
Abstract
Objective
Out-of-pocket payments for prescribed medicines are still comparatively high in Portugal. The abem program was launched in Portugal in May 2016 to aid vulnerable groups by completely covering out-of-pocket costs of prescribed medicines in community pharmacies. This study assesses the impact of the program on poverty and catastrophic health expenditures.
Methods
A longitudinal study was carried out with the analysis of several program databases (from the beginning of the program in May 2016 to September 2018) covering the cohorts of beneficiaries, daily data on medicines dispensed, social referencing entities, and solidarity pharmacies. The study provides estimates of standard poverty measures (intensity and severity) as well as the incidence of catastrophic health expenditures.
Results
More than 6000 beneficiaries were supported (56.8% female, 34.7% aged 65 or over), encompassing 127,510 medicines (mainly nervous system and cardiovascular system) with an average 26.9% co-payment (payments totalling €1.5 million). The program achieved substantial reductions in poverty (3.4% in intensity, 5.6% in severity), and eliminated cases with catastrophic health expenditures in medicines that would have affected 7.5% of the beneficiaries.
Conclusions
Findings confirm a continuous increase in the number of beneficiaries, enabling access to medicines especially for the vulnerable elderly, and a sizable impact on eliminating out-of-pocket payments for medicines in the target population.
Introduction
Poverty is a multidimensional concept with diverse causes and is closely associated with health. It is a public health concern because poor people are at risk of not having the means to prevent and treat a disease, and poor health can lead to people becoming impoverished.1,2 To address these concerns, there is a growing number of actions being carried out that seek to resolve social and health inequalities.2,3 Even so, the fact remains that health care costs represent a heavy financial burden on individuals. A European study showed that 45% of the people interviewed considered health care costs a financial burden, with 11% describing them as a heavy financial burden. Looking at expenditures on medicines specifically, 39% declared the costs represented some financial burden, and 13% reported them to be a heavy financial burden. 4
In 2016, 25.1% of the Portuguese population was at risk of poverty or social exclusion, above the European Union’s (EU) average of 23.7%. 5 Minors are the age group most affected, and significant inequalities exist, especially among the long-term unemployed, migrants, ethnic minorities, and poor people living in rural areas. 6 Data from 2020 reveal that despite an improvement, 19.8% of the population was still at risk of poverty or social exclusion. Additionally, 28.1% of the Portuguese population self-reported unmet health care needs due to financial reasons, almost twice the EU average (14.8%). 7 Of the three possible reasons for unmet health care needs (financial, distance and/or lacking transport, and waiting lists) Portugal was one of the 12 countries where respondents stated financial reasons as the number one cause for why they did not receive the health care they needed. 8
In 2017, 57.6% of Portuguese health expenditure financing was supported by the National Health System (NHS) and the Regional Health Services of the Autonomous Regions, while 27.2% was funded by households, through direct out-of-pocket (OOP) payments. The remainder was financed by other public health subsystems, private entities, and insurance companies. 9 Pharmaceutical and other medical non-durable goods represented 23.3% of households’ expenditures on health. 9 This is an alarming situation for vulnerable populations. Reducing the share of OOP expenditures in total health expenditure is highlighted in a set of eight policies that reduce health inequities among adults, ranked by the highest average reductions in limiting illness reported among adults in 24 countries.10,11
Portugal has a high level of OOP payments, at 45% of total expenditure on medicines, higher than the EU average (34%). Not surprisingly, 10.1% of the Portuguese population in 2016 avoided using medicines because of their cost. 12 Another study found that 17.6% of those aged 15–64 years old and 26.8% of those aged 65 years or more, had on at least one occasion not purchased all the medicines they needed because they could not afford them. 13 Overall, the frequency of this situation increased for the whole population from 15.1% in 2013 to 19.7% in 2015. 13 Likewise, almost 30% of the elderly population in Portugal recently stopped purchasing some prescribed medicines, with 40.1% perceiving OOP expenses on medicines as having become higher. 14 High OOP costs can have a negative impact on medication adherence, health outcomes, and the quality of life. This experience is not unique to Portugal, and there have been recent health financing policy reforms and measures taken in several countries to deal with these concerns. 15
