
Abstract
Background:
Early initiation of high-efficacy therapies (HETs) has been associated with improved disease control in pediatric-onset multiple sclerosis (POMS). However, some children remain clinically stable on low-/moderate-efficacy therapies (METs), highlighting the need for decision-support tools.
Objective:
To develop a Therapeutic Escalation Score (TES) to identify children at low risk of early escalation after initiating MET.
Methods:
We analyzed treatment-naïve children with POMS who initiated MET between 2010 and 2024 in the French MS registry (Observatoire Français de la Sclérose en Plaques (OFSEP)). TES was derived using Cox regression modeling based on baseline clinical and magnetic resonance imaging (MRI) variables, with internal validation in OFSEP and external validation in the Italian MS registry Registro Italiano Sclerosi Multipla (RISM).
Results:
We included 455 children from OFSEP (training n = 303; validation n = 152) and 573 from RISM. TES incorporated age, year of treatment initiation, Expanded Disability Status Scale score, prior-year relapses, brain lesion location, and T2 spinal cord lesions. A TES threshold of 1.34 stratified patients by 1-year escalation risk. In OFSEP, low-risk patients had a 1-year escalation probability of 3.6% (negative predictive value: 97.0%). In RISM, discrimination was similar (area under the curve (AUC): 72.8%–73.8%).
Conclusion:
TES is a baseline-only prognostic tool using routine clinical and MRI data to identify children with POMS unlikely to require early escalation after MET initiation.
Keywords
Introduction
Pediatric-onset multiple sclerosis (POMS) requires early and effective therapeutic intervention to reduce long-term disability and prevent treatment failure. A common approach follows a stepwise escalation strategy, initiating low/moderate-efficacy therapy (METs) and intensifying to high-efficacy therapy (HET) in case of breakthrough disease.1,2 However, recent evidence suggests that early initiation of HET may provide superior disease control and better long-term outcomes.3–10
However, some MET-treated patients remain clinically stable (30%–60% across studies), whereas HET carries higher infection risks and uncertain long-term safety in children.3,11–13 In addition, there are no standardized strategies for treatment de-escalation once disease control is achieved. In this context of heterogeneous real-world practice, identifying at treatment initiation children unlikely to require early escalation remains an unmet need.
Several predictive scores to assess MS progression, disease activity, or treatment response during follow-up have been developed in adult patients, but they were not intended to guide initial treatment decisions and are not tailored to POMS.14–17
Given these gaps, we aim to develop a predictive composite score for therapeutic escalation in POMS using two large observational cohorts, the French and Italian registries for MS (Observatoire Français de la Sclérose en Plaques (OFSEP) and RISM). By integrating clinical, radiological, and demographic variables, this tool aims to identify children at low short-term risk of escalation among children initiating MET.
Materials and methods
Study design
This observational cohort study was based on data from 120 Italian and 44 French expert centers participating in the Italian MS register (RISM) and the French MS database called OFSEP (www.ofsep.org).18,19 Regarding the latter, for each patient, clinical and imaging data were collected during routine follow-up visits, usually once a year, using a dedicated software, the European Database on Multiple Sclerosis “EDMUS,” by a neurologist with a particular interest in MS. 20 These data were collected retrospectively at the time of the first visit and prospectively thereafter.
Patients enrolled in the OFSEP study (NCT02889965) and the RISM provided written informed consent for participation. The OFSEP cohort received regulatory approvals (CNIL 914066v3 and ethics committee; CPP 2019-A6-51.T), and the study complied with MR-004 requirements. This study followed the TRIPOD + AI reporting guidelines.
Patients
Patients with POMS were eligible for inclusion if they received a first MET before the age of 18 from 1 January 2010 to 8 June 2024 and were diagnosed with clinically definite relapsing–remitting MS at treatment initiation. Eligible MET included the following: azathioprine, dimethyl fumarate, glatiramer acetate, interferon beta, methotrexate, mycophenolate mofetil, and teriflunomide. Given international heterogeneity in drug classification, therapies were grouped pragmatically as MET versus HET, consistent with prior registry-based studies. 3
Procedure
Follow-up started at the date of MET initiation and ended at the first occurrence of therapeutic escalation to a HET for inefficacy, last clinical visit, or permanent discontinuation of MET without subsequent HET. Temporary treatment gaps ⩽90 days were considered continuous exposure. Discontinuations followed by HET initiation within 12 months were classified as escalation events, whereas switches for non-inefficacy reasons or HET initiation beyond 12 months were censored at the date of discontinuation (Supplemental Methods).
Outcomes
The primary outcome was MET escalation due to insufficient efficacy in controlling MS activity. Escalation was defined as initiation of a HET (alemtuzumab, fingolimod, mitoxantrone, cladribine, natalizumab, ocrelizumab, ofatumumab, or rituximab) following initial exposure to a MET. Escalation had to occur within 12 months of MET discontinuation and be prompted by either a relapse within the preceding 12 months or inefficacy explicitly reported by an MS specialist. Escalation due to insufficient efficacy reflected a multidisciplinary clinical judgment integrating relapses, MRI activity, and overall disease course, as documented in the registry, based on internationally recognized criteria such as those outlined in the European Committee for Treatments and Research In Multiple Sclerosis/European Academy of Neurology (ECTRIMS/EAN) and American Academy of Neurology guidelines.21,22
In secondary analyses, the outcome was defined as therapeutic escalation to HET for any reason and assessed using the same modeling and validation strategy as for the primary outcome (Supplemental Methods).
