
Abstract
Moulages are contact media – images made by contagion in the most literal sense: their production relies on a process in which the object to be reproduced is touched by the reproducing material. In the case of dermatological moulages, the plaster touches the infected skin of the sick and, once dried, serves as the negative form for the waxen image of a disease. Focussing on the collection of the Hôpital Saint-Louis in Paris, the article situates the production of dermatological moulages within the visual culture of 19th-century medicine and raises the question how an ancient technique of image production could become such a prevalent tool for the documentation of skin diseases during a period usually associated with the rise of scientific medicine and a reconsideration of theories of contagion in medical aetiology.
Dermatological waxes are not pleasant to look at (Figures 1 to 3). They appear very real and can make you feel sick, even though there is never a doubt that they are likenesses and not humans, made of wax and not of flesh. Based on imprints taken from a sick person’s skin, wax moulages are fragments of the human body cast in a mould. They are reproductions of visible symptoms, of rashes, blisters or scaly patches, conditions that harm the human’s physical surface, sometimes even eating into the flesh. It is hard to look at them without getting one’s own body involved, without the sensation of an itch or the feeling of disgust. And yet, there is a curious, maybe obscene, attraction, spurred by the appeal of lifelikeness that images made of wax tend to provoke.
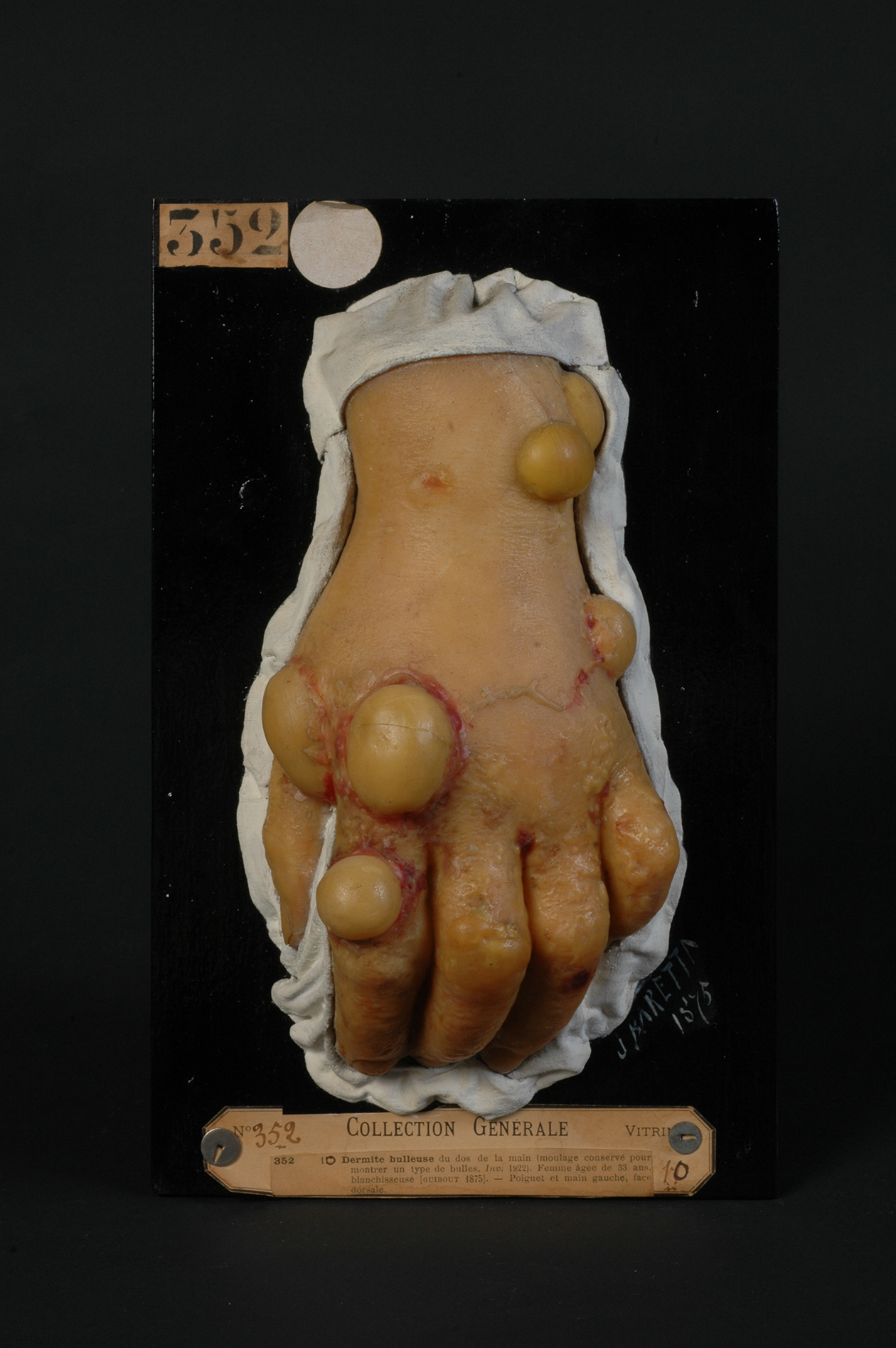
Jules Baretta, ‘Dermite huileuse du dos de la main. Femme agée de 33 ans, blanchisseuse’, 1875. Musée de l’Hôpital Saint-Louis, Paris, General Collection, moulage no 352. Photo: © F. Marin, P. Simon/Musée des moulages – Hôpital Saint-Louis – AP-HP.

Jules Baretta, ‘Lésions syphilitiques tertiaries de la langue; glossite scléreuse profonde, variété scléro-gommeuse’, ca 1867. Musée de l’Hôpital Saint-Louis, Paris Collection Fournier, moulage no 2. Photo: © F. Marin, P. Simon /Musée des moulages – Hôpital Saint-Louis – AP-HP.

Jules Baretta, ‘Épithéliome du nez, dévelopé sur un lupus tuberculeux ancient. Homme agé de 36 ans, professeur’, 1888. Musée des moulages, Hôpital Saint-Louis Paris, General Collection, moulages no 1364. Photo: © F. Marin, P. Simon /Musée des moulages – Hôpital Saint-Louis – AP-HP.
Dermatological wax moulages connect to the sense of touch in a number of ways. They reproduce diseases affecting the skin, seat of the organ of touch. During the 19th century, when the waxen reliefs became a widespread medium for dermatological documentation, skin was, as studies of skin have shown, described as simultaneously the individual’s delimitation and protective shield and the human’s most sensible organ, highly susceptible to pain, making the body most irritable at its surface (Benthien, 2002; Fend, 2017: 85–8; te Hennepe, 2007, and for a recent summary of skin studies, Lafrance, 2018). Over the course of the 19th century, the capability of the senses, including touch, was increasingly subject to minute measurement and mapping (Paterson, 2019). Medical discourse addressed skin as exquisitely sensible in all its parts and highly impressionable (e.g. Masse, 1886). The moulages are thus lifelike reliefs of conditions that were known to result in excessive stimulation of the sense of touch through pain or itch. In the emotional sense of the term, the moulages can in turn touch those who look at them and, by means of empathy, evoke malaises once felt by those whose lesions had been reproduced. Moreover, based on casts, they are contact images, the production of which involves touch, as the plaster used to make the mould converges with a sick person’s body. They are images made by contagion in the literal sense of the term given that the word derives from the Latin contagio, a compound of cum (with) and tangere (to touch). Analogous to the spread of a disease through direct or mediated contact between two bodies, the process of making the moulage involves physical contact of body and image. Finally, the moulages often reproduced symptoms of diseases that are and were considered to be contagious, most importantly syphilis, the sexually transmitted disease that caused major public health concerns in 19th-century Europe and whose study constituted a significant aspect of dermatology.