Dignitude, a private institution, was founded with the mission of developing solidarity initiatives to promote the Portuguese population’s wellbeing and quality of life. 16 In May 2016, Dignitude launched the abem program, a solidarity partnership of institutions from the social sector with the private health sector and local governments nationwide. The aim of this program was to ensure the access of vulnerable groups to medicines and to guarantee that prescription medicines be free for underprivileged households, with no OOP payments. All eligible households meeting low-income criteria, referenced by local entities such as municipalities and local charitable institutions, are entitled to the benefits and to an abem card. Each beneficiary goes to the pharmacy with their prescriptions and presents the abem card. This entitles them to have 100% of their OPP expenditure on all prescribed medicines paid for by the program. While their OOP expenditure is covered by abem, the remainder of the medicine’s cost are met by the NHS and other payers. The program is funded by Dignitude, with contributions from private donors and the referral entities. 16
The aims of the current study are to (1) identify the main characteristics of the abem program and (2) quantify the impact of the program by estimating its effect on poverty and on the incidence of catastrophic health expenditures.
Methods
Study design
A longitudinal, descriptive study was carried out, from the beginning of the program on 24 May 2016 through to 30 September 2018, using microdata on program participants.
Databases and longitudinal analysis
Data were retrieved from several program databases: (1) the beneficiary database (grouped by households), which includes sociodemographic data, all the beneficiaries that are or have been active in the abem program, with the entry date and suspension/end dates; (2) the medicines-dispensed-daily database, which includes the prices of the medicines, the abem co-funding, the quantity, the dispense date, and the beneficiary record; (3) the reference entity database, where the beneficiaries/households inclusion criteria used by each referring entity are described; and (4) the participating community pharmacies, with geographic information.
We linked additional databases to this data, covering (1) the drug classification, which encompassed the medicine’s characteristics (international non-proprietary name, pharmaceutical form, dosage, package dimension, Anatomic Therapeutic Chemical (ATC) classification, and generic classification); and (2) the Drug Consumption Information System repository of pharmaceutical NHS sell-out data (SICMED), which contains data from a voluntary panel of about 80% of all pharmacies in Portugal, to extrapolate the total reimbursed pharmaceutical market in Portugal, with the various reimbursement plans and rates.
Microdata from the Portuguese Household Budget Survey (2015/2016) 17 were also used for the analysis, to estimate patterns of expenditures on food, as these are part of the eligibility criteria.
The statistical analysis performed presented central tendency and dispersion measures for continuous variables, and absolute and relative frequencies for categorical variables. The data cover household demographics, prescription medicines acquired, and the direct funding paid by the abem program.
Poverty measurements and incidence of catastrophic health expenditure
For evaluating the poverty reduction impact of the abem program, three indicators created by Foster et al. were calculated. 18 These were the poverty rate, poverty intensity index, and poverty severity index. These measures are frequently used in economic studies of poverty and their use is supported by a vast academic literature.
The poverty rate is defined as the proportion of the population whose equivalent income is below the poverty line, defined as 60% of the median equivalent income. It was calculated using the following formula
The poverty intensity index was calculated based on the formula
The poverty severity index was calculated by the following formula

The poverty rate is a relatively crude measure in that it treats as equal individuals who are only one euro below the poverty line and individuals who have incomes lower than that. The poverty intensity and severity indexes, by contrast, are sensitive to the differences across poor households’ incomes. Note that the poverty intensity index has a linear relationship with the relative difference between the individual income and the poverty line, and can be interpreted in terms of the transfers needed to eradicate poverty. On the other hand, the poverty severity index has a quadratic relationship, with the relative difference between the household’s income and the poverty line, putting even more weight on the individuals further away from the poverty line. 18
Our other analysis estimated the incidence of catastrophic health expenditures situations avoided by the program – an outcome originally proposed by the WHO in 2000. 19 OOP payments in health are defined as catastrophic when they exceed a threshold above which the household cannot afford to pay for them. Depending on the sources of available information and the context, this threshold can be defined in various ways.19,20 In this study, it is defined as the difference between the household’s estimated income and the median expenditure on food for a household with a similar composition. The WHO considers several alternative levels of OOP payments in health as catastrophic. Here, since we consider OOP only for prescription medicines, we consider expenditures over 10% of the household disposable income as catastrophic.
