
Abstract
Objectives
Variation in patterns of referral from primary care can lead to inappropriate overuse or underuse of specialist resources. Our aim was to review the literature on strategies involving primary care that are designed to improve the effectiveness and efficiency of outpatient services.
Methods
A scoping review to update a review published in 2006. We conducted a systematic literature search and qualitative evidence synthesis of studies across five intervention domains: transfer of services from hospital to primary care; relocation of hospital services to primary care; joint working between primary care practitioners and specialists; interventions to change the referral behaviour of primary care practitioners and interventions to change patient behaviour.
Results
The 183 studies published since 2005, taken with the findings of the previous review, suggest that transfer of services from secondary to primary care and strategies aimed at changing referral behaviour of primary care clinicians can be effective in reducing outpatient referrals and in increasing the appropriateness of referrals. Availability of specialist advice to primary care practitioners by email or phone and use of store-and-forward telemedicine also show potential for reducing outpatient referrals and hence reducing costs. There was little evidence of a beneficial effect of relocation of specialists to primary care, or joint primary/secondary care management of patients on outpatient referrals. Across all intervention categories there was little evidence available on cost-effectiveness.
Conclusions
There are a number of promising interventions which may improve the effectiveness and efficiency of outpatient services, including making it easier for primary care clinicians and specialists to discuss patients by email or phone. There remain substantial gaps in the evidence, particularly on cost-effectiveness, and new interventions should continue to be evaluated as they are implemented more widely. A move for specialists to work in the community is unlikely to be cost-effective without enhancing primary care clinicians’ skills through education or joint consultations with complex patients.
Introduction
One important role of general practitioners (GPs) in the UK National Health Service (NHS) is to decide when patients need to be referred to specialists. Over-referral is costly and may expose patients to unnecessary harm, while under-referral deprives patients of treatments from which they could benefit. There is known to be wide and unexplained variation in the referral rates of GPs which can lead to overuse or underuse of specialist resources. 1 There have been many attempts to improve the effectiveness and efficiency of this process, summarized in a review by Roland et al.2,3 It found that transferring services from secondary to primary care and strategies intended to change the referral behaviour of GPs were often effective in improving outpatient effectiveness and efficiency. However, relocating specialists to primary care and developing joint working between primary and secondary clinicians were largely ineffective.
In recent years, the need to improve efficiency of health services has increased. One initiative in England in 2012 was the transfer of responsibility to clinical commissioning groups (CCGs). This required GPs working as part of CCGs to balance their responsibility to their patients with a responsibility to manage NHS budgets. More recently, a number of new models of care, intended to provide more integrated care as well as increasing efficiency have been encouraged. 4 Similar initiatives are ongoing in other countries. 5
Our aim was to update the earlier review on primary care strategies to improve the effectiveness and efficiency of outpatient services. While our primary interest was to identify evidence for England and Wales, we also drew upon international evidence so our findings would be relevant for other countries. We considered the four domains of interventions considered in the previous review, plus an additional one:
Transfer: The substitution of services delivered by specialists for services delivered by primary care clinicians. Relocation: Shifting the venue of specialist care from outpatient clinics to primary care without changing the people who deliver the service. Liaison: Joint working between specialists and primary care clinicians to provide care to individual patients. Professional behaviour change: Interventions intended to change the referral behaviour of primary care clinicians, including referral guidelines, audit and feedback, professional education and financial incentives. Patient behaviour change: Decision aids and aids to patient choice designed to influence decisions about referral to and discharge from specialist clinics.
Methods
We conducted a scoping review to map rapidly the key concepts underpinning a research area and the main sources and types of evidence available. 6 A more detailed report of our methods and findings has been published elsewhere. 7 We considered interventions to improve outpatient efficiency in each of the five domains.
Data sources and search strategy
MEDLINE, EMBASE, HMIC Health Management and Policy database and the King’s Fund database of grey literature were searched for literature published between February 2005 and April 2014 using terms relating to primary care, interventions considered within the five intervention domains and outcomes such as outpatient referral or appointment.
Study selection
Key findings on effectiveness and cost-effectiveness across the intervention categories.