This article looks at the wax moulages from an interdisciplinary perspective: it brings art historical methods for the analysis of media and materiality to bear on issues concerning the history of science and medicine. It tries to understand what objects or images (in the broadest sense of the term) those pathological reliefs are and how they relate to other media recording morbid conditions during the 19th century: colour printing and more importantly photography, a contact medium too and one that entertained a close and at times even symbiotic relationship with wax moulages. I aim to explain the surprising success of the wax moulage, a medium that might have been perceived as retrograde during a period usually associated with the rise of scientific medicine and the virtues of objectivity. The article embeds the wax moulages within narratives of modern medicine while also challenging them by mobilising touch. Skin and the sense of touch are, after all, not only the object of dermatology but also the instruments with which this discipline is conducted: from the doctor touching the patient or handling a moulage, via the draughtsman recording a symptom with his hand to the mouleur applying plaster and fabricating a waxen relief. In turn, patients experienced touch as part of their suffering or when plaster was applied on their skin and they might have had their own relation to the touching objects cast from their bodies. The aim is to make touch an issue in the discussion of 19th-century medicine which has so long been dominated by notions of the ‘medical gaze’. I thus hope to bring tactile experience into the history of dermatology and medical media in the way Classen has done for a broader cultural history of touch (Classen, 2012). More specifically, I propose the notion of ‘contact’ as a way of thinking the history of contagious disease together with the entwined media history of casts and moulages on the one hand and photography on the other hand.
The Hôpital Saint-Louis and the Visual Practices of Dermatology
Dermatological wax moulages were made, collected and used in various centres of dermatological research as well as for popular health education in Europe and North America. 1 This article focuses on one particular collection of wax moulages – the Musée de l’hôpital Saint-Louis in Paris, with more than 4,000 pieces the largest collection of its kind. It still exists today and remains largely in its late 19th-century arrangement within purpose-built premises on the hospital grounds (Figure 4). 2

Photograph of the interior of the Musée des moulages at the Hôpital Saint-Louis in Paris today. © Musée des moulages, Hôpital Saint-Louis, AP-HP.
The history of the Parisian wax moulages is closely tied to that of the Hôpital Saint-Louis. Built in the 17th century, it was meant to alleviate the pressure on the overcrowded Hôtel-Dieu in central Paris and allowed for the isolation of the sick during times of epidemics (Gougerot and Brodier, 1932; Tilles and Wallach, 1996). Initially only used during such periods, it was turned into a permanently open public hospital in 1773 while remaining a facility for the treatment and confinement of contagious diseases, including smallpox and cholera. By that time, the growing city had incorporated the site into the now populated Faubourg du Temple. As part of the reforms to medical institutions in the aftermath of the French Revolution, it was transformed into a clinic specialising in the treatment of contagious and chronic conditions. Circumstances in the hospital were far from ideal even by late 18th-century standards. A report on an epidemic disease that raged in the hospital in 1798 describes the situation of the hospital, beginning with the fortunate aspects: located outside the city centre and surrounded by gardens, it was protected by hills from northerly winds and by elevated streets to the south from the exhalations of Paris. Ample courts allowed the sick to promenade and a generous distribution of the buildings guaranteed the circulation of air. At the same time, rooms are described as cramped and the author also mentions the proximity of the Mont Faucon, once the location of the Parisian gallows and later used as a rubbish dump from which badly smelling ‘miasma’ blew towards the hospital (Ruette, 1798: 27). Miasma was, at the time and by some physicians until the second half of the 19th century, considered to be a major ‘propagator of contagious diseases’ 3 . The notion came under pressure later on, but it is not entirely different from what is called – and feared – as aerosols today. In the monumental 60 volume Dictionnaire des Sciences Medicales published between 1812 and 1822 and an important platform for a younger generation of physicians (Plumauzille, 2010), ‘miasme’ and ‘contagion’ remain closely connected, all the more so as the entries are provided by the same author, Jean-Baptiste Nacquart (1813, 1819). The latter does however narrow down the definition of miasma, stressing that only ‘exhalations rising from the body of a sick person’ (1819: 354) are medically relevant. The hospital’s history is interlinked with the fear and management of contagion throughout, an aspect further discussed at the end of this article.
From 1800 onwards, the Hôpital Saint-Louis was turned into a specialised clinic focusing more and more on disorders of the skin and on venereal diseases. The transformation of the early modern hospital into a dermatological clinic is a good example of the structural changes leading to the formation of modern medicine in post-revolutionary France as described by Michel Foucault in his pivotal 1963 Naissance de la clinique. Analysing the modern clinic as an epistemological space in which the treatment of the sick goes hand in hand with the study of diseases, Foucault emphasised the role of vision and the interaction of the ‘visible and the articulable’ in the production of medical knowledge (Deleuze, 2006: 41–58; Foucault, 1973[1963]: 112–113). The notion of the ‘medical gaze’, arguably the most influential (and misleading) concept that resulted from the Birth of the Clinic, has since been critiqued as a rather crude account of the modern public health system’s power dynamics (Hannaway and La Berge, 1998: 34). Foucault himself later renounced the subtitle of his book ‘une archéologie du regard médical’ in favour of, as Gilles Deleuze has pointed out, a notion of visibility, adding the insight that ‘the places of visibility will never have the same rhythm, history or form as the field of statements’ (Deleuze, 2006: 43). When speaking of visibility, neither Foucault nor Deleuze had physical images in mind. Despite his emphasis on the role of vision in medical practice, Foucault never engaged with the rich imagery of 19th-century pathology and his Birth of the Clinic long predated the interest in scientific images that developed during the past three decades. However, I regard images as part of and contributing to the specific visual organisation of the clinic and mobilise them to further the argument of the distinct rhythm of visibility. This article is thus concerned with the different temporality of the pathological image and especially of the dermatological moulage, an object produced by casting which always recalls the moment of (more or less direct) touch and the former presence of what has been cast. 4 The cast and the precarious status of an allegedly unfiltered lifelikeness has served art historians like George Didi-Huberman (1997) to challenge certain traditional art historical narratives and to propose an anachronist way of writing history. Developing Foucault’s and Didi-Huberman’s propositions, I will show how the particular temporality of the dermatological moulage contests linear narratives about the development of scientific medicine and of the progression from ‘old’ to ‘new’ visual media. What is more, the wax moulages open the possibility of being in touch with the sick in a different manner and of seeing them as participants in both the making and interpretation of their own images.
Early on, the Hôpital Saint-Louis’ specialisation as dermatological clinic was stimulated by a prestigious – and richly illustrated – publication, Jean-Louis Alibert’s, 1806 Description des maladies de la peau observées à l’hôpital Saint-Louis. The atlas’s title already indicates the nosographic approach to the pathological conditions, the claim for visual empiricism and the significance of the site where the observations are made. In Alibert’s account, the dermatological clinic is an epistemological space in which diseases roam and progress until they are stilled by the eye of the physician identifying the moment when they present their characteristic features. During this fruitful moment (Alibert, 1806: vi; see also Fend, 2013: 152–5; and on ‘characteristic images’ Daston and Gallison, 2007: 82), the disease becomes visible as an entity perceived as a clinical picture.
The fact that Alibert illustrated his folio atlas with 52 coloured engravings by a prominent printmaker, Salvatore Tresca, demonstrates that the development of dermatological observation and diagnosis went hand in hand with the use of images (Figure 5). Alibert points out that accurate description in conjunction with the use of images allows dermatology to become a science (Alibert, 1806: xxj; Fend, 2018: 83). At the same time, the physician foregrounds the power of the prints and their colours to emotionally engage the readers and to form lasting impressions in their minds. (Alibert, 1806: xx; Fend, 2013: 153–156; Jacyna, 1998: 190–3). This dual potential of the images to aid and underpin dermatology’s ambition to be a science while addressing the affects is equally a quality of the wax moulages.

