
Abstract
Introduction
Suboptimal access to dermatologic care is dependent on patient location and insurance type. Although there have been attempts to address access issues, barriers to providing excellent dermatologic care to all patients at the right time still exist. The objective of this study was to investigate the clinical impact of Dermatology Extension for Community Healthcare Outcomes (ECHO) project participation on primary care providers’ diagnostic and treatment tendencies and accuracy.
Methods
This was a retrospective cohort study constructed using Dermatology Extension for Community Healthcare Outcomes case and recommendation data from November 2015 to June 2021. The University of Missouri-based Dermatology Extension for Community Healthcare Outcomes specialty hub team offers regularly scheduled live interactive tele-mentoring sessions for primary care providers who practice in rural and underserved areas. 524 patient cases presented by 25 primary care providers were included in the analysis. Of those, 449 cases were included in diagnostic concordance, and 451 in treatment concordance analysis.
Results
Less than 40% of all diagnoses were fully concordant with an expert panel. Over 33% of patients were misdiagnosed, and over 26% received partially correct diagnosis. Only 16% of all treatment recommendations were fully concordant with an expert panel.
Discussion
Diagnostic and treatment accuracy of participants is low, and Dermatology Extension for Community Healthcare Outcomes platform ensured patients received correct diagnosis and treatment quickly. Although tele-dermatology models are effective, they continue to be underutilized. Dermatologists in practice and training should be encouraged to adopt innovative clinical educational models, like Dermatology ECHO, to expand access to dermatologic expertise for the most marginalized populations.
Keywords
Introduction
Dermatologists are failing to meet the skin health needs of large populations of patients in the United States.1–4 The American Academy of Dermatology (AAD)'s most recent Burden of Skin Disease report shows that one in four individuals (aged 0–64 years.) have skin disease treated each year, as do half of those 65 years. and older. 5 Two-thirds of patients with skin disease are treated by health care providers who are not board-certified dermatologists and part of the reason for this appears to be barriers to referral. 5 Recent surveys through AAD's Specialty Positioning initiative demonstrate that one-third to one-half of non-dermatology physicians report having serious difficulty referring patients to dermatology when needed. 6
Suboptimal access to dermatologic services may be highly dependent on patient insurance type.4,7,8 Medicaid acceptance rates by dermatologists for patients of all ages in 2004 was 32%.9,10 In addition, only 17% of nonacademic dermatologists accept Medicaid. 11 A more recent study reported that privately insured patients are accepted by dermatologists over 90% of the time, compared to 29.8% of publicly insured patients. 12 Access to pediatric dermatologists is even more limited, reflected by a 44% average refusal rate of “new pediatric Medicaid-insured patients by Medicaid-listed providers” and the overall pediatric Medicaid acceptance rate of only 19%. 7 Lack of access to dermatologic expertise is detrimental to patients, resulting in greater morbidity and mortality.13–15 The impact of skin disease on patients’ mental health is also well established.16–19
There have been multiple attempts to address the problem of access to dermatologic services but it continues to be a barrier for the specialty in meeting its strategic goal of providing excellent dermatologic care at the right time and place for all patients. 20 There are different contributing factors influencing accessibility, including inadequate numbers of board-certified dermatologists relative to population, preference for practice in urban or suburban locations, and practices limiting the number of Medicaid or uninsured patients they accept. 21 The solution goes well beyond simply training more dermatologists. Creative and innovative practices are needed today whereby dermatologic expertise can be exported to those providing care in dermatologically underserved areas.
