
Abstract
Objectives
The lifelong health impacts of adverse childhood experiences are increasingly being identified, including earlier and more frequent development of non-communicable disease. Our aim was to examine whether adverse childhood experiences are related to increased use of primary, emergency and in-patient care and at what ages such impact is apparent.
Methods
Household surveys were undertaken in 2015 with 7414 adults resident in Wales and England using random probability stratified sampling (age range 18–69 years). Nine adverse childhood experiences (covering childhood abuse and household stressors) and three types of health care use in the last 12 months were assessed: number of general practice (GP) visits, emergency department (ED) attendances and nights spent in hospital.
Results
Levels of use increased with increasing numbers of adverse childhood experiences experienced. Compared to those with no adverse childhood experiences, odds (±95% CIs) of frequent GP use (≥6 visits), any ED attendance or any overnight hospital stay were 2.34 (1.88–2.92), 2.32 (1.90–2.83) and 2.67 (2.06–3.47) in those with ≥ 4 adverse childhood experiences. Differences were independent of socio-economic measures of deprivation and other demographics. Higher health care use in those with ≥ 4 adverse childhood experiences (compared with no adverse childhood experiences) was evident at 18–29 years of age and continued through to 50–59 years. Demographically adjusted means for ED attendance rose from 12.2% of 18-29 year olds with no adverse childhood experiences to 28.8% of those with ≥ 4 adverse childhood experiences. At 60–69 years, only overnight hospital stay was significant (9.8% vs. 25.0%).
Conclusions
Along with the acute impacts of adverse childhood experiences on child health, a life course perspective provides a compelling case for investing in safe and nurturing childhoods. Disproportionate health expenditure in later life might be reduced through childhood interventions to prevent adverse childhood experiences.
Introduction
Exposure to adverse childhood experiences (ACEs) is strongly related to poorer health across life. ACEs include being a victim of physical, sexual or emotional abuse or neglect as a child and exposure to chronic environmental stressors such as living in a household affected by domestic violence, substance misuse or mental illness. Such exposure can: alter early neurological development including both pleasure and reward centres and pre-frontal cortical impulse control; 1 increase adolescent and adult health-harming behaviours;2–4 change hormonal and immunological systems contributing to chronic tissue inflammation and increased allostatic load; 5 and increase risks of adults having poor social adjustment, reduced cognitive capacity and low mental wellbeing. 6 These physiological and psychological changes lead to increased rates of physical and mental health conditions as well as poorer educational and employment outcomes.2,4,7,8
Strong relationships between ACEs and ill health should result in greater demands on health services amongst those exposed to greater childhood adversity. However, only a few studies have examined the relationship between childhood stressors and adult health service use. Relationships have been identified between childhood abuse and health service use 9 and between increased ACEs and increased prescription drug use.10,11 One Canadian study found each additional ACE (from a possible six) increased the risk of high use of general practitioners by 12%, emergency rooms by 29% and other services by 19%. 12 Little is understood about when during life such increases in use become evident or about how such use relates to socio-economic factors such as deprivation. Thus, while ACEs can increase ill health, service use may depend on individuals having access to health care regardless of their socio-economic status 13 especially as ACEs are more prevalent in poorer populations. 2
Most countries are facing increasingly unserviceable demands on health care budgets. 14 Savings might arise from investing in preventing ACEs. Our aim was to examine the relationship between ACEs and health care use in England and Wales and to explore this relationship in different age groups to understand if and when a legacy of childhood adversity has an impact on health care use.
Methods
Survey sample
A national representative household survey of adults resident in Wales (February to May 2015) and locally representative household surveys in three English regions (Hertfordshire, Luton, Northamptonshire; June to September 2015) were undertaken using the same data collection tools. The surveys aimed to explore relationships between exposure to adverse experiences in childhood and a range of outcomes in adulthood including the adoption of health-harming behaviours, development of long-term health conditions and use of health care.