Prediction horizons of 1, 3, and 5 years were defined a priori according to their clinical relevance for assessing early treatment escalation in POMS. The 1-year horizon was chosen as the primary evaluation period, as it corresponds to the most informative interval for early therapeutic decision-making. Longer horizons (3 and 5 years) were analyzed secondarily to evaluate the temporal stability of predictive performance.
Statistical analyses
The included OFSEP population was randomly split into a training data set (2/3) and an internal validation data set (1/3). The Italian Multiple Sclerosis Register (RISM) served as an external validation data set.
We developed a clinical composite score, the Therapeutic Escalation Score (TES), in the training set. The TES considers clinical, radiological, and demographic variables (Supplemental Methods). Candidate predictors were selected based on clinical relevance and prior literature. Predictors were first screened using univariate Cox models (p < 0.20) and subsequently entered into a multivariable model optimized using the Akaike information criterion to ensure model parsimony. The score was derived using a conventional multivariate Cox model combined with the time-dependent receiver-operating characteristic (ROC) curves, making it possible to assess its predictive ability (Supplemental Methods).
In a first step, missing MRI and Expanded Disability Status Scale (EDSS) data were handled using a multiple imputation approach by chained equations. The 20 imputed data sets generated were analyzed separately and then pooled using Rubin’s rules.
Once the TES was constructed in the training set, the optimal threshold for dichotomizing the score into two groups, patients at high risk versus low risk of MET escalation, was determined by using time-dependent ROC curves and by maximizing the Youden index (sensitivity + specificity—1). Performance metrics of the score at 1 and 3 years, including sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), area under the curve (AUC), and calibration, were then estimated. Model optimization and sensitivity analyses are detailed in the Supplemental Methods.
Finally, we applied the TES threshold value to the validation data sets to confirm the performance of TES. Because brain lesion location was not available in the RISM registry, external validation was performed under several plausible assumptions regarding the distribution of this predictor. Four scenarios were explored to assess the robustness of the model to this missing variable:
Scenario 1: All patients assigned supratentorial + infratentorial lesions.
Scenario 2: All patients assigned either supratentorial or infratentorial lesions.
Scenario 3: About 50% of patients were randomly assigned both lesion types.
Scenario 4: About 70% of patients were randomly assigned both lesion types, consistent with the distribution observed in the OFSEP data set.
The statistical analyses were conducted using Altair SLC 2024 software for descriptive analyses and R software version 4.2.2 with the survPen and timeROC packages for modeling.
Data availability
Anonymized data will be made available for researchers whose proposed use of the data has been approved by the corresponding author, both the OFSEP and RISM scientific committee, and both the OFSEP and RISM steering committee.
The link to use the TES calculator is as follows: https://www.ofsep.org/TES_calculator.html
Results
Characteristics of the training and validation sets
From 4002 and 5770 children with POMS in the OFSEP and RISM databases, respectively, 455 and 573 met the inclusion criteria. The OFSEP cohort was split into a training set (n = 303) and an internal validation set (n = 152) (Figure 1). Baseline characteristics were broadly comparable across data sets, with slightly higher EDSS and lower relapse and MRI activity in RISM (Table 1; Supplemental Table 1).
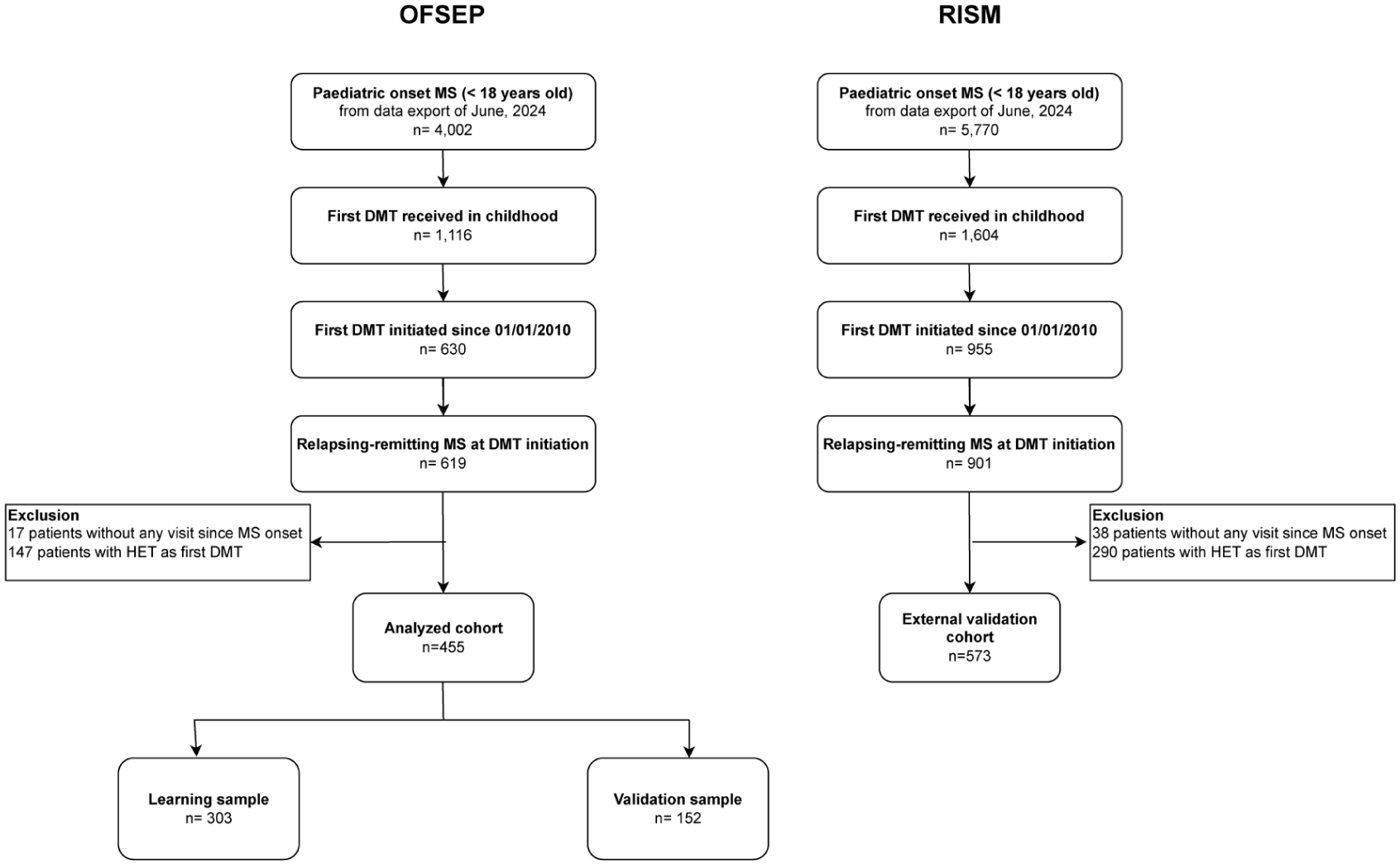
Study flow diagram.
