
Abstract
Introduction
An innovative teleconsultation platform has been designed, developed and validated between summer 2017 and winter 2018, in five mountain huts and in three remote outpatient clinical centres of the Italian region Valle d’Aosta of the Mont Blanc massif area.
Methods
An ad-hoc videoconference system was developed within the framework of the e-Rés@MONT (Interreg ALCOTRA) European project, to tackle general health problems and high-altitude diseases (such as acute mountain sickness, high-altitude pulmonary and cerebral oedema). The system allows for contacting physicians at the main hospital in Aosta to perform a specific diagnosis and to give specific advice and therapy to the patients in an extreme environment out-hospital setting. At an altitude between 1500–3500 m, five trained nurses performed clinical evaluations (anamnesis, blood pressure, heart rate, oxygen saturation), electrocardiographic and echography monitoring on both tourists and residents as necessary; all of the collected data were sent to the physicians in Aosta.
Results
A total of 702 teleconsultation cases were performed: 333 dismissed (47%), 356 observed (51%) and 13 immediate interventions (2%). In 30 cases the physicians decided there was no need for helicopter and ambulance rescue intervention and hospital admissions. The main physiological measures, the classified pathologies, the severe cases and the cost savings are described in this article.
Discussion
The e-Rés@MONT teleconsultation platform has been discussed in terms of treated cases, feasibility, proactivity in reducing complexities, direct and indirect advantages, and diagnostics help; moreover, general and specific pros and cons have been debated, and future steps have been exposed.
Keywords
Introduction
Technology plays a vital role in further improving the healthcare sector. Digital technologies and the evolution in communication are changing the approach in the practice of medicine. Telemedicine has quietly become a part of healthcare and of everyday practice. 1
Recently, the potential for remote patient management through evolving technologies has increased patients monitoring as well as advice to physicians. In fact, a physician is now able to assist from a distance, and this is crucial in a mountain environment. 1 , 2 Telemedicine offers a pragmatic, convenient and low-cost solution for high altitude and expedition medicine.3–6
In order to improve healthcare for both tourists and residents in a mountain environment, and to manage acute mountain sickness (AMS) and general health problems, an innovative teleconsultation system has been developed within the EU Interreg V-A ALCOTRA 2014–2020 e-Rés@MONT project (code 492, start date 31 August 2016, end date 1 March 2018).
Mainly, the aim of the e-Rés@MONT project was to design, develop, perform and experiment with an innovative healthcare service to support mountain populations. The development of this project not only helped people who live in mountain areas but also improved the attractiveness of such areas for tourists. A network of structures and professional operators was built around Mont Blanc (Italy, France and Switzerland). The e-Rés@MONT project ended on March 2018 and the project was realised in collaboration with a group of five nurses trained in emergency setting and mountain medicine before they started their activity.
A specific Web platform was designed and implemented to be accessible via tablet with a mobile connection, providing:
A user friendly interface customised for the two groups of users, nurses and physicians; A multimedia text chat-audio-video real-time conference system, built on purpose for privacy reasons, allowing a connection with a medical doctor in a remote hospital; Methods for storing images and videos for clinical evaluation; A tool for the risk assessment of acute diseases which was accessible via Web and via a mobile application (app), based on a modified version of the National Early Warning Score (NEWS)
7
adapted in order to monitor oxygen saturation (SaO2) and blood pressure (BP) at different altitudes; A survey for individual lifestyles; An automatic evaluation of AMS based on the Lake Louise Score (LLS)
8
version 1993; An automatic evaluation of high altitude pulmonary edema (HAPE) and high altitude cerebral Edema (HACE)
9
; An automatic evaluation for severity Glasgow Coma Scale (GCS) to measure the consciousness of the patients.
10
When the Internet connection was unavailable, a decision support system (DSS) app on a tablet provided the nurses with the risk scores necessary to assess the severity of the patient and allowing them to decide whether to call the emergency system directly. Once the Internet connection was restored, all data recorded and saved locally were automatically sent to the hospital.
At the hospital, the physicians on duty checked all of the data and, if necessary, they would require a video consultation with the nurse and the patient. Once the diagnosis was made it would be stored within the platform and sent to the nurse who in turn would have to confirm the reading and communicate it to the patient.
A healthcare model, the first of this kind in Europe to our knowledge, based on a telecooperation and virtual teleconsultation service in mountain environment has therefore been developed and employed with both the locals and the people who spend time in a mountain environment episodically (tourists, hikers, climbers, etc.).
This model of teleconsultation is uncommon, at least in Italy; as a matter of fact, the Italian Law (12 July 2012) defined the goals of telemedicine: secondary prevention, diagnosis, care, rehabilitation and monitoring, rules are transferred to future integrations. In the meantime, the Italian Autonomous Region of Valle d’Aosta, in concordance with the Italian Government defined their guidelines for the use of telemedicine.
Methods
A platform of teleconsultation was designed and developed by the Institute of Information Science and Technologies (ISTI) in collaboration with the Institute of Clinical Physiology (IFC) part of the National Research Council (CNR) of Italy. The platform allowed to access a Web system (Figure 1(a)), via a tablet equipped with a mobile 3G/4G connection. The trained nurses from remote mountain huts in the Italian Northern mountain area, at an altitude between 1533–3500 m, were enabled to send multimedia data (physiological parameters: blood pressure (BP), heart rate (HR), SaO2; electrocardiogram (ECG) and echography) to the hospital in Aosta where a doctor would make a diagnosis.
