
Abstract
Objective
In the context of increasing demand for ambulance services, emergency mental health cases are among the most difficult for ambulance clinicians to attend, partly because the cases often involve referring patients to other services. We describe the characteristics of mental health emergencies in the East Midlands region of the United Kingdom. We explore the association between 999 (i.e. emergency) call records, the clinical impressions of ambulance clinicians attending emergencies and the outcomes of ambulance attendance. We consider the implications of our results for optimizing patient care and ambulance service delivery.
Methods
We conducted a retrospective observational study of records of all patients experiencing mental health emergencies attended by ambulances between 1 January 2018 and 31 July 2020. The records comprised details of 103,801 ‘999’ calls (Dispatch), the preliminary diagnoses by ambulance clinicians on-scene (Primary Clinical Impression) and the outcomes of ambulance attendance for patients (Outcome).
Results
A multinomial regression analysis found that model fit with Outcome data was improved with the addition of Dispatch and Primary Clinical Impression categories compared to the fit for the model containing only the intercept and Outcome categories (Chi-square = 18,357.56, df = 180, p < 0.01). Dispatch was a poor predictor of Primary Clinical impression. The most common predictors of Outcome care pathways other than ‘Treated and transported’ were records of respiratory conditions at Dispatch and anxiety reported by clinicians on-scene.
Conclusions
Drawing on the expertise of mental health specialists may help ‘999’ dispatchers distinguish between physical and mental health emergencies and refer patients to appropriate services earlier in the response cycle. Further investigation is needed to determine if training Dispatch operatives for early triage and referral can be appropriately managed without compromising patient safety.
Introduction
Demand for ambulance services has been increasing year-on-year.1–4 In the United Kingdom (UK), 5 United States 6 and Australia 2 people presenting with mental health problems are important contributors to rising demand. Such patients involve severe presentations, including anxiety, depression, psychosis, acute behavioural disturbance, intentional drug overdose and attempted suicide. 7 Mental health emergencies are among the most time consuming and difficult cases for ambulance clinicians to attend, partly because they often involve referral to other services, which requires longer on-scene times.8,9 This is part of a general trend in which the role of ambulance services is changing from conveying most patients to hospital to include assessing and referring patients to alternative health care services – for example, general practitioners or mental health nurses, particularly for non-urgent cases or exacerbations of chronic conditions.10,4
In the UK, non-urgent cases account for an estimated 40% of all 999 (that is, emergency) calls attended by ambulances, 11 while only 8% of 999 calls are for patients with life-threatening illnesses or injuries. 10 In the context of financial constraints and rising demands on ambulance services, there is a need to consider alternative pathways to hospital conveyance when responding to patients with non-urgent conditions, including some mental health disorders.11,12 Prior research has explored the characteristics of medical emergencies attended by ambulances1–3 and opportunities for alternative care pathways for common physical conditions, such as falls. 13 But few studies examine the epidemiology of mental health emergencies14,15 or consider how well care pathways are tailored to patient needs.
In a recent publication, we investigated the characteristics of mental health emergencies in the UK geographical area of East Midlands occurring during the first national UK ‘lockdown’ associated with the COVID-19 pandemic in 2020. 7 That research involved engaging with call-and-dispatch phone operatives, ambulance and other clinicians and research specialists within the National Health Service. We observed that there was often considerable disagreement about patients’ conditions between Dispatch codes (how phone operatives record emergencies at the point of ‘999’ calls) and Primary Clinical Impressions (ambulance clinicians’ preliminary diagnoses of patient conditions on-scene). However, no research elucidates the specific nature of this disparity. Furthermore, whereas research has investigated the pathways between Dispatch records, Primary Clinical Impressions and Outcome (the end result for patient care resulting from ambulance attendance) in the UK and elsewhere, that research considered physical conditions.16–19
The present study describes the epidemiology of mental health emergencies attended by the East Midlands Ambulance National Health Trust (EMAS). We analyse 102,079 records of mental health emergencies attended by ambulances in the East Midlands. We describe the characteristics of mental health emergencies including Dispatch records, Primary Impression records and Outcome records. We then explore the association between the three measures, including how well Dispatch records reflected Outcomes for patients, and the characteristics of Dispatch and Primary Clinical Impressions together that explained each Outcome for patient care. Finally, we consider the implications of associations between Dispatch, Primary Clinical Impression and Outcome for improving service delivery.