Salvatore Tresca after Moreau-Valvile, ‘Syphilide pustuleuse en grappe’, stipple engraving, coloured à la poupée, from: Jean-Louis Alibert, Descriptions des maladies de la peau, 1806. Credit: Wellcome Collection. Attribution 4.0 International (CC BY 4.0).
Wax Moulages: Making and Display
Image production was a continued concern at the Hôpital Saint-Louis and after early attempts to install a pathological museum featuring watercolours of skin diseases, the idea of building a collection of waxen replica gained momentum. The material wax and the technique of casting had already been used to document skin diseases elsewhere (Schnalke, 1995). Beyond the immediate diagnostic purposes, the building of a significant collection was meant to protect the status of the Hôpital Saint-Louis, and of France more broadly speaking, as the international centre for dermatology. The circumstances of the inauguration of the dedicated museum for wax moulages illuminate this. New facilities on the hospital’s premises, combining an outpatient surgery on the ground floor with a library and a museum space on the first floor, were constructed from 1882 onwards (Tilles and Wallach, 1996). The building was finished in 1886 and the moulages fitted into their vitrines, yet the official opening of the museum was delayed until 1889, to coincide with the centenary of the French Revolution, the Paris World Fair and the first assembly of the International Society of Dermatologists. The nearly 200 delegates met in the lecture hall surrounded – and by far outnumbered – by the waxen representatives of the sick. One of the attendants, the Viennese dermatologist Moriz Kaposi, reported that there could not have been a more fitting assembly hall praising its ‘wall decoration’ as ‘grave and scientifically stimulating’. 5
By the mid-19th century, physicians at the Hôpital Saint-Louis, namely Charles Lailler, who worked at the hospital between 1863 and 1887, had been actively seeking an artisan who would be able to provide such lifelike reproductions of skin diseases. In 1863, they found Jules Baretta, a manufacturer of trompe l’œil fruit made of papier mâché with a business in one of the famous Parisian arcades. According to an obituary for Baretta, Lailler was attracted by the ‘faithfulness’ with which the ‘nature, form and colour of the fruits were rendered’ and immediately hired the ‘passionate artist’. 6 Apparently, Baretta first familiarised himself with his new subject and accompanied doctors on their hospital rounds to learn the basics of dermatology along with – I propose – an expert way of seeing skin diseases. In parallel, he was experimenting with the materials and procedures for his moulages.
Like many other mouleurs, Baretta never put the specifics of his practice into writing. But judging from 19th-century manuals on the techniques of moulding, third person accounts of Baretta’s procedures, reports from more recent mouleurs and conservators (Schnalke, 2004) as well as contemporary re-enactments (Noirot, 2014), this much can be said about the making of dermatological moulages: To start with, a particular appearance of a disease to be reproduced had to be singled out by one of the physicians, in the manner already suggested by Alibert. In this first act of turning a disease into a characteristic image, a detail to be cast had to be chosen, before the patient was sent to Baretta, whose studio was situated on the hospital grounds. The patients must have been informed to some extent about the procedures, as their active participation was required. Nineteenth-century manuals for moulders describe how, when working from ‘living nature’, the person who serves as a model had to be conveniently positioned before fine plaster was spread over the respective body part, and the patient too had to stay still while the material set (Lebrun and Magnier, 1850: 51–57). They needed to know in advance that the initially cold plaster develops heat and slightly contracts the flesh while hardening. When moulding a person’s face, particular precautions had to be taken, as eyes and mouth must remain closed while breathing needs to be enabled. Once the plaster had dried, it could be removed, and, in the case of a dermatological usage, provided a negative form into which melted and pigmented wax was poured in several layers to produce the actual moulage. Given the complexity of the procedures, this can hardly be called mechanical reproduction. Baretta’s manual skills were crucial. What is more, the relief of the wax cast had to be reworked and refined, and in some cases, a mix of casting and sculpting was used. This has been established recently by French sculptor and historian Fabien Noirot, who re-enacted Baretta’s technique taking as his example the moulage of a man with a tumour on his nose (Figure 3). 7 This lesion would have been difficult to cast without hurting the patient, but it is also technically impossible to cast certain cavities, making caving and sculpting inevitable for a successful three-dimensional reproduction. Finally, colour was added to the waxen relief, and, at times, hair was applied to make eye brows, eye lashes or other kinds of hair depending on the bodily region involved. Such supplements had diagnostic value only insofar as their absence might have felt like a lack, like part of a condition. In excess of the reproductive process of casting, these addenda serve to increase the lifelikeness and effect of the moulage.
Touch was involved in multiple ways in the making and display of the moulages: it was mobilised, controlled and prohibited. A patient’s skin came in contact with the plaster when the mould was formed, yet probably not directly. As Noirot convincingly argues, a fine film – probably peau de baudruche, a material made from the skin of beef intestine – separated the plaster from the human skin to protect delicate and often moist growths or other cutaneous eruptions. While contact was needed, a blending of fluids had to be avoided and pain or discomfort for the patient at least minimised. The haptic abilities of the hand were required to make moulds and casts, and the mouleur would have touched the sick as well as the tools and materials used to fabricate the waxen reliefs.
Once the moulage was finished, touch seems to be held at bay by elaborate framing. The unsightly margins of the waxen reliefs are covered by white cloth and the objects are fixed on dark boards, to prevent sight of and contact with their hollow interior. Once the moulage was mounted, it would have been the boards that were handled, rather than the impressable wax and with it the replicated lesions. 8 The assembled objects were signed and dated by the moulder, who left an authoritative trace like an artist. Furthermore, they were usually accompanied by a label listing the name of a condition, the name of the person who carried it along with basic information about their age, gender and profession. Last but not least, the label typically lists the name of the physician who treated the patient and selected the features of the disease to be retained in wax. Usually it also refers to the dermatological literature in which the case was further discussed. The label thus guided the viewer to the adjacent library in which the connected publications could be consulted. This ensemble of framings and references turns the moulage into a scientific object (see in more detail Fend, 2018).
Casting and Photography
Commissioning dermatologists and specialist visitors alike praised the wax moulages as highly effective means of dermatological study. Devergie lauded them as ‘reproductions of diseased and disease as complete and truthful as possible’ stressing that Baretta is a moulder and not a modeller. 9 The fact that the waxen reliefs are based on casting rather than being sculpted imitations is key for the truth value the moulages were granted. It is thus important to make a distinction between models and moulages from today’s perspective as well. As Anna Maerker (2011) has argued in her study of the famous anatomical models at La Specola in Florence, it is crucial to be specific about what kind of representations we are dealing with in terms of materiality, mode of production and the narratives that surround them. In the same way Maerker’s Model Experts addresses and theorises the anatomical waxes at La Specola as models, the dermatological reliefs need to be considered in their quality as casts. While models and moulages share the material wax – the lifelikeness it affords and its association with flesh – the one is modelled, and represents an ideal anatomical body even if it is inside out, the other is a reproduction of one of countless manifestations of a disease.
The wax moulages’ character as imprints is essential for their recognition as scientific tools, and the 19th-century impulse to capture skin diseases through plaster, and to preserve their appearance in the form of highly resembling wax reliefs, owed a lot to the popularity and esteem of casting as a trustworthy means of reproduction. Casting had an unprecedented revival during the 19th century and was frequently used for the making of memorial objects like death masks (Pointon, 2014), as an artistic medium in its own right but also for the duplication and documentation of artefacts. While ancient sculptures had been copied via plaster casts since the Renaissance, casting was now used as part of a number of scholarly or scientific endeavours from anthropology and medicine to forensics and architecture (Flour, 2010; Papet, 2001).
