
Abstract
Objectives
The prominence given to issues of patient safety in health care organizations varies, but little is known about how or why this variation occurs. We sought to compare and contrast how three English hospitals came to identify, prioritize and address patient safety issues, drawing on insights from the sociological and political science literature on the process of problem definition.
Methods
In-depth qualitative fieldwork, involving 99 interviews, 246 hours of ethnographic observation, and document collection, was carried out in three case-study hospitals as part of a wider mixed-methods study. Data analysis was based on the constant comparative method.
Results
How problems of patient safety came to be recognized, conceptualized, prioritized and matched to solutions varied across the three hospitals. In each organization, it took certain ‘triggers’ to problematize safety, with crises having a particularly important role. How problems were constructed – and whose definitions were prioritized in the process – was highly consequential for organizational response, influencing which solutions were seen as most appropriate, and allocation of responsibility for implementing them.
Conclusions
A process of problem definition is crucial to raising the profile of patient safety and to rendering problems amenable to intervention. How problems of patient safety are defined and constructed is highly consequential, influencing selection of solutions and their likely sustainability.
Introduction
Recent years have seen huge public interest, policy attention and organizational endeavours focused on the quality and safety of health care. The reasons for this are multiple, including a series of scandals and high-profile incidents, 1 a growing mass of evidence on the epidemiology of avoidable harm,2–4 and the emergence of the modern patient safety movement and associated organized advocacy. 5 Perhaps less remarked has been the variability in attention given to different topics in quality and safety. For example, while surgery has seen welcome improvements over time, the safety of those with mental illness has received rather less attention in research and policy. 6 Yet questions of how problems of quality and safety are defined and identified, what counts as a solution, and how those choices influence practice have received scant attention in the literature.
In this paper, we offer an analysis of how problems of patient safety come to be recognized, conceptualized, prioritized and matched to solutions in health care organizations. We use three qualitative case studies of English National Health Service (NHS) hospital trusts as our data sources. Our analysis draws on an important social science tradition that describes the genesis and trajectory of ‘social problems’.7–10 These accounts emphasize that social problems cannot be treated as self-evident facts: instead, problems are constructed or created by various collective social processes that themselves are dynamic and contingent.11–13 As a result, issues may be defined as problems at some times but not others, and their prominence may amplify or diminish over time, for example at the level of health policy formation,14–16 or in the work of social movements to orchestrate action around quality and safety.17,18
Recent research has begun to examine different problematizations in health care, showing, for example, how dominant constructions, articulated through standards and measures, may be misaligned with ‘local’ understandings of what needs to be improved and how.19,20 However, examination of the processes by which dominant groups, such as senior managers in health care organizations, construct and advance particular problematizations of patient safety issues has been limited. As Cornelissen and Werner note, such top-down constructions of problems can be taken for granted, 21 yet they too rely on active work ‘to mobilize potential adherents and constituents, to garner bystander support, and to demobilize antagonists’. 22
Here, we seek to apply the insights of the problem-definition literature to understand how those in senior managerial positions in health care organizations (sometimes known as the ‘blunt end’, as opposed to the ‘sharp end’ of care, where patient-facing clinical activities take place 23 ) come to identify and characterize patient safety problems and organize responses. Across the three case studies that form our data, our focus is on the social processes of problematization – how issues come to be identified and understood as problems that required action – and the consequences of that problematization for their resonance with staff and for allocation of responsibility.
Methods
In-depth qualitative fieldwork, involving interviews, ethnographic observation and document collection, was carried out in three purposively chosen hospital trusts, as part of a wider mixed-methods study.24–26 At the time of study, each site was undertaking concerted, hospital-wide efforts to improve quality and safety, which formed a key focus of our data collection. All three were teaching hospitals with close relationships with nearby medical schools; two (‘Appleby’ and ‘Berryton’) were acute trusts providing a wide range of secondary care services to large local catchments; the third (‘Cherryville’) was a tertiary centre providing specialist services.