Although direct information on eligible abem household incomes was unavailable, it was possible to estimate the upper limit of income for each household, since the eligibility rules used by the reference entities are known.
The softwares used were Microsoft Access Database®, Microsoft Excel 2016®, and SAS (SAS Institute, Cary NC, USA).
Results
Characteristics of the program
The abem program grew from its implementation in May 2016, until September 2018, as did the number of institutions referring the beneficiaries/households to the program. In the first year, only 13 entities took part in the initiative, but by 2017 there were 43 entities involved. In September 2018, 95 entities were part of the program, spread over the Portuguese mainland and the islands of the Azores and Madeira. Growth was also seen in the number of participating pharmacies. In the first year, 188 pharmacies were involved, almost doubling to 356 in the following year. By September 2018 there were 528 pharmacies involved, representing 18.1% of all pharmacies in Portugal.
The number of beneficiaries has also increased. When abem was first implemented, 447 beneficiaries took part in the initiative, whereas at the end of the study, 6305 people were supported by the program. Initially, most of the beneficiaries were from the Lisbon metropolitan area, but this soon expanded throughout the country. In December 2016, of the 1702 beneficiaries, 54.9% were female, with a mean age of 42 (SD 27) years. The most prevalent age group was 41–64 years old (27.8%). In September 2018, the number of beneficiaries was 6305, with a mean age of 51 (SD 25) years, with the most prevalent age group being 65 years or older (34.7%), followed by 41–64 years old (33.3%), and with the female ratio increasing to 56.8%.
There has also been a growing trend in the number of beneficiary households. At the start of the program, 183 households were in the program, whereas at the end of the study, there were 3253 households.