We used the national postcode address file to select respondents on the basis of residence. Households were selected through random probability sampling stratified by each of the four areas and then by small area deprivation using lower super output areas (LSOAs; geographic areas with a population mean of 1500). Within each region, LSOAs were categorized into quintiles of deprivation based on their ranking in, for Wales, the Welsh Index of Multiple Deprivation (IMD) 2014 15 or, for English regions, the English IMD 2011. 16 Both IMDs use a composite deprivation measure based on domains including income, employment, health, education, access to services, community safety and physical environment. However, Welsh and English IMDs are not directly comparable and therefore deprivation quintiles were calculated separately for England and Wales, with region of residence included as a potential confounder in all multivariate analyses.
Questionnaire
We used established questions from the Centers for Disease Control and Prevention short ACE tool 17 with 11 questions measuring childhood exposure to abuse and family dysfunction experienced by respondents before the age of 18 years. Responses were reduced to nine ACE categories: verbal, physical, and sexual abuse; exposure to domestic violence, parental separation and growing up in a household with mental illness, alcohol abuse, drug abuse or with an individual who had been incarcerated (Supplementary Table 1). Individuals were then categorized into an ACE count group based on the total number of ACEs they reported.2,4
Three self-reported measures of health care use in the last 12 months were collected: number of visits to GPs, number of emergency department (ED) attendances, and number of nights spent in hospital (excluding episodes relating to pregnancy). Responses were categorized into: higher GP visits (six or more); ED attendance (at least one in the last 12 months; yes, no) and overnight hospital stays (at least one in the last 12 months; yes, no). Demographics were age categories, sex, deprivation quintile and ethnicity (white, or black and other minority ethnic group (BME)).
Data collection
For selected households in English regions, a letter was delivered prior to researcher visits that outlined the study, when researchers might visit and information on how to opt out. In Wales, potential participants were presented with a letter upon researcher visits. Trained researchers visited selected houses on all days of the week between the hours of 9 a.m. and 8 p.m. Potential participants were given a study information sheet that outlined the purpose of the study and provided details of its voluntary, confidential and anonymous nature. Individuals were informed that they could withdraw at any point and that doing so would not affect any aspect of their health treatment or other services. After receiving informed consent, the questionnaire was delivered to those meeting the study inclusion criteria (aged 18–69 years; cognitively able to participate in a face-to-face interview and resident in the selected LSOA).
Interviews were conducted by researchers who then entered responses onto data tablets (computer-assisted personal interviewing). However, for sensitive questions, including those measuring ACEs, tablets were passed to respondents to complete questions directly (computer-assisted self-interviewing). All data collection occurred in respondents’ homes and, except where translators were required, questions were asked on a one-to-one basis. As well as English language, and Welsh for those surveyed in Wales, respondents could opt to be interviewed in French, Spanish, Polish, Hindi, Punjabi, Urdu, Gujarati, Bengali, Marathi, Pashto, Sindhi, Saraiki and Balochi.
Data analysis
Data input was undertaken in Microsoft Excel with all statistical analyses completed in SPSS v22. Analyses used chi squared for bivariate examination of associations with health care use and subsequent multivariate modeling employed binary logistic regression to identify relationships independent of demographics. Modelled estimates for prevalence of health care use variables were calculated for ACE count and deprivation quintile combinations using an estimated marginal mean function to adjust for other demographic factors. Binary logistic regression models were repeated for each of five age categories in order to explore how relationships between ACEs and health care use varied with age.
Results
Based on ACE prevalence identified in other UK surveys, 2 overall sample size was set at approximately 7500. Overall, 28,349 households were visited during the study periods. However, 42.8% (n = 12,127) did not result in contact with a resident (e.g. unoccupied premises at time of visit). Of occupied households, 20.8% (n = 3371) were ineligible (e.g. out of age range) including 56 where language could not be accommodated. Another 32.1% (n = 5200) declined to participate and 47.2% (n = 7651) completed a questionnaire. Thus, based on known occupied eligible households, overall compliance was 59.5%. Here however, any individuals who did not complete all questions required for analyses were also removed resulting in a final sample of n = 7414.
