
Abstract
Treatment of multiple sclerosis (MS) has become increasingly multifaceted and comprises not only a variety of disease-modifying drugs with different mechanism of action but also a wide range of symptomatic therapies. Today, it is not possible for the family physician or even many general neurologists to master the current treatment algorithm, and this calls for the establishment of multidisciplinary MS Care Units. The core of the MS Care Unit would, in addition to MS neurologists and nurses, typically comprise neuropsychologists, clinical psychologists, physiotherapists, occupational therapists and secretaries, and will work together with a group of different specialists on formalized diagnostic workup procedures, protocols for initiation and follow-up of disease-modifying therapies. It is obvious that the terms of performance of different MS Care Units will vary across regions and need to be balanced with clinical practice according to local conditions. Although the main objective for establishment of MS Care Units will be to offer the single MS patient seamless and correct management of the disease to increase patient satisfaction and quality of life, it may even be cost-effective for the society by maintaining the working ability and reducing the costs of home help and custodial care by keeping people with MS resourceful.
Keywords
Introduction
In neurology, the establishment of stroke units has dramatically changed the treatment of acute stroke. The comprehensive stroke unit has reduced the length of stay in hospital and combined reduction of death and improved functional outcome compared to previous treatments. Stroke patients, who receive organized inpatient care in a stroke unit, are more likely to be alive, independent and living at home 1 year after the stroke.1–3
Another area, in which multidisciplinary clinics have been shown to be useful, is in the management of amyotrophic lateral sclerosis where a number of studies have shown improved care of the patients.4–6
Treatment of multiple sclerosis (MS) is more complex than treatment of acute stroke and amyotrophic lateral sclerosis. MS is a disease that typically affects young people and has a chronic long-lasting course. Disease-modifying therapy (DMT) has become increasingly multifaceted and comprises a wide range of drugs with different mechanism of action and adverse effects that need meticulous monitoring.7,8 The quick access to a large set of investigations, including magnetic resonance imaging (MRI), multimodal evoked potentials, optical coherence tomography, immunological tests and antibody tests, requires an advanced level of organization. Even symptomatic therapy has become more extensive, involving a wide range of treatments for spasticity, bladder, bowel and sexual disturbances, pain, fatigue and cognitive impairment. 9 It is not possible for the family physician to master the current treatment algorithm embracing an increasing number of disease-modifying drugs, and not even the general neurologist giving care to only a few patients with MS will acquire the expertise necessary to provide the gold standard of therapy in patients with therapeutically complicated MS.
Patient population and needs
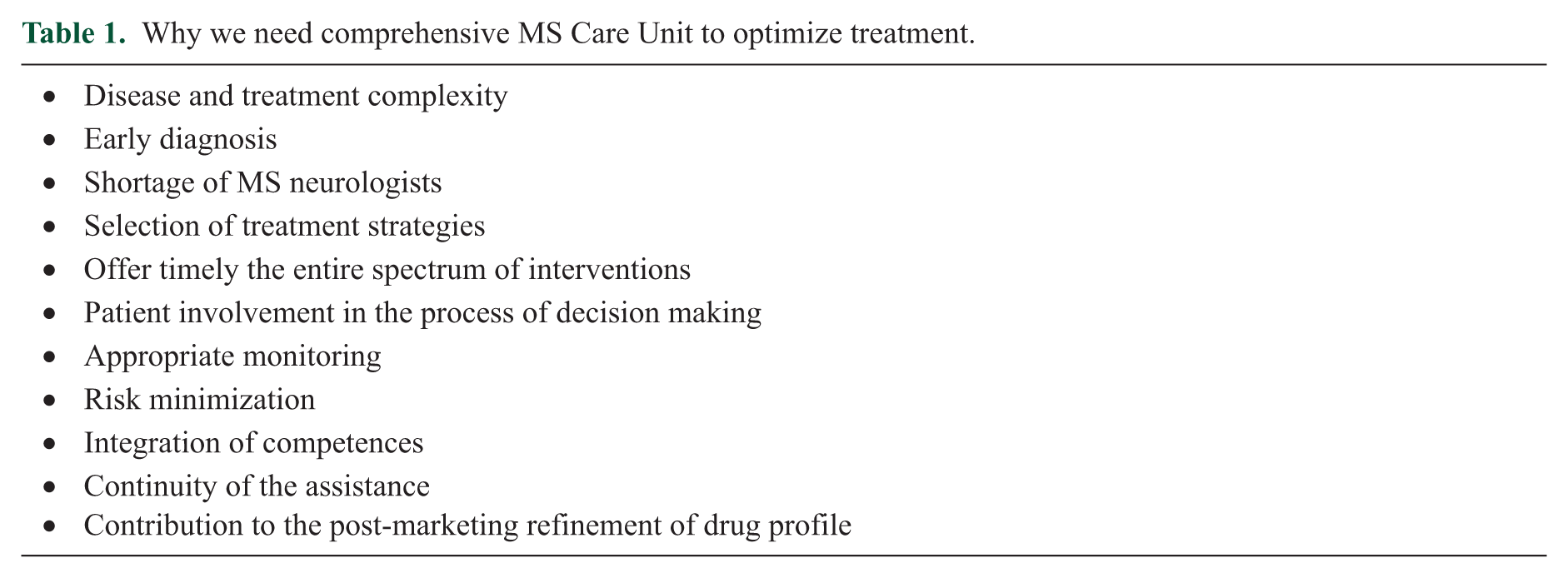
There are many reasons why we need to promote worldwide the concept of MS Care Unit, summarized in Table 1.