The fact that moulages are crafted from imprints is also the reason why the dermatologists ranked them equal with photographs. Photography did not supersede the moulage as a means of dermatological documentation, as some historians of dermatology have suggested; rather, the two media are products of the same era, as art historian Mary Hunter has also argued in her study of the Péan collection within the Musée des moulages (Hunter, 2008, 2016: 145–152). The heyday of wax moulages coincides largely with that of analogue photography, a medium based on the contact of light with a photosensitive material. From the 19th century onwards, photography has been perceived and theorised as an indexical medium (Geimer, 2007), and casts were understood in a similar manner. The post-mortem portrait became a popular subject of photography and ancient Roman death masks were seen anew through the camera lens. As an effect of the encounter between the two media, the linguistically difficult and blurred distinction between the hollow imprint that serves as the mould for the convex cast was now referred to in the language of photography as ‘negative’ and ‘positive’ (Crowley, 2016; on death masks and photography see also Pointon, 2014).
As for dermatological moulages and the particular case of the Hôpital Saint-Louis, there is first of all a chronological conjunction. The first plaster moulds were taken almost exactly at the same time as the first photographs of skin lesions. Baretta was hired in the early 1860s when dermatologist Alfred Hardy also initiated the production and collection of photographs of skin diseases and started working with ophthalmologist and photographer Arthur de Montméja. The first published outcome of their collaboration, the Clinique photographique de l’hôpital Saint Louis, illustrated with hand-coloured photographic prints, appeared in 1868. Baretta had finished his first successful moulage in 1867. 10 The photographs and wax moulages look of course very different from one another, as each medium produces its distinct mode of resemblance (Figures 6 and 7). Take a photograph and moulage of ‘Acne’, for example: both show the face of a man frontally, with the facial features (wittingly or not) dominating over the symptoms. Yet, while the moulage evokes a person at peaceful rest – the procedure of casting necessitates the shutting of the eyes – a stern look confronts us from the photographs. The photograph adheres to some degree to the conventions of portrait photography, as it is less focused and includes elements of clothing. But both the moulages’ and the photographs’ claim for truth were predominantly based on their means of production.

Jules Baretta, ‘Acné rosée, couperose érythémato-pustuleuse. Homme agé de 35 ans’, 1875. Musée de l’Hôpital Saint-Louis, Paris, General Collection, moulage no 342. Photo: © F. Marin, P. Simon /Musée des moulages – Hôpital Saint-Louis – AP-HP.
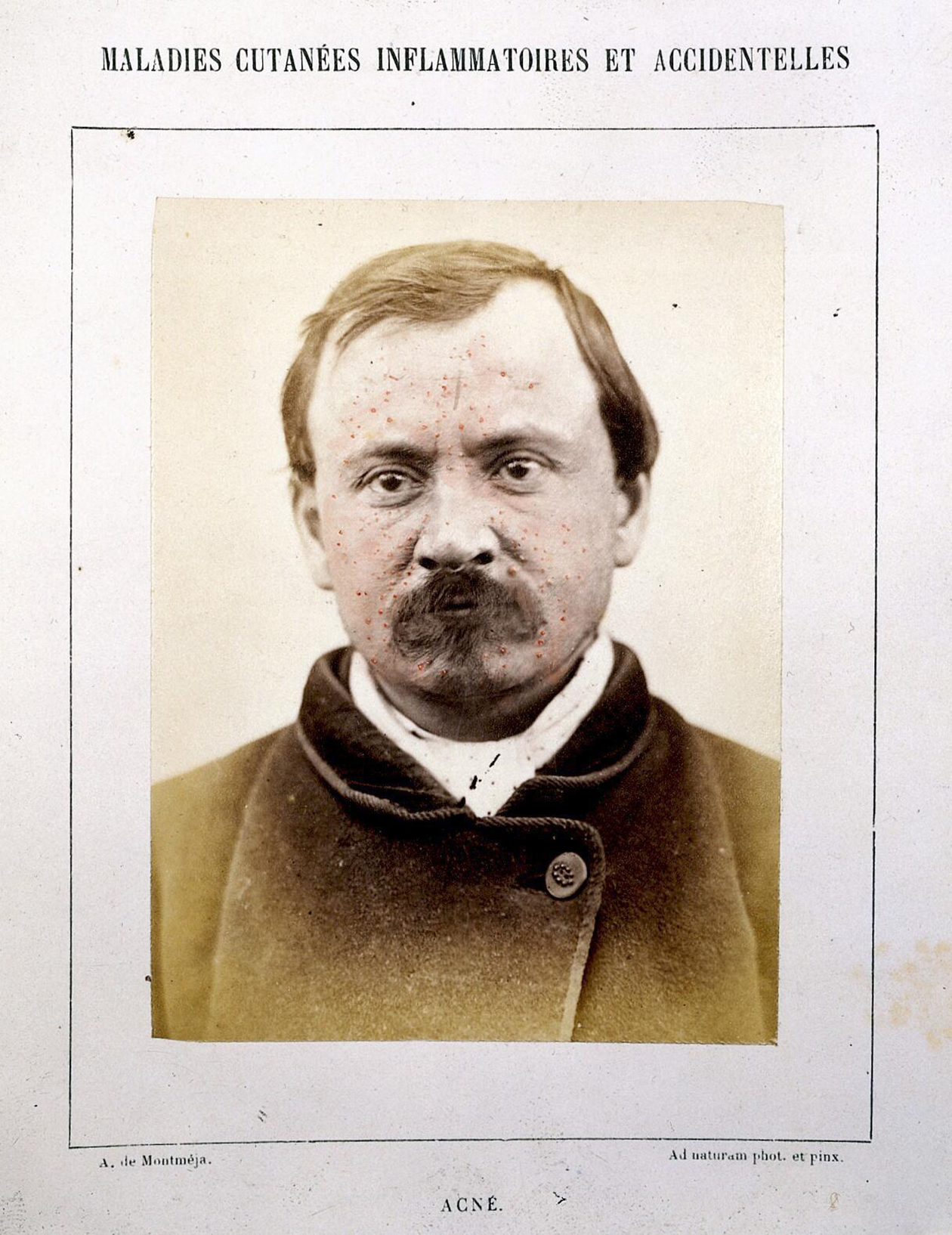
Photograph of a man with ‘Acne’. From Hardy and Montméja, Clinique photographique de l’Hôpital Saint-Louis, 1868. Credit: Wellcome Collection. Attribution 4.0 International (CC BY 4.0).
No matter what the degree of human intervention in the choice of the motif, the focus, the taking of the photograph, the later colouring of the print or the reworking of the wax cast, the trustworthiness of the respective image relied first on their indexicality or the mechanical aspect of their production and only second on the lifelikeness enhanced by colouring. Drawings, wax moulages and photographs were all named ‘reproductions’, and the ways in which photographs and casts captured ‘nature’ were accounted for in exactly the same terms. Praising the photographs of his Clinique photographique de l’hôpital Saint-Louis, Hardy states: The artistic, and no doubt most important, part of this work was entrusted to one of my students, Mr Montméja, who adds to a profound knowledge of skin diseases an incontestable talent as a photographer and colourist; we can say that his plates represent nature caught in the very act. (Hardy and de Montméja, 1868: I) [The] genius of the caster […] shall guide him in the choice of poses and in the use of the appropriate means to make him capture nature in the very act [saisir la nature sur le fait]. This should allow the moulder to fix, on solid matter, a fleeting and transient but characteristic moment. (Lebrun and Magnier, 1850: 52, see also Papet, 2001: 74–77)
This association of photography and casting as media that reproduce nature ‘purely’ and mechanically raises the question whether the wax moulages should be considered within the framework of what Lorraine Daston and Peter Galison (2007) have termed ‘mechanical objectivity’. 12 The authors identify photography as a prime instrument of mechanical objectivity because, according to the rhetoric surrounding scientific photography, the camera produced images in a disinterested manner devoid of subjective human intervention. I suggest that the popularity of casts for scientific and scholarly documentation relied on the fact that they were (to an extent) mechanically produced and could thus partake in the idiom of mechanical objectivity. However, whether the casts were able to operate in this manner depended on the context in which they were made and circulated. Similar to memorial casts, the medical imprint with its potential to evoke the moment of touch when the plaster had been in physical contact with a suffering person can prompt a sentimental response.
