
Abstract
Introduction
The ubiquitous nature of mobile technology coupled with the acceptance of mobile health (mHealth) among the elderly offers an opportunity to augment the existing medical workforce in long-term care. The objective of this review and narrative analysis is to identify and analyse facilitators and barriers to adoption of mHealth for the elderly.
Methods
Studies over the last year were identified in multiple database indices, and three reviewers examined abstracts (k = 0.82) and analysed articles for themes which were tallied in affinity diagrams to identify frequency of occurrence in the literature (n = 36).
Results
The three facilitators mentioned most often were independence (18%), understanding (13%), and visibility (13%). The three barriers mentioned most often were complexity (21%), limited by users (12%) and ineffective (12%).
Discussion and conclusions
The reviewers concluded that the work done so far illustrates that mHealth enables a perception of independence. Future research should focus on the barriers of complexity of technology and improving existing medical literacy in order to facilitate further adoption.
Introduction
The US National Institute of Standards and Technology defines mobile devices on multiple levels, and these have been edited to list only those attributes that are addressed by this review: A mobile device has a small form factor, at least one wireless network interface, local non-removable data storage, an operating system that is not a fully-fledged desktop or laptop operating system, and applications that are available through various methods. Mobile devices may also contain one or more digital cameras or video recording capabilities and a microphone. 1 The existence of mobile technology enables mobile offices, cloud-based data, abundant wi-fi and mHealth. Generations of people, defined by year of birth in Appendix 1, demonstrate similar characteristics due to events that occurred at the same or similar stages in their lives; the two generations discussed in this review are the oldest generations still living: baby-boomers (born 1946–1964) and traditionalists, or the silent generation (born prior to 1946). The two older living generations, traditionalists and baby-boomers, accept mobile technology, and some estimate that by 2020 69% of those over 60 years old will own a mobile device; an important factor as most of the world looks toward 5G as the next standard.2–4
Baby-boomers are more likely than traditionalists to accept newer communication technology, and as baby-boomers age they are more likely to carry mobile technology with them into old age, following the model of diffusion of technology.2,3,5 About 20% of public national health expenditure (NHE) is spent on the elderly, but the elderly only comprise 13% of the population. 6 As the numbers of the elderly grow, so will associated public health expenditures. In the USA 10,000 individual baby boomers retire each day, and worldwide the number of those over age 60 years is expected to triple over the next 20 years, which removes more individuals from the workforce who pay for the care of the elderly.6–8 mHealth creates an opportunity to expand services without expanding the existing workforce. Through mHealth, diffusion of technology leverages communication systems and the social environment to monitor, record and relay a variety of patient-related data, education and training to both patients and practitioners; examples frequent in the aging population are hypertension, myocardial infarction and hypoglycaemic episodes.9–11 mHealth influences behaviour such as physical activity, diet and medication adherence. 12 It reminds patients of upcoming appointments and locates lost patients, and its influence is independent of proximity to providers/caregivers. 12 If the demographic of the population that consumes a large percentage of NHE willingly accepts mHealth, then more research should be done to leverage its effect on outcomes and its acceptance in the standard of care.
Texting intervene have become a powerful use of mHealth. 13 Examples are smoking cessation, diabetes education, clinical appointment reminders and daily medication management. 14 Physicians using mHealth for remote monitoring can intervene before serious complications occur with the patients’ health such as chronic heart failure, arrhythmias, blood sugar levels and many other diseases. 14 Aging patients can use mHealth to track physical activity and adopt a healthier lifestyle, and mobile technology in general is becoming more secure.15–17 Technical challenges complicate the advance of mHealth, specifically in areas of semantic interoperability between disparate devices, scalability in linking healthcare providers to end-users, unified agreement among health care providers, universal availability, management and ownership of medical and health data, and determining who is managing all the information. 14
The purpose of this review and narrative summary is to identify and analyse facilitators and barriers to the adoption of mHealth solutions through the use of sensemaking. Due to the rapid rate of growth of mobile technology, we examined only a recent 12-month window, but we queried the largest medical indices for online or web-based interventions in which mobile devices enable care independent of proximity of patient to provider. We analysed articles in the final selection as narratives. We used narrative analysis and sensemaking to identify common themes in the literature. 15 Our intent is to identify facilitators and barriers most often mentioned in the literature to spur additional research that can provide leverage and overcome those barriers most prevalent in the literature.
