
Abstract
Background:
Few studies assessed drug dispensations for periods >5 years pre-multiple sclerosis (MS) onset or examined the time pre-MS symptom onset.
Objective:
The objective of this study was to examine prescription drug dispensations up to 15 years pre-MS symptom onset.
Methods:
Matched cohort study linking prescription, clinical and administrative data, 1996–2018.
Results:
Among 1243/6212 MS/non-MS persons, those with MS had higher dispensation rate ratios (RRs) pre-onset for systemic antibacterials up to 15 years (RR (range) = 1.15–1.30; q-values (range) = 0.11–0.31), airway drugs up to 8 years (RR (range) = 1.49–1.71; q-values (range) = 0.26–0.35), sex hormones (females only) up to 7 years (RR (range) = 1.19–1.46; q-values (range) = 0.26–0.39) and psychoanaleptics up to 6 years (RR (range) = 1.36–1.59; q-values (range) = 0.09–0.31), but lower beta-blockers (years 13–14 pre-onset, RRs = 0.10; q-values (range) = <0.00001–0.31). After multiple-comparison adjustment, beta-blockers remained significant.
Conclusion:
Drug dispensations differed up to 15 years pre-MS onset and may reflect early disease.
Keywords
Introduction
Healthcare use, including prescription drug dispensations, increases before multiple sclerosis (MS) onset1,2 and could serve as a potential indicator of the prodromal phase.2–4 However, most studies have only examined dispensation patterns in the 5 years pre-MS onset, or the period before the first MS or demyelinating-related diagnostic code or an MS diagnosis identified from administrative data.2–4 Few have considered a longer period or examined the time pre-clinical MS symptom onset, as determined by an MS neurologist. Understanding pre-classical MS symptom onset dispensation patterns may contribute to efforts aimed at recognizing and managing MS earlier and provide insights into the underlying clinical evolutions. 1 Therefore, we examined prescription drug dispensations by drug class up to 15 years before symptom onset in an MS clinic cohort compared to matched persons without MS (pwoMS) in British Columbia (BC), Canada.
Methods
This matched cohort study used multiple data sources from BC. PharmaNet provided data on prescription dispensations at community/outpatient pharmacies which were grouped by drug class (Anatomical Therapeutic Chemical (ATC) classification system, 2nd level, Supplemental Table S1). The Medical Service Plan included physician visits and the Discharge Abstract Database included hospitalizations, with diagnoses coded using the International Classification of Diseases, Ninth and Tenth Revisions (ICD-9/ICD-10). Population registry data included sex, birth date, registration dates for healthcare coverage, and postal code which was linked to neighbourhood-level income as a measure of socioeconomic status, and region of residence (urban/rural). Population Data BC facilitated data linkage and provided secure access to de-identified data for analyses. Data were available from January 1996 to September 2018.
We included people diagnosed by a neurologist at one of four participating BC MS clinics using the prevailing criteria and with a known MS symptom onset date, as determined by the neurologist, typically at the first clinic visit. For 6.3% of participants with an earlier MS-related claim (an MS/demyelinating disease-related ICD-9/10 code or MS disease-modifying drug (DMT) prescription fill), the claim date was assigned as the MS symptom onset date (Supplemental Tables S2 and S3). Each person with MS (pwMS) was matched with up to 5 pwoMS (without MS/demyelinating codes, DMT dispensations or an MS clinic visit) from the general population by sex, exact birth year, 3-digit postal code at the year of MS symptom onset and residency time, without replacement. The pwMS and the matched cohort had to be BC residents for ⩾90% of days annually for ⩾5 years pre-MS symptom onset until the pwMS’s first clinic visit. The matched cohort were assigned the same onset date as their matched pwMS.
We utilized overdispersed-Poisson regression modelling, incorporating person-time as the offset, to compare yearly dispensation rates by drug class (ATC, 2nd level) between pwMS and pwoMS in the years pre-MS symptom onset date. The Benjamini–Hochberg procedure was applied for multiple comparisons. Findings were reported as rate ratios (RRs, 95% confidence intervals (CIs)). Analyses were performed using Rv4.0.5.
Results
The cohort comprised 1243 pwMS and 6212 matched individuals; 72.2% were female, averaging 37.8 years (standard deviation (SD) = 11.4) at MS symptom onset (Table 1).
Characteristics of the persons with multiple sclerosis (pwMS) and the matched cohort without MS drawn from the general population, British Columbia, Canada.