The final samples provided coverage of all measured demographics. Comparison between the sample and adult general populations (18–69 years) in study areas identified oversampling of those aged 60–69 years, females, black and ethnic minority (BME) and more deprived individuals in the English sample and of younger (18–29 years), white ethnicity and mid-level deprivation (deprivation quintile 3) individuals in Wales (Supplementary Table 2).
Relationships between health care use in the last 12 months and adverse childhood experiences, deprivation and other demographics.
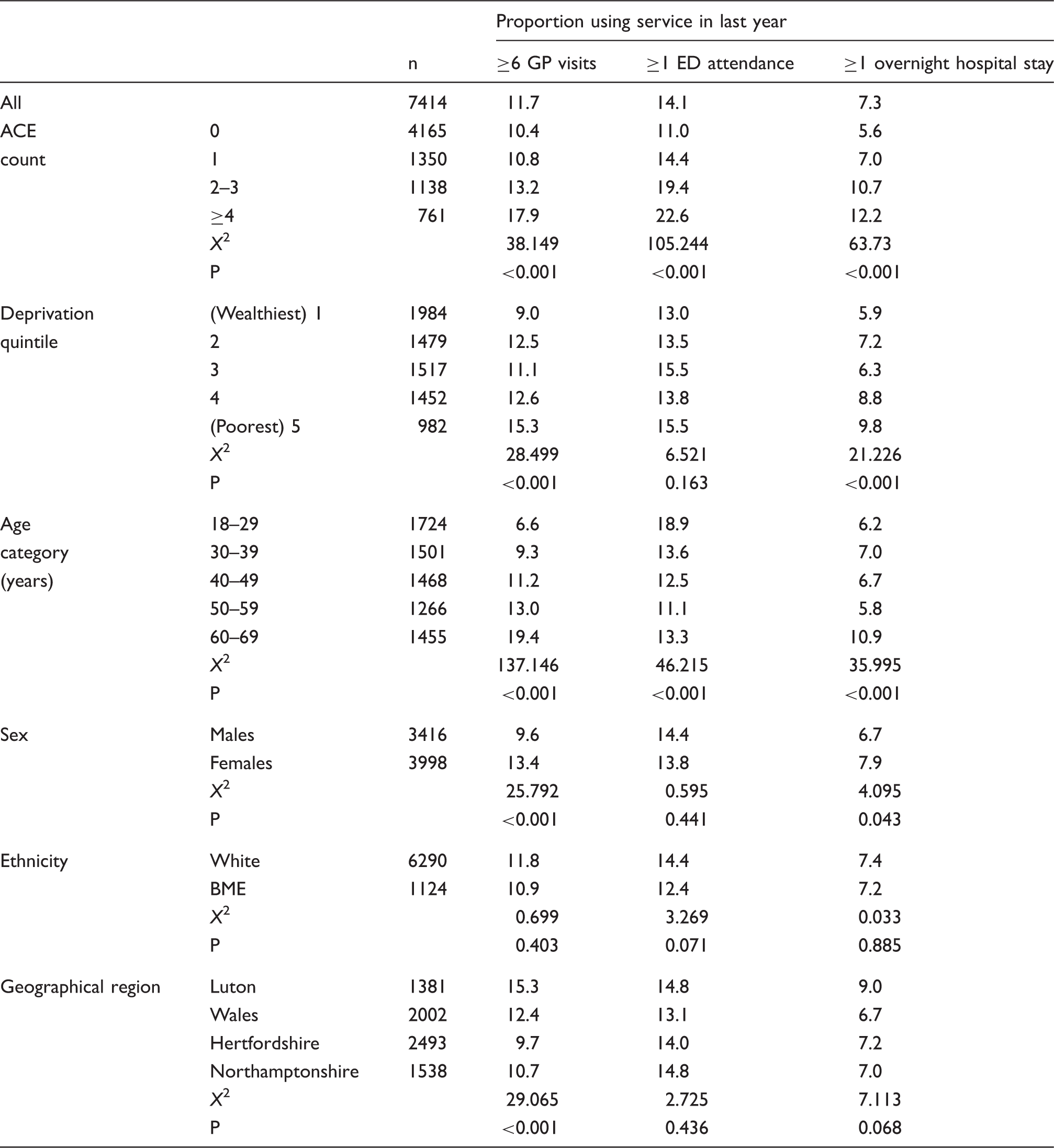
BME: black and minority ethnic groups; ED: emergency department.