Methods
We identified keywords from our initial research and matched with those existing on the database of Medical Subject Headings (MeSH), which is managed by the US National Library of Medicine. Figure 1 illustrates the searches performed in both PubMed and CINAHL, as performed on other reviews.18–22
Search with inclusion and exclusion criteria.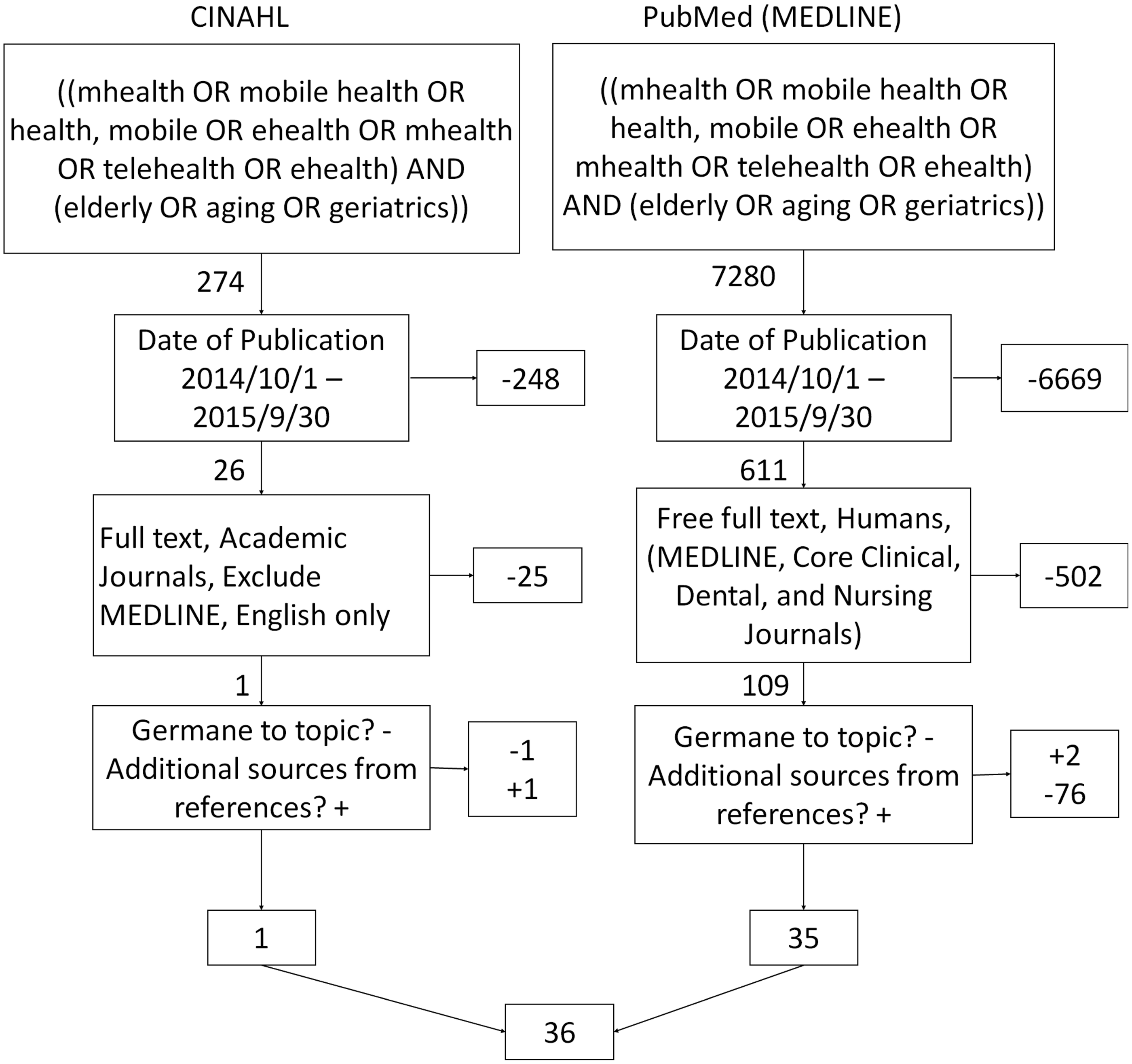
Searches were conducted in each database using the same key terms and Boolean operators. The initial search resulted in more than 7500 results. We included clinical trials, secondary data analysis and reviews. In light of our one-year analysis period (1 November 2014–30 September 2015), reviews were kept to increase the external validity of our review, as performed in other published reviews.20–22 After filtering for full text and academic journals, and excluding duplicates, we were left with 117 articles to review. CSK and MM independently read all 117 abstracts and made a recommendation of whether the topic was germane to our objective. A Kappa statistic was calculated for this initial review (k = 0.82, very strong reliability). The calculations are included in Figure 2. A consensus meeting enabled the authors to compare recommendations and agree on a final sample for analysis (k = 1.0). This process eliminated 68 articles. The references of the remaining 48 articles were scanned to identify sources that could yield value to our review, as performed in other published reviews, which added an additional three.20–22 Articles were read by at least two authors and if at least two authors agreed that the article was not germane, the article was excluded. This second recommendation removed an additional 12 articles (n = 36).