The balance of qualitative data-collection techniques varied by site, but in all three sought to cover both the ‘blunt end’ (senior clinicians and managers responsible for devising and implementing initiatives) and ‘sharp end’ (clinicians responsible for delivering care, and the subject of efforts to improve culture, processes and behaviour). Having obtained ethical and research governance clearances, we undertook fieldwork that included: (i) qualitative interviews with blunt- and sharp-end participants on safety in general and the particular approach adopted in their hospital; (ii) ethnographic observation of day-to-day care processes in a selection of units in Appleby (acute wards and maternity services) and Berryton (acute wards). We conducted 64 interviews and 56 hours’ observation in Appleby, 11 interviews and 190 hours’ observation in Berryton, and 24 interviews in Cherryville (where observations were not possible). As we undertook the main analysis of our data, the implications of constructions of quality and safety at the blunt end became an increasingly interesting focus of inquiry, and we therefore undertook further analysis to deepen our understanding of how it was received and acted upon at the sharp end.
In undertaking this additional analysis, we deployed an approach based on the constant-comparative method, 27 assisted by NVivo software. Our ‘sensitizing concepts’ came from the social scientific literature on problem definition. Initially, we coded data excerpts that related broadly to these themes, before developing a coding framework that distinguished different parts of the process of defining problems and identifying appropriate solutions and facilitated cross-case comparison.
Results
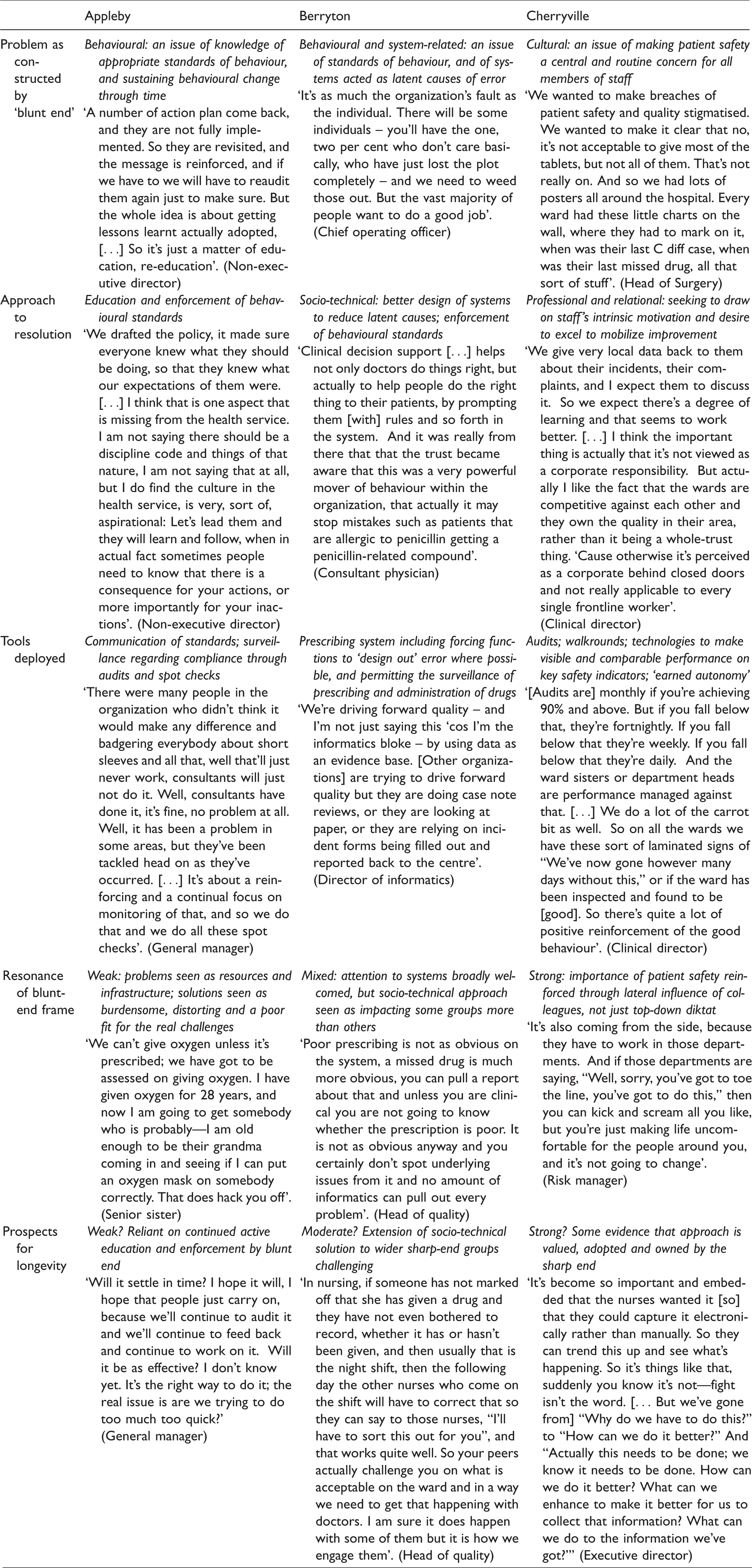
We found that patient safety was acknowledged as a priority both by senior leaders of the hospitals and by clinicians delivering care, but that it was in competition with other organizational priorities for the inherently limited space on the organizational agenda. 28 We examine in turn how each organization sought to reassert the primacy of safety concerns (see also Table 1). We found in particular that in each organization it took certain ‘triggers’ to problematize safety – bring it into being as a social problem – such that it was positioned at the forefront of organizational concerns and seen as something amenable to action. The form taken by these triggers, however, differed across cases. How problems were constructed – and whose definitions were prioritized in the process – then had important consequences for the organization’s response.
The construction of problems, resolutions and responsibilities in the three sites.
Appleby: the problem of serious incidents and the behavioural solution
At Appleby hospital, a series of serious incidents involving patient harm were assembled into a crisis that triggered the organizational re-centring of patient safety as a problem amenable to organizational intervention. This problematization brought dormant concerns about patient safety to life, raised its profile and created a window of opportunity
7
in which to convert safety risks into actionable problems. We just had a little clutch [of incidents] in particular that came together in which – there was almost like an emotional response within the organization, of people saying, ‘Crikey this just isn’t good enough’. (Executive director, Appleby) You are responsible for this, and you need to do a, b, c, and d, and we will come back and ask and check, and if you are found to be lacking, then you are responsible. […] It starts with the policy, and then it starts with having people responsible, people understanding what the expectations are of them. (Non-executive Director, Appleby) I’m very clear that unless you get personal accountability down to an individual level, then I can make all the things around policy change that perhaps have got to improve – [but] unless I’m actually monitoring what individuals are doing, and as we’ve been very clear that this is the standard