The incidence of higher GP use increased with age while ED attendance was elevated in the youngest group and overnight hospital stays in the oldest. Ethnicity was not significantly related to health care use. Women reported marginally higher overnight hospital stays and substantially elevated levels of GP use. Region of residence was also related to higher GP use but not other health care use (Table 1).
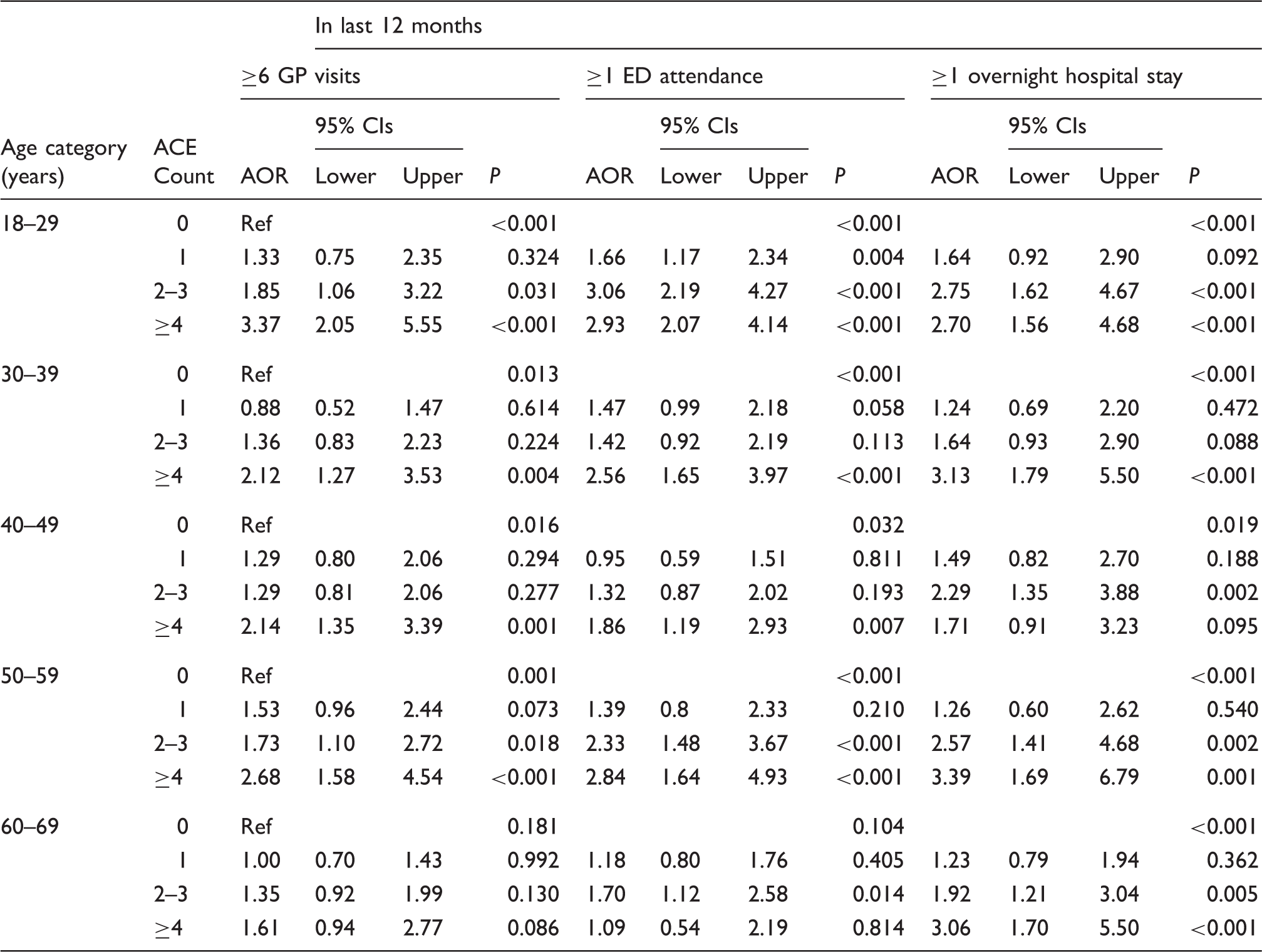
Logistic regression analysis of adverse childhood experiences, deprivation and demographics relationships with health care use.