Methods
Study setting and design
The East Midlands, located in the Central Eastern part of England, spans an area of 15,627 km2. The region’s estimated population is 4.8 million, including the urban areas of Derby, Leicester, Lincoln, Northampton and Nottingham. The region is the third most rural region in England. In 2016, 18.5% of people in the East Midlands lived in the most deprived quintile.20,21
We employed a cross-sectional design using retrospective observational routine data from EMAS. The study included all patients of any age who had been attended by ambulance for mental health-related emergencies between 1 January 2018 and 31 July 2020. The time period was selected based on the availability of records using a consistent recording process. In 2018, a new recording process was introduced, so records prior to 2018 were not comparable with records collated from 2018 onwards. The dataset analysed included two independent variables (Dispatch codes and Primary Clinical Impression codes), and more than 100,000 cases with a minimum of 13 and maximum of 39,465 cases per category of each independent variable. The sample size and number of cases per independent variable (see Table 3) met the requirements for statistical power for multinomial regression where, typically, a minimum of 10 cases per independent variable is considered sufficient. 22
Study variables and measures
Research measures.
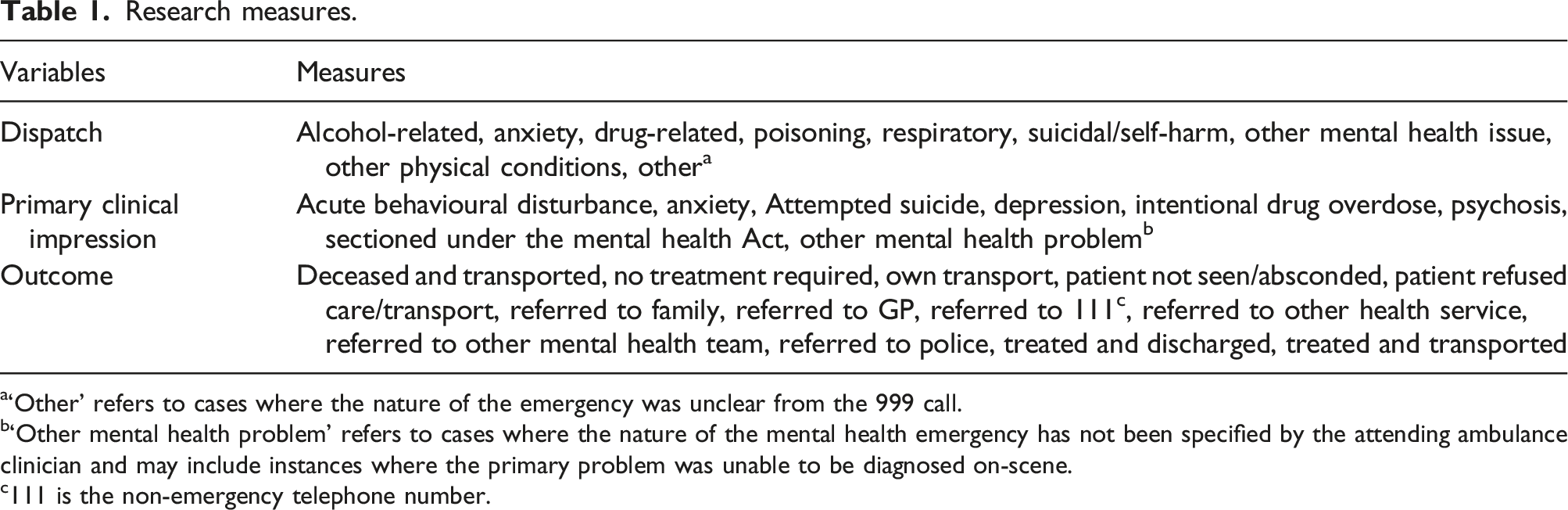
a‘Other’ refers to cases where the nature of the emergency was unclear from the 999 call.
b‘Other mental health problem’ refers to cases where the nature of the mental health emergency has not been specified by the attending ambulance clinician and may include instances where the primary problem was unable to be diagnosed on-scene.
c111 is the non-emergency telephone number.
EMAS uses the Advanced Medical Priority Dispatch System, outlined in detail by Heward et al. 23 Attending clinicians record a ‘Primary Clinical Impression’ of patient symptoms, which is informed by the professional judgement of the clinician as well as the mental health history reported by the patient or other individuals known to the patient and are present at the time of ambulance attendance, such as family members. Ambulance clinicians may also access additional medical support through a Clinical Care Support Desk.