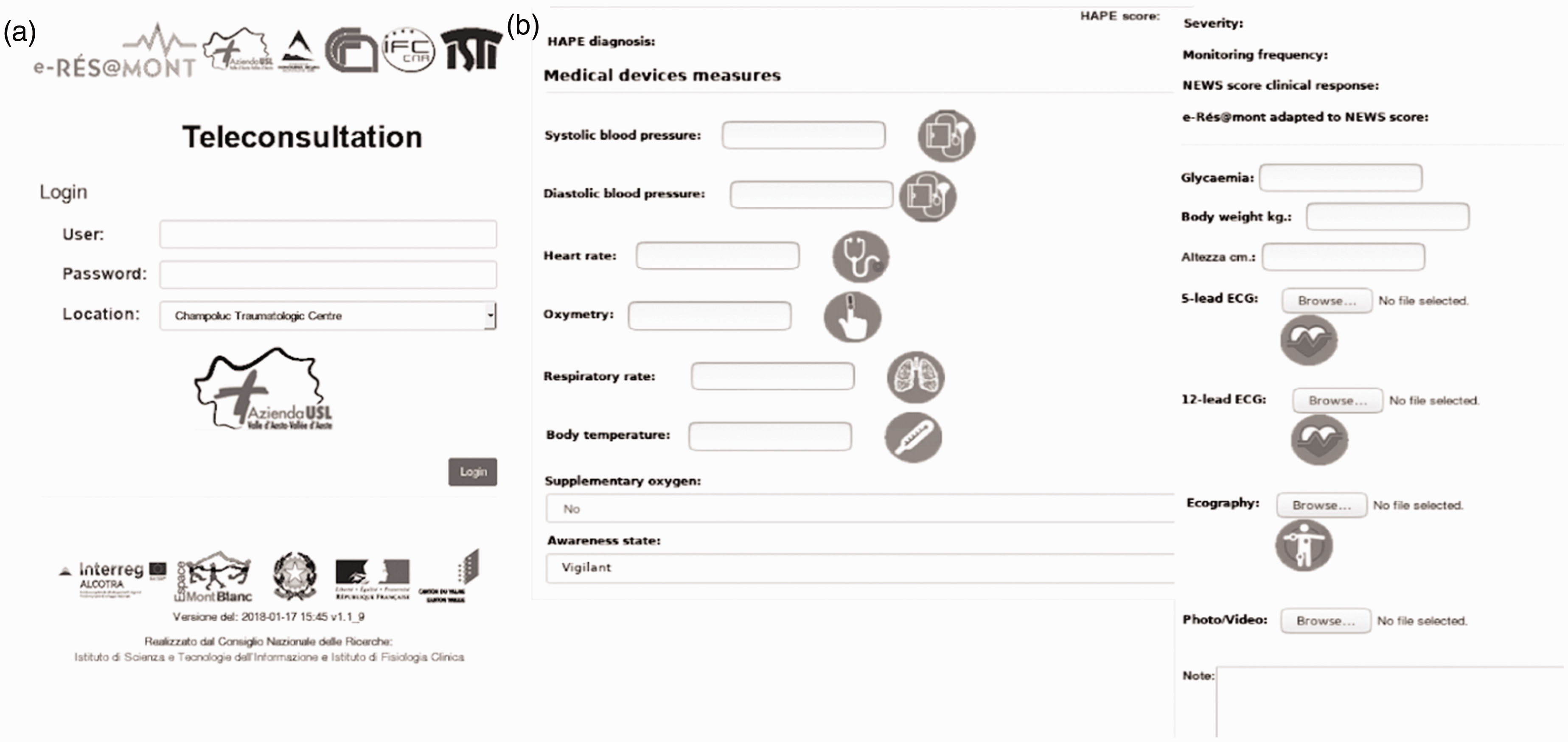
The login page of the e-Rés@MONT teleconsultation Web system (a) and the medical devices measures page (b). ECG: electrocardiogram; HAPE: high altitude pulmonary edema; NEWS: National Early Warning Score.
This platform provided an ad-hoc videoconference system built using the most recent technologies with auto-adapting video-band. When the connection was unavailable, a DSS, in the form of an offline Web app, provided scores and suggestions to the nurses which allowed them to evaluate the clinical severity, to dispense emergency aids and to call rescue services when needed. When the connection become available again, the locally stored data were sent to the hospital. Based on the acquired information, the presence of AMS was also automatically assessed. Doctors and nurses chose the validated scales, readjusted physiological parameters according to the altitude, defined tools and drugs, and identified a protocol to follow. As for symptoms, the patients were submitted to clinical evaluation (i.e. vital parameters, SaO2, body mass index (BMI), LLS questionnaire for AMS scoring); moreover, a five or 12-lead ECG and lung ultrasound could be performed. Based on the data received, the doctor on call would make the medical decisions, and nurse(s) who provided care to the patient(s) would receive the appropriate instructions.
All the subjects needing evaluation for AMS or any other symptoms were submitted to a standardised clinical evaluation: anamnesis, state of consciousness, BP, HR, respiratory rate (RR), body temperature and SaO2 monitoring. When necessary, the nurses would also perform ECG monitoring and ultrasound examination with a portable appliance.
Figure 1(b) shows the Web page dedicated to the collection of parameters obtained through medical devices for the teleconsultation.
The NEWS was used to determine the disease level of severity in patients and to solicit critical care intervention. In this study, the NEWS was adapted on the basis of the altitude therefore the SaO2 and systolic blood pressure (SBP) parameters were normalised. 11 The system, depending on the NEWS, can classify the subjects based on colour codes for disease levels of severity: white stands for mild diseases, yellow for medium-severity diseases that need a medical consultation in a short time, red for a level of severity that requires a direct call to the emergency system by phone (European emergency number 112).
In case of a yellow code and the simultaneous lack of Internet connection, the nurses should check the patient again within half an hour for a new clinical evaluation.
Figure 2 shows the teleconsultation list page accessible to the physicians: an immediate visual comprehension of the situation utilising the severity codes is presented, offering the possibility to search by single or multiple fields and globally on all the collected data.