Note: P values appearing in reference rows relate to testing of the overall contribution of each variable to the model. 95% CI = 95% confidence intervals.
For binary variables, reference categories are female (for sex) and white (for ethnicity).
AOR: adjusted odds ratio; BME: black and minority ethnic groups; ED: emergency department; Ref: reference category.
Modelled sample incidence of health care use by ACE count and deprivation (adjusted to sample average for age, sex, ethnicity and residence) found higher GP use in the last 12 months to range from 7.3% of the most affluent quintile with no ACEs to 23.8% in the least affluent quintile with ≥ 4 ACEs (Figure 1(a)). Equivalent figures for ED attendance and overnight hospital stays were 9.3% versus 21.8% (Figure 1(b)) and 4.1% versus 17.0% (Figure 1(c)), respectively. In all cases, a greater proportion of the variance was explained by ACE counts than deprivation (Table 2, Figure 1(a) to (c)) with increasing ACE counts contributing consistently to levels of all types of health care use across deprivation quintiles.
Adjusted mean percentage of individuals within each category of heath care use by deprivation quintile and ACE count. Adjusted means are calculated using estimated marginal means function and are adjusted through logistic regression modelling for confounding from other variables in the model; here age, sex, region of residence and ethnicity. 95%CI = 95% Confidence Intervals.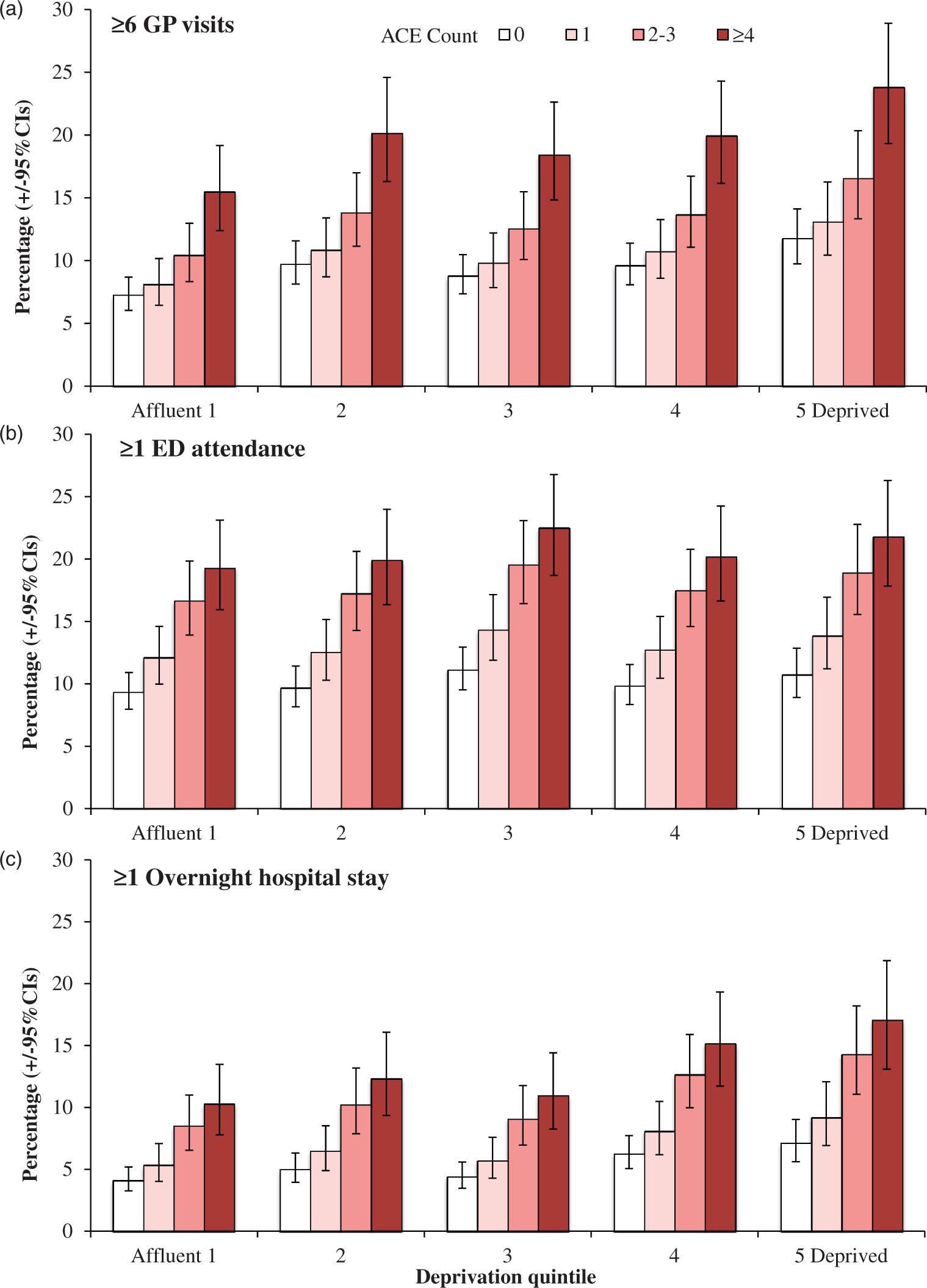
Logistic regression by age shows increases in ACE count are strongly related to higher GP use, ED attendance and overnight hospital stays even in those aged 18–29 years (Table 3). Adjusted odds ratios (≥4 vs. no ACEs) were higher for all categories of use across all other age groups although the difference was not statistically significant for overnight hospital stays in those aged 40–49 years and for both higher GP use and ED attendance in those aged 60–69 years. Adjusted odds for demographics and other independent variables included in the model are presented in Supplementary Table 3. Figure 2 presents the modelled sample incidence of health care use by age. As young as 18–29 years, proportions reporting higher GP use more than triple between those with 0 and ≥ 4 ACEs and for ED attendance and overnight hospital stays more than double (Figure 2(a) to (c)).
Adjusted mean percentage of individuals within each category of heath care use in the last 12 months by age and stratified by ACE count. Adjusted means are calculated using estimated marginal means function and are adjusted through logistic regression modelling for confounding from other variables in the model; here deprivation, sex, region of residence and ethnicity. 95%CI = 95% Confidence Intervals. Age stratified logistic regression analysis of health care use in last 12 months and relationships with adverse childhood experiences.