of practice that we expect, that you just won’t get sustainable, manageable change. (Senior Nurse, Appleby) What we’re trying to do is get a message out there which says you’re a part of this organization [which] is taking the patient experience and the quality of patient care very seriously indeed. Success will come from changing that culture so that it becomes important to everybody, rather than endlessly finding more and more things to audit. (Non-executive director, Appleby) When you visit the ward and you see that there is only one or two members of very stressed looking staff looking after a high case workload, then although I know it’s a good hospital generally, it does generate some concern. (Consultant Physician, Appleby) To come and assess somebody and have to go through a three-page assessment on how to give oxygen? I think that is a waste of time and paper. Especially for somebody who has trained as a nurse. (Nurse, Appleby) I think [the focus on the deteriorating patient has] taken away a lot of common sense. […] You talk to management, the people who are bringing this in and going, ‘No, you have to do it then’. But I have to look after my patient first, they are not going to die of a lack of temperature, they are going to die of a lack of oxygen! But some of these people just seem so blinkered. (Nurse, Appleby)
Berryton: technical opportunities, socio-technical solutions
A different trigger lay behind the problematization process in our second case: Berryton. Here, a new system for electronic prescribing presented the hospital’s blunt-end executives with opportunities to make care safer in two ways: by including ‘forcing functions’ that would prospectively identify contraindications, possible dosing errors and patient allergies; and by developing capacities in the system to identify both individual medication errors and broader patterns relating to drug prescribing and administration. [The system] was not built to produce those reports. It was built as a clinical system, so Informatics have had to do work on the back end of the system to pull this stuff out because it was not built in that way. (Head of quality, Berryton) If [a failing] is down to you not being bothered, we will take action. If it’s down to you not having the education, we will take action. If it’s down to the system not working properly, we will take action. It’s as much the organization’s fault as the individual. (Executive Director, Berryton)
The rather different process of problematization, mode of response and implications for the responsibilities of sharp-end staff appeared to result in greater engagement than in Appleby, at least among some groups. More positive attitudes were founded in a sense that the IT systems mitigated some of the challenges of securing safety solely through individuals’ own efforts. [A nurse] spoke to me about [the IT system]; she feels that it’s good. It ensures safety. She said, ‘It’ll make sure you give [drugs.] It’ll stop you forgetting to give things’. And she liked it. (Fieldnotes, Berryton) They’re scared, [that’s] why the nurses quite often write an essay […] They write that ‘covering your arse’-type thing’. (Senior Nurse, Berryton) We started with the nurses, and that’s largely because nurses administer, don’t they, on the whole. I think it’s becoming clear that the doctors have up to now been not been quite so easy to provide the evidence to say, ‘You didn’t do this’. (Senior Nurse, Berryton)
Cherryville: creation of shared mission