Why we need comprehensive MS Care Unit to optimize treatment.
Our knowledge of the current treatment of MS across the European countries is insufficient. The European MS Platform (EMSP) has performed a mapping of 26 MS registries in Europe in spring 2017 and demonstrated the currently existing fragmentation in data collection and data analysis; in most registries and cohorts, the neurologist alone is filling in patient data.
The quality of health care varies according to European nations, regions and settings (http://www.emsp.org/wpcontent/uploads/2015/08/MS-in-EU-access.pdf). Different studies have been reported focusing on collecting and publishing report data on the quality of the health care models. Although the studies made the above data increasingly available to the public, more studies are needed to evaluate patients’ perspective on MS care models. Since the ultimate goal of the multidisciplinary MS Care Unit approach is to increase patient satisfaction and quality of life (https://www.msif.org/living-with-ms/what-influences-quality-of-life/seven-principles-to-improve-quality-of-life/), core and transversal to the implementation of the above approach is the development of an effective framework to enable people with MS engagement and activation.
A recent study analysed responses from MS neurologists in several European countries regarding choice of therapy to various clinical situations. The treatment choices varied considerably, even in countries with the same access to all approved drugs for treatment of relapsing-remitting MS. 10 Early treatment and personalized approach are considered as two fundamental steps for the success of DMTs in MS, both are linked to the definition of various clinical and laboratory prognostic and predictive factors,7,11 easily available in well-organized clinical centres only. Accurate monitoring of the treatment response and a quick shift to an alternative DMT can only be possible if the contact of the patient with the treating neurologist is facilitated by an appropriate assistance setting, including some recent technical developments, such as remote control by wearable devices. Approval of new DMTs is usually associated with post-marketing studies to a better definition of the safety/efficacy profile. Databases and registries are used to provide this type of information; however, the quality of these tools is essential and again depends on the MS centre organization. 12
MS affects several body systems and patients invariably require specialized interdisciplinary support. Both patients with relapsing and progressive forms of MS may benefit from a multidisciplinary approach. 13 The MS neurologist and MS specialist nurse are the key persons in the management of all patients with MS.
Patients with an Expanded Disability Status Scale (EDSS) score of 0–3 are usually managed as outpatients, and the main mission in these patients is to provide adequate treatment with disease-modifying drugs. Mild impairment tends to require specific management of symptoms such as spasticity, urinary disorders or mild gait/posture disturbances. Fatigue is a common complaint even at lower level of disability. Collaboration with external therapists may provide encouragement for patients to maintain regular physical activities.
In patients with greater degree of disability (EDSS score: 3–6), management involves a multidisciplinary team consisting of a physiotherapist, speech therapist, occupational therapist and neuropsychologist. Close collaboration with external social care services is required to maintain the working ability of the patient and connection to the labour market.
The major intervention in patients with an EDSS score >6 remains the management of the many symptoms and neurological deficits that are the result of the progressive clinical phenotype. 14 The main goals of physical therapy and rehabilitation are to maintain patients’ autonomy and quality of life at home and to avoid complications to the MS disease. Management tends to focus largely on physiotherapy and occupational therapy aiming primarily on disability compensation, but also towards functional recovery, so that patients can continue with their activities. The majority of patients with high EDSS scores require technical aids, such as a wheelchair, crutches and ankle foot orthoses, and are reliant on considerable support from their carers. Several studies consistently indicated the need for MS patients to have psychosocial support.15,16
The proportion of patients using inpatient, outpatient and social care increases with the degree of disease severity. A Swedish study analysed the use of health, social and informal care services and satisfaction with care in a population-based sample of people with MS in Stockholm County. 16 During a 3-year period, 92% had been in contact with a neurology outpatient clinic. Over two-thirds had been in contact with other hospital outpatient departments; the most frequently used was departments of urology. There were no significant differences among patients with various disease severities (EDSS) regarding the proportion using outpatient care at departments of neurology. The great majority of MS patients used hospital specialist care and primary care in parallel, with many departments and services involved.