Kappa calculations.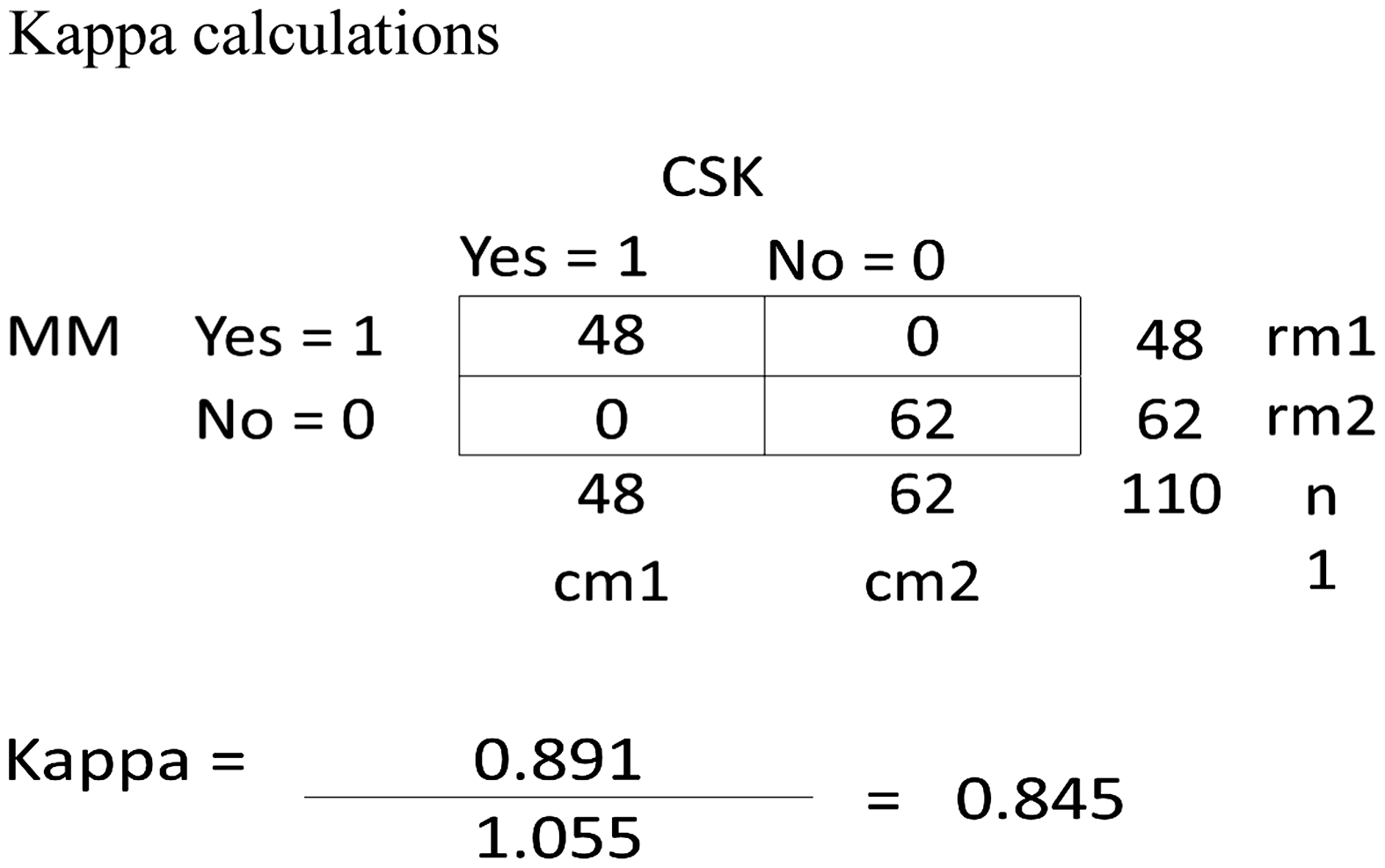
We noted facilitators and barriers to adoption along with general observations in a literature matrix. We met to review and discuss our observations, which we named consensus meetings, and we used narrative analysis and sensemaking to identify themes. 15 The authors can either add the sentence indicating no ethics approval was required to the end of the previous paragraph, or omit it, whatever is their preference, as it is obvious to all that a review of published material does not require ethics or IRB approval.