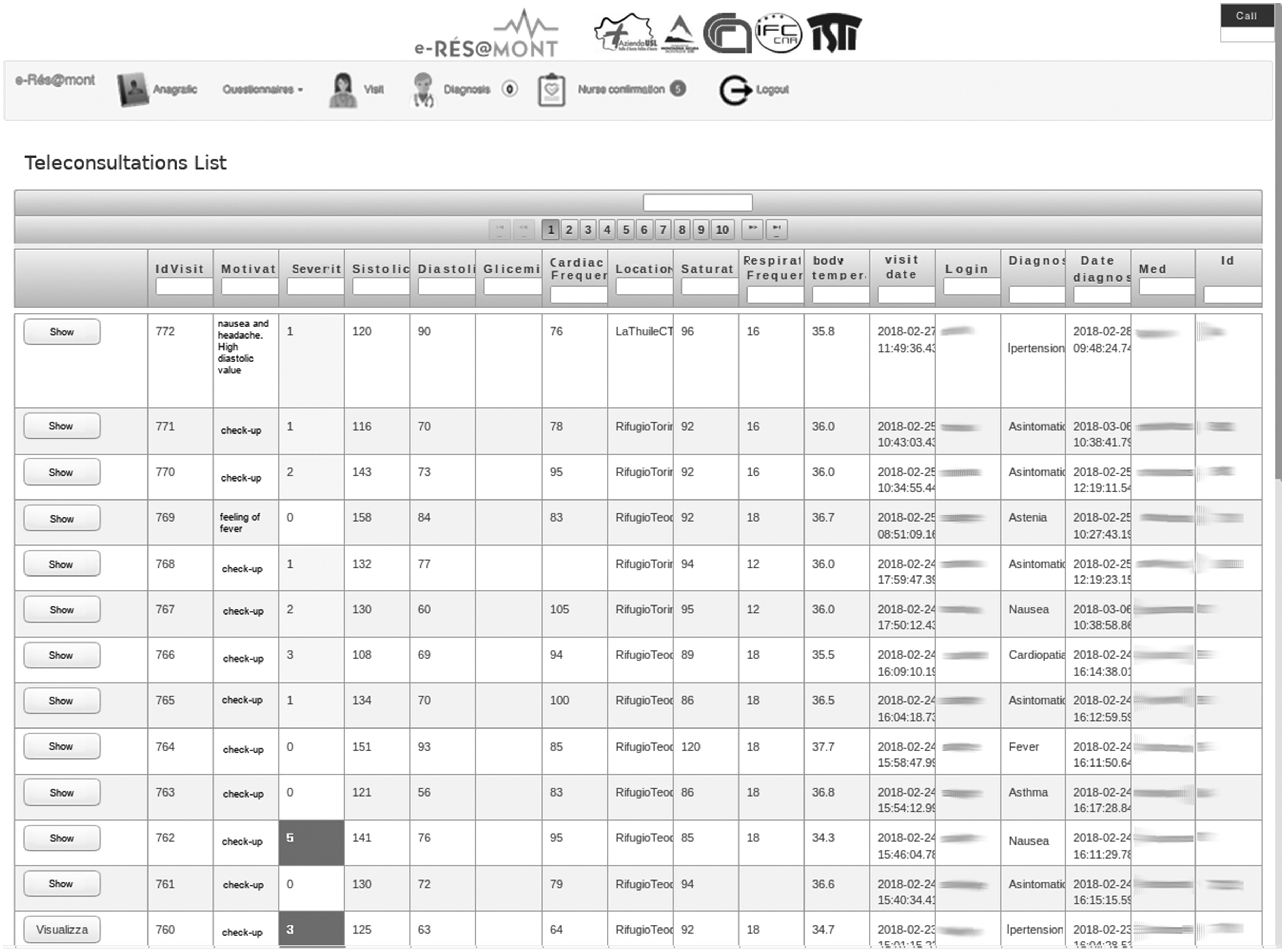
The teleconsultation list page.
Cutting-edge Web technologies were adopted: users had to open a browser (e.g. Firefox or Chrome) from a tablet and access a Web page. Behind the Web page there was a persistence module deputy with the aim to handle all the data, a logic module, also including the DSS providing risk scores and suggestions, a signalling module which can put in contact the nurse tablet with the physician tables (on activation, the connection continued peer to peer, without intermediary).
The videoconference data-rate was auto-adapted depending on the Internet band. The system is developed at Pisa, by a team from CNR-ISTI, as a prototype, and is connected to the Internet backbone (server) via cable.
In each mountain hut involved in this study, there were tablets equipped with a subscriber identity module (SIM) card, or a satellite connection with a wi-fi router providing a local area connection.
The final system has been deployed in the hospital and connected via cable to the Internet. In the Aosta hospital, a router was programmed to provide a secure connection for the tablet of the physicians (Figure 3).
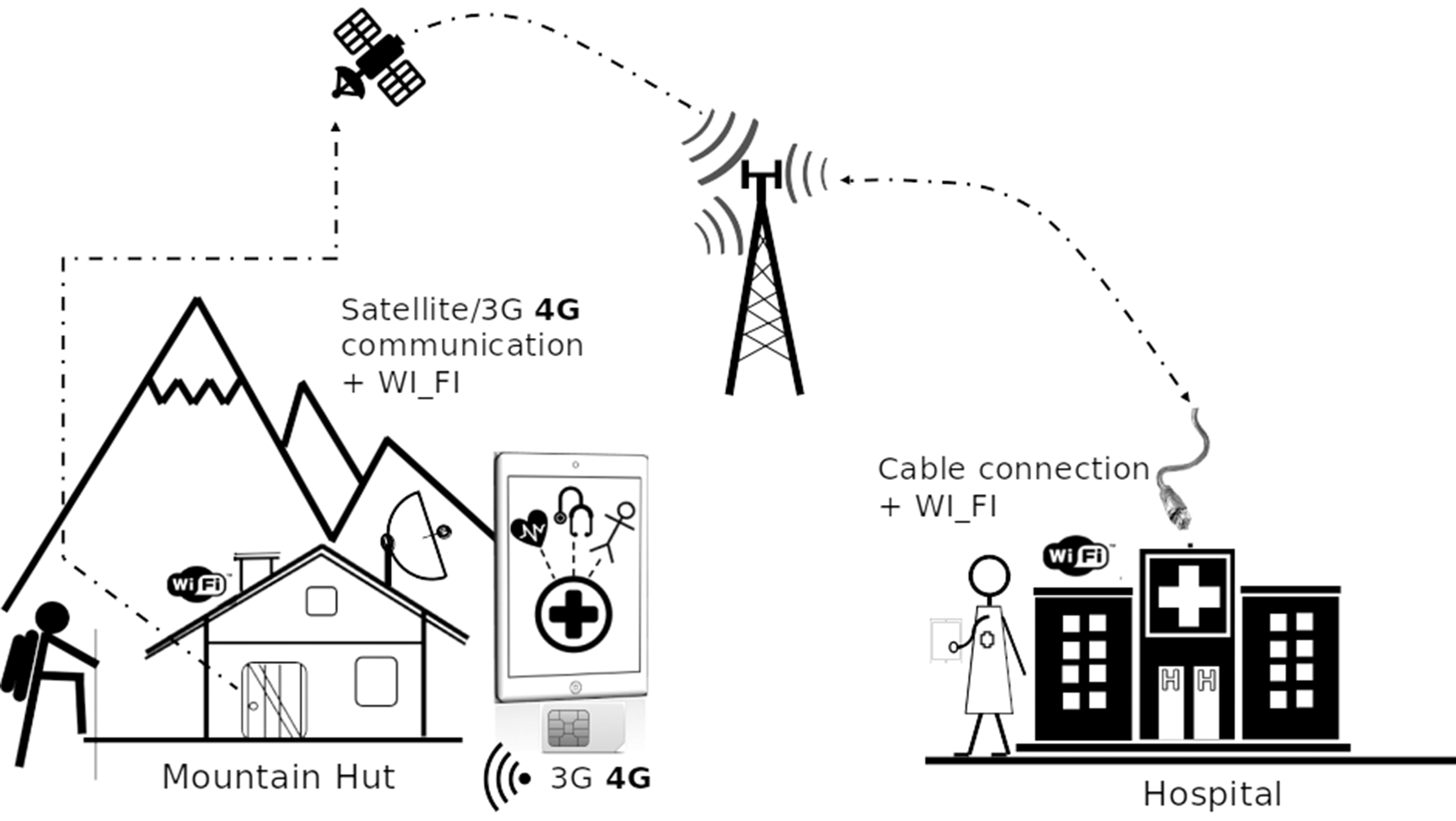
Connections schema.