As at September 2018, the number of people per household varied from 1 to 11, with an average of 1.9 and a median of 2.0. People in the household include mostly applicants (51.5%), their offspring (22.3%), spouses (18.6%), and grandchildren (2.5%). Other cases, such as son or daughter-in-law, parents, siblings, grandparents, and others comprised 5.1% of the total.
Of the 6305 total beneficiaries of the program, 3786 were consumers, that is to say, had used their card when obtaining medicines. This means 60.0% of beneficiaries have benefitted from abem’s co-funding arrangement, while the rest are potential consumers who have not yet used the card to obtain medicines but who are also protected against the financial risk. We compared the percentages of beneficiaries and consumers by age group. As expected, certain age groups consume more medicines than do others: the age groups 41–64 and 65 years or older had a higher percentage of consumers than did other age groups. While the percentage of beneficiaries over 65 years was 34.7%, this age group had 40.9% of the consumers. For the 41–64 group, the total percentage was 34.7% beneficiaries and 35.8% consumers. The female subgroup displayed a similar pattern, accounting for 56.8% of beneficiaries and 60.1% of consumers. These patterns can be seen in Figure 1. Population pyramid by gender (green: men, orange: women) and age group for beneficiaries versus consumers (dark line).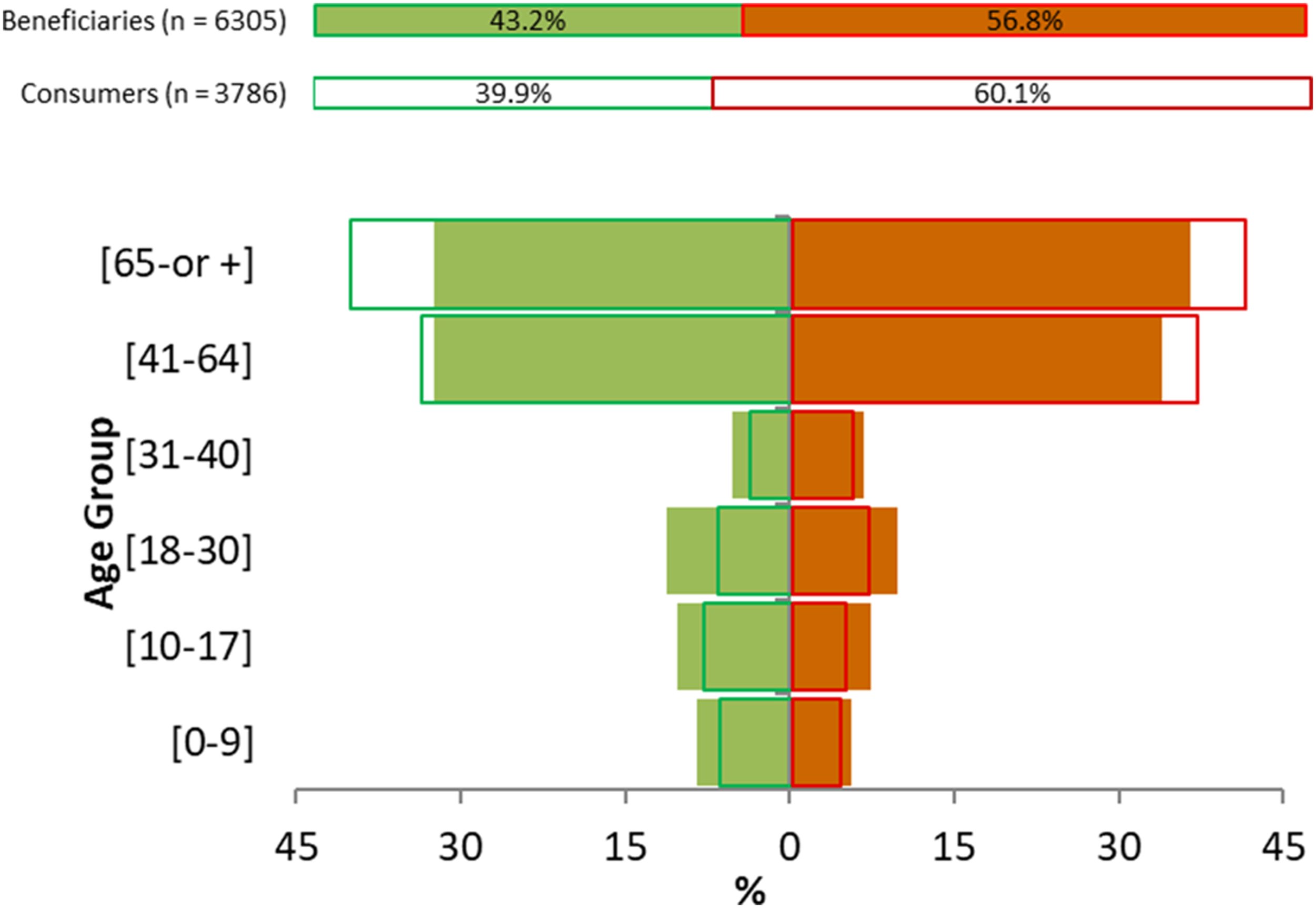
Since the start of the program, the total cost of the medicines supplied to consumers was €1.5 million, of which €0.403 million (26.9%) was provided by the abem program. The average monthly co-payments amount per abem consumer varied from €16.23 (May 2016) to €20.62 (July 2018).
Since the program started, the total number of medicines dispensed was 127,510 packages in 43,064 dispenses, about 3.0 packages per dispense. On average, an abem consumer benefited from 3.5 (May 2016) to 6.6 (January 2018) packages per month. About 48% of the packages dispensed were generics.