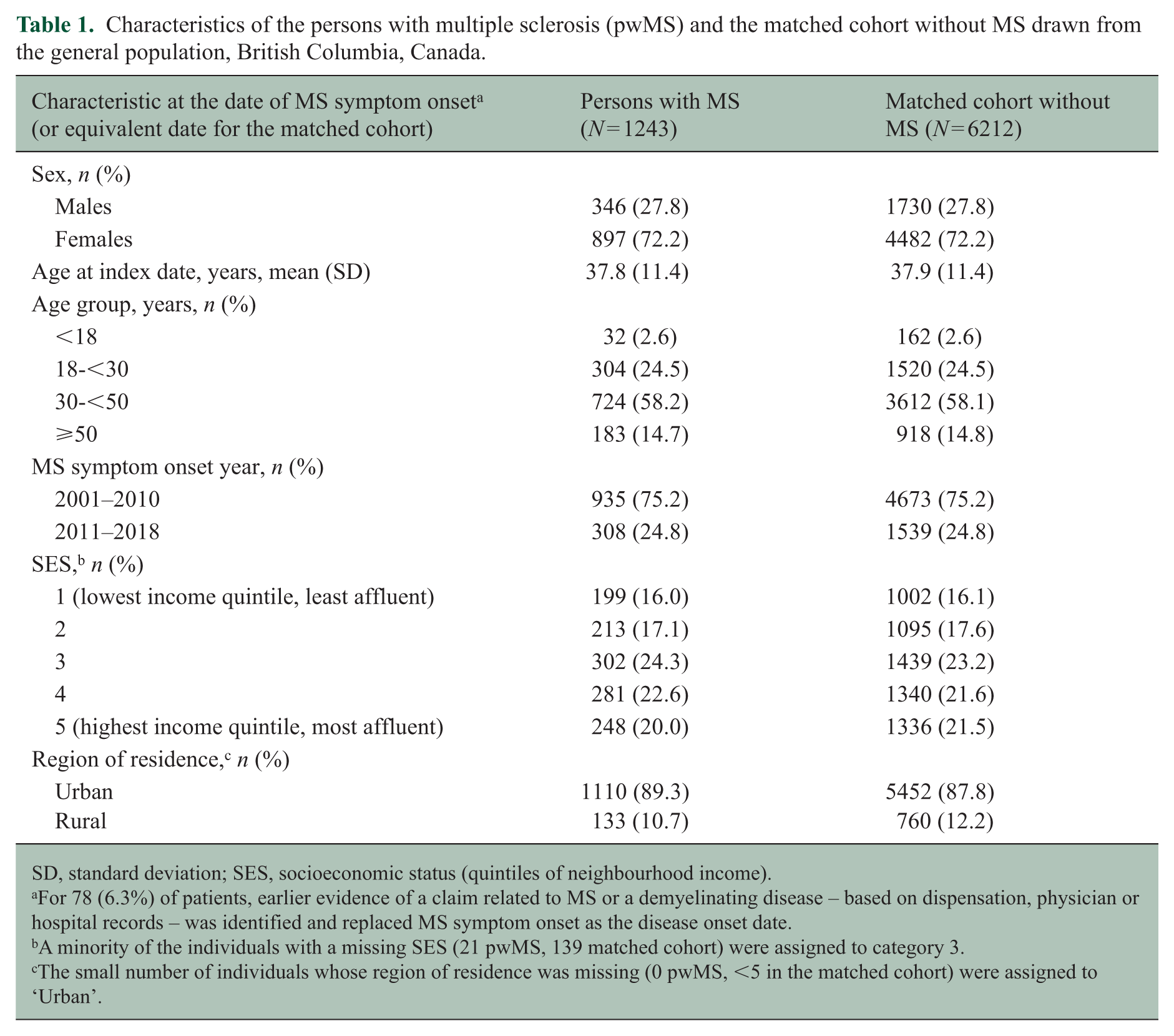
SD, standard deviation; SES, socioeconomic status (quintiles of neighbourhood income).
For 78 (6.3%) of patients, earlier evidence of a claim related to MS or a demyelinating disease – based on dispensation, physician or hospital records – was identified and replaced MS symptom onset as the disease onset date.
A minority of the individuals with a missing SES (21 pwMS, 139 matched cohort) were assigned to category 3.