The ‘Outcome’ is what ultimately happened to the patient. The decision of the clinician attending a mental health emergency on whether to convey the patient via ambulance to hospital or to refer the patient elsewhere is usually determined following clinical evaluation and discussion with the patient. These outcomes include ‘Treated and transported’ and ‘Referred to General Practitioner (GP)’. When a patient lacks capacity because of an acute or pre-existing condition, the clinician makes the decision based on the ‘best interests’ of the patient, which sometimes involves involuntary detention using legal procedures, such as the Mental Health Act 2007. In some cases, the Outcome recorded by the ambulance clinician is determined by the patient, such as instances where the patient refuses treatment or absconds from the scene of ambulance attendance.
The categories reported in Table 1 were coded in consultation with the Head of Clinical Audit and Research for EMAS and with reference to Dispatch codes and details recorded by Emergency Medical Dispatcher phone operatives, which are guided by the Field v13 Responder Guide: Medical Priority Dispatch System approved by the International Academy of Emergency Medical Dispatch. 24 This protocol has been developed over 40 years of filed usage and is considered best practice. 25 Dispatch codes are determined by the description given by the ‘999’ caller about the condition of the patient. Primary Clinical Impression codes are determined by the paramedic attending the emergency based on a preliminary diagnosis of patient condition, and thus tend to be more specific than Dispatch Codes.
Our coding closely mirrors the categories used by EMAS Emergency Medical Dispatchers, but with several exceptions. For Dispatch codes, ‘Other physical condition’ includes multiple conditions that occur infrequently in the dataset, such as cardiovascular and diabetic events. For Outcome codes, ‘Referred to other health service’ includes referral to numerous services such as private clinics and surgeries. Similarly, ‘Referred to other mental health team’ includes referral to multiple services such as mental health nurses, private mental health clinics and crisis teams. Outcome coding also aggregates equivalent services that operate regionally or locally – for example, independent mental health crisis teams with equivalent roles in the community operate in major cities.
Data analysis
The data obtained from EMAS comprised 103,801 individual patient records of mental health emergencies related to 999 calls. Any records missing Dispatch, Primary Clinical Impression or Outcome records were removed. This reduced the dataset to 102,079 records.
After undertaking descriptive analysis of each study variable, we computed a multinomial regression model to explore the association between Dispatch and Primary Clinical Impression records, and the Outcome of ambulance attendance. The null hypothesis of the regression model tested was that there was no difference between the model fit to Outcome data without predictor variables (Dispatch and Primary Clinical Impression records) compared to the model fit to Outcome data with predictor variables. A likelihood ratio test was conducted to evaluate the overall goodness of fit of the two models. All descriptive and analytical statistical analysis was undertaken using the statistical software IBM SPSS Statistics 27.
Results
Descriptive results
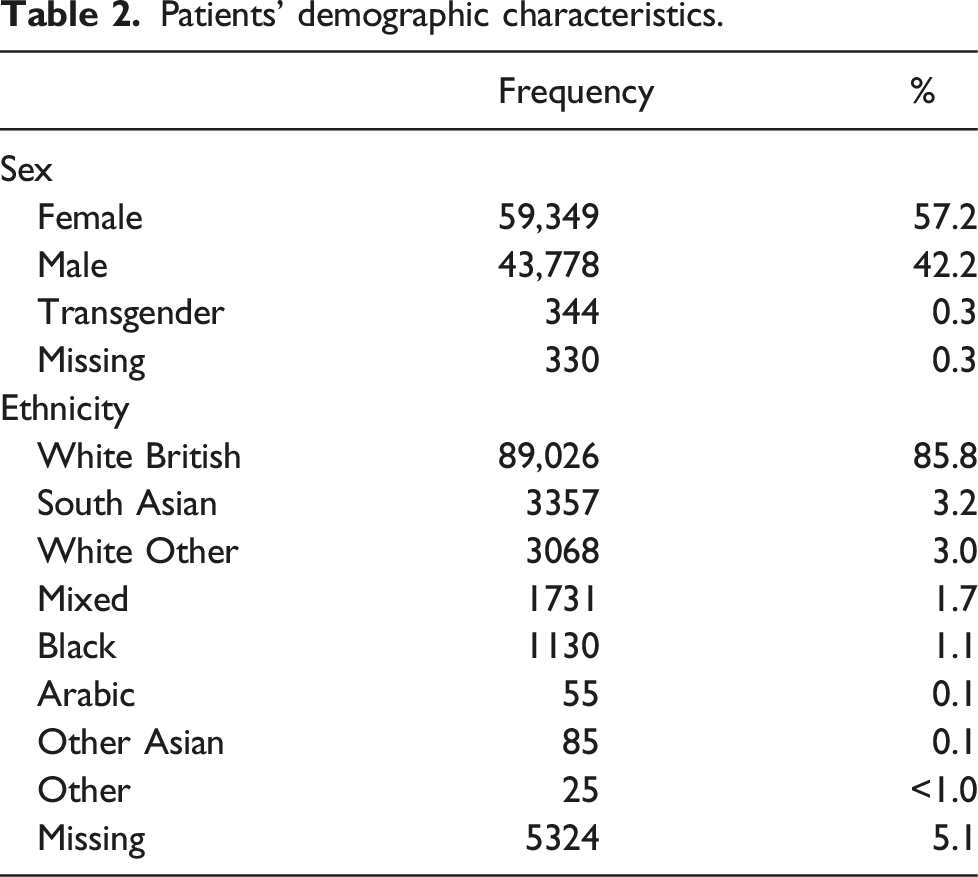
Patients’ demographic characteristics.