Demographics and clinical features.

Statistical comparisons were performed using the chi-square test for categorical variables and the Mann–Whitney U test for continuous variables. Continuous MET exposure was defined as the absence of treatment discontinuation for 90 days or more. EDSS = Expanded Disability Status Scale; HET = high-efficacy treatment; MET = moderate-efficacy therapy; NA = not available; SAE = serious adverse event; SD = standard deviation. Continuous MET exposure was defined as the absence of treatment discontinuation for 90 days or more.
First-line therapies were predominantly injectable or oral MET. Median follow-up was 7.8 years [4.4–10.6] (Supplemental Table 1). Overall, 254 (83.8%) on MET discontinued their first treatment, mostly due to breakthrough disease (144 patients; 56.7%). Among switchers to HET due to insufficient efficacy (n = 158, 52.1%), 47.5% escalated to natalizumab (n = 75) and 41.1% to fingolimod (n = 65) after a MET exposure of 1.5 years [0.8–3.6]. The preferred type of HET for escalation due to insufficient efficacy had shifted from natalizumab to anti-CD20 therapies from 2018 in both the OFSEP and RISM cohorts (Supplemental Table 2).
Therapeutic Escalation Score (TES)
After applying the multiple imputation method and a multivariate analysis of MET escalation due to inefficacy, six factors were retained, including age, EDSS, year of MET initiation, number of relapses, brain lesion location, and number of spinal cord lesions (Supplemental Figures 1–8 and Supplemental Tables 3–5). The TES is defined by the following formula

The definition of the factors and the complete result of the Cox model are provided in Supplemental Tables 3–5. The distribution of TES is shown in Supplemental Figure 8. When the log-hazard ratio (logHR) is positive, the TES increases with the value of this risk factor (Table 2). For instance, the TES increases with the number of relapses, the EDSS, and the number of T2 spinal cord lesions. More accurately, a one-unit increase in the TES is associated with a 3.5-fold higher risk of the treatment escalation due to insufficient efficacy (p < 0.001). This relationship is illustrated in Figure 2(a) using TES deciles (Supplemental Table 5). Half of the patients had a TES > 1.13, while only 28 patients had a TES < 0, indicating a reduced risk of switching due to insufficient efficacy. Patients in the second decile (TES between 0.03 and 0.42) have a 3.82-fold increased risk of switching to HET due to insufficient efficacy.
Final multivariable Cox model and corresponding coefficients used to derive the TES.

Coefficients correspond to log-hazard ratio (logHR) from the final multivariable Cox model, estimated after multiple imputation and pooled using Rubin’s rules. For TES calculation, each retained predictor is coded as a binary indicator (0/1) and multiplied by its corresponding log-hazard ratio, except for year of MET initiation, which is entered as a centered continuous variable (year of initiation—2014). Positive coefficients indicate an increased risk of treatment escalation due to insufficient efficacy. Reference categories are age <16 years, EDSS: 0.0, no relapse in the previous year, brain lesion location other than combined supratentorial and infratentorial involvement, and no spinal cord lesion. HR = hazard ratio; METs = moderate-efficacy therapies; TES = Therapeutic Escalation Score.