At least in some countries, there is still an unmet need for physiotherapy, occupational therapy, equipment and aids, together with social, financial and employment unmet needs. Overall, the unmet needs were more frequent in patient with progressive MS.17,18
Ongoing initiatives
The Multiple Sclerosis International Federation (MSIF) movement’s new strategy, 2017–2021, identified the potential for good quality, rigorous patient data and analysis to speed up discoveries in MS research, inform decisions made by all the health workers and the other stakeholders involved and ultimately improve outcomes for people living with MS. To meet the above need, in 2017 MSIF launched an international collaborative initiative, which will engage and commit experts from around the world, and is led by the Italian MS Society, with the overall goal to identify and define the functional domains that matter most to people with MS and develop research-based methods to be used in MS Care decision-making processes, in data sharing and ultimately in regulatory decision-making.
There are currently different ongoing actions of the MS Care Unit. The MS Brain Health initiative is in the process of doing a Delphi survey to define by consensus the metrics that the wider MS community need to measure how they are functioning against internationally defined quality standards.
Within the frame, the importance of patient activation programmes in MS management has been recently discussed in a review that reflects the content of the presentations, audience polling results and discussions of the second Pan-European MS Multi-stakeholder Colloquium. 19 It was proposed that evidence-based care practice guidelines for MS should be developed at the European level (http://www.eurims.org/News/recommendations-on-rehabilitation-services-for-persons-with-multiple-sclerosis-in-europe.html). These guidelines would supplement the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS)–European Academy of Neurology (EAN) Clinical Practice Guideline on Pharmacological Management of Multiple Sclerosis.
The MS Care Unit
According to the recent ECTRIMS-EAN guidelines for treatment of MS, the entire spectrum of disease-modifying drugs should only be prescribed in centres where there is an adequate infrastructure to provide proper monitoring of patients, comprehensive assessment, and detection of side effects and ability to promptly address them. 20
In some countries (e.g. Canada), certain MS drugs are marked ‘XX®’ and should only be prescribed by neurologists, who are experienced in the treatment of MS, are knowledgeable of the efficacy and safety profile of XX and are able to discuss benefits/risks with patients. This condition will of course always be accomplished of a multifocal MS Care Unit. 21
A multidisciplinary MS Care Unit approach can be defined as the presence of a group of different specialists, who work together and with the MS neurologists and nurses with a formalized diagnostic workup procedure, protocols for initiation and follow-up of DMTs and management of complications. The MS Care Unit should offer availability of a specific single contact neurologist and nurse, who can provide information, support and advice to the individual MS patients. This is imperative as a recent study on the effect of organizational features on patient satisfaction with care in Italian MS centres clearly showed that patient satisfaction was inversely associated with hospital size, probably because larger hospital may have failed in building an individualized relationship between patients and the MS neurologist and nurse and tailoring the communication of information. 22
The premises of the MS Care Unit should comprise an outpatient clinic with consulting/examining rooms, rooms for procedures, for example, lumbar puncture and filling of intrathecal baclofen pumps, and a dedicated quiet room or area, free from distraction or interruption, where patients receive information about their disease. Ideally, the MS Care Units should have their own infusion centre and other spaces dedicated to other professionals. In addition, the MS Care Unit should have inpatient facilities or have access to admission of patients to a department of neurology with well-designed care for MS patients.
Organization of the MS Care Unit
The core of the MS Care Unit is the patients and would in addition to MS neurologists and nurses comprise (at least three of) neuropsychologists, clinical psychologists, physiotherapists, occupational therapists, speech therapists, social workers and secretaries, and the multidisciplinary MS clinic should offer specialist services in dietary matters, and in the treatment of spasticity, incontinence and pain. Some of these services may, however, be provided by a MS neurologist or MS nurse in the MS Care Unit with special education and interest (Figure 1).