Number (N) and percentage (%) of mental health emergencies by dispatch, primary impression and outcome categories.
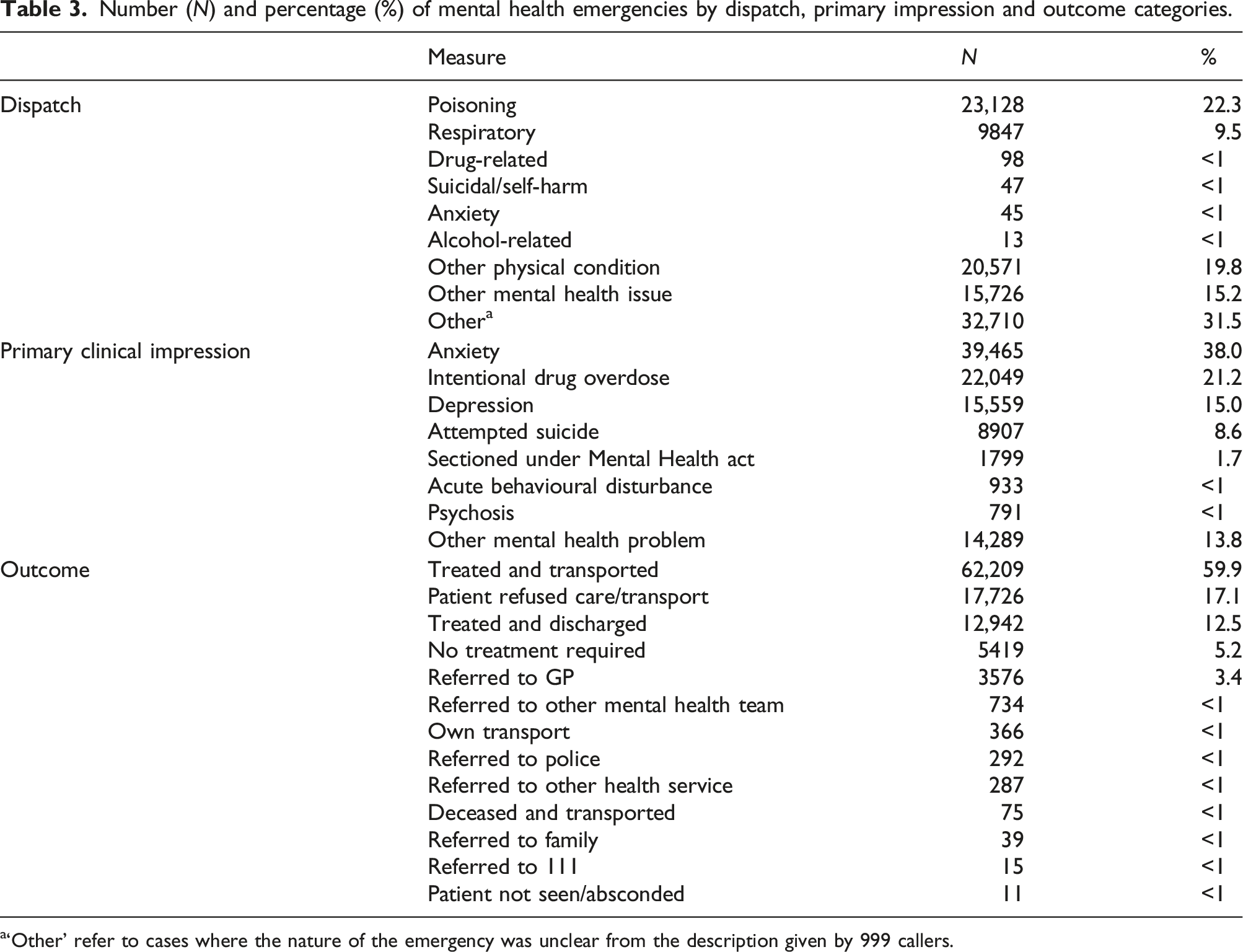
a‘Other’ refer to cases where the nature of the emergency was unclear from the description given by 999 callers.