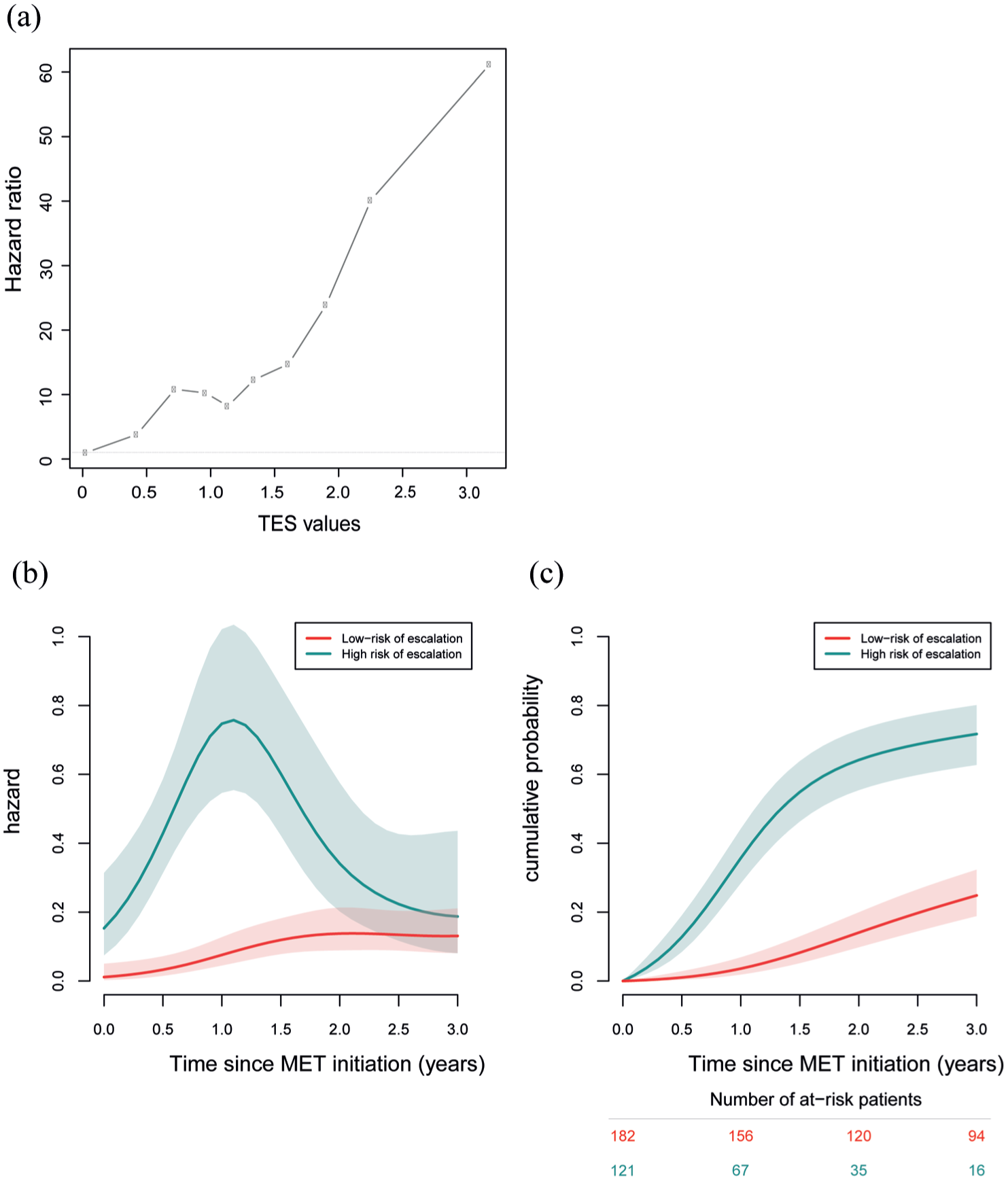
Evolution of the risk of switching from initial MET to HET according to the TES in the OFSEP training set. (a) Hazard ratios for treatment escalation are shown according to TES deciles, with the first decile serving as the reference category. (b) Dynamics and (c) cumulative probabilities of treatment escalation due to MET inefficacy are presented according to TES risk groups, using a threshold of 1.34.
Predictive performances of the TES in the training set
As the TES is a quantitative variable, it is essential to identify subgroups according to their risk of escalation. AUC values from the time-dependent ROC curve demonstrate the good discriminative performance of the TES throughout follow-up at 1 and 3 years, with the highest predictive power observed early after MET initiation (AUC: 85.9%; 95% CI: 80.0–90.9; Supplemental Table 6). The optimal TES threshold that corresponds to the maximum value of sensitivity (89.5%) and specificity (70.0%) was determined at 1.34 (PPV = 37.9% and NPV = 97.0%; Supplemental Table 7).
Thus, two risk groups were defined: a low-risk group of escalation to HET (TES < 1.34), accounting for 182 patients, including 72 who switched, and a high-risk group (TES ⩾ 1.34), accounting for 121 patients, including 86 who switched. Baseline clinical and MRI characteristics according to the TES threshold are presented in Supplemental Table 8. Compared with the low-risk group, patients with TES ⩾ 1.34 were younger, initiated MET earlier after diagnosis, had more frequent relapses in the preceding year, and showed a higher proportion of infratentorial involvement, consistent with the predictors contributing to the score. In the high-risk group, the risk of treatment escalation markedly increased up to 1 year and then decreased thereafter, whereas in the low-risk group, it remained generally constant over time with a slight increase from 1 year. At 1 year, the MET escalation rate was estimated at around 75 switches per 100 person-years in the high-risk group and 8 switches per 100 person-years in the low-risk group, corresponding to an annual probability of MET escalation approximating 53% (1
Internal validation of the TES
The predictive performance of the TES was then evaluated in the internal validation set, which included 152 children from the OFSEP registry. At 1 year, the TES demonstrated an AUC of 69.1% [95% CI: 49.4–88.83] with a sensitivity of 59.6% and a specificity of 65.6% (Supplemental Tables 13 and 14). The metric calibration was estimated by the mean error between predicted and observed probabilities and was 0.088. Figure 3(a) shows that the threshold of 1.34 discriminated between the two groups according to MET escalation. The cumulative probability of therapeutic escalation to HET due to inefficacy was 4.7% (95% CI: 0.1–9.0) at 1 year and 24.6% (95% CI: 13.9–34.0) at 3 years in the low-risk group, compared with 11.7% (95% CI: 2.4–20.1) at 1 year and 51.8% (95% CI: 32.3–65.6) at 3 years in the high-risk group (p = 0.005).