a
Models included deprivation quintile, sex, ethnicity and geographical region; adjusted odds ratios for these variables are presented in Supplementary Table 3. Ref: reference category; P values appearing in reference rows relate to testing of the overall contribution of each variable to the model. 95% CI = 95% confidence intervals. AOR: adjusted odds ratio; ED: emergency department.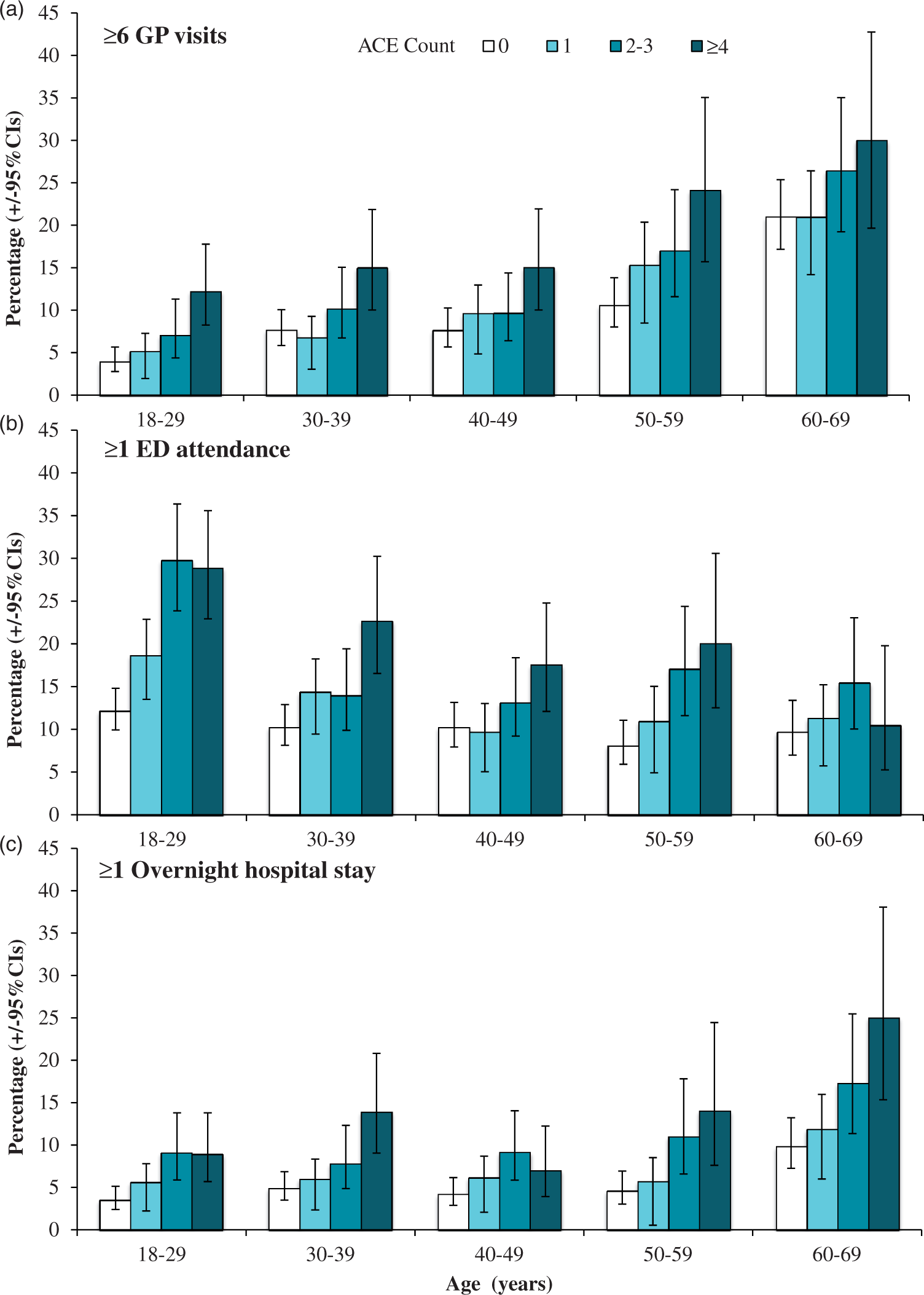
Discussion
Main findings
ACEs are strongly predictive of higher GP use, greater use of emergency care and increased hospitalisation. While GP use and hospitalisation were also related in part to deprivation, the impacts of ACEs appear independent of such deprivation and added to levels of health care use in a dose response fashion across socio-economic groups. Thus, compared with individuals with no ACEs living in the most affluent quintile, levels of higher GP use among those living in the most deprived quintile rose by two-thirds for those with no ACEs but threefold for those with 4 + ACEs.