Research ethics
There were no human or animal subjects for this research; therefore this research qualifies for an exemption of the oversight body in the US for the independent committee requirement in the 1975 Declaration of Helsinki, known in the US as Institutional Review Boards (IRB) and regulated by the US Code of Federal Regulation (CFR) title 45, part 46.
Results
Over the course of the year that was analysed, 107 co-authors published 36 works that studied, analysed and discussed mobile technologies as applicable to the aging population. Articles originated from multiple countries, and a total of 103 factors of facilitation (60, or 60%) or barriers (43, or 43%) were observed. We identified 11 themes in both categories. The detailed list of facilitators and barriers to adoption from each study are shown in Appendix 2. Studies are listed in order of publication, with the most recent articles at the top.
Facilitators
About 28% more facilitators were noted than barriers (60:43). Mobile technology is accepted by the younger elderly (55–70 years), it is easy to wear, it can extend the existing support structure in an active or passive manner, it enables home care, it is highly customisable, it provides structure for those who need it, it can improve outcomes through early detection of symptoms through real-time channels of communication, and it can serve as a vector to increase medical literacy and medication adherence without the limits of proximity currently associated with a traditional method of delivery.2,23–48 The positive aspects of mobile technology seem to increase the quality of life and sense of independence for users, and it can increase a patient’s understanding and ability to self-monitor medical conditions which can lead to improved outcomes.23,30,31,33,35,36,38,41,45,47,49–59
Facilitators of adoption.

The theme most often mentioned was independence; identified in 11/60 of total occurrences (18%).30,33,35,36,38,41,45,47,49,56,57 mHealth enables self-monitoring, self-management, self-medication, overcomes issues of anxiety that can be experienced in crowded environments such as clinics, hospitals or even malls, and it enables patients to live alone and increase their health literacy. Themes of understanding and visibility were mentioned in 8/60 occurrences (13%).23,26,27,29,34,36,38,39,42–44,51,55,57 mHealth enables the elderly to increase understanding of conditions as well as terms and symptoms associated with their conditions from credible sources, it creates a sense of structure to those who need it, provides prompt feedback, and increases patient engagement. mHealth reveals to providers the challenges associated with caregiving in an active or passive manner, on a near real-time basis or data collection over several hours. This capability enables providers to track the status of a larger number of patients and analyse statistics on a high level. Effective, outcomes, and communicative were mentioned in 6/60 occurrences (10%).27,28,30,37–40,45,46,48,53,54–56,58 mHealth can change behaviour through feedback. It can mentally stimulate patients to delay the advance of dementia, improve triage decisions and arrangement of transportation through communication channels, increase self-efficacy augmenting existing interventions and thereby outcomes. The last two phrases highlight an overlap that was observed between these three themes. The outcomes theme included early diagnosis, mobile interventions to stimulate mental activity, encouraging a more active role of patients in their conditions, and increased medication and therapy adherence, and an enabler to detect falls.27,39,45,46,56,58 Mobile technology can also serve as a tool of communication to augment existing modalities to provide real-time data and increase the level of communication between patient and provider.28,30,37,40,45,54
Quality of life was mentioned in 5/60 occurrences (8%), and it encompassed observations that mobile technology can make life easier, convenient and more comfortable for the user.23,30,31,38 One study showed a positive impact on lifestyle indicators. 52 Mobile technology gives the elderly a sense of self-identity and emotional support for health habits which improves health-related quality of life.31,38
Cost, acceptance and access were each mentioned in 3/60 occurrences (5%). Cost included both equipment and delivery modalities.25,36,46 Acceptance of mobile technology by the elderly was mentioned in the introduction, and it was reinforced in the literature.23,25,52 The improvement of access included technology to enhance coordination of care without the limitations of proximity or mobility.40,46,55
The theme of convenient was only mentioned once (2%). The authors pointed out that elderly with dementia are willing to wear mobile technology, they willingly accept it, and they feel that it is convenient to use for multiple purposes. 23
Barriers
Barriers to adoption.