To gain a deeper knowledge of the medicines dispensed under the program, we analysed the therapeutic groups, using the ATC/WHO classification. 21 Regarding the share of abem co-payment, 31.7% of the funding went to medicines for the nervous system (ATC N), 21.8% for the cardiovascular system (ATC C), and 10.6% for the respiratory system (ATC R). ATC N represented 35.1% of quantities dispensed, ATC C 23.8%, and medicines for the alimentary tract and metabolism (ATC A) 12.6%. These different shares and ranks highlight the heterogeneity among therapeutic groups of consumers’ co-payments. These top three therapeutic groups comprise 71.5% of the total packages dispensed.
To assess if the abem cohort had consumption patterns similar to those of the NHS market, a correlation study was performed across ATC groups between NHS co-funding shares and the program’s co-funding shares. Figure 2 shows that from the level two ATC/WHO analysis of the drugs dispensed under the abem program, there is a high positive correlation (r = 0.9301) with the NHS dispensed medicines. Correlation across ATC group shares between abem reimbursed medicines and NHS reimbursed medicines.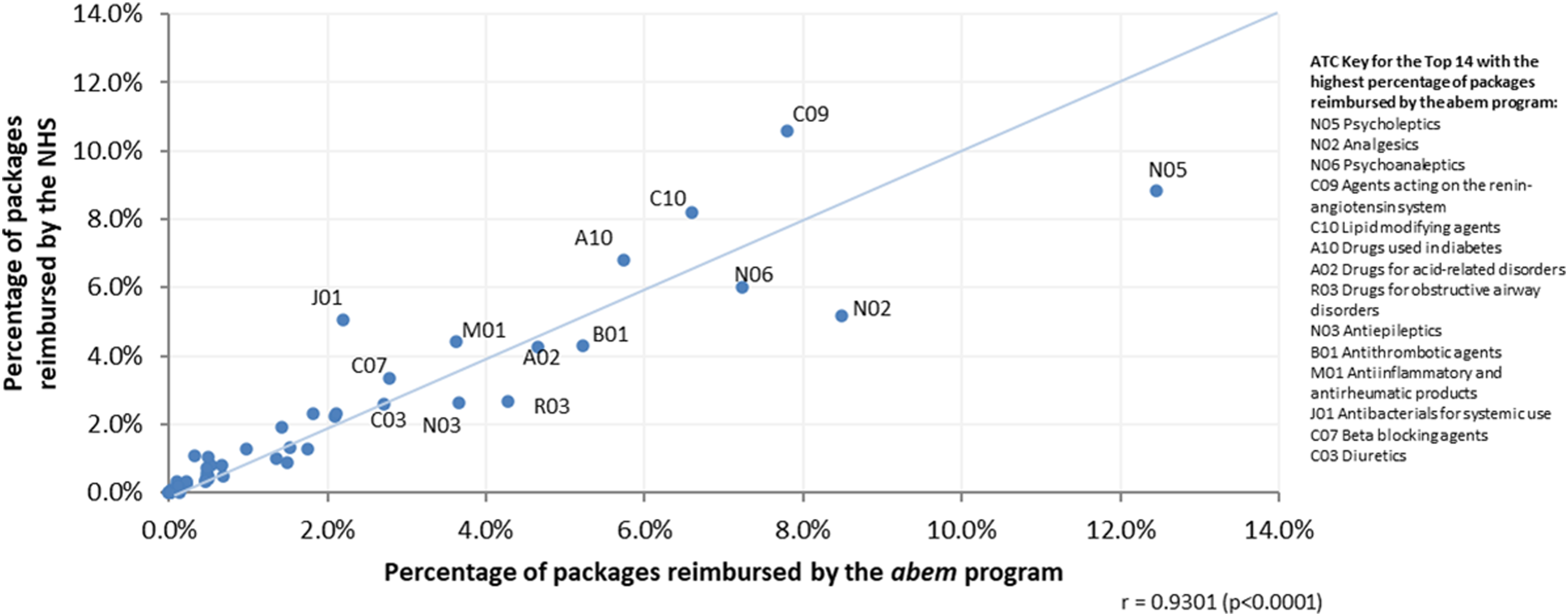
A more detailed analysis of the top therapeutic groups in an ATC level revealed the following. The most commonly consumed medicine for the nervous system were psycholeptics (ATC N05). This represented 35.5% of the medicines consumed for this purpose - the most common of these being Alprazolam with 11.1% (1717 packages) of the active substances in N05. Agents acting on the renin-angiotensin system (ATC C09) accounted for 32.7% of the medicines for the cardiovascular system, with the association of losartan + hydrochlorothiazide the most common with 8.4% (815 packages). Among the medicines for the alimentary tract and metabolism, the most common were those used in diabetes (A10), which represented 45.5% of medicines consumed for this purpose, the most common of these being metformin with 25.0% (1782 packages).