The small number of individuals whose region of residence was missing (0 pwMS, <5 in the matched cohort) were assigned to ‘Urban’.
Compared to the matched pwoMS, pwMS had a higher dispensation rate for systemic antibacterials (elevated in years −15, −8, −7 and −6 pre-MS symptom onset, RR range = 1.15–1.30) (Figure 1 and Supplemental Figure S1 and Table S4). Obstructive airway disease-related drug RRs were elevated in year −8 (RR = 1.71; 1.01–2.89) and year −4 (RR = 1.49; 1.07–2.07). Among females, sex hormones were elevated from year −7 (significant in six of these years, RR range: 1.19–1.46). Psychoanaleptic drugs were elevated from year 6 pre-MS symptom onset (significant in years −6 to −2; RR range = 1.36–1.59). Analgesic dispensation rates were elevated in each of the 4 years pre-onset (RR range = 1.43–1.55). Closer to the date of MS symptom onset, dispensations for acid-related disorders were elevated in year −2 (RR = 1.40; 1.02–1.91) and topical antifungals in year −1 (RR = 1.62; 1.17–2.23). Other drug classes exhibiting sporadic elevations are described in the Supplementary results.
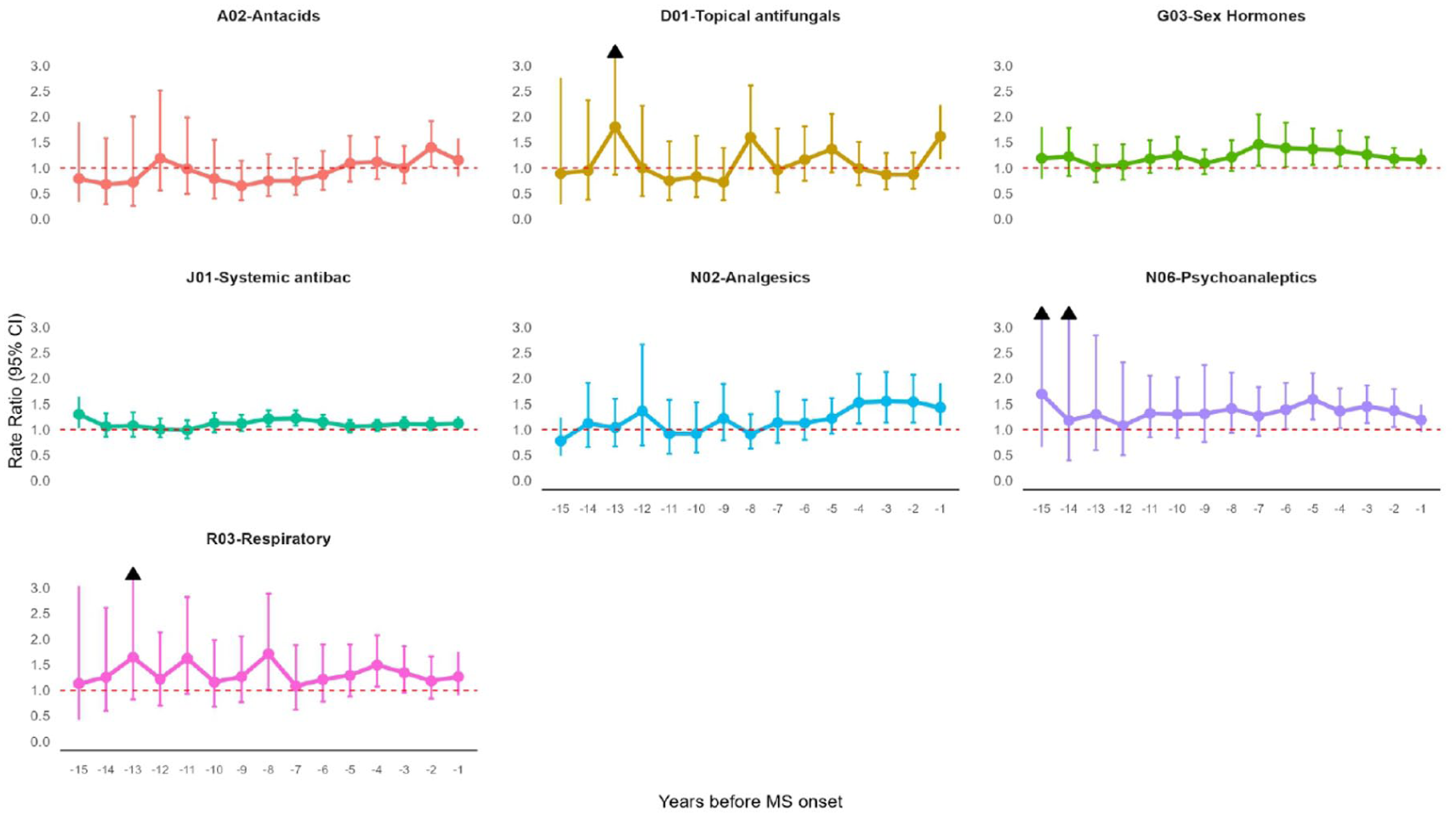
Comparison (rate ratios) of selected drug classes (ATC 2nd level codes) in each of the 15 years before MS onset between persons with multiple sclerosis (pwMS) and the matched cohort without MS in British Columbia, Canada.