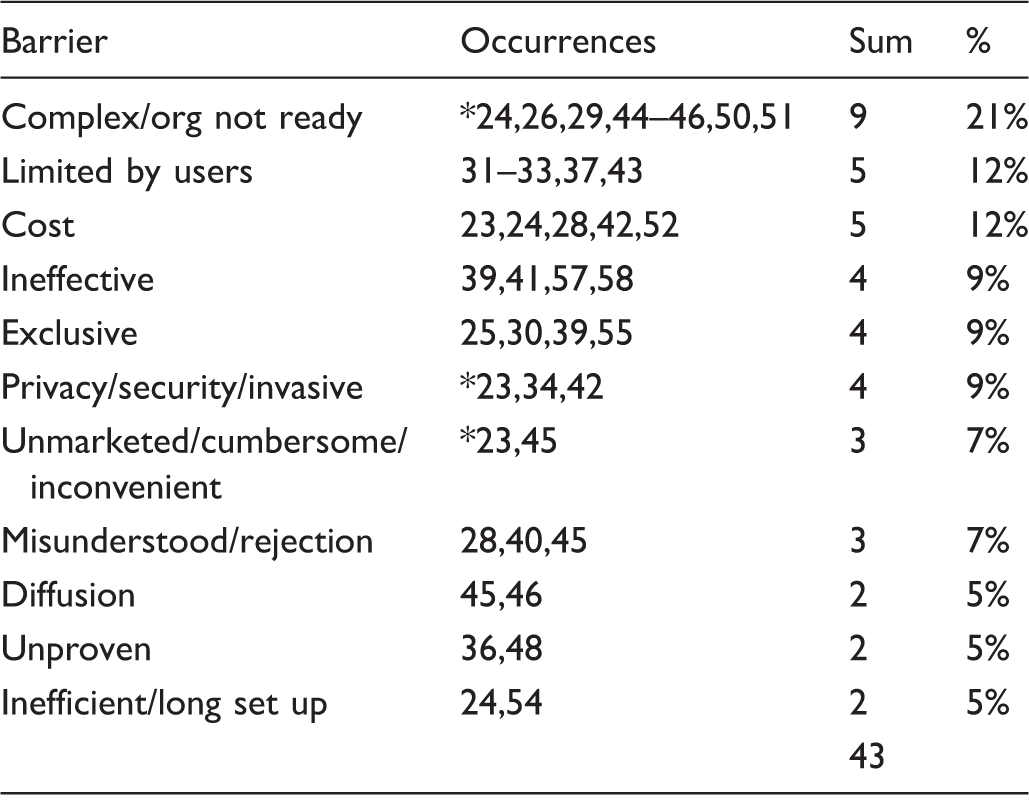
Note: *multiple themes mentioned in one article.
Of note, in the construction of the narrative analysis, we grouped several similar themes. For instance, the barrier of complex was mentioned eight times and org not ready was mentioned only once. We chose to group these two to provide more meaningful data. But this caused a problem because both of these themes were mentioned in the same article. To identify those inconsistencies and raise the reliability of this review, we identified the duplicates with an asterisk before the reference number.