Impact on poverty and catastrophic health expenditures
Poverty rate, poverty intensity index, and poverty severity index in the population covered, without and with the abem program from 2016 to 2018.
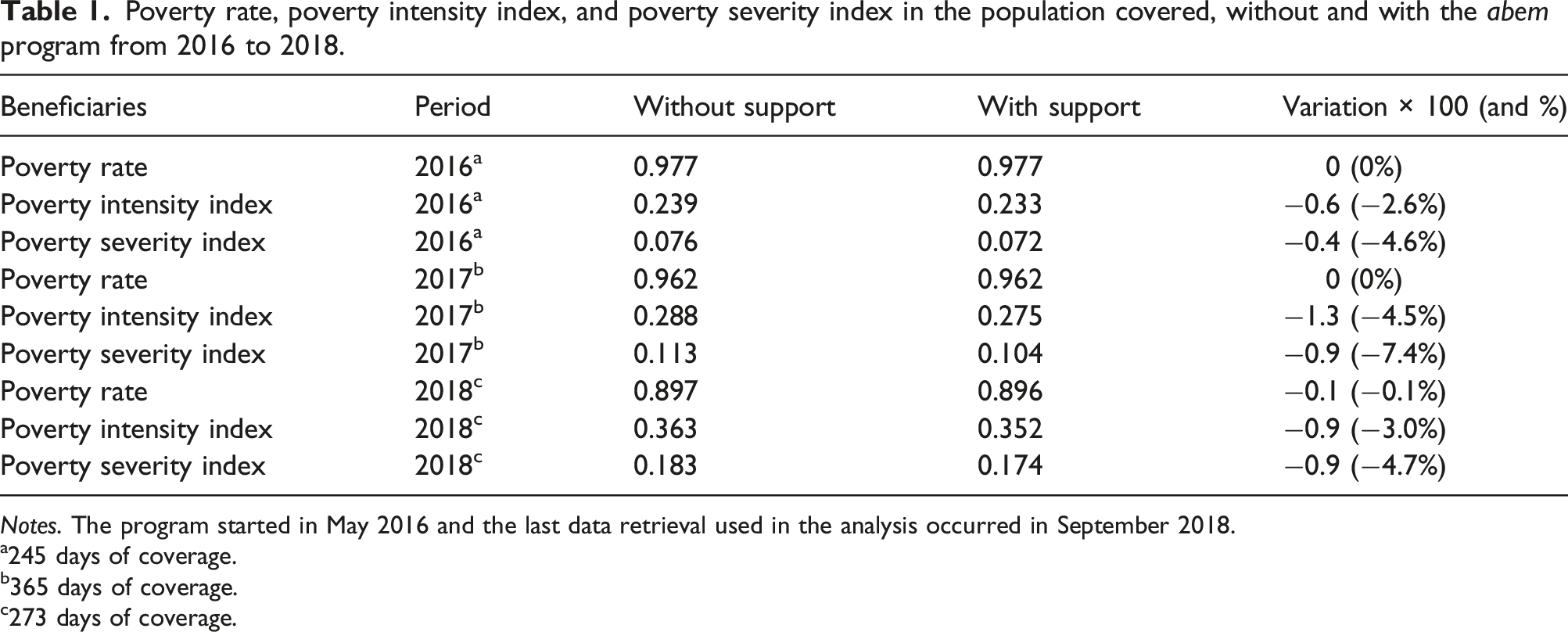
Notes. The program started in May 2016 and the last data retrieval used in the analysis occurred in September 2018.
a245 days of coverage.
b365 days of coverage.
c273 days of coverage.