GPs: general practitioners; GPSIs: GPs with a special interest; RCTs: randomized controlled trials; MRI: magnetic resonance imaging; CT: computed tomography; QOF: Quality and Outcomes Framework.
Titles and abstracts of studies identified by the searches were assessed for inclusion by two researchers. Those selected were reassessed by a third researcher. Full texts were then assessed against the inclusion and exclusion criteria by four researchers. Disagreements or uncertainties were resolved by discussion within the research team.
Data extraction and analysis
Study data were extracted by four reviewers into a template. Findings for each intervention category were then summarized by one reviewer, and the summaries discussed and modified by the research team as necessary, to generate an overall conclusion about the impact on outpatient effectiveness and efficiency.
Results
Our search identified 21,135 records, from which 183 were eligible for inclusion. Only a few were controlled trials or systematic literature reviews, with much of the literature comprising observational studies (Figure S1, available online). We provide an overview of the principal findings for each intervention category with examples of the studies which form the basis of each of our conclusions. Where a systematic review or randomised controlled trial (RCT) is available, we include at least one of these as the example; otherwise we have selected references which we believe provide the strongest support (Table 1). A number of studies report interventions within more than one category.
PRISMA flow diagram.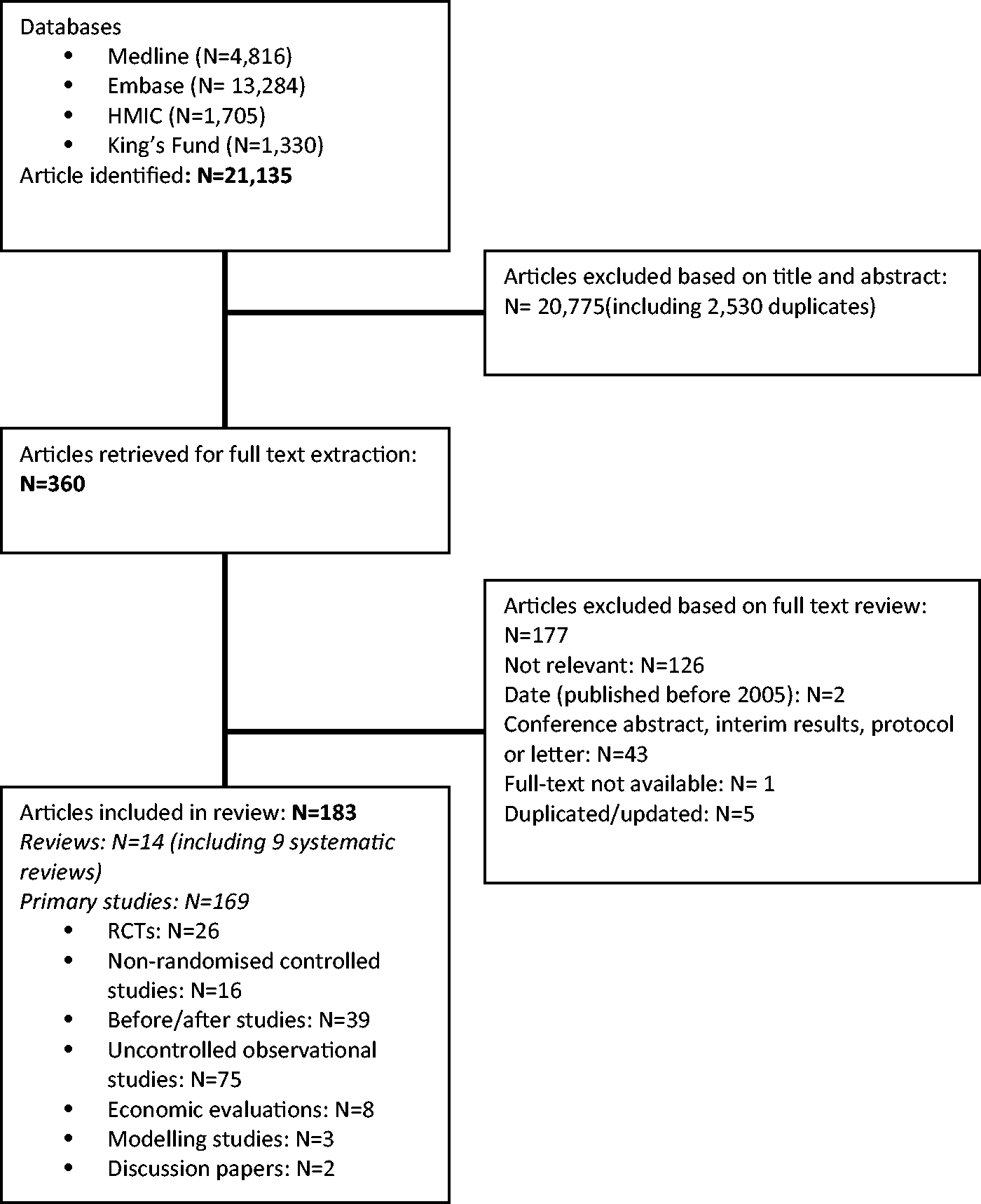
Transferring care to primary care
Our review covered six interventions in which services or elements of services were transferred from secondary to primary care:
Minor surgery (six studies) Medical care of chronic disease (16 studies) GPs with a special interest (10 studies) Outpatient discharge to primary care (13 studies) Direct access by GPs to diagnostic tests and investigations (25 studies) Direct access by GPs to specialist services (seven studies)