Wax moulages are complex objects as they can and could be – even for their initial makers and users – troubling objects. First of all, nobody ever denied the significance of the handmade, that is the expert artistic and dermatological skills needed for the making and later colouring of both the waxes and the photographs. On the contrary, Baretta signed his moulages, thus pointing to his authorship and marking them with a gesture known from painters. Many of his contemporaries lauded him concurrently for his skills as moulder and for his talent as an ‘artist’ (Doyon, 1888: 57, Feulard, 1889; Jeanselme, 1923: 219). The artisanal and the artistic seem to be going hand in hand. In the passage from the Nouveau manuel du mouleur, it is in relation to artistic practices of casting that the phrase ‘saisir la nature sur le fait’ occurs, while the authors also point to a fortunate pose for casting, chosen thanks to the ‘genie du mouleur’. With this latter phrase the authors insinuate intervention and intuition using a term – genius – more typically associated with artists.
The uncertainty as to whether to focus on the artistic aspect (the moulage as a fabricated object involving an author’s intervention) or the mechanical element of the reproduction (associated with the authority of the imprint) surrounded casts and wax figures since the Renaissance. The extreme resemblance ceroplasty could achieve was potentially also a problem, as it could be regarded as the effect of mere copy and hence a lack of artistry (Didi-Huberman, 1997; Grootenboer, 2013). By the 19th century, this mode of reproduction and the material wax already had a long-lasting connection: in Roman antiquity, images of ancestors were made of wax and based on casts. Used in funeral ceremonies, they were simultaneously associated with lifelikeness and death and were meant to substitute for the once living figures they represented (Didi-Huberman, 1999; Klier, 2004). This also held true for the early modern effigies of the king, which were crucial actors during the kings’ funeral rites in England and France between the 15th and 17th century. In France, the waxen effigy, meant to represent the king ‘après le vif’ (both after the life and as if alive), was based on casts of the face and substituted for the monarch during the precarious interim period between the death of the old king and the enthronement of the new. The later aristocratic art of wax portraiture transformed after the French Revolution into the popular wax displays of Madame Tussaud’s in London or the Musée Grévin in Paris (Kornmeier, 2008; Schwartz, 1998). Here, the possibility of confounding representation and represented had become part of the wax museums’ entertainment strategies. This development was dismissed by early historians of ceroplasty, notably Viennese art historian Julius Schlosser (Schlosser, 1910; Panzanelli, 2008), as a vulgarisation of a once serious art form. Yet again, the potentially ‘excessive mimesis’ (Siegert, 2014) became a predicament of ceroplasty. I propose that the longue durée history of ceroplasty and the imprint as well as the revival of the wax figure and of casts were very present when moulages became a key medium for the documentation of skin diseases.
Reproductions, Ex Votos and Substitutes
Casting as a technique and the wax figure were tied to traditions that the 19th-century medical adaptations could not entirely control. This becomes particularly clear in a later dermatological atlas where wax moulages, photography and new printing techniques interact in multiple ways: Ernest-Henri Besnier’s Musée de l’hôpital Saint-Louis. Iconographie des maladies cutanées et syphilitiques: avec texte explicative published in 1895–1897 which appeared simultaneously in English translation. As the title manifests, the atlas remains somewhat undecided whether it wants to be a catalogue of the museum or a study of the visual manifestations of skin diseases and syphilis. What is more, patients and moulages become interchangeable in Besnier’s Iconographie as photographs and waxen imprints coincide in new ways. Each case study is organised around an existing moulage from the museum which was then photographed for the publication and reproduced in photo-lithochromes (Figure 8). Photo-chromolithography is a hybrid procedure, used quite successfully around the turn of the 20th century before being superseded by photomechanical techniques of colour printing (Twyman, 2013: 326). Reproduced on a full page, the colour prints also aim to approximate the size of the moulages and to emulate the latter’s life-sizedness. There is always a reference to the museum piece, indispensible for the practicality of the book as a museum guide. However, the respective case notes often skip a step in the complex process of mediation, simply taking the print as a direct image of the condition. One case note, for example, is introduced as follows: ‘The photo-lithochrome, which accompanies the text, shows the right hand and wrist of a man suffering from a rare form of Dermatitis herpetiformis’ (Besnier et al., 1895: 11). Through their very elision, the moulages are thus treated as proper substitutes for the sick. Praising the faithfulness and truth of both the moulages and the photographs of them, Besnier no less than Henri Feulard in his introduction to the volume clearly align the two indexical media (Besnier and Fournier, 1895–1897: III-IV).
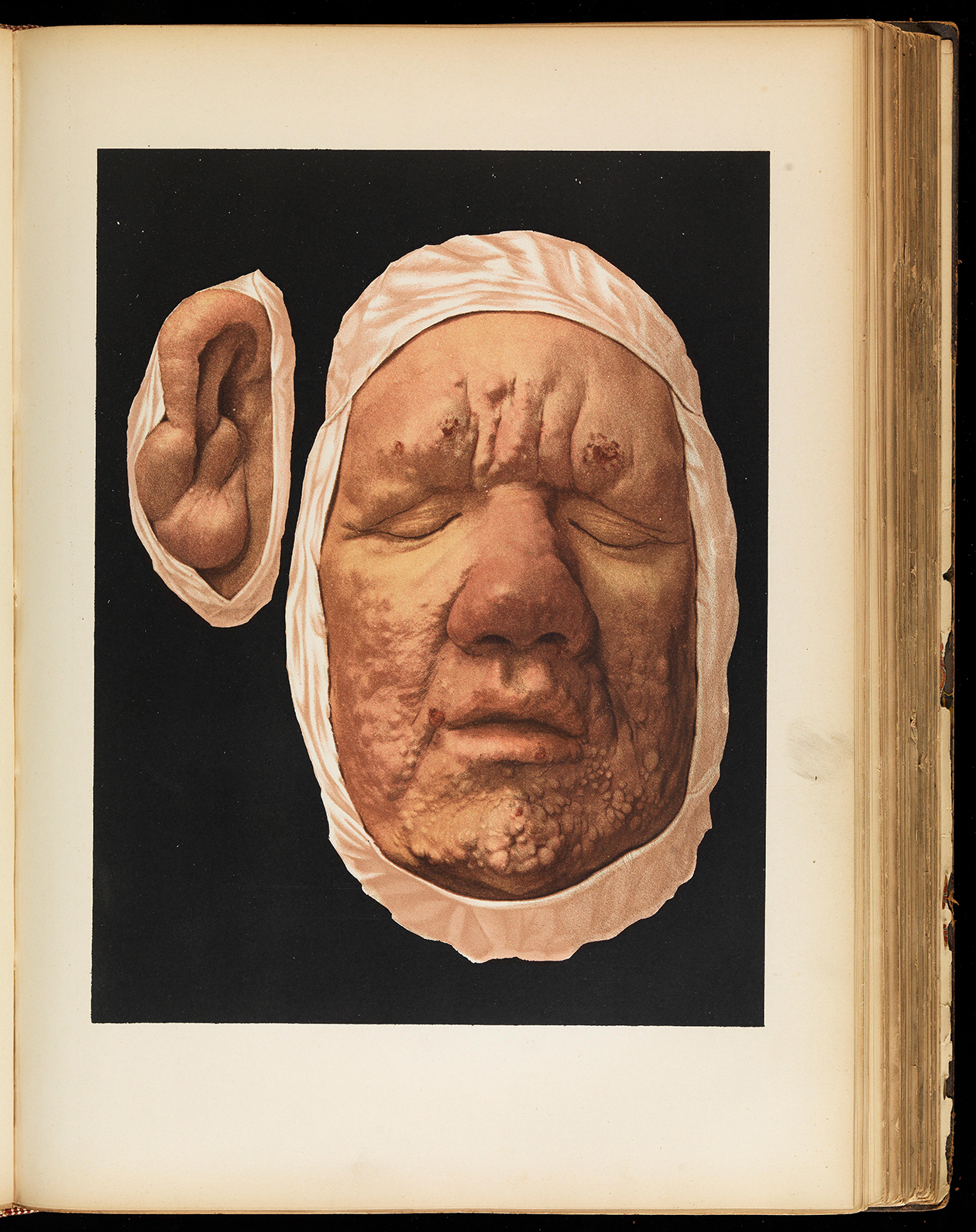
Photo-lithochrome of a wax moulage of a 27-year–old man suffering from ‘Lèpre tuberculeuse typique’. From: Ernest Besnier, Musée de l’hopital Saint-Louis. Iconographie des maladies cutanées et syphilitiques: avec texte explicative, 1895-97, plate 15. Credit: Wellcome Collection. Attribution 4.0 International (CC BY 4.0).