There was a higher level of specificity in Primary Clinical Impression, indicating the greater insight that can be gleaned by clinicians on-scene. The single most common categories were ‘Anxiety’ (38.0%), ‘Intentional drug overdose’ (21.2%), ‘Depression’ (15.0%) and ‘Attempted suicide’ (8.6%). The aggregate ‘Other mental health problem’ (13.8%) category accounted for only a little over tenth of all cases. Strikingly, whereas Dispatch complaints related to ‘Anxiety’ account for less than 1% of cases, 38% of patients were given a preliminary diagnosis of ‘Anxiety’ by clinicians on-scene.
Turning to Outcomes, in most cases the ambulance transported the patient from the scene. The single most common Outcome was ‘Treated and transported’ (59.9%), accounting for well over half of all cases. The other main Outcomes were ‘Patient refused care/transport’ (17.1%), ‘Treated and discharged’ (12.5%), ‘No treatment required’ (5.2%) and ‘Referred to GP’ (3.4%).
Determinants of Outcome for patients experiencing mental health emergencies
Likelihood-ratio tests.

The results of Likelihood-ratio testing, reported in Table 4, indicate that there was a statistically significant relationship between the independent variable ‘Primary Clinical Impression’ and the dependent variable ‘Outcome’ (p < 0.01). The Chi-square and P-value for ‘Dispatch’ in the Likelihood-ratio table also indicate that the independent variable ‘Dispatch’ was redundant in the final model.
Multinominal logistic regression model predicting mental health emergency outcome from dispatch and primary clinical impression. The reference category for Outcome is ‘Treated and transported’.
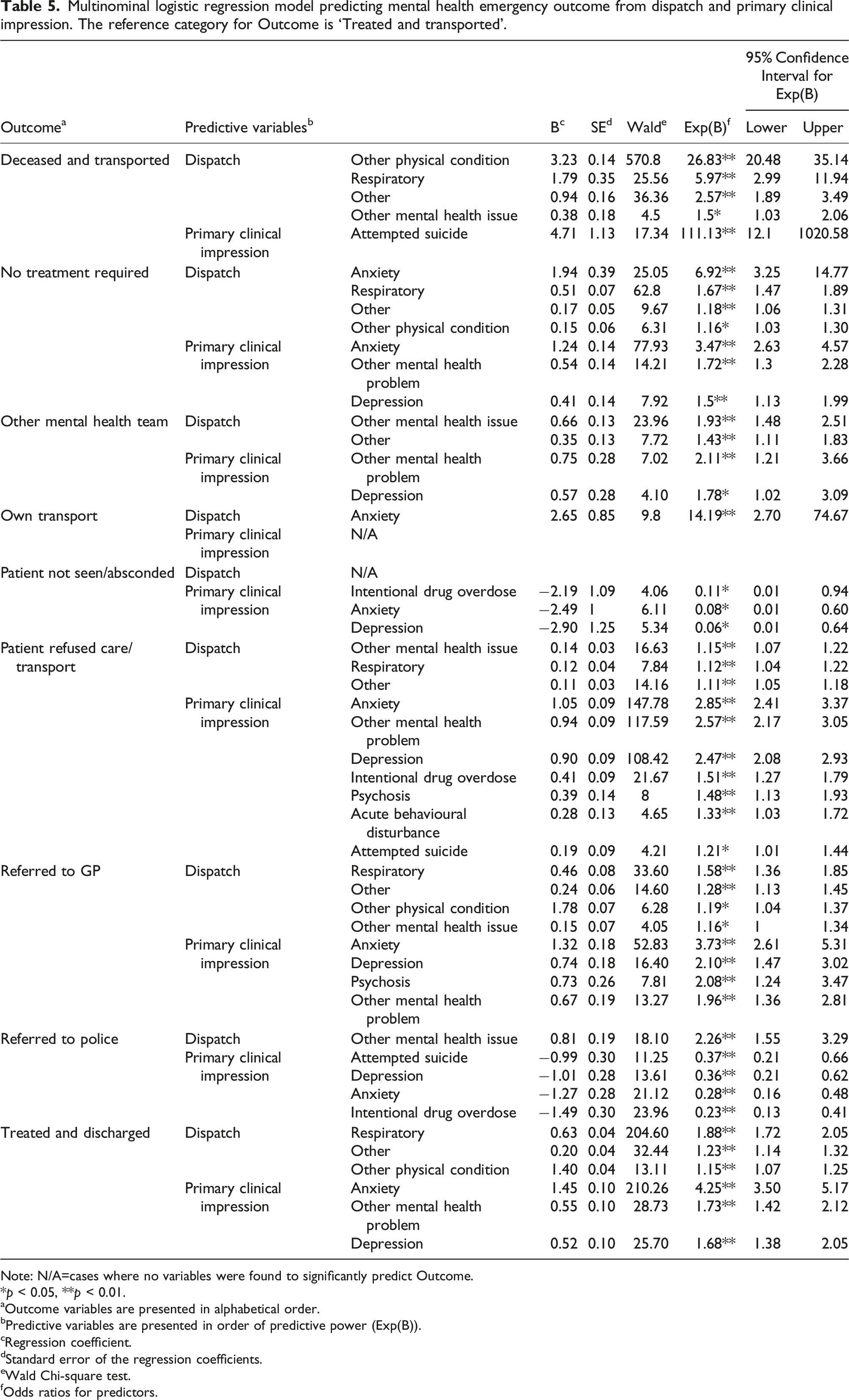
Note: N/A=cases where no variables were found to significantly predict Outcome.
*p < 0.05, **p < 0.01.
aOutcome variables are presented in alphabetical order.
bPredictive variables are presented in order of predictive power (Exp(B)).
cRegression coefficient.
dStandard error of the regression coefficients.
eWald Chi-square test.
fOdds ratios for predictors.