Critically, the impacts of ACEs on health care use appear to be established by the beginning of adulthood. Thus, in those age 18–29 years, the adjusted prevalence of higher GP use in the last 12 months tripled from those reporting no ACEs to those reporting ≥4 ACEs. Marked increases in ED attendance by 18–29 year olds were seen in both those with 2–3 and ≥4 ACEs with levels more than doubling compared to those with no history of ACEs. Overnight hospital stays showed a similar escalation with increases especially marked in those with a legacy of 2–3 and ≥ 4 ACEs.
Such early increases in health care use may result from increased unintentional injury and violence, mental health conditions, substance use or related somatic complaints; all of which have been associated with ACEs.4,18,19 In the oldest group, there was no independent relationship between ACEs and either higher GP use or ED attendance. In part, this may reflect the strong relationships between ACEs, chronic disease and consequent premature mortality 7 removing individuals that have suffered health impacts from high ACEs from the studied population. However, it may also relate to increasing levels of age-related illness and consequent health care use even in those with lower ACE counts.
Relationship to other studies
Recent estimates suggest that globally almost one in four children have suffered physical abuse, one in five girls suffered sexual abuse 20 and one in three women have been victims of intimate partner violence. 21 A single case of non-fatal child maltreatment is estimated in the USA to result in lifetime costs of $10,530 in adult medical needs and $144,360 in lost productivity. 22 In the UK, the annual costs to adult mental health and substance use services related to childhood sexual abuse have been estimated at £178 million. 23 Other ACEs, such as childhood exposure to domestic violence, have also been linked independently to poor mental health and the adoption of health-harming behaviours. 24 While the impacts of these specific ACEs on health and health care are substantive, results here and from studies elsewhere 12 suggest ACEs have a cumulative impact with each additional ACE suffered increasing risks of ill health and health care use.
Limitations
Interpretation of results from this study is limited by an overall response rate of 59.5%. Further, respondents may not have reported exposure to ACEs or health service use accurately. Response rates and levels of ACEs reported were however similar to other ACE studies. 2 While there were some differences between population and sample demographics (Supplementary Table 2), reported levels of health care use were similar to those reported in national surveys. Thus, 13.1% of Welsh respondents reported at least one ED attendance in the last 12 months and 6.7% reported at least one overnight hospital stay, compared with 17% and 9%, respectively, in the 2015 Welsh Health Survey. 25 The slightly lower levels in our survey may relate to our sample being restricted to adults below the age of 70. No comparable figures were available for GP attendance. Finally, our study design was retrospective. Therefore, only correlation and not causal relationships between exposure to ACEs and subsequent health care use could be established.
Implications for policy
Despite escalating older populations, non-communicable diseases and costs of treatments raising health care demand, investment in the prevention of ACEs as a mechanism to improve life course health is rare. Although programmes to reduce child maltreatment are available (e.g. home visiting, parenting education), 26 even in the European region their implementation at scale is limited. 27 The large-scale implementation of programmes to prevent intimate partner violence in households or to screen for and support parents with substance use or mental health conditions (e.g. in paediatric primary care) 28 is also far from ubiquitous. However, such programmes have the potential to reduce exposure to ACEs and consequently associated health harming behaviours, non-communicable diseases and pressures on health and social services. Our results demonstrate that individuals with high ACE counts present at younger ages and more frequently. A trauma informed health care service should be equipped to appropriately identify and support such individuals; both improving their health and reducing subsequent needs for health care.
Footnotes
Acknowledgements
We thank the residents of Wales, Hertfordshire, Luton and Northamptonshire who participated in the survey and to the staff of BMG research and Future Focus Research for data collection. We would also like to thank Ann Robins, Peter Barker, David Conrad, Kelly O’Neill, Chandraa Bhattacharya, and Barbara Paterson for their support with the development and delivery of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by Public Health Wales, Public Health England and Luton, Northamptonshire and Hertfordshire Councils.
Ethics approval
Ethical approval was obtained from Liverpool John Moores University’s Research Ethics Panel (England and Wales) and Public Health Wales (Wales) and the studies adhered to the Declaration of Helsinki.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.