By a large margin, the theme of complex/org not ready was mentioned the most often (9/43, 21%).24,26,29,44–46,50,51 Due to the cost of technology, this method of delivery of care highlights a digital divide, and it creates a sense of exclusivity and complexity which can create limitations based on the user’s abilities.23–25,30–33,37,39,43,45,46,55 This theme encompassed observations that organisations need additional technical personnel to handle the additional workload associated with this new modality of care.
Limited by users and cost were mentioned in 5/43 occurrences (12%). Users’ health literacy can greatly influence how they search and use information on the Internet, and this can be a significant issue for the elderly population with low literacy, and it could also be experienced through language barriers. Authors noted that the user’s inability to function on a mobile device may thwart the good that the application could provide, and gender plays a significant role in determining application usage. The other facet of this theme was the effects that social contracts could play in the patient’s interaction with the application. Doctors notice that patients will report adherence to, or cessation from, the desired activity based on pressure from family or providers to do so. Using mobile technology to report the same statistics could make it even easier to falsify data. This is an interesting contrast from other facilitating themes that implied the mobile device would remove the social contract all together. 36 But the social contract is also mentioned as a barrier again in the ineffective theme.
The themes Ineffective,39,41,57,58 exclusive25,30,39,55 and privacy/security/invasive23,34,42 were mentioned 4/43 times (9%). Authors identified that mobile interventions may be inadequate to address the onset of mental decline and that if data is misrepresented, more urgent or complex assessments may not be readily addressed without human involvement. The exclusive theme appeared in several ways: a digital divide between classes; technology that is limited to just those with a smartphone; a modality that may only be sensitive to time and context measures of hospital and clinical-based assessments; and one study only measured results from adult, well-educated, white females. The theme of privacy/security/invasive was not a surprise. Mobile technology has commonly been the subject of issues of privacy, security and invasion of privacy and security for all ages. The elderly would be a greater risk to this barrier because the elderly has less time to recover from a breach.
Themes of unmarketed/cumbersome/inconvenient23,45 and misunderstood/rejection28,40,45 occurred 3/43 times (7%). While cumbersome and inconvenient are self-explanatory, unmarketed is less so. The latter element of the theme pointed out that many consumers are not aware of the capabilities that mobile technology can offer. The former theme addresses a lack of education concerning mobile health technology and the fact that some patients refuse to self-manage their conditions. The latter explains that the adoption of mobile technology is slow and that skills using text are not ubiquitous.
The last three themes were mentioned 2/43 times or 5%: diffusion,45,46 unproven36,48 and inefficient/long set up.24,54 Diffusion emphasises that adoption of mHealth is still relatively slow. Unproven tells us that there are very few RCTs in this area, and the efficacy of mobile technology to increase adherence or cessation has not been established.36,48 The theme of inefficient/long set up identifies the complexity that this technology can insert into an already long visit for primary care and the technology takes a significant amount of time to customise.24,54
Discussion
Since mobile technology can also serve as a tool of communication, it augments existing modalities to provide real-time data and increase the level of communication between a patient and provider. Adoption of mobile technology has many characteristics that fit diffusion of innovation, which is a 50-year-old discipline that explains the uptake of innovation. 59 This review analyses studies, articles and other reviews concerning the topic of mHealth and the aging population. Diffusion is a special type of communication concerning a new topic, and mHealth is a relatively new modality to deliver healthcare. 59 Communication is identified as a common theme in six articles.28,30,37,40,45,54 Diffusion also deals with social change, and mHealth applications involve social change and the acceptance of this modality of delivery of care to a specific elderly population. 58 Acceptance is mentioned three times as a facilitator23,25,52 and three times as a barrier (misunderstood, rejected).28,40,45 Diffusion is even mentioned multiple times in the narrative analysis of the studies, but it is mentioned as a barrier because of how long it takes for the spread of this technology and associated acceptance.45,46 This last point addresses the last dimension of diffusion which is time. Time is mentioned twice as a barrier; specifically in relation to long set-up times.24,54
There were some similarities of themes even within the same article that were identified as both facilitators and barriers. For instance convenience was listed as a facilitator when discussing how easily some mHealth devices can be worn, but the same article mentioned the obtrusive nature of other wearable mHealth devices. 23 While this might seem to be a dichotomy of themes, the article referred to the convenience of a smartphone but the obtrusive nature of the video vest that was used for one study. Another example of this is the effectiveness that mental stimulation can have on prolonging the onset of dementia, which our reviewers identified as effective in one aspect of the disease. 39 However, the authors noted that mental stimulation was only one factor that may delay the onset of dementia. Our reviewers identified this as ineffective because it would not apply to all of the potential dementia sufferers in the aging population. 39
There may be themes that appear confusing in their context. Diffusion was listed as a barrier instead of an enabler. The reviewers used the term diffusion as a barrier because adoption is slow or there is a lack of texting ability among some of the elderly.45,46
The facilitators identified by this review can serve as levers to encourage desired behaviour and create greater visibility and extend existing support and care from both family and providers. The barriers identified by this review offer great opportunities for researchers as topics of RCTs in the future to better understand and overcome them. Application developers should recognise and focus on the facilitators identified in this review as opportunities for greater diffusion of mHealth for the elderly. Providers and administrators should both recognise the additional modality of care for the elderly in mHealth, and they should look for ways to enable it. Policymakers should continue to find ways to pay for this capability through reimbursement codes for physicians and grant money for development. This last point is the lynchpin that will make or break mHealth and will ultimately determine if it can be used to augment current long-term-care efforts, and enable early detection of conditions such as dementia.