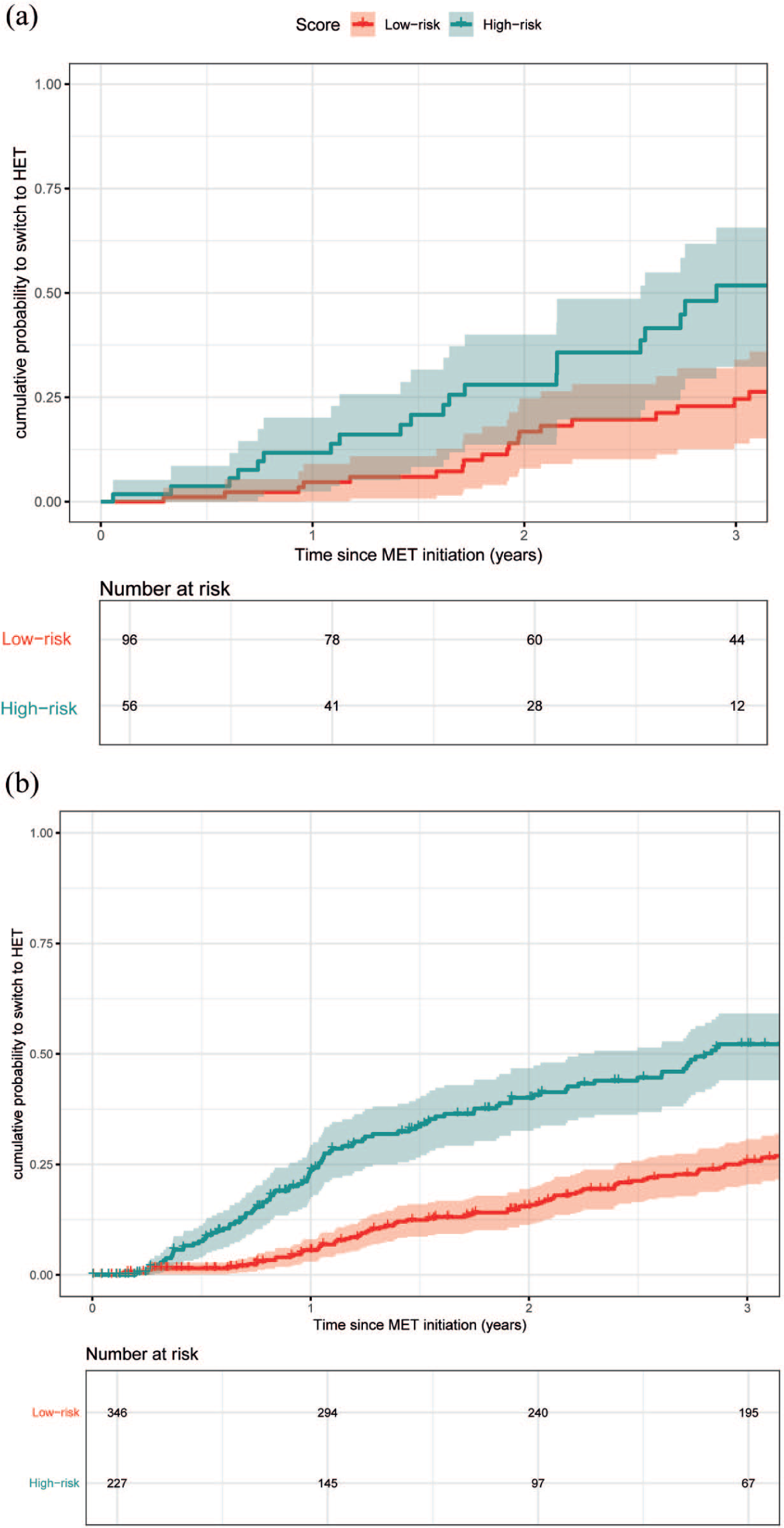
Evolution of the risk of switching from initial MET to HET according to the Therapeutic Escalation Score (TES) in the OFSEP and RISM validation sets. Kaplan–Meier curves showing the cumulative probability of treatment escalation due to MET inefficacy in (a) the OFSEP validation set (p < 0.01) and (b) the RISM validation set (illustrative of Scenario 4; p < 0.0001), stratified by TES-based risk groups using a threshold of 1.34.
External evaluation of the TES in the independent RISM cohort
The model was externally evaluated in the RISM cohort under assumptions for a missing predictor, as brain lesion location was not available in this data set. Four scenarios were explored to estimate this variable (Supplemental Table 15). Across all scenarios, the TES maintained a predictive accuracy with AUCs between 72.8 [95% CI: 66.7–78.9] and 73.8% [95% CI: 67.9–79.8] at 1-year post-MET initiation with a sensitivity ranging from 48.4% to 77.3% and a specificity ranging from 62.2% to 81.1% (NPV: 91.6%–95.0% and PPV: 22.7%–26.9%; Supplemental Table 15; Supplemental Figures 13–16). The mean error between predicted and observed probabilities ranged from 0.068 to 0.080 depending on scenarios. Predictive performance remained consistent across the different scenarios explored, suggesting that model discrimination was robust despite this missing predictor. Scenario 4 is illustrated in Figure 3 because it reproduces the distribution of brain lesion locations observed in the OFSEP training set and, therefore, represents the most plausible scenario for comparison. In the low-risk group, the cumulative probabilities of escalating to HET due to inefficacy ranged from 5.0% (95% CI: 2.5–7.5) to 8.4% (95% CI: 5.7–11.1). Conversely, in the high-risk group, the cumulative probabilities of MET escalation ranged from 22.4 (95% CI: 16.8–27.7) to 26.6% (95% CI: 18.2–34.1) (Table 3; Figure 3(b); Supplemental Figures 13–16). Three years after MET initiation, 51.3%–59.5% patients in the RISM cohort with a TES ⩾ 1.34 had escalated to HET due to inefficacy, while 71.2%–75.7% had not escalated to HET in patients with TES < 1.34 (Tables 3 and 4; Supplemental Tables 13–15; Supplemental Figures 13–16). These findings support the use of TES primarily to exclude early escalation rather than to predict escalation with high certainty.