The triggers of the problematization of patient safety in Cherryville shared something in common with both Appleby and Berryton. Here, as in Appleby, a series of serious incidents and ‘near misses’ had punctured widely held assumptions that quality and safety were under control, offering a crisis as basis for action. The action itself was led by a newly-appointed chief executive. And, as in Berryton, a new IT system – in this case, for incident reporting – provided the opportunity for continued renewal of knowledge of problems. How Cherryville utilized these windows of opportunity, however, diverged. Here, managers and senior clinicians worked together to use narratives to create shared emotional commitment and sense of mission, and seek input from all quarters on potential solutions. Serious incidents were thus used to both prompt acknowledgement of the existence of a problem and facilitate engagement across the staff in developing an appropriate set of solutions. We launched with an event [where] I talked about a patient who had died of a line-associated septicaemia. ‘Whilst that was happening’, [I said,] ‘we could not say we were a centre of excellence’. So we used that patient’s story. [That] was actually really quite powerful because nobody then could [ask,] ‘Why are you doing this?’ (Executive Director, Cherryville) The idea is that each team leader has some jobs that they have to ensure that they do, pretty much continuously. And for almost all the team leaders there are one or two jobs that are specifically around patient safety. (Consultant Surgeon, Cherryville) The reports now get put on the board about trips and falls every month. And obviously the ward really look to be better than the other wards. Do you know what I mean? So a bit of competition. (Patient liaison lead, Cherryville) Visiting the area and discussing. Certainly, with my experience working on the ward, the people that work on the ward don't always understand the gravity of things that are happening. They don't understand where that goes, they fill in the incident form and nothing happens. That's what they see. And unless that's brought back to them, by way of visitation or feedback or whatever, they will stop reporting. (Risk manager, Cherryville) As a clinician and a manager, I can help them pick what those issues are. The support, constant support, but also the pressure, that slight pressure. And I wish I didn’t say it and I wish I didn’t need it, but pressure to keep going. (Clinical nurse specialist, Cherryville) The trust has been quite good at communicating and having regular briefings about opportunities to even talk to the chief exec, and regular briefings with the execs. So, there’s been quite an open forum of communication. […] There seems to be more openness and two-way discussions, not just told what to do. (Matron, Cherryville)
Discussion and conclusion
This study suggests that a process of problem definition within organizations may be important in raising the profile of patient safety and to rendering problems amenable to intervention – ‘out of the realm of accident and into the realm of human control’. 12 Noticing a problem is important, but attention is also needed to how problems of patient safety are defined and constructed, because this process influences the selection of strategies for resolving them and the viability of those strategies. Dramatic triggers or crises 28 may reprioritize safety, but opportunities for improvement may be squandered if they quickly fade in organizational memory, or if problems are constructed in ways that do not achieve the right balance between personal accountability, systems improvement, and use of data and feedback. 30
To avoid the cycles of problems that emerge into furore and then fade into obscurity, described so well in accounts of the ‘issue-attention cycle’, 8 purposeful and reflective work is required not just in recognizing problems of patient safety but also in constructing those problem and their consequences for the solutions and responsibility for realizing them. The precise nature of the crisis is relevant here, but it is not determinative: there are opportunities for intervention by organizational actors to construct the problem in narrower or broader terms. For example, it may be important to avoid framing safety problems as mostly tractable to changes in individual behaviour (as in Appleby), and to manage the prioritization of aspects of care that are easily measured and that risk ‘colonizing’ 31 work time by incentivizing the creation of evidentiary artefacts to head off the blame (as in Berryton).