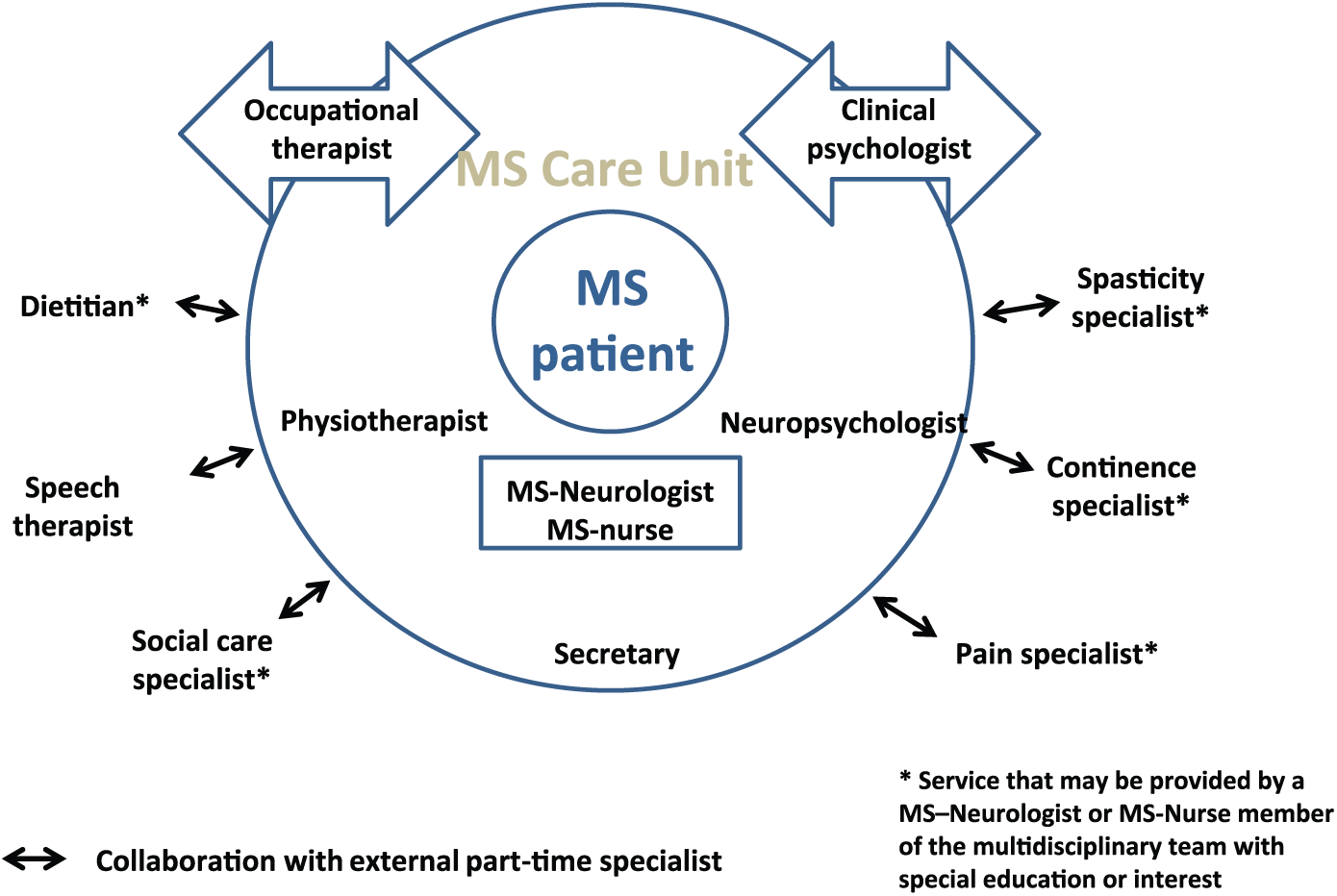
Minimum requirements for a multidisciplinary MS Care Unit.
In patients with relapsing forms of MS, the correct diagnosis and DMT should be secured by the neurologists in the MS Care Unit, who have special interest in MS, and who use the majority of their clinical working hours with treatment of MS patients. Together with the MS specialist nurses, these neurologists constitute the backbone of the health care persons in the MS Care Unit.
The multidisciplinary MS Care Unit should collaborate with a pharmacist with special knowledge of MS therapies and be able to offer the full range of approved DMTs for relapsing and progressive MS and to tailor the treatment to the single patient’s need. In addition to personalized therapy using drugs licenced for the treatment of MS, the MS Care Unit should have a variety of experimental therapies at disposal of patients with therapeutic refractory MS. This approach requires specially trained MS neurologists and MS nurses. 21
The neuropsychologist is essential for the assessment of neuropsychological problems that in MS patients can be classified into three broad categories: cognition, mood disorders and behavioural symptoms. Irrespective of the severity of the deficits, it is important to diagnose all cases of cognitive impairment and to monitor its evolution at regular neuropsychological assessment by a neuropsychologist or an occupational therapist supervised by a neuropsychologist (e.g. at the start of and during immunotherapy, and in the event of worsening). Cognitive rehabilitation may keep the mildly cognitive MS patient able to maintain working and the more progressed patients able to stay in their own homes.
In patients with moderate or more pronounced disability, the mainstay of treatment for both weakness and spasticity is physical therapy and exercise. 23 Hence, physiotherapists constitute an essential group in the multidisciplinary MS Care Unit, and they should have a strong collaboration with physiotherapists in rehabilitation clinics and in the primary health sector.
Occupational therapists may be an integrated part of the multidisciplinary MS Care Unit or can be associated to the unit. The majority of patients with high EDSS scores require technical aids in order to maintain independence and ability of staying in their own homes. Usually, the occupational therapist works in close collaboration with the physiotherapist and the neuropsychologist.
Patients with speech difficulties may benefit greatly when their deficits are managed by a speech therapist who usually is an external collaborator in smaller clinics.
The whole neurorehabilitation team in the multidisciplinary MS Care Unit liaises regularly with the patient’s external therapist to encourage and facilitate maintenance of physical and social activities. Collaboration with external neurorehabilitation institutions is important in relation to patients who are in need of longer inpatient rehabilitation stay.
