
Abstract
Objectives:
To assess loss of employment, work hours, and wages of people with aquaporin-4 antibody-positive or double-seronegative/antibody status unknown neuromyelitis optica spectrum disorder (NMOSD) internationally.
Methods:
An investigator-designed survey was administered to adults ages 18–70 years with NMOSD and distributed by neurologists in 23 countries, July 2022 to September 2023.
Results:
There were 897 participants (635 aquaporin-4 antibody positive, 262 double-seronegative/untested; 81.4% female, average age 42.5 years, average disease duration 7.6 years, median 2 disease attacks since diagnosis). NMOSD impact was visual loss (34.0% unilateral; 28.2% bilateral), 61.8% with spinal cord disease, 55.6% with pain, 43.6% with fatigue, 38.2% with depressed mood, and 25.0% with gait aid use. In total, 92.6% took immunosuppressive therapy. Employment rates were 62.6% before and 36.3% after NMOSD diagnosis. In a multivariable model, statistically significant independent associations with unemployment in NMOSD were older age (odds ratio (OR) = 0.97, p < 0.001), being female (OR = 0.48, p < 0.001), bilateral visual loss (OR = 0.61, p = 0.02), highest frequency of depressed mood (OR = 0.29, p < 0.001), and walking aid use (OR = 0.38, p < 0.001).
Discussion:
Approximately 1/3 of people living with NMOSD of potential working age are in the workforce. Unemployment in NMOSD is associated with previously recognized factors but also self-reported low mood, gait aid use, and bilateral visual loss.
Introduction
Approximately 170,000 people worldwide have neuromyelitis optica spectrum disorder (NMOSD), an inflammatory autoimmune disease of the central nervous system with a relatively low prevalence of 0.5 to 4/100,000.1,2 Both cardinal symptoms of NMOSD, including visual loss and spinal cord dysfunction, and secondary symptoms such as fatigue, pain, and mental health outcomes, can lead to cumulative and permanent disability for patients living with the disease. In turn, these deficits could impact adults of working age in work contexts, influencing their ability to work and earn income.
In this study, we aim to quantitatively characterize the economic impact of NMOSD on employment, work hours, and wages of people living with the disease internationally. Given the significant impact of NMOSD on the central nervous system, we hypothesize that working adults with NMOSD will experience high prevalences of unemployment, reduced working hours, and loss of personal income. Moreover, as the disease predominantly affects women, we also aim to delve into the demographic and clinical variables that are associated with socioeconomic outcomes. This could inform approaches to disease treatment that allow preservation of a person’s socioeconomic functioning in society.
Methods
Ethics approvals
The protocol was approved by the Massachusetts General Brigham Institutional Review Board and by each site’s local ethics board as needed. Data were collected anonymously. Survey completion by participants implied consent.
Participant recruitment and data collection
Participants with NMOSD were recruited from 23 countries (Albania, Argentina, Australia, Brazil, China, Colombia, Dominican Republic, Egypt, Guinea, India, Indonesia, Iran, Italy, Kuwait, Malaysia, Mexico, Singapore, Spain, Thailand, Turkey, the United Kingdom, the United States, Venezuela) from April 2022 to August 2023. Recruitment efforts were led locally by neurologists. Participants completed the survey during clinic visits or were contacted by telephone and provided an online link. Inclusion criteria were age between 18 and 70 years and a diagnosis of NMOSD, as determined by the neurologist. An aquaporin-4 (AQP-4) antibody assay was not required for inclusion, as not every study center had consistent access to antibody testing. Participants with myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD) were excluded. Several centers offered support for participants’ survey completion, for example, for low vision or hand weakness. The U.S. participants were previously reported in a separate study. 3
Survey design
The 65-question survey took approximately 30 to 40 minutes to complete (Supplemental Appendix A). The survey covered (1) demographic variables, (2) clinical history of NMOSD, (3) employment and wages, (4) treatments and medications, (5) comorbidities, and (6) symptoms of NMOSD. All clinical data were self-reported, including antibody status, presence of visual loss, fatigue, pain, depression, and other conditions.
The survey was drafted in English, derived from focus group discussions of U.S. NMOSD patients, and translated by local neurologists and research staff into Hindi, Indonesian, Mandarin, Malay, Brazilian Portuguese, Spanish, and Thai.
Definitions of main outcomes and predictors
Employment was defined as participants who reported working at least 40 hours per week (including those who were “self-employed”), or full-time, which excluded part-time employees, students, and others. Work hours were only considered for participants who were employed pre-diagnosis. All income and wage data were reported in the participant’s currency and converted to a standard currency and exchange rate, using data on international dollars in 2022, the time of survey.
International dollars are a hypothetical currency designed to standardize global currencies to a single standard, based on the U.S. dollar.
Data analysis
The prevalence of outcome variables of interest (e.g. employment) is reported pre- and post-NMOSD diagnosis and by gender.
Univariate analyses were conducted with variables selected a priori—participant age at study enrollment, gender, years of formal education, country income-level stratum, presence of myelitis, unilateral or bilateral visual loss, frequency of fatigue, frequency of depressed mood, pain level, disease duration, use of walking aids, and number of attacks—to build multiple linear and logistic regression models. Only explanatory variables that were statistically significantly associated with the desired output variable (p < 0.20) were included in final models.