The photo-lithochromes receive further visual commentary, exceeding the didactic strategies of the museum itself. Most of the reproduced moulages are accompanied by a printed line-drawing which facilitates the recognition and description of a condition with pointers linking individual symptoms with their nomination. Photographs, taken directly from patients and, in some cases, from microscopic probes, complement the visual documentation. They are printed in much smaller size, in black and white, and integrated into the text (Figure 9). Such differently sourced and printed images work jointly to illustrate a case note referring to distinct aspects of the verbal ‘observation’. Typically, the note sets off with a description and interpretation of the visible features of a condition as recorded in the moulage and illustrated via the photo-lithochrome, the understanding of which is aided by a line-drawing. In addition, microscopic analysis is frequently consulted and documented via circular microphotographs (Figure 10). This method helps with the identification of diseases, but, as Besnier makes plain, is always subordinate to the macroscopic autopsy (Besnier et al., 1895: 145).
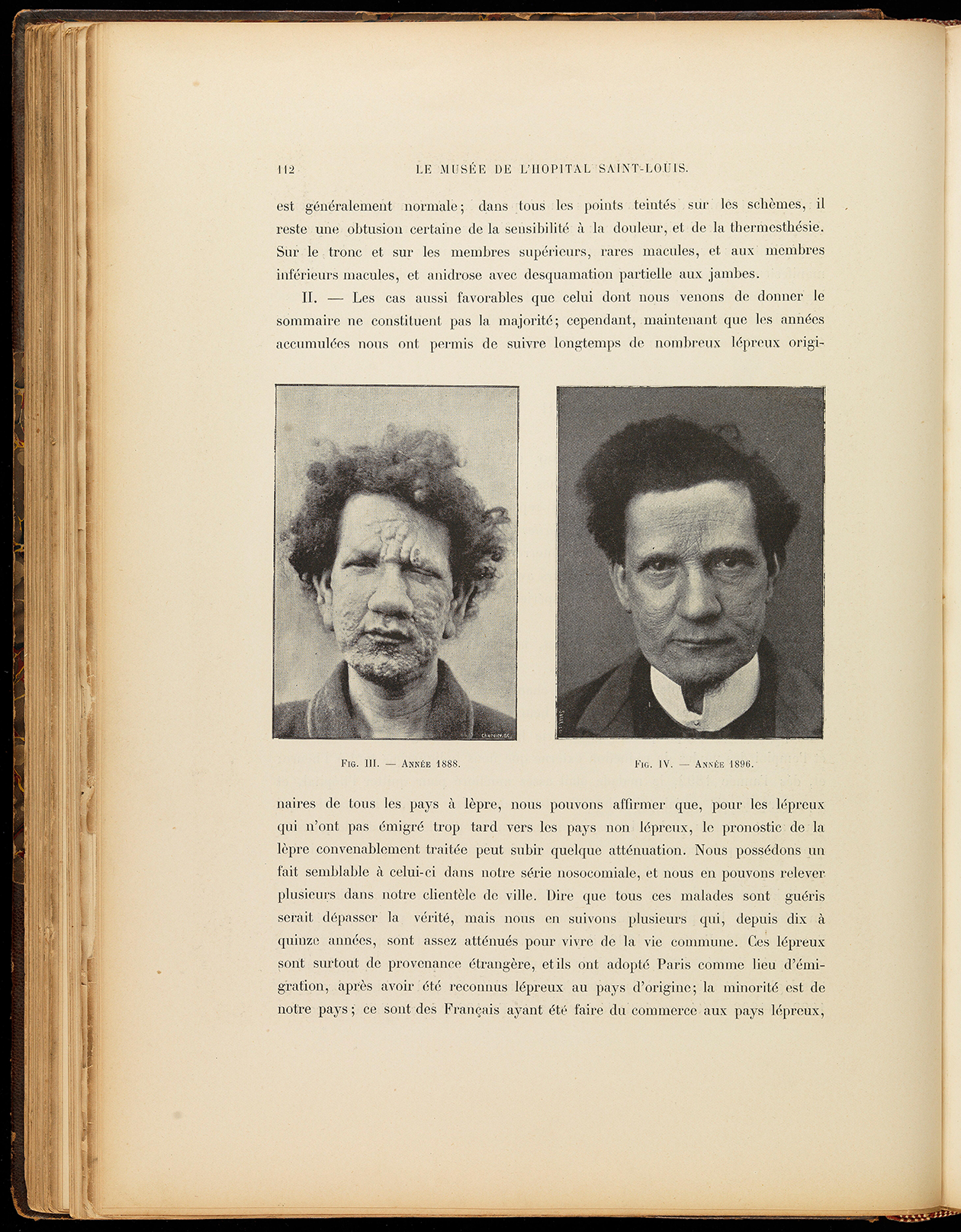
Photographs of patient suffering from ‘Lèpre tuberculeuse typique’, before and after cure. From: Ernest Besnier, Musée de l’hopital Saint-Louis. Iconographie des maladies cutanées et syphilitiques: avec texte explicative, 1895-97, p. 112. Credit: Wellcome Collection. Attribution 4.0 International (CC BY 4.0).