Project Extension for Community Healthcare Outcomes (ECHO)
Project ECHO is an innovative educational and mentoring model that began 16 years ago as the brainchild of Sanjeev Arora, MD, a board-certified hepatologist at the University of New Mexico.22–24 Dr. Arora identified an unacceptably high number of patients in his state dying of untreated hepatitis C secondary to poor access to care and specialty expertise, as demonstrated by a 10-month wait to be seen in his clinic. The program he developed is based on a Hub and Spoke model of educational conferencing where primary care providers (PCPs) and other clinicians (Spokes) videoconference with an expert (Hub) team using web conferencing technology from their clinical setting or home.25,26 The hub team is multidisciplinary, and the conference consists of a short didactic followed by discussions about patient cases that are challenging for the PCPs. It creates a collegial, supportive, tele-mentoring learning collaborative where evidence-based, best practices are shared and discussed. Rates of sustained virologic response of patients treated by PCPs participating in Hepatitis C ECHO (58.2%) were similar to those treated at an academic medical center (49.7%), showing that application of ECHO model resulted in high cure rates. 23 This case-based format is founded on the principles of adult learning and widely accepted as a more effective educational approach than traditional continuing medical education (CME) formats.27–29
There are currently 1117 ECHO programs in the United States, and over 1000 in 60 countries worldwide. 30 They focus on different diseases and conditions, such as autism, child psychiatry, COVID-19, and opioid use disorder, or community-related topics, such as public health, collaborative education, adult vaccination, among others. 30–33
Dermatology ECHO
The first Dermatology ECHO in the world began in 2015 at the University of Missouri (MU) with a hub team of experts that includes general and pediatric dermatology and dermatopathology.34,35 Since then, 16 Dermatology ECHO programs have been developed in seven countries. 30
The MU Dermatology ECHO biweekly hour-long sessions Consist of a hub team expert didactic presentation and one or more de-identified case presentation(s) by participating PCPs.35–38 Short introductions are followed by a 10 to 15-minute expert didactic presentation related to skin disease. Previous presentations included topics such as delusions of parasitosis, dysplastic nevi, evaluation of pigmented lesions, melanoma screening and detection, systemic therapy for psoriasis, among others. A Dermatology ECHO hub team clinical lead moderates case presentations and discussions that follow the didactic presentation.
Participating PCPs submit de-identified case presentations 3–5 days prior to the Dermatology ECHO. PCPs who are interested in presenting a case complete a short case form that includes patient age, gender, preliminary diagnosis (if any), preliminary treatment (if any), history of the skin condition, and de-deidentified pictures of the condition are enclosed. The form also requests the impetus for case presentation, such as questions about diagnosis or treatment. Cases are uploaded into the Microsoft OneDrive protected cloud storage, and reviewed by the hub team prior to the Dermatology ECHO session. 39 Two to nine cases are typically discussed during each hour-long session.
During a 3 to 5-minute PCP-led case discussion, submitted images are shared with participants by the hub team clinical lead. Case presentations are followed by clarifying questions asked by hub team members and other participants. The hub team clinical lead invites hub team members to provide their expert opinion and recommendations regarding the case. Dermatology ECHO supports the “all teach, all learn” learning framework, and the clinical hub team lead facilitator also invites participating PCPs to share their experiences and provide any additional recommendations regarding the case. 40 After each case discussion, the clinical hub team lead facilitator completes the “recommendation form” summarizing recommendations, which is shared with participants using the OneDrive folder.
Occasionally participants may disagree when discussing case recommendations, although this is a rare phenomenon. When it does occur, the clinical hub team lead will summarize all recommendations made during the discussion and the final decision on diagnosis and treatment will be at the discretion of PCP presenting the case. In this case the hub team will also ask the PCP to present the follow-up outcomes discussion in the future and share lessons learned with all participants.
Dermatology ECHO sessions are recorded, with recordings used only for research and evaluation purposes. Program evaluation shows an increase in participating PCPs’ self-efficacy in diagnosing and treating a variety of basic skin diseases.41,42
Dermatology ECHO offers the promise of greater clinical understanding and quality of care by enhancing communication between participating PCPs and dermatologists. The primary goal of this study was to investigate the clinical impact of Dermatology ECHO on participating PCPs’ diagnostic and treatment choices and accuracy.
Materials and methods
The MU Institutional Review Board (IRB) determined that this project included de-identified anonymous secondary data analysis, therefore not requiring IRB approval.
This was a retrospective cohort study constructed using Dermatology ECHO case data from November 2015 to June 2021. Cases from 19 November 2015 to 3 January 2020, were submitted on PDF forms, and cases submitted after 4 January 2020, were submitted through an online Research Electronic Data Capture (REDCap) 43 form and exported into Excel. 44 All case data was then combined and entered in an Excel database. 44
Dermatology ECHO case presentations
A total of 543 cases were presented during the study period. After removing cases with missing matching preliminary and final diagnostic or treatment data, 524 cases were included in the analysis. Of those, 449 cases were included in diagnostic concordance analysis, and 451 in treatment concordance analysis. Nine data elements were extracted from each presented case: patient age, patient race, patient sex, PCPs’ clinic county, unique patient count, preliminary diagnosis, hub team recommended diagnosis, preliminary treatment, and hub team recommended treatment.