The evidence suggests that both minor surgery and care for a range of chronic diseases (including diabetes, asthma, alcohol dependence and chronic obstructive pulmonary disease) can be provided safely and effectively in primary care, as well as some evidence that additional primary care resources can reduce secondary care utilization.8–10 There is also evidence that GPs can follow up patients across a range of diagnostic groups, including cancer, dementia and renal failure, as an alternative to hospital follow-up.
For surgery, medical care and postacute follow-up, it is important that primary care practitioners have additional training and support where needed. The previous review 3 suggested that quality of surgery in general practice was low compared to outpatients, and we found one further study that reinforced that view. 14 However, several other studies that evaluated more specialist, highly-trained GPs (GPs with a special interest (GPSIs)) found no difference from hospital doctors.11,12 Support may be required to ensure that GPs and nurses are confident with their additional roles, 13 and that support from specialists is available when queries or problems arise. 14 Administrative support, such as electronic decision support tools may be needed to ensure that follow-up protocols can be followed reliably. 15
A large number of studies have been conducted that examine the effects of giving GPs access to a wider range of diagnostic tests including magnetic resonance imaging, computed tomography, diagnosis and management of deep vein thrombosis, retinal photography for diabetic retinopathy and gynaecological ultrasound. Especially when combined with a referral protocol, it is evident that GPs can make effective use of a wide range of diagnostic facilities. However, several studies of imaging showed a very low rate of positive findings,10,16 suggesting that investigations may be undertaken when not needed, although in some cases these investigations may still allow avoidance of outpatient referrals.
Seven papers reported on direct access of GPs to specialist services, bypassing the need to see a consultant. Some showed benefits such as improved access and improved patient satisfaction from direct referral to audiology. 17 In one example of direct access to a low visual aid clinic, direct access resulted in an increase in referrals, possibly indicating that unmet need was being addressed. 18 While the costs of transferring services are not frequently reported, cost-effectiveness is likely to depend upon local contractual arrangements, and differ by condition and procedure.