Compared to the reference condition ‘Treated and transported’, nine Outcomes were predicted by Dispatch and Primary Clinical Impression categories, although few Dispatch records predicted Outcome compared to Primary Clinical Impressions. The Outcome ‘Deceased and transported’ was strongly predicted by ‘Other physical condition’ recorded at Dispatch (Exp(B):26.83), and ‘Attempted suicide’ reported by attending clinicians (Exp(B):111.13), reflected in Primary Clinical Impression records. The Outcome ‘No treatment required’ was most strongly predicted by ‘Anxiety’ at Dispatch (Exp(B):6.92) and ‘Anxiety’ reported by attending clinicians (Exp(B):3.47). Referral to ‘Other mental health team’ was predicted most strongly by the record ‘Other mental health issue’ at Dispatch (Exp(B):1.93) and ‘Other mental health problem’ (Exp(B):2.11) by clinicians on-scene. The Outcome ‘Patient refused care/transport’ was most strongly predicted by ‘Other mental health issue’ at Dispatch (Exp(B):1.15) and ‘Anxiety’ by attending clinicians (Exp(B):2.85). The Outcome ‘Treated and discharged’ was predicted most strongly by records of ‘Respiratory’ condition at Dispatch (Exp(B):1.88) and ‘Anxiety’ (Exp(B):4.25) reported by attending clinicians, reflected in Primary Clinical Impression records. For Outcomes ‘Deceased and transported’, ‘No treatment required’ and ‘Patient refused care/transport’, the second strongest predictor at Dispatch was records of ‘Respiratory’ conditions. The Outcome ‘Referred to GP’ was most strongly predicted by ‘Respiratory’ complaints at Dispatch (Exp(B):1.58) and ‘Anxiety’ (Exp(B):3.73) and ‘Depression’ (Exp(B):2.10) by clinicians on-scene, reflected in Primary Clinical Impression records. Regression coefficients (B) indicate that the Outcomes ‘Referred to police’ and ‘Patient not seen/absconded’ were negatively associated with ‘Anxiety’, ‘Depression’ and ‘Intentional drug overdose’ reported by clinicians on-scene, reflected in Primary Clinical Impressions. Overall, odds ratios (Exp(B) indicate that the most common predictors of Outcome care pathways other than ‘Treated and transported’ were records of ‘Respiratory’ conditions at Dispatch and ‘Anxiety’ reported by clinicians on-scene.