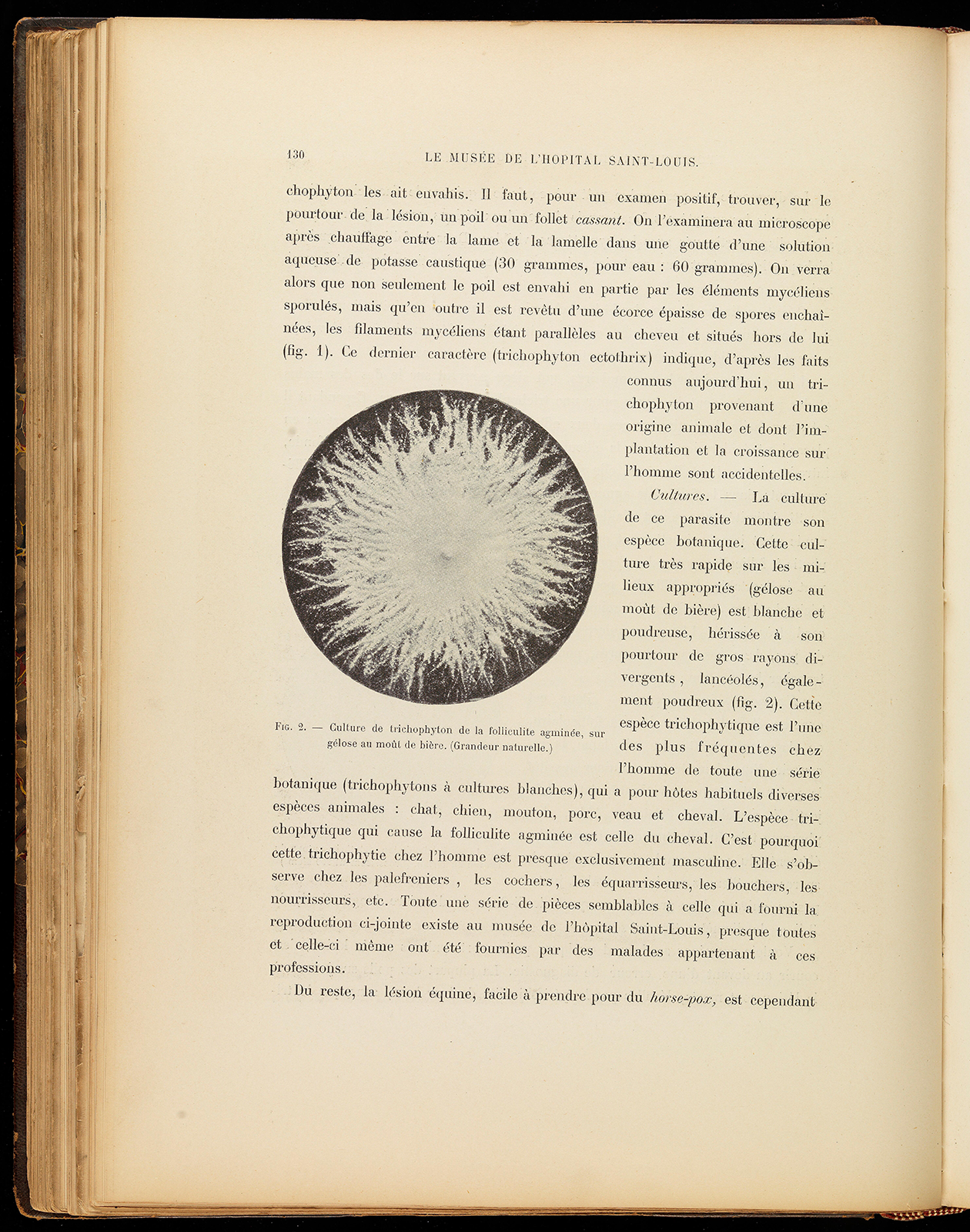
Page with microphotography of ‘Culture of Tripophyton’. Ernest Besnier: Musée de l’hopital Saint-Louis. Iconographie des maladies cutanées et syphilitiques: avec texte explicative, 1895-97, p. 130. Credit: Wellcome Collection. Attribution 4.0 International (CC BY 4.0).
The close coordination of images and text along with the combination of different types of images enhance the scientific claim of the publication, similar to the systematic order and reference system in the museum itself. Still, the large photo-lithochromes of the moulages also interrupt the reading process, as they emerge in their colourful presence from the background’s uniform blackness. The moulages’ quality as objects, reliefs mounted onto a wooden board, is downplayed as the body parts are cut out around their linen wrappings. The black boards are replaced by the non-descript background, and Baretta’s signatures are eliminated. Rather than the moulder’s wax work, the lifelike images come to the fore and with them the bodies of the sick. The waxen reliefs return to be pieces of skin, vehicles for the reddened relief of lesions, and in their white cloths they emerge from the dark almost like ghosts.
The photo-lithochromes act as moulages just as the moulages operate as substitutes for living patients. While this makes sense within the practicalities of medical didactics and diagnosis, allowing for a focused engagement with stilled symptoms, the strategies of image making, handling and display still inherit early modern understandings of the image surrounding the king’s lifelike effigy or magical beliefs in ex-votos. Ex-votos, offerings given in gratitude to a deity or saint after the fulfilment of a vow, often come as more or less lifelike imitations of body parts, when the vow made relates to a health condition. They were frequently based on casts and made of wax, a material that came into use for ex-votos in Europe since the late Middle Ages. Like the dermatological moulages, ‘wax anatomical ex-votos fragmented the human body into critical functioning (and malfunctioning) parts’ (Holmes, 2009: 161). Displays of ex-votos in churches and the arrangement of the body fragments at the Musée de l’hôpital Saint-Louis also show remarkable similarities and historians of dermatological waxes have compared moulages and votives before (Bastos, 2017; Schnalke, 1995). In fact, wax moulages and ex-votos were explicitly likend in 19th-century France and both were associated with miraculous healings (see in more detail Fend, 2018: 95–96). The Nouveau manuel complet du mouleur expresses the wish that pathological museums comprising dermatological wax moulages showing a patient before and after a successful cure, ‘would remain like the ex-votos of churches to attest their miraculous healings’ (Lebrun and Magnier, 1850: 219). The waxen ‘before-and-after’ images discussed in the Manuel were made and displayed in a spa and meant to be seen by actual and potential patients, in the case of the latter as a form of advertisement. While the scenario was different in a clinical setting, one still wonders whether the sick treated at the Hôpital Saint-Louis also got to see the casts taken from their bodies. As they were required for their making, they must at least have seen their condition preserved in a mould. At this moment, they might well have had the feeling that the disease was taken off them, externalised. Some of the patients possibly believed in the magic potential of the imprints that were later turned into waxen reliefs, hoping they helped in healing a disease like ex-votos. Perhaps the secularised give and take scenario of the modern clinic – I offer to be an object of study in exchange for a cure – was not always as cynical as Foucault had it in his Birth of the Clinic (1963). The wax moulages cannot simply shake off the traditions of religious and magical practices they partially inherit and sit uncomfortably within the parameters of modern medicine.
Contagion
Dermatological wax moulages are contact images that have the power to also emotionally touch as they simulate uneasy encounters with diseases and diseased. Physically touching the moulages was a potentially disquieting experience too. While they were, of course, touched during their making and arrangement in a vitrine, and must have been occasionally handled, the waxen reliefs as displayed in the dermatological museum were made first and foremost for visual study. The framing itself encourages ocular focus. At the same time, the attachment on the wooden board made sure that eventual manual users touched the object and not the waxen replica of the disease. The lay-out of the Musée de l’hôpital Saint–Louis, described by Kaposi shortly after its official opening (1890:190), regulates and partially restricts visual and tactile access to the moulages. The fragile items were kept behind glass to be protected from being touched by their audience. I suspect though that it also works the other way around, the observers are protected from the lifelike imitations of conditions they might have been reluctant to touch, even if they were physicians or students of medicine.