The clinical psychologist may facilitate the development of effective communication and relationship between the clinician and the patient, which may significantly increase MS patients’ satisfaction with healthcare. In relation to adaption to the new life situation after having the diagnosis of MS and when deterioration of health occurs, the accessibility to psychological support and crisis therapy is essential. Effectively, the National Institute for Health and Care Excellence (NICE) guidelines recognize that psychological support should be routine in the management of patients with MS (NICE 2003 and NICE 2014).24,25
The medical social worker or counsellor is important offering advice on social security matters to MS patients at different stages of the disease course and is mediator of social care and home care services delivered by the public social services departments. These services include home help, personal assistants, transportation, physiotherapy and technical aids such as a crutches and other walking aids, wheelchair and mini crossers.
The personnel of multidisciplinary MS Care Unit should be able to offer expertise in treatment of spasticity, incontinence and pain and to give advice on dietary aspects, conveyed by specially educated MS neurologists or MS nurses with special interest in the topic, and for matters that are not mastered by the personnel in the MS Care Unit, connection and collaboration with external specialists should be established.
The role of the general practitioner in the management of MS patients vary considerably between countries in Europe, and in countries in which the family physician is much involved, the team in the multidisciplinary MS Care Unit should keep a close collaboration with the patients’ general practitioner.
In many countries, practicing neurologists are responsible for management of the majority of people with MS. The multidisciplinary MS Care Unit should offer collaboration on second opinion of patients with diagnostic challenges and assist in the treatment of patients with aggressive MS course and of patients not responding to conventional therapies.
The fully developed integrated multidisciplinary MS Care Unit encompasses staff members with many different skills, including occupational therapist, speech therapist, dietician, medical social worker or counsellor, clinical psychologist, laboratory technician and specialists in treatment of spasticity, incontinence and pain, who may be members of the multidisciplinary team, may be MS neurologists or MS nurses, with special expertise or may be external experts collaborating closely with the staff of the MS Care Unit (Figure 2).
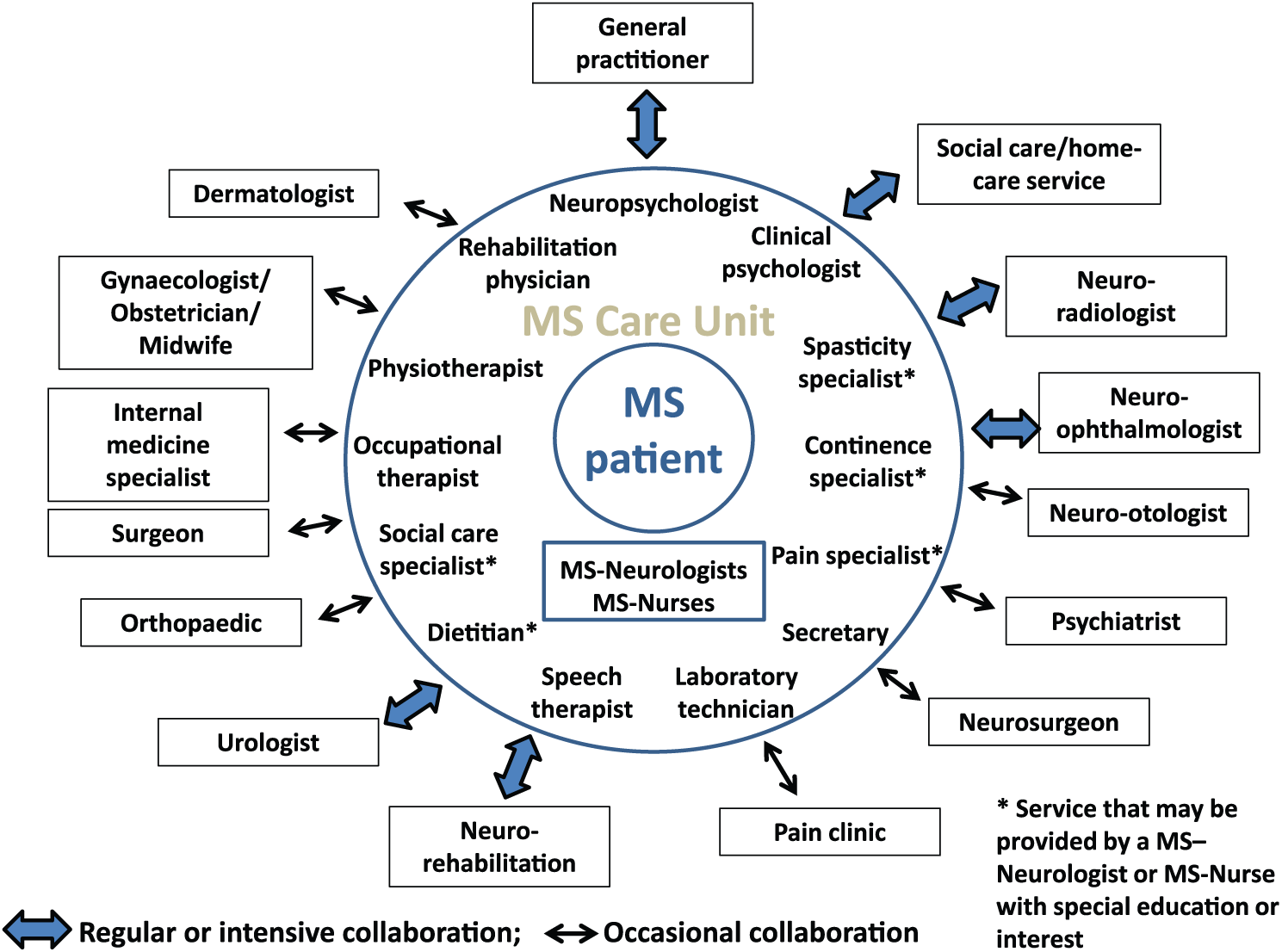
Organization of the fully developed integrated multidisciplinary MS Care Unit.