Preliminary diagnosis and treatment presented by PCPs were then matched with final hub team recommended diagnosis and treatment. Participating PCPs were 15 physicians—medical doctors (MDs) and Doctor of Osteopathic Medicine (DOs) and 10 nonphysician providers—advance practice nurses (APRNs) and physician assistants (PAs).
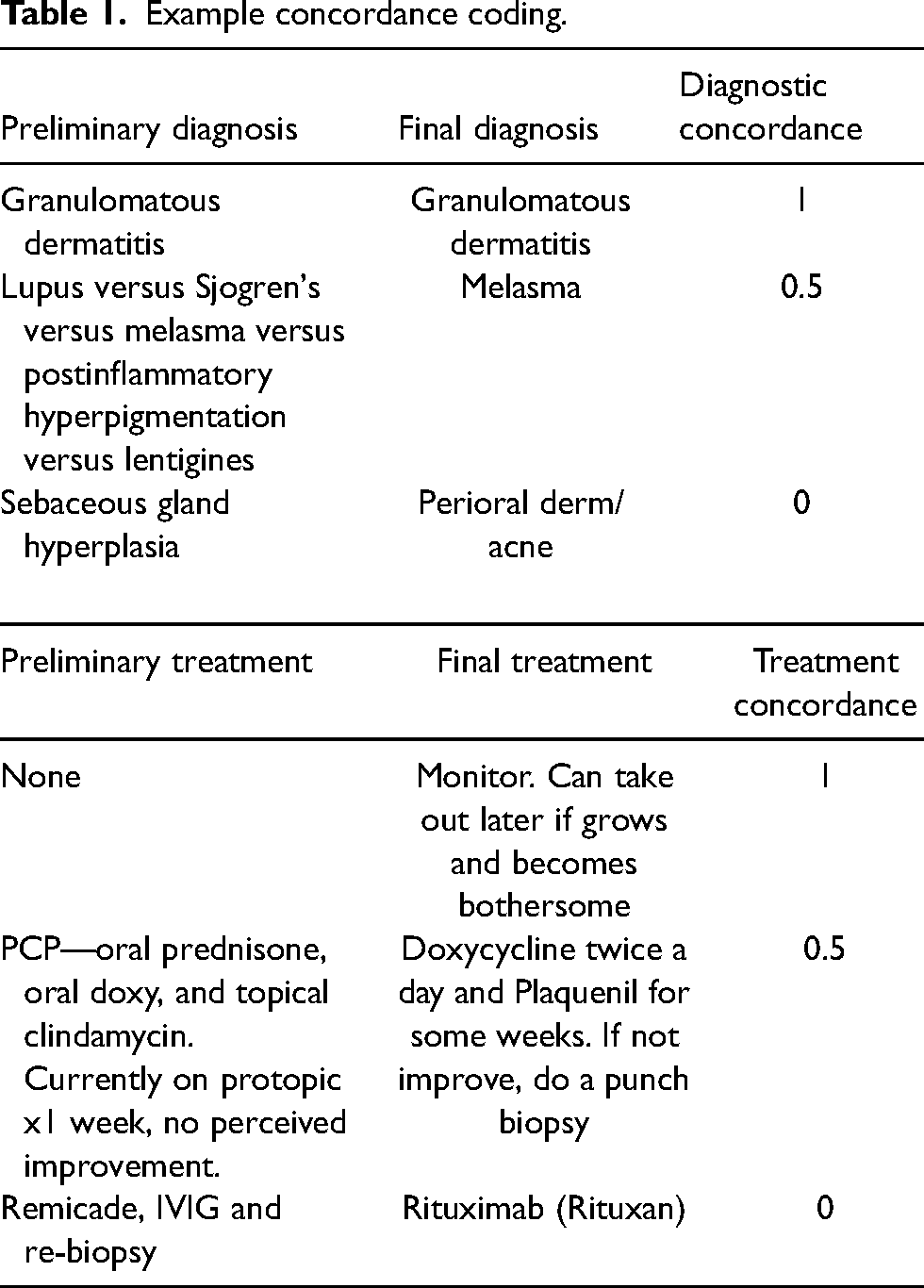
Concordance analysis considered the hub team recommended diagnosis and treatment as accurate and final. The following concordance definitions were used: 0 = poor, 0.5 = fair, and 1 = perfect (Table 1). Two dermatologists (KE and KB) independently coded diagnostic and treatment concordance. Study co-author (MB) reviewed and reconciled cases and identified coding differences. KE, KB, and MB met and corrected coding disagreements. Through discussion, each dermatologist shared their rationale for coding and came to a unified conclusion as to the final coding determination.