Looking at the final column in Table 1, almost all beneficiaries have income so low that the transfers received were not enough for their income to climb above the poverty line. That is to say, the percentage change in the poverty rate for each of the 3 years was essentially unchanged. However, the transfers did narrow the distance between their income and the poverty line as reflected in the decrease in the poverty intensity and severity indices. In 2016, after the first 8 months of the program’s implementation, there was a decrease of about 2.6% in the intensity of poverty and 4.6% in its severity. After the second year, the decrease was even more notable, 4.5% in the intensity and 7.4% in the severity of poverty. Finally, in 2018, the reduction of poverty intensity and severity were of 3.0% and 4.7%, respectively. This can be translated into an overall 3.4% decrease in the intensity of poverty and 5.6% in the severity of poverty over the survey period.
Therefore, this medicines funding initiative has increased beneficiaries’ purchasing power and reduced the distance to the poverty line, thereby reducing poverty’s intensity and severity.
Incidence of catastrophic health expenditure (CHE) from 2016 to 2018.
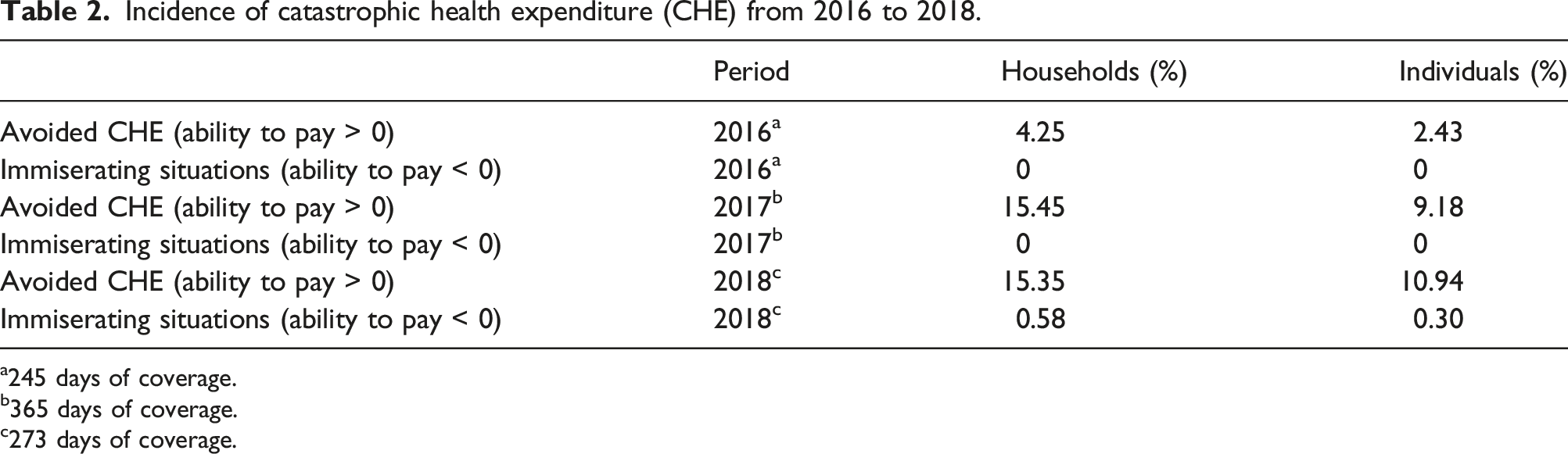
a245 days of coverage.
b365 days of coverage.
c273 days of coverage.