Some neighbouring specialities are extremely important collaborators such as neuro-radiologists, neuro-ophthalmologists and urologist.
A reliable and expert neuro-radiological service is of paramount importance for the diagnostic workup of patients suspected of MS and for monitoring the disease evolution and response to DMT as well as adverse effects to therapy. Several large multidisciplinary MS Care Units have special MS MRI facilities closely collaborating with or embedded in the unit.
Collaboration with neuro-otologist is important in the treatment of patients with vertigo or balance problems, and neurophysiologists are often responsible for performance of visual, somatosensory and motor-evoked potentials that are a part of the diagnostic workup in some patients.
Psychiatric comorbidities are common in MS patients and also require special care. 26 Every phase of MS can lead to initial denial and later acceptance phases that can be handled appropriately by psychotherapy. Many of these symptoms can be managed by the personal of the MS Care Unit, but in some cases, the choice of antidepressant or initiation of neuroleptics will need discussion with psychiatrists.
Collaboration with other specialities, for example, internal medicine specialists, endocrinologist, rheumatologists, specialists in infectious diseases and cardiologists is necessary, not only to treat complications of the MS disease but also to manage comorbidities.
Spasticity is in generally handled by the neurologists in the MS Care Unit with pharmacological treatment and botulinum toxin injected locally, but when severe spasticity in the legs requires intrathecal baclofen administration, a multidisciplinary approach is needed, including collaboration with neurosurgeons.
Tremor can be one of the most disabling symptoms of MS that in many cases do not respond satisfactorily to pharmacotherapy and, hence, requires either the use of assistive devices or surgical intervention such as deep brain stimulation. The decision for particular therapeutic measures may be reached by a team that includes expert neurologists, neurosurgeon, psychiatrist and psychologist.
For treatment of spasticity complications such as joint contractures, hip dislocations, scoliosis and deformed extremities, collaboration with orthopaedics is required, as well as for treatment of fractures caused by the falls that frequently occurs in disabled MS patients.
Other surgical interventions are required in refractory and more severe cases of bladder dysfunction where enterocystoplasty (Bricker) and urinary diversion become alternative treatment modalities, and in cases of severe swallowing disorders where gastrostomy may be needed.
The fully developed integrated multidisciplinary MS Care Unit will usually be connected to a clinical trial unit and a MS research unit with laboratory facilities.
Patients’ perspective
A multidisciplinary clinical approach that integrates patient-care (diagnosis, treatment and follow-up) and rehabilitation activities (including neuropsychological and social support) would enhance the efficacy of therapy (all aspects including compliance and adherence and not only limited to effectiveness) and provide better patient overall satisfaction. 27 The availability of a specific single contact neurologist and nurse, who can provide information, support and advice to the individual MS patient, is a major advantage over a regular outpatient clinic. Patients may be exposed to a variety of experimental therapies, which may not be available to office-based neurologists.
Accompanying acceptance of the need to integrate patient perspectives is an increase in the demand for research-based methods and tools to measure the effectiveness of incorporating patient input into the MS care models and, ultimately, its impact on patients’ health and quality of life. 28 Given the plethora of functional domains affected in patients with MS, a multidisciplinary care team, such as the one described in this paper, is needed in order to improve MS patients’ quality of life. 29
Rehabilitation is essential in the management of the MS patient during the patient journey along the course of MS. 14 The rehabilitation physician could be included in the core team of the MS Care Unit and be working together in a team with physiotherapist, speech therapist and occupational therapist that could deliver appropriate neurorehabilitation treatment.
Why are multidisciplinary MS Care Units important?
DMT has become increasingly complex and comprises a wide range of drugs with different mechanism of action and adverse effects that need meticulous monitoring.7,8 The establishment of multidisciplinary MS Care Units would facilitate timely and correct treatment and increase the safety for patients treated with DMTs. The use of the entire therapeutic armamentarium seamlessly and correctly requires expert neurologists and MS nurses.
The presence of several MS expert neurologists in the MS Care Unit enables ad hoc real-time conferences about patients presenting with diagnostic or therapeutic challenges.