Comparison
Chiarini et al. conducted a review of mHealth technologies for chronic disease and elders. 60 We attempted to classify different types of mHealth solutions implemented for elderly and other patients with chronic conditions. Our review focuses on mHealth and the elderly, but we do not include solutions for non-elderly populations. Our review classifies in terms of common themes. Another departure from the other review is that we did not include Google Scholar as a database source. From our experiences conducting systematic reviews, Google Scholar presents a very large number of non-peer-reviewed results which create false positives due to the immature nature of its filtering capabilities. The other review did not list a standard to organise the review.60,61 Our review built upon the international standard of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) by adding a narrative analysis.15,62
Theoretical contributions
A theoretical construct or framework could be derived from this analysis. About 50% of the facilitators identified were the feeling of independence, the increase in understanding and the visibility that mHealth applications enable for the elderly population. Additionally, about 50% of the barriers dealt with the complexity of mHealth, the limitations of users’ health literacy to fully understand the data presented by mHealth applications and the cost of the technology. Frequency of occurrence does not equate to importance of that issue, however the percentage of time that the facilitator or barrier is mentioned does equate to the probability of its mention based on our sample. In order to gain any external validity, however, a much larger sample would need to be taken. Additionally, the reviewers identified themes based on the idea of sensemaking, but we did not intend to infer causality. We are merely associating the themes as being facilitators of or barriers to the adoption of mHealth in the aging population.
Limitations
The reviewers identified limitations with this review. Any time a sample is selected for analysis from a population, there is a risk of selection bias which fails to achieve a representative sample. To control for this risk, the reviewers conducted a careful background search to ensure that we properly understood the population of mHealth and the elderly, and we discussed mHealth in a group setting to ensure a similar focus. We carefully crafted a search and selection protocol and executed it separately. We also met multiple times during each stage of the search and selection process to ensure that the protocol for selection could be repeated. The kappa value of 0.82 shows a very strong score of inter-rater reliability. Also, the limited time from for the data selection of 12 months can limit the external validity of the study. While other reviews examined up to five years (n = 42), our review with its focus on mHealth and the aging population did not analyse a significantly different number of articles (n = 36).
The articles selected for analysis were published in academic journals. However, the issue of publication bias exists because journals prefer to publish studies with significant findings rather than those with no statistical significance. 63 This means that studies without significant results are typically rejected for publication and they would not have had the opportunity for selection in this review.
Conclusion
Mobile technology interfaces with the elderly population as a mechanism to connect with children and grandchildren, and it appears to offer a modality of care recognised as a means to independence, greater medical literacy and higher quality of life. The same mobile devices, applications and technologies that have become indispensable in society today offer a modality of care that should not be ignored. As mHealth technologies grow, emerging applications of the technologies will enable life-changing uses for the elderly population. The application of mHealth has the potential to improve outcomes and change the course of health care as it is provided today.
Footnotes
Acknowledgements
The authors would like to thank Priyanka Karem for her assistance in locating and organising the many articles for analysis and for her work on the references.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.