The showcases themselves are installed along the walls of the museum’s large rectangular hall, forming a kind of enclosure from the outside world as the space is solely lit through a glass roof and by artificial light (Figure 4). Spiral stairs in the corners give access to a gallery with a second storey of vitrines. Behind the scenes, accessible via a narrow hallway, are showcases mainly dedicated to cases of syphilis. The lethal venereal disease, documented with a great many reproductions of infected genitals, thus occupied a secluded space even within this specialist display and was kept out of immediate sight for the dermatologists entering the museum or listening to lectures in the hall. This channelling of visibility can be attributed to a sense of decorum within the medical profession, but we might also see it as a tribute to the lifelikeness of the colourful wax moulages and to the fact that these powerful objects might themselves prompt a fear of contagion and be contagious in their affective potential. It has been argued for popular medical displays like Hartkopf’s traveling anatomy museum that ‘the ability to depict disease without contagion was important for the wax display in the later nineteenth-century anatomical museum as well, where the subject matter was often pathological in nature’ (Sandberg, 2002: 43–44). However, while promoters of popular medical shows, in France in particular the Musée Spitzner touring during the second half of the 19th century and featuring among other objects moulages by Baretta, might have stressed the safety of their displays, they could not stop the imaginary dimension of contagion and actually exploited the spectacular and scary effects of the waxen replica. Contagion – and fear of it – was a constant companion in 19th-century Europe. Infection through physical contact was especially associated with venereal diseases, most importantly syphilis. Concern about the transmission of the then incurable disease resulted, among other things, in a system of public regulation and medical checks of prostitutes. The production and use of moulages taken from prostitutes was part of this monitoring and the associated study of syphilis (Hunter, 2016: 126–128).
Many wax moulages at the Hôpital Saint-Louis reproduce diseases that were at the time known to be contagious, spread by more or less direct physical contact. It is however not impossible that they were also physically infectious or perceived as such. The fact that objects could be contagious was regularly discussed in the medical literature. In the early modern period, the porous material wax was, as Lucia Dacome has pointed out, ‘considered prone to absorbing bad air and was therefore regarded as a potential carrier of disease’ (2017: 6). Nineteenth-century dermatology, including the doctors at the Hôpital Saint-Louis, were heavily involved in the virulent medical debate about contagion and its mechanisms (see e.g. Fournier, 1857, 1860). While Alibert did not list contagion among the first causes of dermatological conditions, he considered contact with objects to be a potential source of contagion. Clothes and hats can be contagious, he warned, suggesting in relation to an especially virulent form of syphilis that ‘even the use of the same furniture’ can spread the condition (Alibert, 1806: 185). In the later 19th-century medical literature, this list was extended to the physicians themselves and in particular their clothes as likely transmitters of disease (see e.g. Bernheim, 1877: 20–22). The entire hospital environment including the museum, with its waxen objects wrapped in linen and its furniture, was thus conceivably contagious.
As is well known, the question of contagion was highly topical in mid- and late-19th-century life sciences and the regular discussions at the weekly meetings of the French Académie nationale de Médecine demonstrate that it was a matter of national urgency. The scientific stakes were as high as the sociopolitical ones, since questions of medical contagion were inextricably linked to those of moral contagion. Microbiological explanations of the causes of infectious diseases impacted on biopolitical measures such as governmental interventions into public hygiene (Aisenberg, 1999: 66–112; Latour, 1988). Historians of medicine have described this moment as a turning point in the development of modern, scientific medicine. In France, it was notably Louis Pasteur and his microbiological research that contributed to the gradual transformation in medical accounts of diseases, now increasingly understood and treated on the basis of their microbiological causes (Amsterdamska, 2009; Mendelsohn, 2003; on the role of portraiture for the making of Pasteur’s scientific persona also Hunter, 2016: 37–107). Dermatology and the medical practices at the Hôpital Saint-Louis were part of this shift. For Alibert, working at the beginning of the century, environmental and behavioural causes of diseases (such as poor diet, heavy drinking, unhealthy working conditions, unfavourable climate) were – for most conditions – prioritized over contagion. In conjunction, observation with the naked eye, close description and the use of images made for him the scientific method of dermatology. By the 1860s, the microscope played a key role in the identification of skin and venereal conditions. The programmatic opening pages of the newly founded Annales de dermatologie et syphiligraphie, closely associated with the Hôpital Saint-Louis, do not only make a case for the need of the specialist journal but also highlight public health issues, aetiology and microbiological analysis.
One might think that the increasing acceptance of bacteriology and the inclusion of microscopic medicine in dermatology made wax moulages obsolete, given their focus on the symptoms visible to the naked eye. But the opposite was the case: dermatological wax moulages saw their greatest distribution and popularity as a medium of medical study and documentation in the decades before and after the turn of the 20th century. At the Hôpital Saint-Louis, a space for microscopy was from the start part of the museum space. Divided from the large hall by the shelf units containing the moulages, the work space was lit by large windows (Kaposi, 1890: 190). The scrutiny of the life-size symptoms of the disease with the help of wax moulages went thus hand in hand with the microbiological quest for their causes, suggesting that etiology complemented rather than replaced nosographic methods and visual autopsy. Moulages were produced and used for another 70 years or so, remaining effective tools of dermatological documentation, study and training as well as potentially contagious in the literal and in the figurative sense.
Conclusion
Wax moulages initially prompt an affective response before potentially leading to a more studious approach to the skin conditions they reproduce. Both are part of how they work and part of their success in the institutional setting of the dermatological clinic. Between the mid-19th and the mid-20th century, the waxen reliefs were fully functional instruments of medical documentation, diagnosis and teaching. Their esteem relied on the one hand on their verisimilitude, their ability to accurately represent morbid phenomena aided by the flesh-like quality of the material wax. On the other hand, it was based on the fact that the moulages derived from casts which allowed them (to some extent) to be discursively framed as mechanical reproductions. As this article has shown, the discourses surrounding this aspect of their production lent them a truth value similar to that of photography, and the two seemingly so different dermatological media were closely interconnected.
At the same time, it is crucial to consider the material histories of wax and the imprint along with the 19th-century connotations and usages of the stuff and the process, be it the popular wax museum, spectacular displays of medical waxes or death masks. I have argued that museums of dermatological wax moulages established their medical purpose with this history in mind and in distinction from their popular counterparts. The moulages were unable to leave these histories and associations behind and remained open to magical beliefs in the power of images. There was the potential for patients to reappropriate the images cast from their bodies, and the medical professionals too inherited (wittingly or not) pre-modern notions of and practices around the image when they treated the wax moulages as substitutes rather than representations of the sick. What is more, both their understanding as contact images and their functioning as substitutes of the sick relied on a mode of production that owed its authority to the fact that the moulages had once, in a mediated way, touched the sick, been in intimate contact with sores and orifices. It is the moulages’ lifelikeness and reliance on touch that brings the diseases precariously close – even if physical distance is kept and guarded by the glass of a vitrine. This effect has not gone away: the lasting presence of these indexical images bridges historical times, as they still seem to connect us with the pains somebody suffered from more than a hundred years ago. In their peculiar temporality and persistence deriving from their reliance on contact they have the potential to trouble linear narratives concerning the development of modern medicine and the replacement of presumably old by new media. The waxen reliefs challenge notions of an allegedly detached mode of medical vision; they appeal to the sense of touch through the eye and through touch they can breed the fear of contagion.
Footnotes
Acknowledgements
This article is based on research on wax moulages conducted over a period of more than a decade. During this time, I gave numerous papers on various aspects of this material and I can only generally thank everyone who has contributed with their comments, questions and insights to the ways my thinking about these objects has evolved. More specifically, I am grateful to the participants of the Research Seminar organised by UCL’s Department of Science and Technology Studies on 7 February 2018, for their excellent questions and for pushing me to think harder about the physical aspects of contagion. Most importantly, I would like to thank Henning Schmidgen and Rebekka Ladewig for inviting me to the conference ‘Symmetries of Touch’ and for providing the opportunity to be part of this special issue.