Adjustment for multiple comparisons attenuated most associations, with only one (beta-blockers at year −14) remaining statistically significant (q-value < 0.00001, Supplemental Table S4). Post hoc descriptive analyses of which physician visit diagnoses occurred within 14-day pre-dispensation indicated antibacterials (J01) were linked to infection and analgesics (N02) to neurologic/musculoskeletal codes (Supplementary Methods 1, Table S5).
Discussion
Dispensation of several medications was elevated up to 15 years pre-MS symptom onset versus pwoMS, extending beyond prior reports but consistent with increased physician visits over a similar period. 5 Systemic antibacterials were elevated up to 15 years pre-MS symptom onset, followed by obstructive airway disease-related drugs (up to 8 years), sex hormones (up to 7 years), psychoanaleptics (up to 6 years) and analgesics (up to 4 years) pre-MS onset, while others increased only in the 1–2 years pre-MS onset (topical antifungals and anti-acid-related drugs). After multiple-comparison adjustments, only beta-blockers (lower at year −14) remained statistically significant. Changes in medication use occur pre-clinical MS symptom onset and may serve as indicators of the prodromal phase.
Elevated psychoanaleptic dispensations align with the increased psychiatric visits observed up to 14 years pre-onset,5,6 and with the higher psychiatric burden recognized post-MS onset. 7 Similarly, higher analgesic dispensations are consistent with our prior work (in an overlapping cohort) of increased pain prescriptions in the 5 years pre-MS onset (based on the first demyelinating event in administrative data rather than the clinical MS symptom onset date). 4 In addition, increased acid-suppressant dispensations correspond with the higher prevalence of physician visits for gastrointestinal complaints reported in the 5 years before the first demyelinating event. 8 Elevated dispensations of anti-infective medications pre-MS onset, including antibiotics, topical antifungals and obstructive airway disease–related drugs, may reflect greater infection susceptibility and lung-related morbidity in the MS prodrome, consistent with what is known of MS after diagnosis. 9 However, the very early rise in antibacterials could also represent a risk (trigger) factor for MS onset. Among females, elevated sex hormone dispensations may reflect intentional pregnancy delay in the context of unresolved health challenges during the prodromal phase.2,10 After multiple-comparison adjustment, only beta-blockers at year −14 remained significant (q < 0.00001), highlighting the exploratory nature of the analyses and warranting cautious interpretation.
A study strength was the use of an MS clinic cohort. However, reliance on symptom onset date to determine MS onset may introduce recall bias. Medication dispensations were elevated up to 15 years pre-clinical MS symptom onset.
Supplemental Material
sj-docx-1-msj-10.1177_13524585261450813 – Supplemental material for Prescription drug dispensations 15 years before multiple sclerosis onset: A matched cohort study, British Columbia, Canada
Supplemental material, sj-docx-1-msj-10.1177_13524585261450813 for Prescription drug dispensations 15 years before multiple sclerosis onset: A matched cohort study, British Columbia, Canada by Marta Ruiz-Algueró, Seid Mussa Ahmed, Feng Zhu, Yinshan Zhao, Ruth Ann Marrie and Helen Tremlett in Multiple Sclerosis Journal
Footnotes
Acknowledgements
Access to data provided by the Data Stewards is subject to approval but can be requested for research projects through the Data Stewards or their designated service providers. The following data sets were used in this study: BC MS Clinical database; Medical Services Plan (MSP) Payment Information File; PharmaNet; Consolidation File (MSP Registration & Premium Billing); and The Discharge Abstract Database (DAD). You can find further information regarding these data sets by visiting the PopData project webpage at ![]() . All inferences, opinions and conclusions drawn in this publication are those of the author(s) and do not reflect the opinions or policies of the Data Steward(s).