Probability of treatment escalation due to MET lack of efficacy by the TES-defined risk group across all cohorts.

Patients were assigned to low-risk and high-risk groups, defined by a TES < 1.34 and ⩾1.34, respectively.
Summary of predictive accuracy of TES across cohorts.

AUC = Area under the receiver-operating characteristic curve; NPV = negative predictive value; PPV = predictive positive value.
Discussion
TES is a clinically applicable tool based on six baseline parameters available at treatment initiation. Developed to identify children unlikely to require early escalation after initiating MET, TES is a prognostic, not causal, model estimating the risk of escalation for POMS patients starting on MET as the initial therapy. 23 A central point is that TES addresses early escalation risk after initiating MET and does not aim to predict long-term disability, cognitive outcomes, or progression independent of relapse activity (PIRA). TES should, therefore, be interpreted as a prognostic model describing real-world early treatment trajectories rather than a tool to guide treatment decisions, and its potential clinical utility requires prospective validation.
At 1 year, TES showed an AUC of 69% in OFSEP and 73% in RISM, based on established predictors of early disease activity.5,6
To enable practical interpretation of the score in future validation studies, TES was operationalized with a dichotomous risk threshold (1.34), derived via time-dependent ROC curve analysis. Its predictive accuracy peaked during the first year of follow-up, likely due to recommended MRI monitoring practices in the first year, which may have led to treatment modifications in children. 24 A patient with a TES < 1.34 has a low probability of escalating to HET within the first year, corresponding to a NPV of 97.1% in the training cohort. Conversely, a patient with a TES ⩾ 1.34 has a 38.3% risk of escalation within the same period. Our findings are supported by the inclusion of an independent internal validation set and an external validation cohort (RISM), which replicated results despite some differences with the OFSEP training set, such as higher EDSS and a lower MRI and clinical activity in RISM. This confirms the generalizability of TES across independent data sets. Because the outcome is treatment escalation due to insufficient efficacy, TES may partly reflect clinical decision-making and should be interpreted as a prognostic model of real-world treatment trajectories rather than intrinsic disease aggressiveness.
TES reflects control of early inflammatory activity (relapses and MRI lesions), which are key short-term drivers in POMS, where disability progression is typically slower.10,25 TES, thus, may help frame future research on individualized treatment stratification in POMS based on these acute-phase parameters.
As expected for a baseline-only model, predictive performance declined over time, possibly reflecting that early escalation is driven by inflammatory activity rather than long-term progression.4,10
However, it should support, but not replace, clinical judgment. It does not account for other factors that influence treatment, such as safety, comorbidities, treatment accessibility, patient tolerance, or patient and family preferences. Therefore, decisions must remain shared between clinicians, children/adolescents, and their families.26,27
Several limitations should be acknowledged. Selected MRI variables required imputation in OFSEP, and lesion location was unavailable in RISM, requiring scenario-based analyses. Accordingly, the external evaluation relied on assumptions for a missing predictor. Although predictive performance remained consistent across scenarios, this should be interpreted as validation under assumptions rather than full replication of the original model specification. Younger children were under-represented. As with any prognostic model, recalibration may be required in other settings, including evolving therapeutic strategies or biomarker availability.
Prospective studies will be necessary to determine whether TES can support individualized treatment strategies in clinical practice.
Conclusion
TES is a baseline-only prognostic tool for early escalation risk after MET initiation in POMS. It may pave the way for future clinical translation pending prospective validation. It may inform risk discussions when considering MET initiation by identifying patients with a low probability of early escalation (rule-out strategy). It does not replace clinical judgment, nor does it imply that delaying HET is safe or equivalent to early initiation when clinically indicated. Further validation, including biomarker integration, is needed to refine its clinical utility within its scope as a short-term, inflammation-driven prognostic model.