To build our ad-hoc videoconference, Web Real-Time Communications (WebRTC) 12 was adopted, an open source project created to enable secure real-time communication of audio, video and data in Web and native apps (Figure 4). It had multiple application programming interfaces (APIs) related to capturing, recording and streaming audio and video, and also for streaming data between users. It is usable through a recent browser (i.e. Firefox or Chrome) on desktop and mobile apps.

An example of a videoconference test via Web Real-Time Communications (WebRTC) between the Institute of Information Science and Technologies (ISTI)-National Research Council (CNR) headquarters in Pisa and one of the participating mountain huts.
For storing data locally in the offline teleconsultation app, Localstorage 13 was used, a technology providing new methods to store information securely and locally in a browser. It has bandwidth, speed and security advantages compared to the old cookies technology, providing even more space. Moreover, information stored using local storage cannot be accessed from a different host.
For sending data between the remote mountain huts and the hospital, Websocket 14 was used, a new full-duplex communication protocol that can remain permanently active, enabling the exchange of information between the client and the server.
Results
Between summer 2017 and winter 2018, 702 teleconsultations were performed with the Aosta hospital within five mountain huts and in one remote outpatient clinical centre with the Aosta Hospital (males 61%; females 39%; average age 49±17 years).
The system performed the functions designed for mountain areas adequately: all data were correctly received at the hospital and teleconsultations allowed the specialists to check all the measurements in order to give their advice and to decide the final diagnosis and treatment. Figure 5 shows the teleconsultations by age groups: distribution is almost normal, although no sample selection was made.
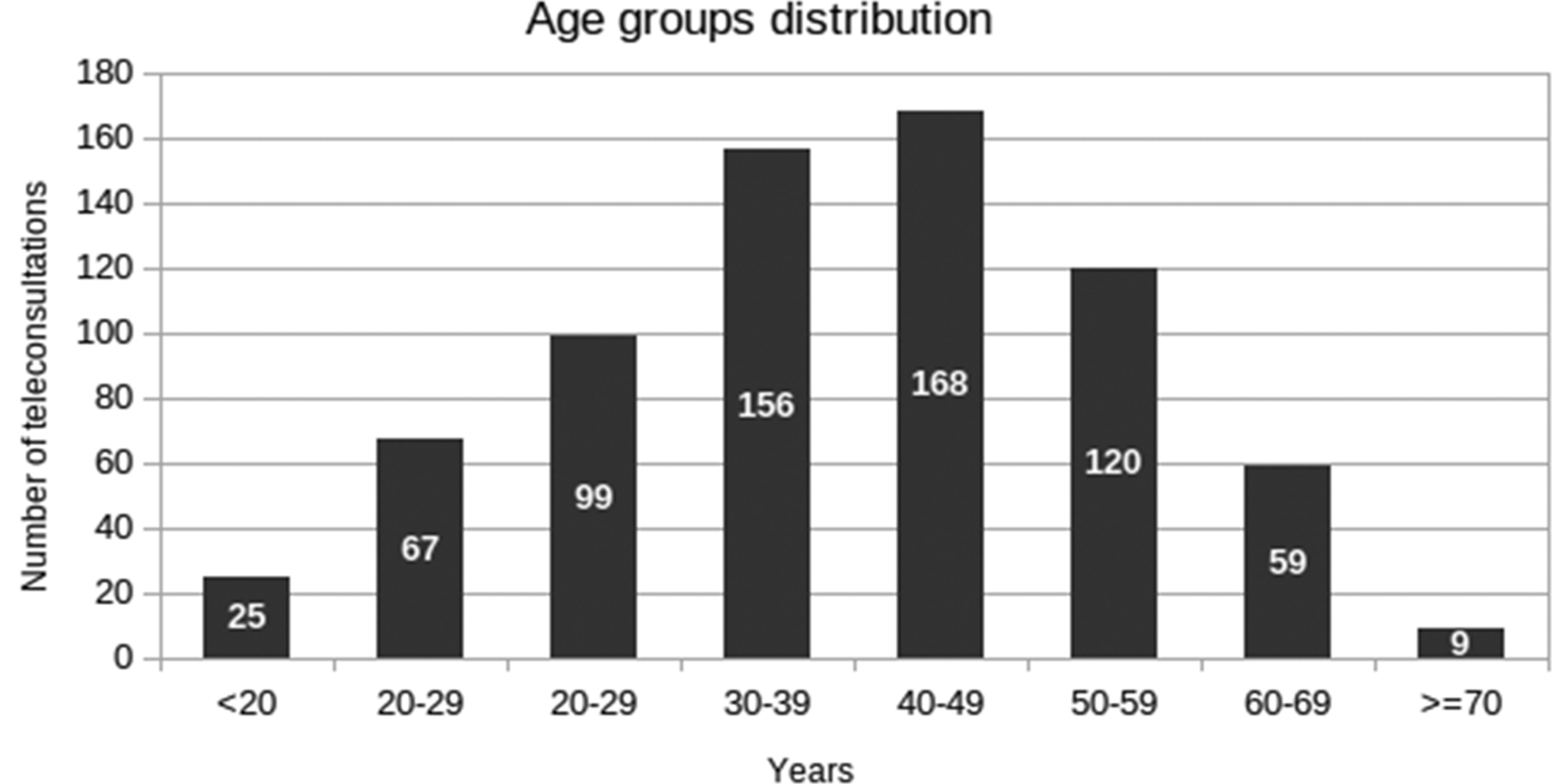
Age groups and distribution of teleconsultations.
In Table 1 the primary measures of age in years, SBP and diastolic blood pressure (DBP), HR, RR beats per min (bpm) and the SaO2, grouped by location, altitude and gender are reported.
Main physiological measures grouped by location, altitude and gender.