Example concordance coding.
Diagnostic and treatment concordance were calculated with 95% confidence intervals (CIs). The chi-square test for Equal Proportions was used to investigate the equality of completeness levels.
Results
Dermatology ECHO case presentations
A total of 25 unique participating PCPs presented 524 cases over a seven-year period (Table 2). We observed that the frequency of sessions changed in 2016, when weekly Dermatology ECHO sessions transitioned into twice monthly, reducing the number of annual sessions. In addition, 2015 data includes only two months of ECHO sessions (November and December), and 2021 data included 6 months of ECHO sessions (January–June).
Case presentations per year.
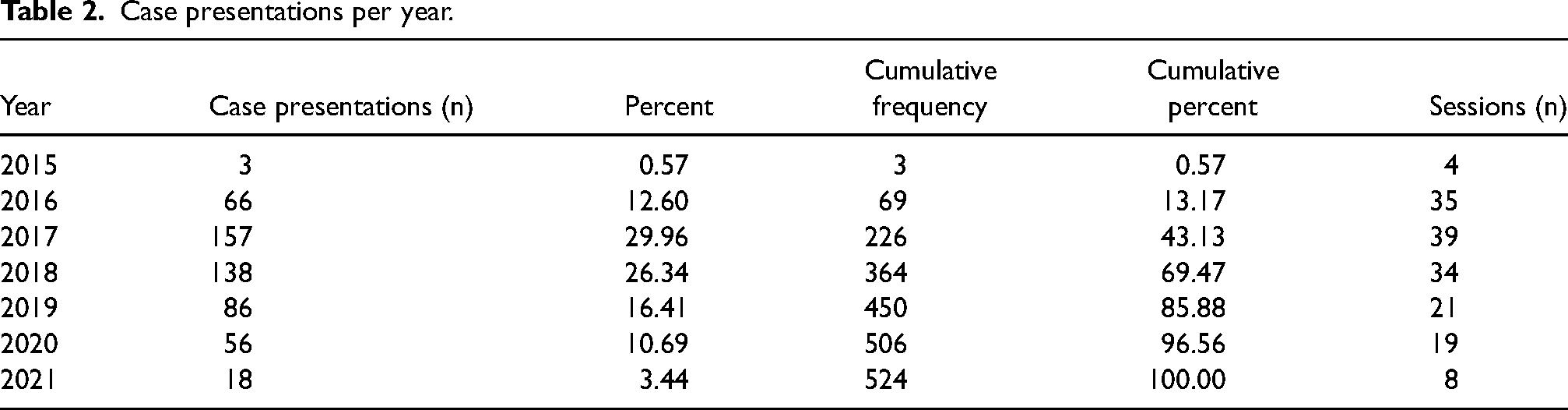
Of the presented cases, 81% (n = 382) were adult, and 19% (n = 88) were pediatric cases. Mean age of patients was 44.03. We observed 54 patient cases missing age information.
Presenting PCPs
A total of 25 PCPs presented cases during the study, 22 from MU, and one each from Texas and Kentucky; one clinician did not indicate location. The average number of case presentation per PCP was 20.96, with median of seven.