Supplemental Material
sj-docx-2-msj-10.1177_13524585261446829 – Supplemental material for A predictive tool for early treatment escalation after initiation of moderate-efficacy therapy in pediatric-onset multiple sclerosis
Supplemental material, sj-docx-2-msj-10.1177_13524585261446829 for A predictive tool for early treatment escalation after initiation of moderate-efficacy therapy in pediatric-onset multiple sclerosis by Nail Benallegue, Fabien Rollot, Pietro Iaffaldano, Giuseppe Lucisano, Marta Simone, Alessandra Lugaresi, Romain Casey, Eleonora Cocco, Sandra Vukusic, Giovanna De Luca, Guillaume Mathey, Francesco Patti, Elisabeth Maillart, Maria Pia Amato, Laure Michel, Roberta Fantozzi, Jonathan Ciron, Francesca De Robertis, Jérôme De Sèze, Maria Gabriella Coniglio, Aurélie Ruet, Massimo Filippi, Pierre Labauge, Sebastiano Giuseppe Crisafulli, Helene Zephir, Diana Ferraro, Caroline Papeix, Christine Lebrun-Frenay, Maria Trojano and David Axel Laplaud in Multiple Sclerosis Journal
Supplemental Material
sj-html-4-msj-10.1177_13524585261446829 – Supplemental material for A predictive tool for early treatment escalation after initiation of moderate-efficacy therapy in pediatric-onset multiple sclerosis
Supplemental material, sj-html-4-msj-10.1177_13524585261446829 for A predictive tool for early treatment escalation after initiation of moderate-efficacy therapy in pediatric-onset multiple sclerosis by Nail Benallegue, Fabien Rollot, Pietro Iaffaldano, Giuseppe Lucisano, Marta Simone, Alessandra Lugaresi, Romain Casey, Eleonora Cocco, Sandra Vukusic, Giovanna De Luca, Guillaume Mathey, Francesco Patti, Elisabeth Maillart, Maria Pia Amato, Laure Michel, Roberta Fantozzi, Jonathan Ciron, Francesca De Robertis, Jérôme De Sèze, Maria Gabriella Coniglio, Aurélie Ruet, Massimo Filippi, Pierre Labauge, Sebastiano Giuseppe Crisafulli, Helene Zephir, Diana Ferraro, Caroline Papeix, Christine Lebrun-Frenay, Maria Trojano and David Axel Laplaud in Multiple Sclerosis Journal
Supplemental Material
sj-pdf-1-msj-10.1177_13524585261446829 – Supplemental material for A predictive tool for early treatment escalation after initiation of moderate-efficacy therapy in pediatric-onset multiple sclerosis
Supplemental material, sj-pdf-1-msj-10.1177_13524585261446829 for A predictive tool for early treatment escalation after initiation of moderate-efficacy therapy in pediatric-onset multiple sclerosis by Nail Benallegue, Fabien Rollot, Pietro Iaffaldano, Giuseppe Lucisano, Marta Simone, Alessandra Lugaresi, Romain Casey, Eleonora Cocco, Sandra Vukusic, Giovanna De Luca, Guillaume Mathey, Francesco Patti, Elisabeth Maillart, Maria Pia Amato, Laure Michel, Roberta Fantozzi, Jonathan Ciron, Francesca De Robertis, Jérôme De Sèze, Maria Gabriella Coniglio, Aurélie Ruet, Massimo Filippi, Pierre Labauge, Sebastiano Giuseppe Crisafulli, Helene Zephir, Diana Ferraro, Caroline Papeix, Christine Lebrun-Frenay, Maria Trojano and David Axel Laplaud in Multiple Sclerosis Journal
Supplemental Material
sj-xlsx-3-msj-10.1177_13524585261446829 – Supplemental material for A predictive tool for early treatment escalation after initiation of moderate-efficacy therapy in pediatric-onset multiple sclerosis
Supplemental material, sj-xlsx-3-msj-10.1177_13524585261446829 for A predictive tool for early treatment escalation after initiation of moderate-efficacy therapy in pediatric-onset multiple sclerosis by Nail Benallegue, Fabien Rollot, Pietro Iaffaldano, Giuseppe Lucisano, Marta Simone, Alessandra Lugaresi, Romain Casey, Eleonora Cocco, Sandra Vukusic, Giovanna De Luca, Guillaume Mathey, Francesco Patti, Elisabeth Maillart, Maria Pia Amato, Laure Michel, Roberta Fantozzi, Jonathan Ciron, Francesca De Robertis, Jérôme De Sèze, Maria Gabriella Coniglio, Aurélie Ruet, Massimo Filippi, Pierre Labauge, Sebastiano Giuseppe Crisafulli, Helene Zephir, Diana Ferraro, Caroline Papeix, Christine Lebrun-Frenay, Maria Trojano and David Axel Laplaud in Multiple Sclerosis Journal
Footnotes
Acknowledgements
The authors thank the RISM Research Assistants Network: Beatrice Biolzi, Camilla Borgo, Antonella Carta, Paola Crida, Daniele Dell’Anna, Marco Delogu, Daniele Di Giulio Cesare, Sonia di Lemme, Chiara Di Tillio, Teresa Fonsdituri, Ilaria Maietta, Agata Marchese, Martina Marciano, Silvia Marinetto, Federica Martini, Chiara Monetti, Cristiana Morano, Ornella Moreggia, Silvia Perugini, Giovanna Ramona Piredda, Chiara Raimondi, Antonino Rallo, Monica Romoli, Ilaria Rossi, Valentina Tallarico, Stefania Treccarichi, and Eliana Zaccone.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: B.N. reports conference travel support and/or speaker honoraria from Biogen and Roche. F.R. reports no disclosures. P.I. has served on scientific advisory boards for Biogen Idec, Bayer, Teva, Roche, Merck Serono, Novartis, and Genzyme, and has received funding for travel and/or speaker honoraria from Sanofi Aventis, Genzyme, Biogen Idec, Teva, Merck Serono, and Novartis. G.L. has no conflict of interest to disclose. M.S. has no conflict of interest to disclose. A.L. reported receiving personal fees from Biogen, Bristol-Myers Squibb, Alexion, Merck Serono, Novartis, and Sanofi-Genzyme and grants from Novartis and Sanofi/Genzyme. R.C. reports no disclosures. E.C. has served on scientific advisory boards for Biogen, BMS, Aldmirall, and Merck and received speaker honoraria from Merck, Novartis, Biogen, Roche, Jannsen, and Alexion. S.V. received grants and research support from Biogen, Novartis, Merck Serono, F. Hoffmann-La Roche Ltd., and Sanofi-Genzyme; consulting fees from F. Hoffmann-La Roche