institute for project management, language editing, and proofreading.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KJK was employed by West Health Institute during the time of the study; AOC was employed by West Health Institute during time of the study; Larissa Kosten was employed by Spectrum Health during time of the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: West Health Institute, a non-profit applied medical research organization, provided an unrestricted grant to Jefferson Health, Kaiser Permanente, and Spectrum Health, and collaborated with each organization in the design, conduct, and reporting of the final results.
Supplemental material
Supplemental material for this article is available online.