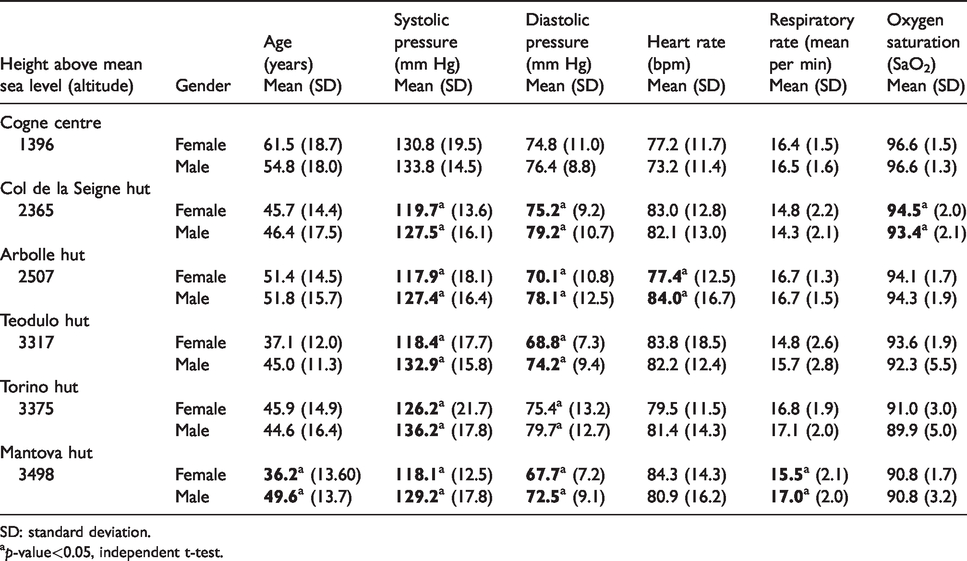
SD: standard deviation.
ap-value<0.05, independent t-test.
As expected, SaO2 decreased as altitude rose, while the mean age, BP and HR were lower in females. Moreover, in Cogne the average age was higher, probably because the healthcare centre supplies the entire local population in addition to the tourists.
Out of 702 consultations, a total of 203 resulted in an identified pathology (Figure 6): the most frequent pathologies were AMS (8.0%), headache (4.0%), minor trauma (2.3%), (which represented the 70% of the entire pathologies) and gastrointestinal disorders (1.3%).
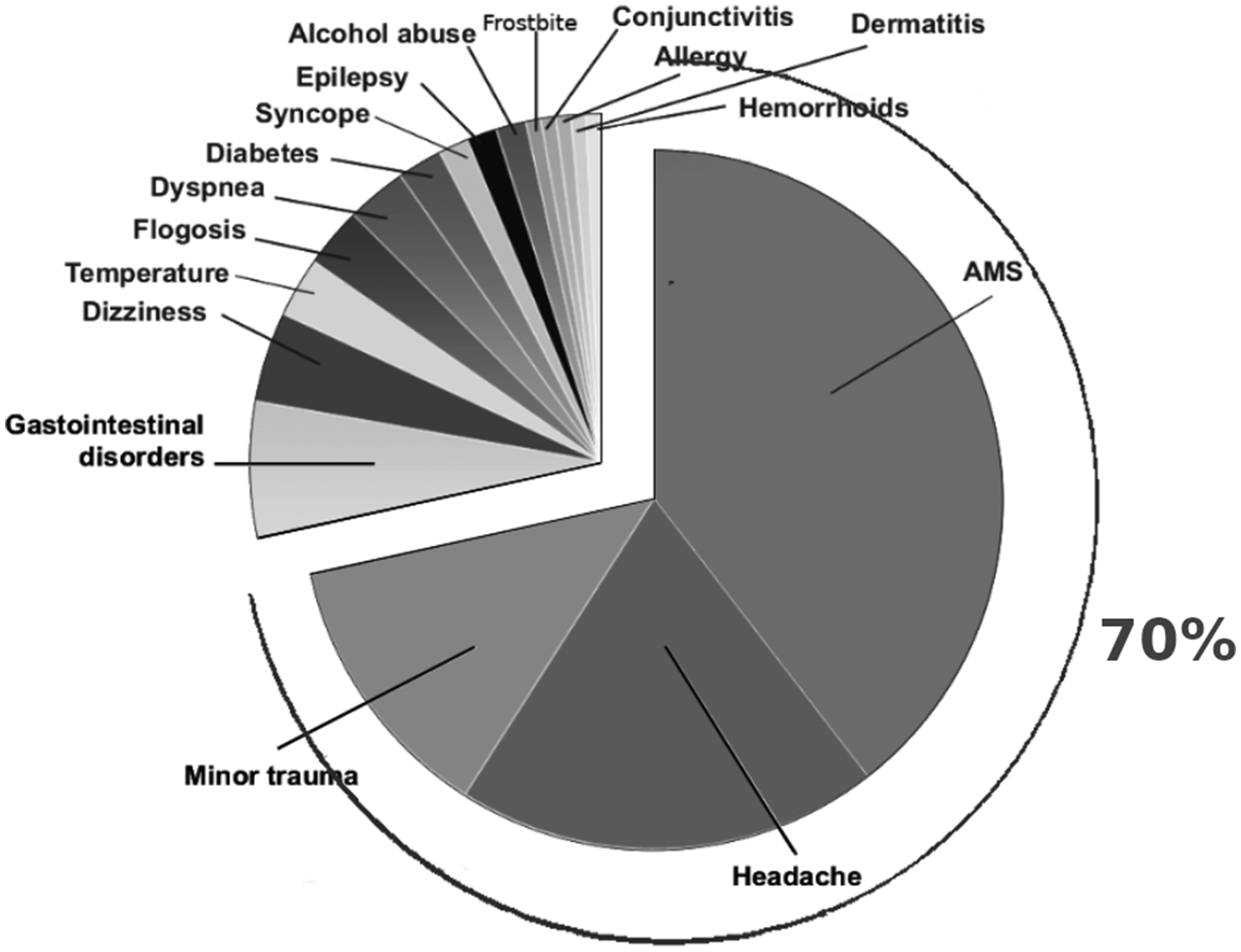
Classified pathologies in the e-Rés@MONT project. AMS: acute mountain sickness.
In Figure 7 the macro-categories of pathologies have been grouped by the mountain huts. The total percentage of AMS was 15.25%. As expected, AMS diagnosis increased at higher altitudes, but some differences have to be acknowledged: at the Mantova mountain hut (3498 m) the AMS percentage was lower if compared with the others at similar altitude: Teodulo (3317 m) and Torino (3375 m) huts.