Ltd., Biogen, BMS-Celgene, Janssen, Novartis, Merck Serono, Sanofi-Genzyme, and Teva; and payment/honoraria for lectures, speaking, etc., from F. Hoffmann-La Roche Ltd., Biogen, BMS-Celgene, Novartis, Merck Serono, Sanofi- Genzyme, and Teva. G.D.L. has no conflict of interest to disclose. G.M. had travel/accommodations/meeting expenses funded by Biogen, Novartis, Sanofi-Genzyme, Merck, Teva, and Roche; had contracts for lectures or boards with Biogen, Sanofi-Genzyme, Alexion, Roche, Merck, and Novartis without compensation/honoraria. He participates in clinical trials by Biogen, Actelion, Roche, Merck, Sanofi-Genzyme, and Novartis without compensation/honoraria. F.P. received personal compensation for serving on advisory boards by Almirall, Alexion, Biogen, BMS, Janssen, Merck, Novartis, and Roche, and research grants from Alexion, Almirall, Biogen, BMS, Merck, Novartis, Roche, Fondazione Italiana Sclerosi Multipla, Reload Association (Onlus), Italian Health Minister, and University of Catania. E.M. reports research support from Biogen and ARSEP foundation and personal fees for lectures and advisory boards from Biogen, Janssen, Merck, Novartis, Roche, Sanofi, and Teva M.P.A. served on scientific advisory boards for and has received speaker honoraria and research support from Biogen Idec, Merck Serono, Bayer Schering Pharma, Novartis, Roche, BMS-Celgene, and Sanofi Aventis, and is Editor of Multiple Sclerosis Journal. L.M. reports personal fees for lectures and advisory boards from Biogen, Janssen, Merck, Novartis, Roche, Sanofi, and Teva. R.F. has no conflict of interest to disclose. J.C. received consulting, serving on a scientific advisory board, speaking, or other activities with Biogen, Novartis, Merck, Sanofi-Genzyme, Roche, Alexion, and Horizon Therapeutics. F.D.R. has no conflict of interest to disclose. J.D.S. received consulting and lecturing fees, travel grants, and unconditional research support from Biogen, Genzyme, Novartis, Roche, Sanofi Aventis, and Teva Pharma. M.G.C. has no conflict of interest to disclose. A.R. received personal compensation for travel or received speaker honoraria from Biogen, Alexion, Novartis, Sanofi, Horizon Therapeutic, and Merck, and research support to the institution from Biogen, BMS, Sanofi, Roche, and Merck. M.F. reported receiving personal fees from Alexion, Almirall, Biogen, Merck, Novartis, Roche, Sanofi, Bayer, Biogen, Celgene, Chiesi Italia SpA, Eli Lilly, Genzyme, Janssen, Merck Serono, Neopharmed Gentili, Novartis, Novo Nordisk, Roche, Takeda, Teva, Alexion, Biogen, Bristol-Myers Squibb, Merck, Novartis, Sanofi, Sanofi Aventis, and Sanofi-Genzyme and grants from Biogen Idec, Merck Serono, Novartis, and Roche. P.L. received consulting and lecturing fees, travel grants, and unconditional research support from Biogen, Genzyme, Novartis, Merck Serono, Roche, and Teva Pharma. S.G.C. received support for congress participation from Mylan, Merck Serono, and Novartis and has served as an advisory board member for Novartis. H.Z. received consulting or lectures, and invitations for national and international congresses from Biogen, Merck, Teva, Sanofi-Genzyme, Novartis, and Bayer, as well as research support from Teva and Roche, and academic research grants from Académie de Médecine, LFSEP, FHU Imminent, and ARSEP foundation. D.F. has received travel grants and or honoraria for speaking or advisory boards from Binding Site, Biogen, Bristol-Myers-Quibb, Celgene, Merck, Novartis, Roche, and Sanofi. C.P. reports no disclosures. C.L.-F. reports no disclosures. M.T. has served on scientific advisory boards for Biogen, Novartis, Roche, Merck, and Sandoz; has received speaker honoraria from Biogen, Roche, Sanofi, Merck, Alexion, Sandoz, and Novartis. D.A.L. served on scientific advisory boards for Alexion, BMS, Roche, Sanofi, Novartis, Merck, Janssen, and Biogen, received conference travel support and/or speaker honoraria from Alexion, Novartis, Biogen, Roche, Sanofi, BMS, and Merck and received research support from Fondation ARSEP, Fondation EDMUS, and Agence Nationale de la Recherche.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data collection has been supported by a grant provided by the French State and handled by the “Agence Nationale de la Recherche,” within the framework of the “France 2030” program, under the reference ANR-10-COHO-002, Observatoire Français de la Sclérose en Plaques (OFSEP) and by the Eugène Devic EDMUS Foundation against multiple sclerosis. The authors thank the patients and neurologists who participate in the OFSEP project by contributing and facilitating access to clinical data, as well as the research assistants in all OFSEP participating centers who contributed to the data collection.
ORCID iDs
AI disclosure statement
During the preparation of this manuscript, the authors used ChatGPT-5 solely for refining the writing and correcting English grammar and syntax errors. The AI tool was not used to generate any scientific content, analyze or interpret data, or conduct literature searches. All scientific ideas, data, analyses, and conclusions presented in this manuscript are the sole work of the authors. After utilizing the tool for language refinement, the authors carefully reviewed and edited the text as needed and take full responsibility for the accuracy and integrity of the final manuscript.
Data availability
Anonymized data will be made available for researchers whose proposed use of the data has been approved by the corresponding author, both the OFSEP and RISM scientific committee, and both the OFSEP and RISM steering committee.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.