Diagnostic trends and concordance
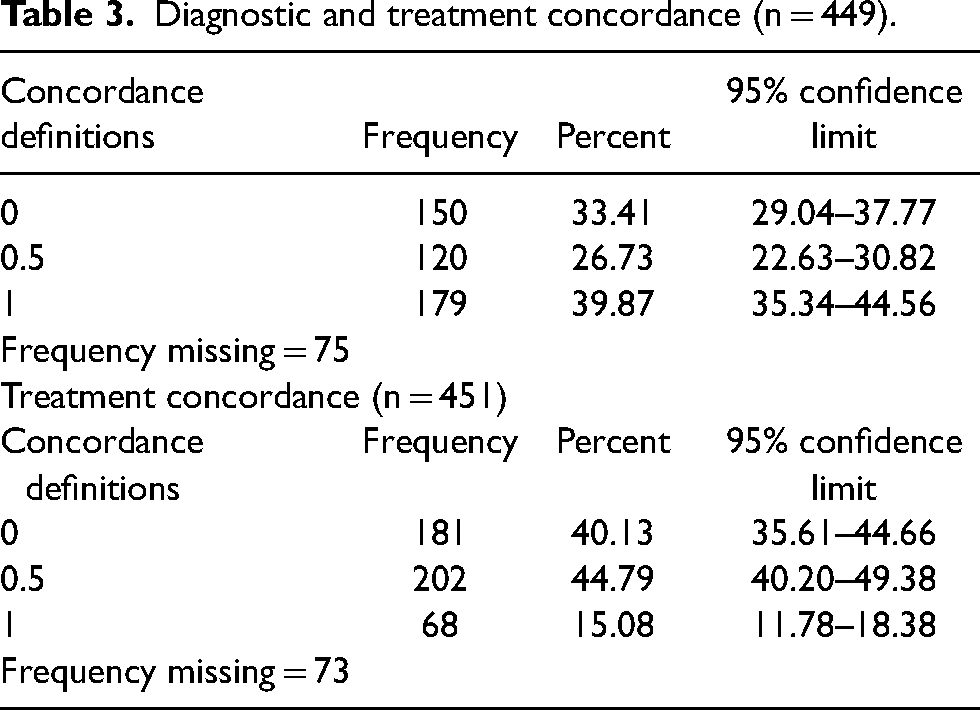
Table 3 shows the summary of diagnostic concordance for all cases. The chi-square test for Equal Proportions indicated the proportions is statistically significantly different (p < 0.0001). The percentage of complete agreement (39.87%) is significantly higher than partial agreement (26.73%) and no agreement (33.41%). The percent of complete diagnostic concordance is similar over the years (Figure 1).
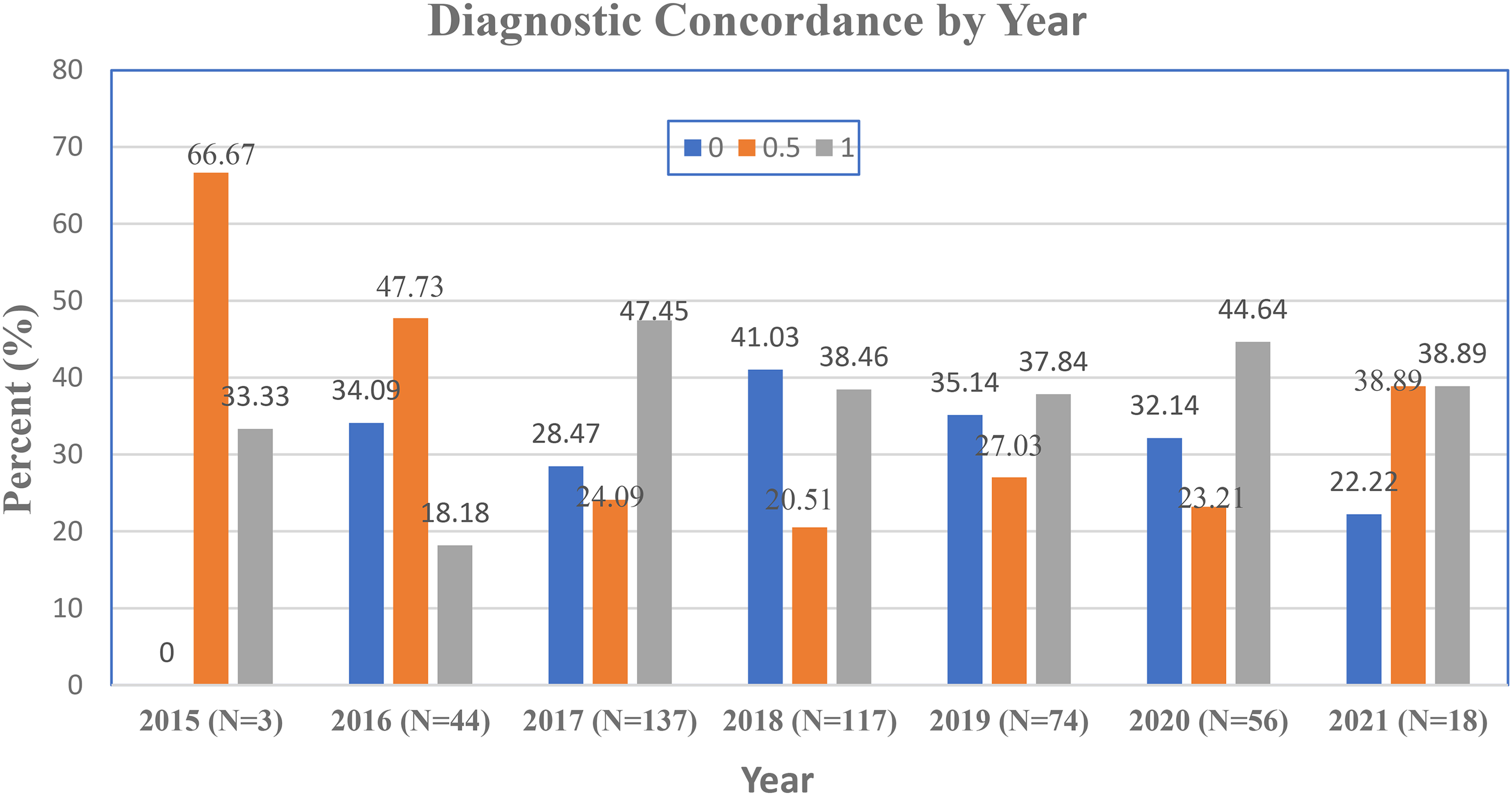
Diagnostic concordance by year.
Diagnostic and treatment concordance (n = 449).
Treatment trends and concordance
Table 3 shows the summary of treatment concordance for all cases. The chi-square test for Equal Proportions indicated the proportion is statistically significant difference (p < 0.0001). The percentage of complete agreement is significantly lower than the percentage of partial agreement (16% vs. 44.50%) (Figure 2).
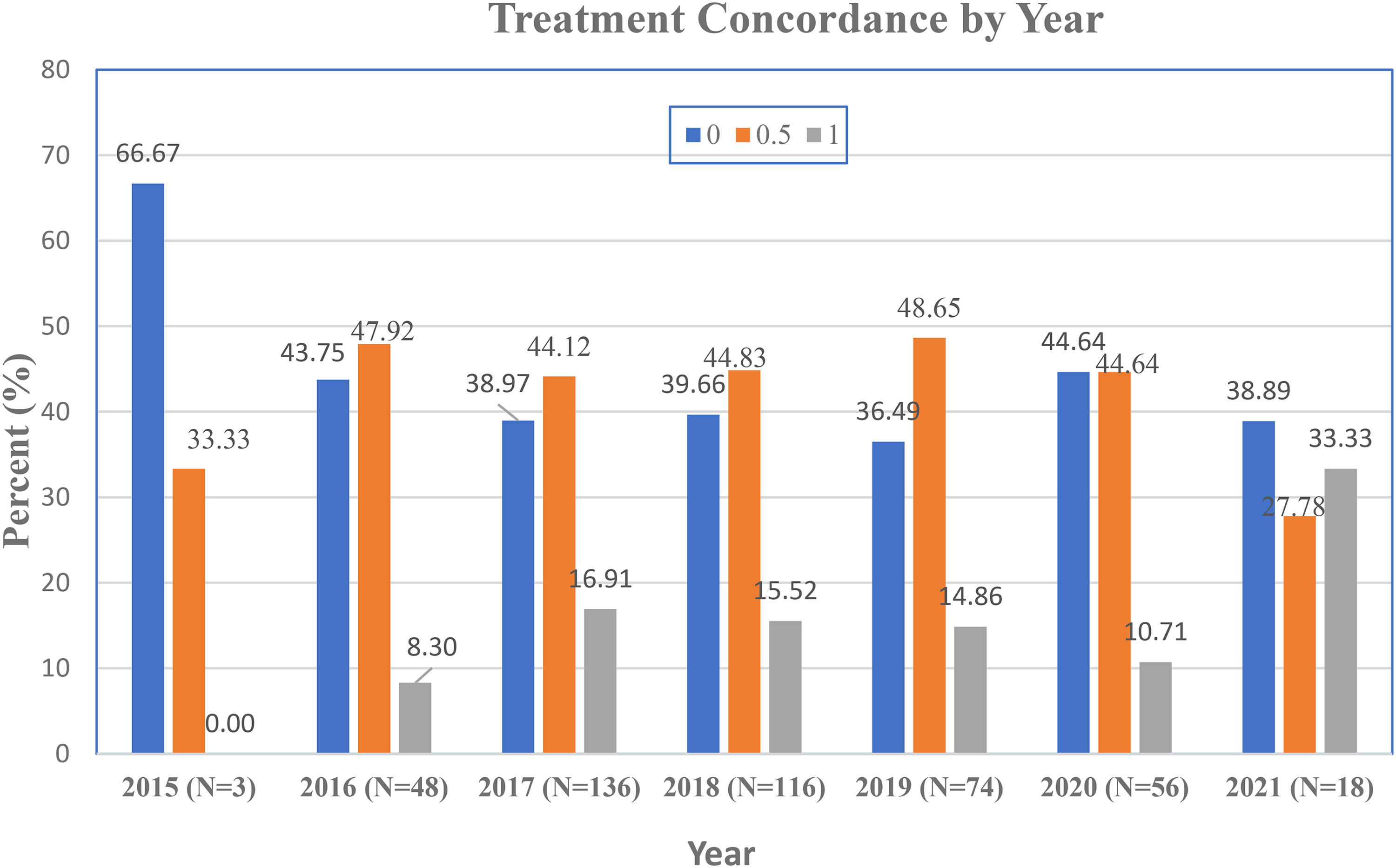
Treatment concordance by year.
Diagnostic categories