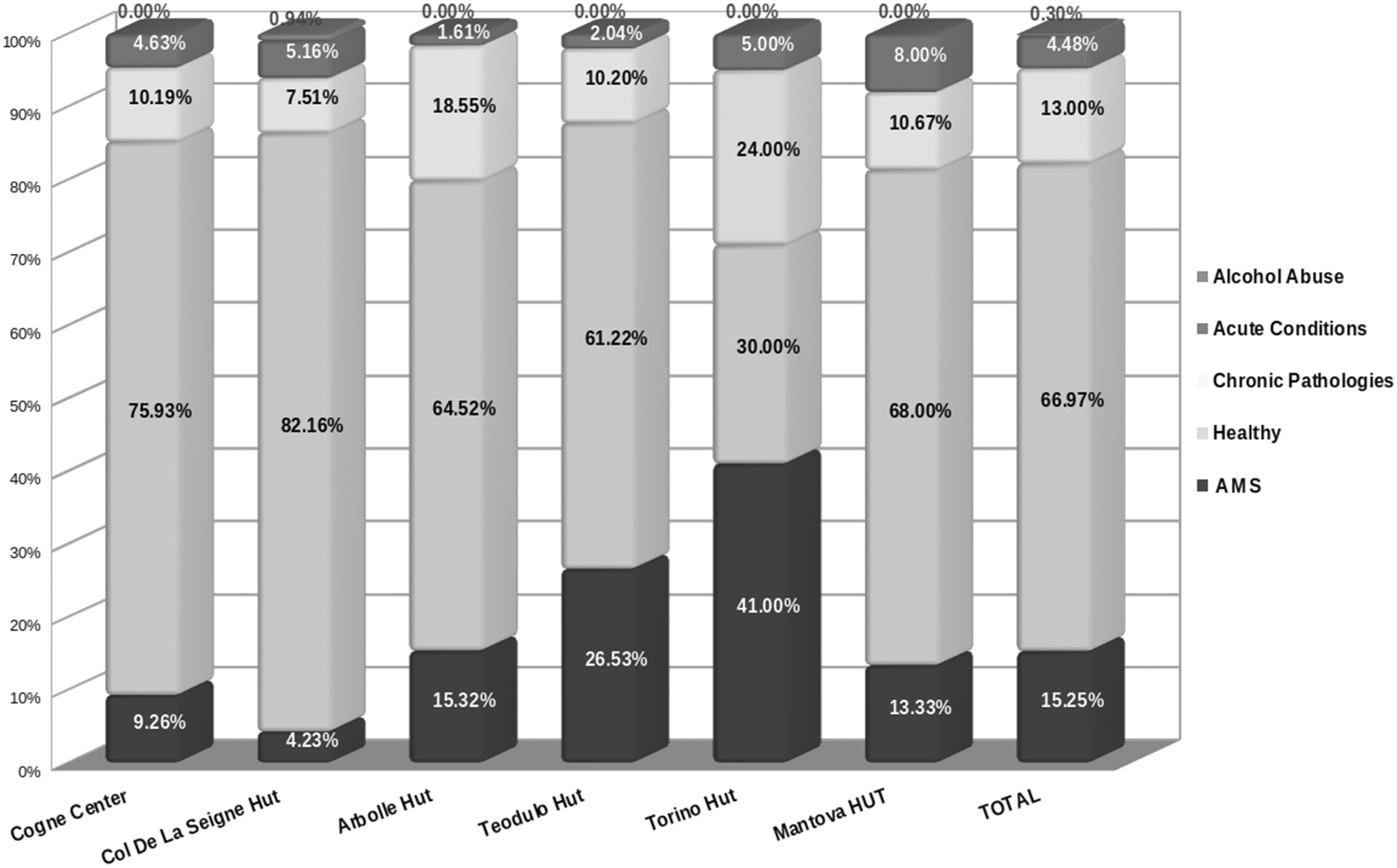
Macro-categories of pathologies: grouped by mountain hut and total. AMS: acute mountain sickness.
On the contrary, at the Torino and Teodulo mountain huts the AMS diagnosis was higher (41% and 26.5% respectively).
The teleconsultation system allowed us to reach a final diagnosis and treatment decision with an average time of 32 min. The subjects evaluated by the system were classified as 333 white codes (47%), 356 yellow codes (51%) and 13 red codes (2%). 15 , 16
Figure 8 shows the distribution of the severity codes grouped by sites: mountain huts at high altitude and wherever the patients’ average age was higher, and red codes were common.
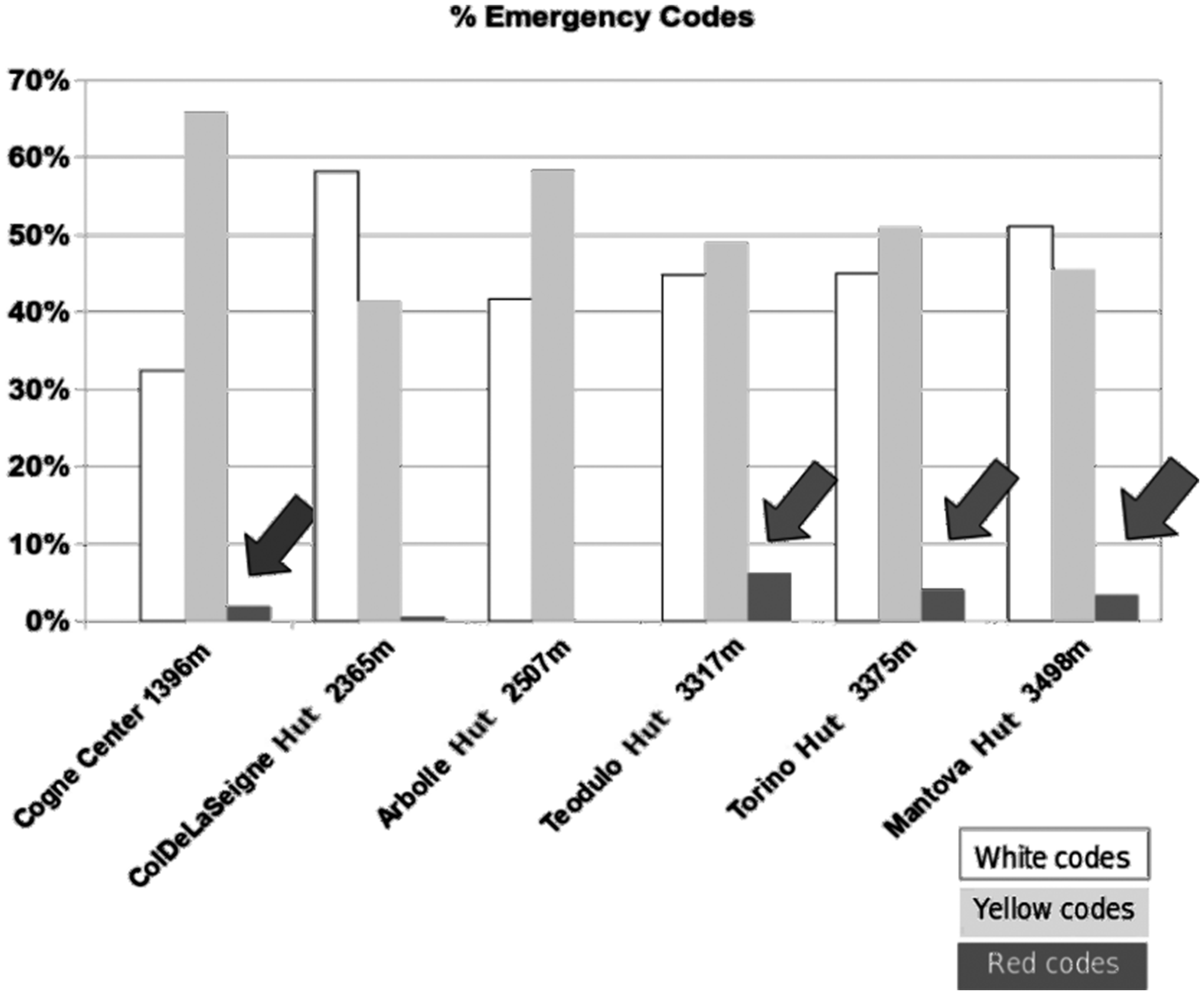
Emergency codes by location.