. All inferences, opinions and conclusions drawn in this publication are those of the author(s) and do not reflect the opinions or policies of the Data Steward(s).
We gratefully acknowledge the neurologists of the British Columbia Multiple Sclerosis Clinics for their important contributions to this study through patient assessments. Current and active members at the time of data extraction are listed according to their clinic affiliation: (i) UBC MS Clinic: A-L. Sayao, MD, FRCPC; A. Traboulsee, MD, FRCPC; J. Hooge, MD, FRCPC (UBC and Prince George MS Clinic); L. Kastrukoff, MD, FRCPC (UBC and Prince George MS Clinic); J. Oger, MD, FRCPC; S. Hashimoto, MD, FRCPC (UBC and Victoria MS Clinics); and V. Devonshire, MD, FRCPC; (ii) Victoria MS Clinic: D. Parton, MD, FRCPC; K. Atwell-Pope, MD, FRCPC; and O. Hrebicek, MD, FRCPC; (iii) Kelowna MS Clinic: D. Adams, MD, FRCPC; D. Craig, MD, FRCPC; and S. Meckling, MD, FRCPC; and (iv) Prince George MS Clinic: L. Daly, MD, FRCPC.
Author contributions
M.R.-A. analysed, investigated and created visualizations. S.M.A. interpreted the results and drafted the manuscript. F.Z. analysed, secured funding, investigated and developed the methodology. Y.Z. conceptualized, secured funding, curated data, investigated and developed the methodology. R.A.M. conceptualized, secured funding and designed the study. H.T. conceptualized, secured funding, designed the study, investigated, administered the project, provided resources and offered supervision. All authors revised the manuscript critically for intellectual content, approved the final version and had full access to the data. The corresponding author had the final responsibility to submit for publication.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: M.R.-A. receives funding from the Michael Smith Foundation for Health Research Trainee Award in partnership with the Tai Hung Fai Charitable Foundation and the Edwin S.H. Leong Centre for Healthy Aging; she received a travel award from MS Canada to attend the endMS Summer School 2024. S.M.A. received travel awards from ACTRIMS to attend the 2024 and 2025 ACTRIMS Young Scientist Summits and from the UBC MS Connect Education Program to attend and present at the 41st ECTRIMS Congress in 2025. Y.Z. and F.Z. have no disclosures. R.A.M. receives research funding from CIHR, MS Canada, Crohn’s and Colitis Canada, the National Multiple Sclerosis Society, CMSC, the Arthritis Society, the US Department of Defense, MMSF, CHRIM and Pfizer Foundation and is a co-investigator on studies receiving funding from Biogen Idec and Roche Canada. She holds the Multiple Sclerosis Clinical Research Chair (Dalhousie). H.T. has, in the last 5 years, received research support from the Canada Research Chair Program, the National Multiple Sclerosis Society, the Canadian Institutes of Health Research, MS Canada, the Multiple Sclerosis Scientific Research Foundation and the EDMUS Foundation (‘Fondation EDMUS contre la sclérose en plaques’). In addition, in the last 5 years, she has had travel expenses or registration fees prepaid or reimbursed to present at CME conferences or attend meetings (e.g. as a member of the International Advisory Committee on Clinical Trials in Multiple Sclerosis) from the Consortium of MS Centres (2023), the Canadian Neurological Sciences Federation (2023), the National MS Society (2022–2025), ECTRIMS/ACTRIMS (2017–2025), MS Canada (2023, 2025) and the American Academy of Neurology (2019). Speaker honoraria are either declined or donated to an MS charity or to an unrestricted grant for use by HT’s research group.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was funded by the National MS Society and MS Canada (RG5063A4/1/RFA-2103-37392; EGID: P002/903124/3743; PI: H.T.). The funders had no role in the methods, analyses, manuscript preparation or decision to submit for publication.
Ethical approval
This study was approved by the Clinical Research Ethics Boards at the University of British Columbia (H20-03232-A007).
Data availability statement
Since we are not the data custodians, we are not authorized to make these data available. However, with the necessary approvals, data may be accessed through Population Data British Columbia.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.