In almost all countries, there is a shortage of MS neurologists and multidisciplinary MS Care Units offer the possibility of transfer of tasks from neurologists to MS nurses or therapists and thereby release neurologist time to patient contact. NICE has recommended that care for people with MS should comprise a coordinated multidisciplinary approach (NICE 2003). 24 Management of people with MS should involve professionals who can best meet the needs of the person with MS and who have expertise in managing MS including consultant neurologists, MS nurses, physiotherapists and occupational therapists, speech and language therapists, psychologists, dieticians, social care and continence specialists, and general practitioners.
However, it is not realistic that every patient is managed in integrated MS care centres all over Europe, and the approach has to be balanced with clinical practice. Hence, in many countries, although it should be encouraged to treat as many people with MS in MS Care Units, collaboration between the MS Care Units and practicing neurologist needs to be established with the MS Care Unit offering the function as reference centres.
Uygunoglu et al. 30 have reviewed the reasons for promoting integrated multidisciplinary clinics focusing primarily on patients with progressive forms of MS. They concluded that the optimum care for patients with MS requires a multispecialist work force which should include not only expert neurologists but also physical medicine and rehabilitation physicians, physiotherapists, speech therapists, neuro-urologists, psychiatrists and psychologists, sleep medicine specialists, specialist MS nurses, social workers, occupational therapists and optional others.
However, Papeix et al. 31 found in a small randomized controlled trial that an integrated multidisciplinary approach was not superior to usual multidisciplinary care in promoting quality of life as measured by the MS impact scale-29. They suggested that in order to enhance the efficacy and to provide better patient satisfaction, the MS nurse specialist should, as part of their work, be involved in ensuring that the chain of multidisciplinary assessments and interventions is organized systematically and that all patients can access the necessary experts. 32
How should the efficacy of the multidisciplinary MS Care Unit approach be measured?
As the MS Care Unit approach advances, there remains a need to identify, define and capture the return of investment across key stakeholders, such as payers, hospital systems and providers, as well as returns experienced by patients. All stakeholders will look for short-term returns on their investment of money, time and effort in order to maintain the momentum. The MS Care Unit approach will apply a prospective model engaging stakeholders in defining metrics to measure its impact (co-accountability model), rather than using a single performance assessment system (top down accountability approach). Within this frame, in measuring the impact of MS Care Unit, it will be fundamental to consider patients and their needs and perspectives as key stakeholders throughout the entire measurement process. The measures of effects of the establishment of multidisciplinary MS Care Units are given in Table 2.
Measures of effects of the establishment of multidisciplinary MS Care Units.
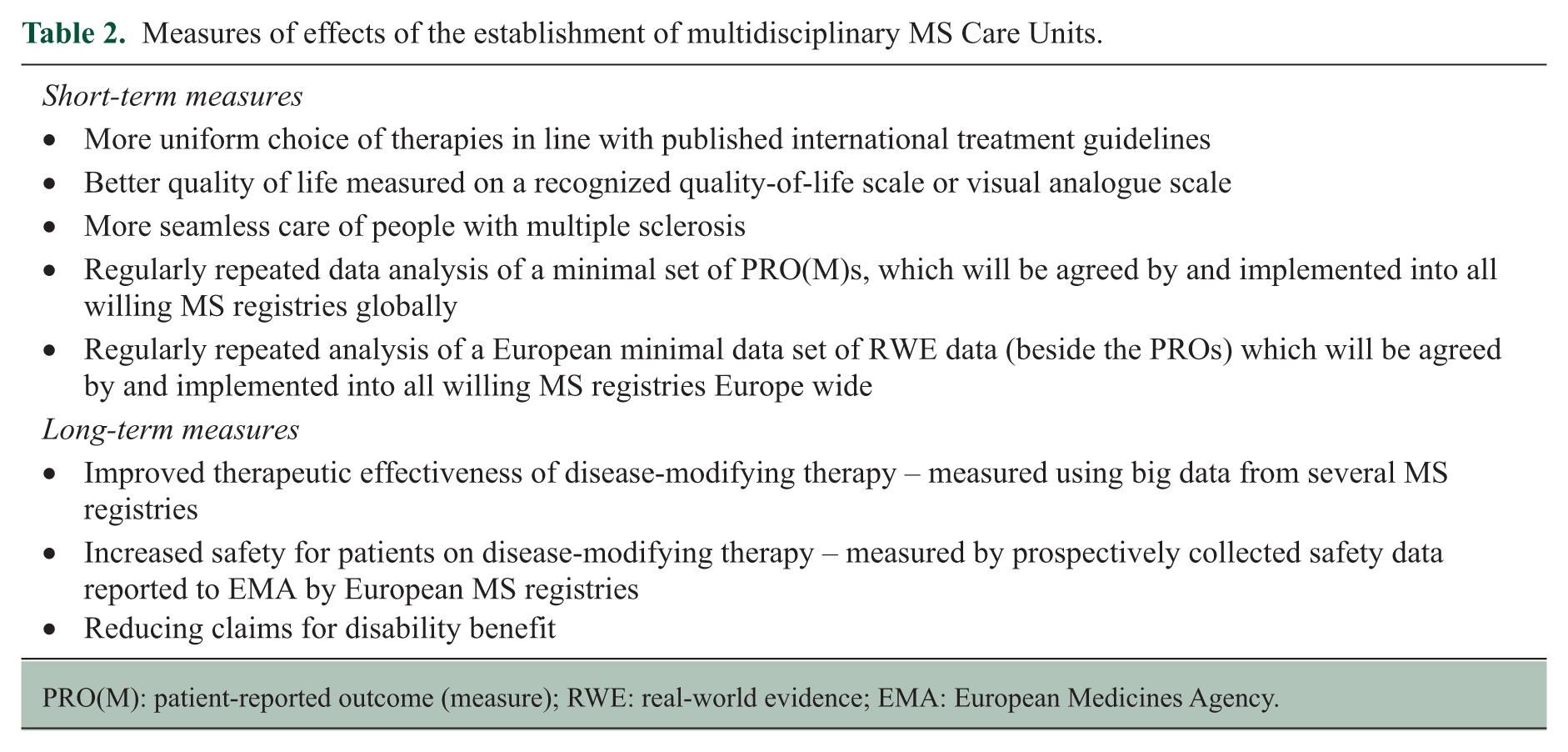
PRO(M): patient-reported outcome (measure); RWE: real-world evidence; EMA: European Medicines Agency.
One of the first successes of the initiative will be the establishment of multidisciplinary MS Care Units in many countries, which could be documented in a survey conducted by the European Charcot Foundation, and for which to develop the relevant co-accountability model to measure the impact on patients and society.