Figure 9 shows the macro-categories of all the pathologies: red and yellow codes versus red codes only (13 red, 17 yellow).
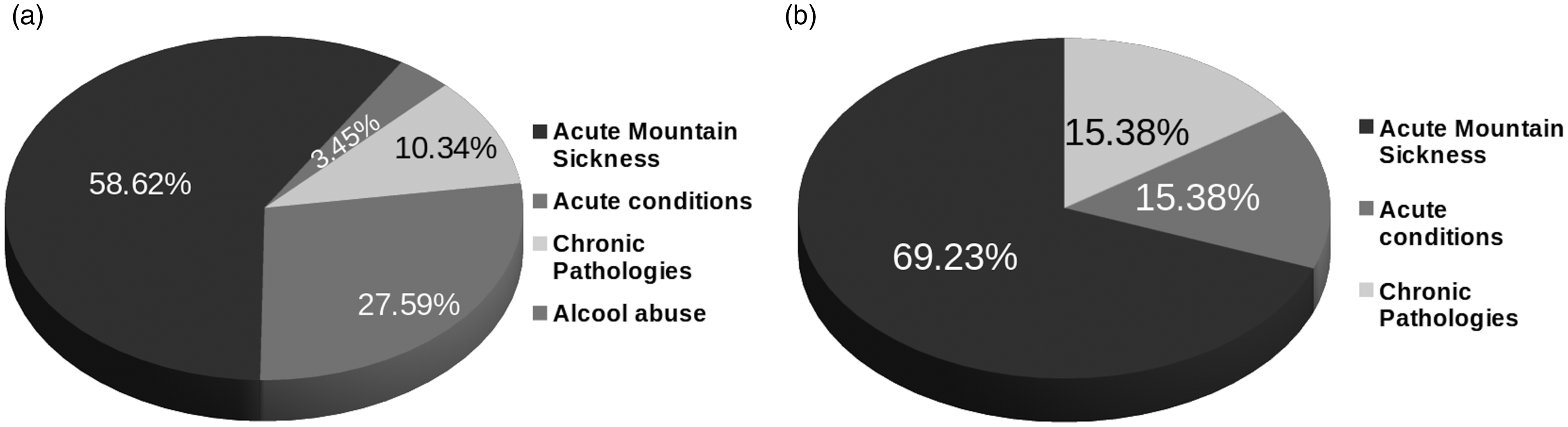
Macro-categories of pathologies for the 30 most severe cases: (a) red and yellow codes; (b) red codes.
In all sites where the e-Rés@MONT teleconsultation was used the AMS represented the most common pathology (58.2%) if we take into account together red and yellow code cases and even more if we consider only the red code cases (69.2%).
Specifically, the diagnoses labelled as red code cases were:
AMS macro-category: severe AMS, vertigo, headache, syncope; Chronic pathologies macro-category: hypertensive crisis; Acute conditions macro-category: hypotension and trauma.
In these 30 cases (yellow and red), the physicians on call in Aosta hospital decided to treat the patient on the spot and in most cases subjects were treated and then taken to a lower altitude as soon as possible on foot. As matter of fact, 30 inappropriate rescue interventions were avoided: 18 ambulance trips and 12 helicopter flights, and consequently the related admittance to emergency and specialised hospital departments were avoided too. On the basis of these data the global savings achieved amounted to 75,489€ as detailed in Table 2.
Global savings achieved.
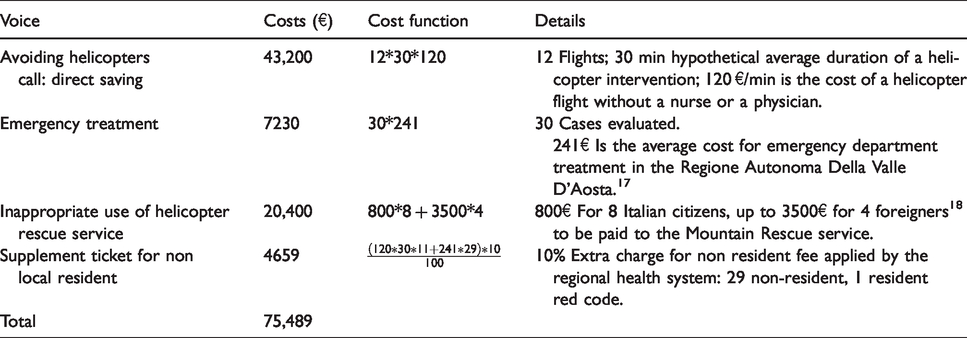
Moreover there were other direct savings for the additional cost for hospital department and indirect savings for leaving helicopters, ambulances, structures and personnel free where needed, reducing traffic and pollution.