Diagnostic categories presented in the Burden of Skin Disease report were used to sort and quantify Dermatology ECHO case presentations. 5 A total of 449 unique diagnoses in 24 separate diagnostic categories were presented (Figure 3). Most cases were in the connective tissue category (n = 51), followed by contact dermatitis (n = 44), and psoriasis/lichen planus (n = 41) (Figure 3).
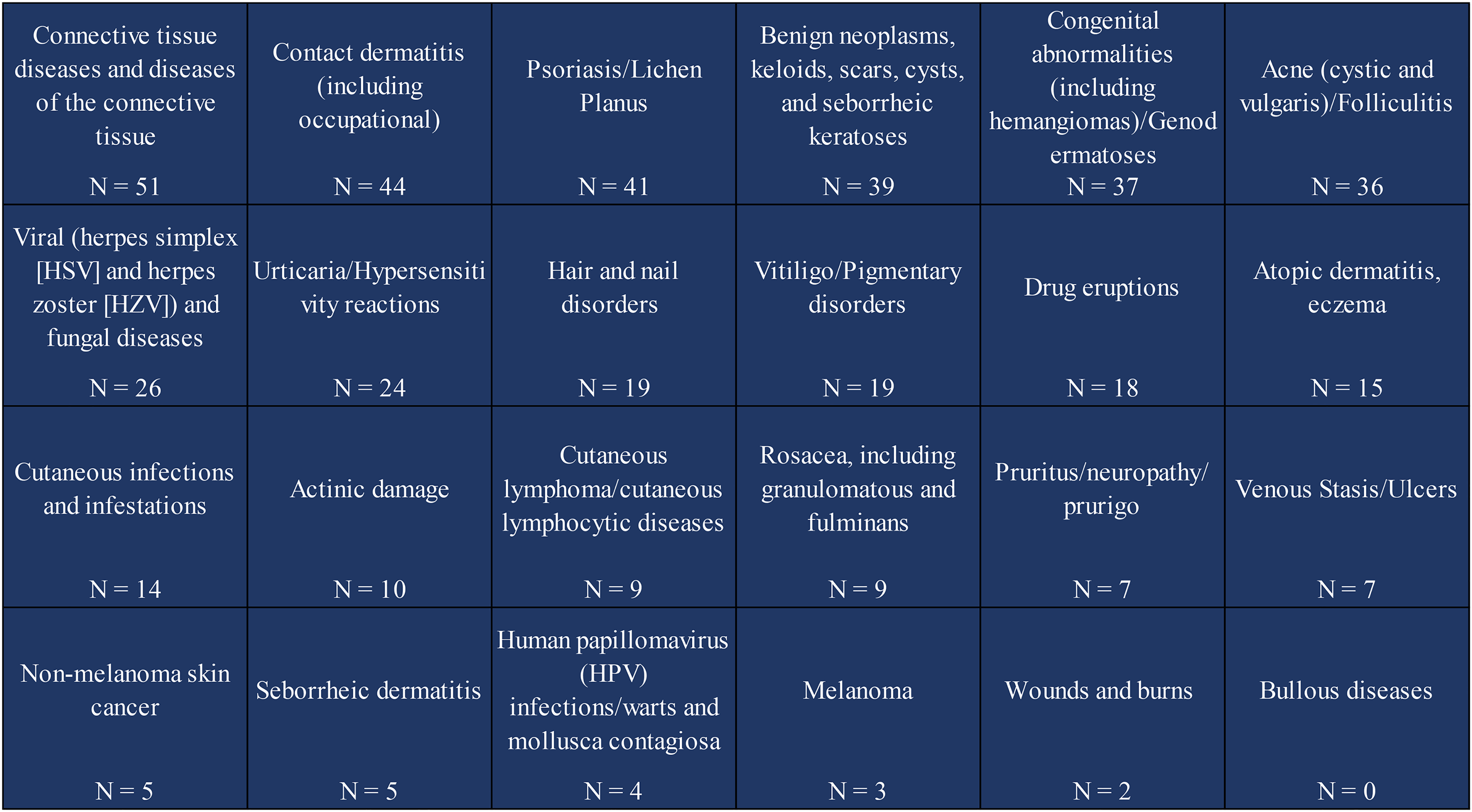
Dermatology Extension for Community Healthcare Outcomes (ECHO) diagnostic categories.
Conclusion
Patient access to healthcare varies greatly and is influenced by geolocation, health insurance status, and socioeconomic status. 45 For dermatology, the workforce shortage remains geographically imbalanced, disproportionately affecting access for patients in rural and other underserved areas that have not seen significant transformative improvement for decades.46–48 Although tele-dermatology has the potential to improve access and reduce costs, barriers remain.49,50 Absence of adequate broadband and connectivity, low reimbursement, liability concerns, lack of access to and knowledge of local resources, and local absence of procedural care have prevented implementation and adoption of telehealth technologies across service regions and healthcare systems.51–55