In Denmark, the initiative has resulted in political plans to establish multidisciplinary MS Centres.
It is, however, difficult to provide a universal measure of the efficacy of the multidisciplinary MS Care Unit because of the considerable variations in treatment choices in specific patient situations shown to exist across different countries, 10 but a more uniform choice of treatments according to published international guidelines after establishment of MS Care Units, shown in a similar survey, would confirm beneficial effect.
The ultimate goal of the multidisciplinary MS Care Unit approach is to increase patient satisfaction and quality of life. Hence, a better quality of life measured on a recognized quality-of-life scale or visual analogue scale should indicate a high patient satisfaction.
It is obvious that the terms of performance of different MS Care Units vary across regions and countries. Hence, the criteria that can define the performance of good quality of an MS Care Unit will need to be defined according to local conditions.
Establishment of MS Care Units may even be cost-effective for the society, reducing claims for disability benefit by maintaining the working ability of people with MS and reducing the costs of home help and custodial care by keeping people with MS resourceful. This would, however, due to the diverse course of MS and complexity of management be difficult to document on the short run and will require socio-economic studies with long-term observation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: P.S.S. has received personal compensation for serving on scientific advisory boards, steering committees or independent data monitoring boards for Biogen, Merck, Novartis, TEVA, GlaxoSmithKline, MedDay Pharmaceuticals, Genzyme, Celgene and Forward Pharma and has received speaker honoraria from Biogen, Merck, Teva, Genzyme and Novartis. His department has received research support from Biogen, Merck, TEVA, Novartis, Sanofi-Aventis/Genzyme, RoFAR and Roche. G.G. has received compensation for serving as a consultant or speaker for, or has received research support from AbbVie, Actelion, Atara Bio, Biogen, Canbex, Celgene, Sanofi Genzyme, Genentech, GlaxoSmithKline, Merck-Serono, Novartis, Roche, Synthon BV and Teva. X.M. has received speaking honoraria and travel expenses for participation in scientific meetings, has been a steering committee member of clinical trials or participated in advisory boards of clinical trials in the past years with Actelion, Almirall, Bayer, Biogen, Celgene, Genzyme, Merck, Novartis, Oryzon Genomics, Roche, Sanofi Genzyme and Teva Pharmaceutical. C.T. has, in his capacity as consultant for EU health affairs, received consultancy fees by Gruenenthal and by PharmaGenesis. In his capacity as Director External Affairs of the European MS Platform, he served in advisory boards and/or workshops by Biogen, Merck, Novartis, Sanofi Genzyme, Servier and Takeda. His employer, the European MS Platform, has received unrestricted project grants from Actelion, Almirall, Bayer, Biogen, icometrix, MedDay, Merck, Mylan, Novartis, Roche, Sanofi Genzyme, SCA, Servier, Synthon, Terumo and Teva. P.Z. has no conflict of interest to declare. G.C. has received personal compensation, outside this work, for participating in scientific advisory boards and for speaking activities from Novartis, Teva, Sanofi Genzyme, Biogen, Roche, Almirall, Celgene, Forward Pharma, MedDay and Excemed.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.