Discussion
Patients experiencing mental health emergencies were often recorded at Dispatch with physical ailments. Table 5 demonstrates that mental health emergencies, such as ‘Anxiety’, are often erroneously identified as physical health emergencies, such as ‘Respiratory’ problems, at the point of Dispatch. Indeed, the most common mental health problems attended by ambulance clinicians included ‘Anxiety’, ‘Intentional drug overdose’ and ‘Depression’. Unsurprisingly, then, Primary Clinical Impression is a better predictor of Outcome than is Dispatch.
These observations suggest opportunities for improving the delivery of emergency medical services and the engagement between primary care and mental health professionals. Dispatch triage includes the option to refer phone-calls to health professionals for consultation. But mental health specialists are not always available for consultation at the time of dispatch decision-making. For example, a clinical assessment team is available for consultation between 8am and 8pm, but clinicians prioritize patients based on the severity of the reported condition and may not always have the resources to respond to mental health emergencies. Thus, while dispatch call centre operatives record the condition of the patient based on the report given by the ‘999’ caller, the decision to deploy an ambulance is predominately based on computer algorithms. 26
Dispatch phone operatives in the UK are not medically trained. As such, dispatch operatives may benefit from more specific training by psychological and psychiatric practitioners in responding to mental health crises. All emergency calls logged by a phone operative in France are passed to a medically trained dispatcher. In 2001 ambulance services covering Paris received approximately 820 calls per day with only 6% resulting in the dispatch of a mobile intensive unit and 16% involving referral to primary care doctors. 26 By comparison, services covering Manchester over the same period, a region with an equivalent population to Paris, received 700 calls per day, all of which received standard paramedic responses – including sending an ambulance. Drawing on the expertise of mental health specialists may help 999 dispatchers to distinguish between physical and mental health emergencies and refer patients to appropriate services earlier in the response cycle.
Limitations
There are four main limitations to this study. First, associations found in this observational study may be subject to unmeasured or unknown confounders. Further studies are required to confirm and explore the associations we identified.
Second, some ambulance services in the UK use earlier versions of the Field Responder Guide to determine dispatch codes and categories, so findings reported here related to Dispatch categories may be difficult to generalize to regions where alternative methods of categorizing 999 calls are in use. Nonetheless, dispatch protocols (e.g. use of computer-based triage and phone operatives without mental health training or expertise) are similar across the UK – six out of the 10 English ambulance services use the same dispatch system. Therefore, the results and implications are generalizable to a wider area.
Third, Primary Clinical Impression categories reflect the patient’s history, including information about prior mental health conditions and clinical observations on-scene, increasing their accuracy compared with Dispatch categories. This probably increased Primary Clinical Impression’s predictive power in determining Outcomes.
Fourth, most patients were of White British ethnicity and identified as female or male. Far fewer were of ethnic minority background, and less than 1% identified as transgender. Thus, the results may not reflect a wider representation of mental health patients in the community.
Conclusions
The role of emergency medical services is changing to include community referral, particularly for non-urgent or chronic conditions, which may include mental health conditions. 11 An implication for optimizing service delivery is that improving dispatch triage by engaging psychological and psychiatric professionals to train phone operatives could help to identify patients in need of ongoing mental health care, and to direct those patients to appropriate primary care services earlier in the triage process. However, further investigation is needed to determine if early triage and referral can be appropriately managed without compromising patient safety.27,4
Footnotes
Acknowledgements
The authors wish to recognize the EDGE Consortium is an International research group consisting of: University of Lincoln, UK: Prof AN Siriwardena, Prof M Gussy, Dr H Moore, Prof F Tanser, Prof G Law; University of Loughborough: Mr Bartholomew Hill; McMaster University, Canada: Prof G Agarwal, R Cooper, M Pirrie, R Ferron, Dr I Bielska; Hamilton Paramedic Service, Hamilton, Canada: B McLeod; East Midlands Ambulance Service NHS Trust, UK: R Spaight.
The data that support the findings of this study are available from the East Midlands Ambulance Service but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This research, including consent to use patient data, was approved by the NHS Health Research Authority, IRAS ID: 264573.