It is estimated that over 50% of the US population has some form of skin disease, of which 22.5% is moderate or severe.42,56,57 Lowell et al. reported that in primary care settings, almost 37%of patients present with at least one skin problem over a 2-year period. 58 However, studies have shown lack of adequate training and education of PCPs, both physician and nonphysician, in diagnosis and treatment of skin disease often result in delayed or missed diagnosis and costly treatments.59,60 Most skin lesions are first identified in primary care.59–61 Diagnostic concordance data comparing accuracy of PCPs and dermatologists in identifying melanoma reveals that PCPs achieve lower diagnostic accuracy compared to dermatologists. 59 However, continuing education, mentoring, and collaboration with dermatologists may help PCPs triage suspicious lesions with greater precision. 62 This study included all cases presented in Dermatology ECHO, malignant and nonmalignant lesions and conditions. While complete diagnostic agreement (39.87%) between participating PCPs and dermatologists was higher than partial agreement (26.73%) or no agreement (33.41%), less than 40% of all diagnoses were fully concordant with an expert panel. Over 33% of patients were misdiagnosed while 26.73% received partially correct diagnoses. Over 60% of patients received preliminary diagnoses that were partially or completely in disagreement with dermatologists.
Though diagnostic and treatment accuracy was low, the patients presented in Dermatology ECHO ultimately received timely and correct diagnosis and treatment. Expert hub team members have also noticed cases presented from long-standing participants tend to become more complex and less common over time.
Recommendation
Dermatologists in practice and training should be encouraged to adopt innovative clinical educational models like Dermatology ECHO to expand access to dermatologic expertise, especially for geographically and socioeconomically underserved patient populations, thus providing expert dermatologic care at the right time and place for more patients.1,20 Although tele-dermatology models, including ECHO, are effective, they continue to be underutilized, emphasizing the need for implementation of innovative, multipronged strategies. 1
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Resources and Services Administration (grant number SP13977-SB11).