Discussion
While on the mountains and rural areas of other parts of the world, such as the Himalayas and other regions,19–21 telemedicine has spread non-sporadically in the last few years, on the European Alps telemedicine is still not common and, in Italy, it is not even fully regulated and practicable, apart from provinces and regions with special status. In this scenario, the teleconsultation platform proposed in this paper has been the first of this kind on the Alps, tackling AMS and general health problems of both tourists and residents.
Technology plays a crucial role in the further development of the patient-centred healthcare, 22 and the e-Rés@MONT platform can help to shorten the distance between patients and medical staff, and improve the timeliness of monitoring, diagnosis and treatment.
Examinations of 702 persons were collected and analysed, partly automatically and partly verified by physicians and by specialists when needed, through the teleconsultation model proposed by the e-Rés@MONT project. The proposed platform has offered many advantages, not only the direct economic one (saving about 75,500€), which is certainly noteworthy but also the indirect ones. The advantages can be listed as (a) reduction of the waiting list (decision on treatment taking an average time of 32 min), (b) monitoring of multiple different pathologies (203 cases resulted in an identified pathology), (c) performing patient follow up, (d) opportunities for checking daily parameters in acute and chronic diseases, (e) providing teleconsultation everywhere, also from the doctors home, therefore reducing car traffic and, thus, the carbon footprint. With the results of the e-Rés@MONT teleconsultation system, it was possible to prevent deterioration in the different emergencies. Based on the physiological parameters measured, a score risk for the acute diseases was built up: the subjects that were diagnosed as a moderate risk were invited to rest and their follow-up was always performed.
Regarding the cons of the system: barriers remain in adopting these new technologies23–25 and it is essential to acknowledge that physicians actually prefer a face-to-face contact with with patients 26 when they need to perform a clinical evaluation. However, often not all consultations require a complete physical examination. Moreover, in this project, the teleconsultation was carried on by expert nurses who had also been trained to use ultrasound devices. From the perspectives of information and communication technology (ICT), one of the possible significant problems of this teleconsultation system regarded connectivity, especially in the extreme and challenging environment where the project was meant to operate. An offline app with a clinical DSS was provided with the aim to reduce the need for a connection to solve relevant potential issues and, in the case of a red code case, the nurses should call the emergency system as soon as possible. Privacy was dealt with by encrypting any exchange of information and any sensitive information in the database. Rights to access the stored information were customised by group of users and by location.
From an economic point of view, initial costs for acquiring devices and training the medical staff could be influential, but operatively cost will be adequately recouped.
Correct diagnosis and treatment are defined as quality of care: telemedicine helps to provide the two main dimensions of quality of care, that are access and effectiveness. 27
The e-Rés@MONT platform also allowed staff to make an AMS diagnosis and to give to the subjects the right indication whether to keep staying at high altitude or to descend. In the results, as expected, the number of AMS cases increased at higher altitudes, but at the Mantova mountain hut, the AMS diagnosis percentage was lower compared to other mountain huts at a similar altitude (the Torino and Teodulo mountain huts). These results could be associated with the fact that mountaineers at the Mantova mountain hut were generally more expert and to get the refuge they took the cableway up to 2980 m and afterwards they walked up to the Mantova mountain hut (3498 m). It is well-known that a slow ascent avoiding as much as possible mechanical transportation to climb a mountain is considered more appropriate for AMS prevention. 28 Appropriate preventive strategies should be adopted, i.e. warnings of acute high altitude disease risk should be visible at the starting point of the cable car, and should be useful in particular for tourists that decide to spend a night at high altitude without previous acclimatization.
Conclusions
The e-Rés@MONT multiparametric platform has been feasible and less time-consuming compared to the usual emergency system in a mountain environment. It can be self-financing with a low-cost sanitary ticket: a hypothesis provided by the Valle d’Aosta Region would be of about 35€.
With appropriate training, the platform could be used by the staff of the mountain huts without nurses or by the mountaineers themselves while staying in a bivouac, thanks to the video contact between doctors and subjects/patients. The e-Rés@MONT telemedicine platform can also be used for medical tourism, not only to improve healthcare in a challenging environment but also to save patients from the hassles of identifying and connecting with an appropriate health services provider, while removing language and cultural barriers. 29
Further studies are needed to assess the impact on health costs on waiting lists. Moreover innovative machine learning techniques can be used to classify diseases.
30
Non-availability of emergency healthcare services in mountainous, isolated and sparsely populated regions is a universal problem.
31
In this regard, on 26 October 2017, a teleconsultation between rescue point in Pheriche ( ), a village in the Khumbu region of eastern Nepal, situated at an altitude of about 4371 m, and Pisa, Italy, was made using the e-Rés@MONT platform. A male Sherpa, 50 years old, was diagnosed with a case of acute respiratory insufficiency: the clinical evaluation was performed in about 30 min and all of the data were shared through the platform.
), a village in the Khumbu region of eastern Nepal, situated at an altitude of about 4371 m, and Pisa, Italy, was made using the e-Rés@MONT platform. A male Sherpa, 50 years old, was diagnosed with a case of acute respiratory insufficiency: the clinical evaluation was performed in about 30 min and all of the data were shared through the platform.
Finally, we can say that the e-Rés@MONT telemedicine platform could also be used in other situations, for example disaster relief, emergency situations32 and high altitude expeditions, because of its ease of use, flexibility, adoption of innovative technologies, API applications and, above all, because it is within everyone’s reach thanks to mobile apps. Furthermore, the proposal platform may form a guide to practice in the field of high-altitude telemedicine.
Footnotes
Acknowledgements
The authors would like to thank Solange Bonin, Marina Cugnetto, Andrea Fiorini, Niccolò Pernechele, Marco Ranfone, Laura Caligiana, Franz de la Pierre, Massimo Stella (Mountain Medicine Centre, Valle d’Aosta Regional Hospital, Italy), Jean P Fosson (Montagne Sûre, Courmayeur, Italy) and Thaneshwar Bhandari, Kamal Thapa, Buddha Basnyat for testing the platform (from Nepal), the partners of the project: Ifremmont, Hesso, Grimm, and Suwas Bhandari, Viviana Guglielmi, Roger Tonetti (Montagne Sûre, Courmayeur, Italy), Diego La Monica and Ovidio Salvetti (Institute of Information Science and Technologies, National Research Council of Italy) for their valuable contributions and suggestions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest concerning the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by the Interreg ALCOTRA EU 2014-2020 project e-Rés@MONT ‘Applications de médecine de montagne autour du Mont-Blanc – Applicazioni di medicina di montagna attorno al Monte Bianco’.