Relocation of specialist services to primary care settings
Our review covered four interventions in which services or elements of services were relocated from a secondary care to primary care setting, with the provider remaining a specialist. These were:
Shifted outpatient clinics (four studies) Specialist attachment to primary care teams (two studies) Community mental health teams (10 studies) Telemedicine (32 studies)
Although studies of shifted outpatient clinics reported that patient satisfaction was high and waiting times were reduced in some cases, the effects on numbers of referrals to both community and hospital services and on costs were unclear.19,20 One new study on attachment of a specialist doctor or nurse to primary care teams reported a reduction in referrals and cost for a clinic run by a GP with special interest together with a specialist allergy nurse compared with referral to a consultant outpatient clinic. 21 A second study described substantial educational benefits for GPs where a consultant visited practices and conducted joint consultations with patients, although this study did not address economic aspects of the intervention. 22
Collaborative models of mental health care appear effective across a wide spectrum of conditions. The evidence suggests that these may be most effective when there are regular opportunities for face-to-face contact between members of the mental health team and the primary care team. 23 There is some evidence that collaborative mental health care can lead to a reduction in further specialist referral 24 but little evidence on the cost-effectiveness of different models of care. 25
Telemedicine ‘store-and-forward’ services have been developed in cardiology, dermatology, ophthalmology and oncology allowing for digital images or other test results be taken locally and sent to specialists for feedback. While services are not physically relocated, this technology allows specialists to provide services within primary care. Teledermatology for images of skin conditions have been shown in most cases to give accurate diagnoses and show potential to reduce referrals, 26 although they appear to be of less value in cases of suspected skin cancer. 27 Few evaluations of telemedicine present robust economic analyses.
Joint management of patients by primary and secondary care clinicians
We found eight new studies relating to shared care of patients, including two systematic reviews.28,29 Overall, these studies suggest that care can be provided in primary care using shared care protocols without loss of quality. Cost savings to patients can be considerable (e.g. transport costs), but savings to the health service are less clear. There are studies which show net savings by moving from outpatient clinics to a shared care model, but such savings are not universal and may depend on the nature of the shared care arrangement.28,30
Professional behaviour change to reduce rates of referral from primary to secondary care
Our review covered seven interventions which attempted to change professional referral behaviour:
Guidelines, including referral proformas (20 studies) Audit and feedback (one study) Professional education including academic detailing (18 studies) In-house review of referrals (four studies) Referral management centres (six studies) Financial incentives (six studies) Advice requests (eight studies)
Several studies (including one systematic review) that considered passive dissemination of referral guidelines, showed them to be ineffective.31,32 However, other studies suggested that guidelines can be effective when used in combination with other interventions such as structured referral proformas.33,34 Studies suggested that both guidelines and professional education have potential to increase as well as decrease numbers of referrals,35–37 and therefore interventions should be aimed at increasing the appropriateness of referrals rather than at demand management. Many studies found that educational programmes were associated with an increase in the appropriateness of referrals,38–40 although some found no impact. 41
From a limited evidence base, feedback on referrals, either internal from within the GP practice (in-house review of referrals) 42 or external 43 can improve the appropriateness of referrals. Evidence for the impact of referral management centres on reducing outpatient referrals was weak. Two studies concluded they were less likely to represent value for money than other approaches such as in-house review of referrals.44,45
Studies on financial incentives focussed on either direct incentives to reduce referrals or on the secondary effects of other incentives. Findings from a review of interventions targeting outpatient referrals suggested that GP fundholding, which created a financial incentive for GPs to reduce referrals for conditions for which they held the budget, resulted in a small reduction in referrals for these conditions. 33 The Quality and Outcomes Framework (QOF), which provided incentives for chronic disease management, appeared to increase referrals in response to particular incentives, for example referrals to a diabetic clinic increased after tighter targets for blood sugar control were introduced into the QOF. 46
A number of studies have evaluated interventions which enable GPs to get email or phone advice from specialists without the need for patients to attend a face-to-face consultation with the specialist. These studies, which cover areas such as endocrinology and neurology, suggest that there is substantial opportunity to reduce the number of patients who are seen in outpatient clinics. Email or phone advice allowed GPs to avoid referral to outpatient consultation47,48 and reduce costs. One study reported that 88% of virtual consultations were resolved without requiring a hospital visit, alongside a reduction of inappropriate referrals from 25% to 10% after introduction of the virtual consultation system. 47
Patient behaviour change
Only one new study, an RCT, assessed the effect of patient coaching or patient decision aids. 49 Patients were offered coaching through an online portal regarding how to discuss their condition with their primary care doctor. Patients in the coaching group were more likely to be referred to a specialist than those who had not received coaching. No difference, however, was found in diagnosis, management or outcomes between groups, suggesting that this increase in referrals may not have been helpful for patient treatment.