In this way, our analysis builds on the classic problem definition literature and indicates how its lessons might be applied in understanding the trajectory of problems in health care organizations. Early approaches to understanding social problems8,32 presented universal, linear models of the process, whereby issues emerge as problems and then fade away. But the natural history may not be so predictable or consistent: potential problems vie with one another for attention, 28 and are contested by groups with divergent interests. Important in this regard are the ‘causal stories’ that are inscribed in problems, which ‘assign responsibility for the condition to someone else and so create a burden of reform. People blamed for a problem and saddled with the burden of reform will resist the new causal theory’. 12 As shown in Table 1, there were commonalities and overlaps in the specific mechanisms used by the three sites. Where they differed, however, was in how they were used to allocate responsibility and ownership of resolution.
Our analysis shows that just as problem definition is a social process, so too is the construction of the underlying causes, the balance of responsibilities, and the most appropriate solution – and critically, these processes offer opportunities for intervention that will affect both the allocation of responsibility and the durability of the problematization. This implies that problem definition should be understood as only the initial step in improving quality and safety: the activity that follows, in terms of constructing solutions and distributing responsibility for implementing them, is also crucial. This implicates not just the ‘pragmatic skills […] of the manager in framing a message’, but also the role of ‘organizational members as active agents’ in the construction of problems and solutions, a feature often neglected in the existing literature. 21
Our study has important limitations. It is difficult to assess the representativeness of the hospitals studied, though we anticipate that our findings would be transferable. We do not have measures of patient safety across the organizations, and thus cannot determine the extent to which the different approaches impacted on performance. There is a danger that the case-study approach used may lend itself to stories that are too simple, creating the risk of painting the sites as black or white rather than deeply complex. Finally, while we used qualitative data collection techniques in all three sites, the balance between ethnographic observation and interview accounts varied; a different understanding of the construction of problems might have emerged had the balance been different, including a greater sense of the downsides of the approach adopted in Cherryville, where ethnographic observation did not take place.
Useful lessons nonetheless can be drawn from our analysis, adding to the existing literature that highlights the importance of boards’ leadership styles in orchestrating change, 30 the balance between use of accountability and information systems and reliance on intrinsic motivation,30,33 and the engagement of professional groups. 34 We suggest that those in senior-level roles should not simply identify patient safety as a challenge: they also need to attend carefully to how they frame it as a problem, and how that process influences the choice of therapies. ‘Burning platforms’ – crises that recentre challenging issues and highlight the need for swift action – may be useful devices for those who seek to prioritize quality and safety in health care contexts overwhelmed by ‘priority thickets’. 25 But these crises may be wasted in the rush to solutions. An approach that promotes shared construction of the problem and solutions, on the other hand, may yield significant benefits. This requires caution and courage, but our data suggest that it may secure a more sustainable re-problematization of quality and safety – rather than creating short-term commotion that quickly becomes part of the noise of competing priorities.
Footnotes
Acknowledgements
We thank Sabi Redwood, Joel Minion, and Janet Willars for data collection. We thank all of the many organizations and individuals who participated in this research programme for their generosity and support. We thank our collaborators and the advisory group for the programme.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
NHS REC approval was obtained for this study (reference 10/H0406/38).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We thank the Department of Health Policy Research Programme (Reference No. 0770017) for funding the wider research project on which this study is based. Analysis of the case studies and write-up of this paper was supported by Mary Dixon-Woods’ Wellcome Trust Senior Investigator award WT097899. GPM acknowledges the support of the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care East Midlands (CLAHRC EM). MDW and GPM are supported by the Health Foundation’s grant to the University of Cambridge for The Healthcare Improvement Studies (THIS) Institute. THIS Institute is supported by the Health Foundation – an independent charity committed to bringing about better health and health care for people in the UK. MDW is a National Institute for Health Research (NIHR) Senior Investigator (NF-SI-0617-10026). The views expressed in this article are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health and Social Care.