Discussion
In its first 29 months, the abem program grew significantly, eventually involving 95 referral entities and 528 community pharmacies spread across the country. By the end of the evaluation period, the program supported 6305 beneficiaries and helped to provide 127,510 medicine packages valued at €1.5 million, of which 26.9% came from the program’s co-funding.
The rising number of beneficiaries, especially among the elderly, and growing financial aid levels suggest the program has improved beneficiaries’ access to prescribed medicines. Our analysis reveals that this was indeed the case. The abem program had a positive impact on beneficiaries who used the card, with average proportional reductions of 3.4% in poverty intensity and 5.6% in poverty severity. This is of the same order of magnitude as the effects on the general Portuguese population of large policy changes, such as the changes that have occurred since 2010 in the minimum guaranteed income program or family allowances. 23 In addition, the abem program implicitly provided insurance even for those beneficiaries that did not use the card.
The abem program has also had a significant impact on catastrophic health expenditures. Our study revealed that the program avoided, on average per year, 7.5% of the consumers from experiencing catastrophic health expenditures, and in 2018, there were even cases where misery-inducing expenditures were prevented. Although the threshold for consideration of the OOP payments in health as catastrophic can vary between 10% and 40% of the household disposable income,24,25 this study considered a 10% threshold because only expenditures on medicines were considered and not total health expenditure. High OOP payments have made catastrophic health expenditures a sizeable issue in Portugal. Expenditure on medicines accounts for about 80% of the OOP household health expenditures for the poorest 20% of the Portuguese population.26,27 Recent evidence has shown that the percentage of families incurring catastrophic health expenditures due to medicine expenditures alone is high in Portugal, and that the greatest expense associated with catastrophic health expenditures is undoubtedly medicines. 28
As well as the effect on beneficiaries, the program has also had positive effects for households. Overall, then, the abem program has had a sizeable positive impact on vulnerable populations by mitigating the consequences of OOP payments for medication. This support constitutes a reinforcement of solidarity and social inclusion policies in Portugal.
Part of the reason for the program’s success has likely been the involvement of local institutions and their close proximity to beneficiaries. This has meant the abem program has been able to target those individuals in greatest need of the transfers, thereby maximizing the positive effects of the program and reducing errors in payments.
Limitations
There are two main limitations to our study. First, data constraints meant impacts have been estimated based on maximum thresholds of the households’ incomes. We suspect this has understated the positive effects of the program. If actual income data were available, we believe greater impacts on poverty and catastrophic expenditures reduction would have been obtained. That is because we were obliged to use the maximum income, corresponding to the program’s eligibility criteria, which likely masked the full positive effects of abem.
Second, the study has only been able to estimate the impact the program has had on direct payments for prescription medicines. It is possible that program users have other health expenditures, about which no information is available.
Conclusions
The abem program has improved the financial and health situation of disadvantaged people in Portugal. But more should be done. Due to financial constraints around 10% of Portugal’s population do not buy prescribed medicines. 12 As such, public policies should be seeking to improve access to medicines and reduce health care inequities. The expansion of the abem program to a wider population and/or to support expenditures other than for medicines are important measures to help vulnerable populations.
Regarding future research, it is of the utmost importance to improve our knowledge of the abem program’s effects, such as its socioeconomic dimensions (for example, the effects on rural vs urban poverty). Researchers could also further explore the impacts of abem on the access to and use of medications.
Footnotes
Acknowledgements
The authors gracefully acknowledge the assistance of community pharmacies and reference entities involved in the abem program, both for their general input and for making the relevant databases available.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Private Institution of Social Solidarity Dignitude funded this research. The study sponsor had no role in the design and conduct of the study, data collection, analysis, and interpretation of data, preparation, review, or approval of the manuscript, nor in the decision to submit the manuscript for publication.
Ethical approval
Ethical approval was not required for this research article.