Discussion
We identified 183 new studies and reviews published since 2005, across five intervention domains. We kept the same conceptual framework for describing interventions at the primary–secondary interface as the previous review, namely transferring care to primary care, relocation of specialist services to primary care settings, joint management by primary and secondary care clinicians and interventions designed to change professional behaviour, adding an additional domain of interventions for patient behaviour change. Behind many of the studies are assumptions about the benefits of proposed changes such as that overall demand will not change when services are made more available or that services in the community are cheaper. There is a lack of evidence for some of these assumptions with little measurement of the impact of interventions on the health care system and a lack of evaluation of cost-effectiveness. These need to be addressed in future research.
Our findings are consistent with those from the previous review, suggesting that transfer of services from secondary to primary care, and strategies aimed at changing the referral behaviour of primary care clinicians, can be effective in either reducing outpatient referrals or increasing the appropriateness of referrals made. New studies on increasing the availability of specialist advice to primary care clinicians by email or phone, and, to some extent, use of store-and-forward telemedicine, showed potential for reducing outpatient referrals and hence reducing costs. Across all the intervention domains evaluated, there was very little evidence available on cost-effectiveness. Further research is needed to clarify whether even those interventions where there is good evidence for a reduction in outpatient referrals are cost-effective, when costs across the whole health system are taken into account.
There was new evidence on the effect of relocating specialists to primary care or joint primary/secondary care management of patients, suggesting that there can be educational advantages for GPs from these interventions. The previous review concluded that relocation of specialists into primary care, although associated with improved access, was not effective in reducing outpatient attendances. Indeed, studies suggest that, by making services more accessible, there is potential to increase demand by reducing referral thresholds, and there may be a loss of efficiency when specialists do clinics in dispersed community settings. There is evidence of reduced referrals when the specialist (doctor or nurse) carries out joint clinics with a GP with a special interest or provides educational input in some other way. In some new models of care proposed in England, 6 it is therefore important that specialists do more than simply see patients in community settings; new arrangements need to add value through increased interaction with clinicians working in primary care if they are to prove cost-effective.
As a scoping review, this study does not include a formal quality assessment of studies, and as such does not allow us to provide a definitive analysis of the strength of evidence available to support each intervention. However, it did allow us to include a wide range of study designs, albeit with recommendations that can only be cautious when the evidence base is weak. This methodology also allows us to describe the breadth of interventions which have been investigated and provide some assessment of their effectiveness from the diverse evidence available. Further systematic assessments of specific interventions may be required where these do not already exist.
This type of review also allows gaps in the research literature to be identified. Studies are needed which employ rigorous experimental designs, supported by qualitative research to assess factors which may have an impact on implementation in other settings. One particular area needing research is assessment of the cost-effectiveness of interventions, taking into account costs to the whole health system. Cost-effectiveness will depend upon local reimbursement arrangements, or tariffs set up for new initiatives such as ‘advice referral’. This information will be important to those designing new service models and commissioning services.
Two motives drive interventions to change care at the primary–secondary interface: to provide care closer to a patient’s home, 50 thus increasing convenience and to improve overall cost-effectiveness. The literature shows that high-quality care in the community can be provided for many conditions and is popular with patients. However, there are only a few robust economic evaluations, especially those which look at the whole health care system, and some studies suggest that community care may in some circumstances be more expensive due to loss of economies of scale, increased cost of staff and the possibility that providing more convenient access to care may increase demand. Outcomes and costs will also depend on whether or not specialist staff change the type of work they do when they work in the community, for example through closer interaction with primary care staff. A further issue is the distinction between price and cost: economic evaluations tend to use standard published NHS costs, but these may in some circumstances be undercut by the prices charged by NHS providers. This may explain discrepancies where purchasers claim cost savings in situations where the literature finds little evidence of cost-effectiveness. The need for better economic evaluations is one of the key conclusions from this review.
Footnotes
Acknowledgements
We thank Isla Kuhn for her assistance in performing the literature searches for this review. The views and opinions expressed in this paper are those of the authors and do not necessarily reflect those of the NIHR Health Services and Delivery Research programme, NHS England or the Department of Health.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the National Institute for Health Research Health Services and Delivery Research programme (project number 12/135/02).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.