The employment regression model excluded students. The work hours’ regression model additionally excluded participants who had 0 work hours pre-diagnosis, as we were interested in the impact of NMOSD on participants who were already working at the time of diagnosis. Although the survey collected continuous data on the number of work hours, we chose to dichotomize work hours to lost/reduced or not because of lower and inaccurate response completion in the free-text numerical response compared to the binary question. The income regression model excluded participants who either did not submit pre- or post-diagnosis income data and those who had no income both pre- and post-diagnosis. Sensitivity analyses were performed post hoc in two separate subcohorts: (1) known AQP-4 seropositive and (2) ages 18–60 years old.
Analyses were conducted using R (4.3.1). A p-value of < 0.05 was considered statistically significant. Reporting followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Data cleaning
Survey data were reviewed for quality and accuracy. From 944 submissions, 25 were removed as duplicate or incomplete submissions (defined as completion of < 75% of survey questions). A total of 22 participants were removed due to age (Figure 1).
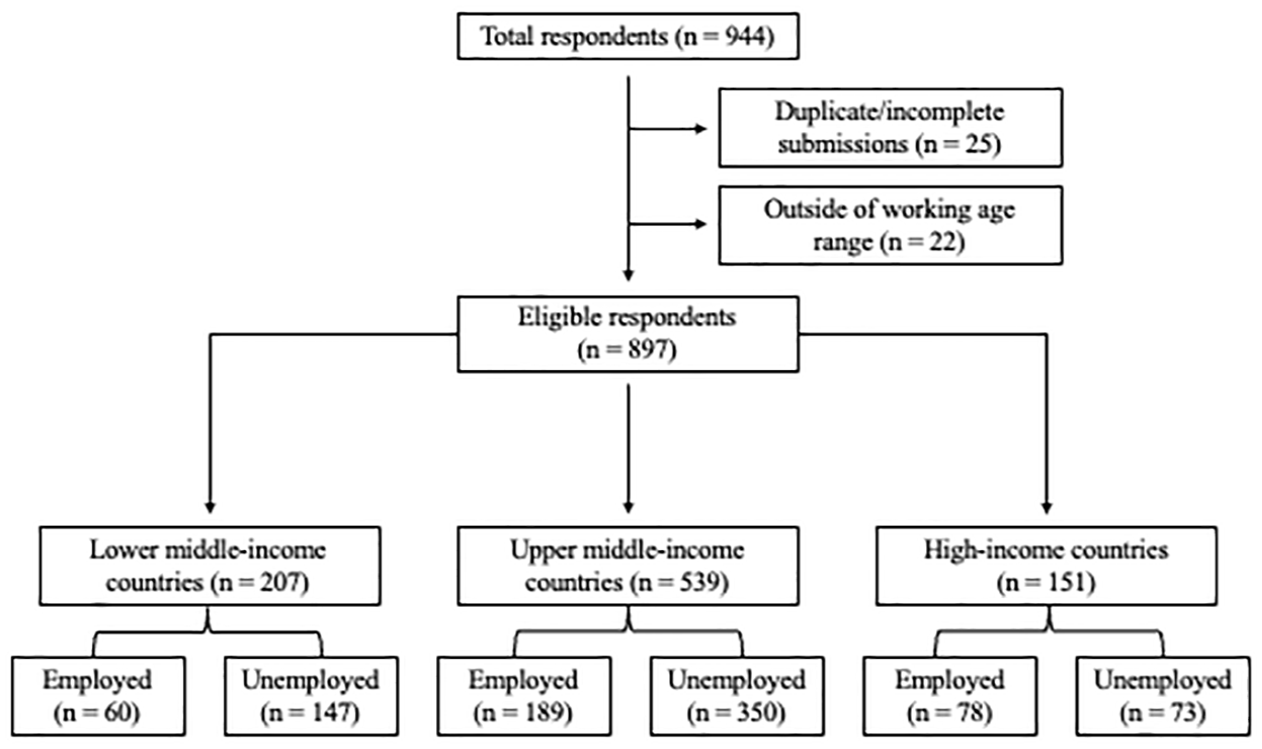
Participant selection and proportions of employed participants.
Additional data cleaning, including translations of survey responses, income conversions, and corrections of obvious errors (e.g. inputting the year of diagnosis instead of age at diagnosis), was conducted. Some participants erroneously reported that they were seropositive to both aquaporin-4 and myelin oligodendrocyte glycoprotein antibodies. In these cases, attempts were made to clarify responses with the study site, which often had the antibody test results.
Countries were classified by World Bank income level. 4 Venezuela was categorized as lower middle-income, as it is unclassified by the World Bank. 4
Missing responses were considered missing completely at random when forced responses were not required. No data imputation occurred.
Results
Demographic
There were 897 participants with NMOSD (81.4% female, mean enrollment age 42.5 ± 12.2 (standard deviation) years, mean disease duration 7.6 ± 7.4 years) (Table 1). Participants had 12.6 ± 4.4 years of formal schooling on average, and 27 (3.0%) were current students. A total of 207 participants (23.1%) were from lower middle-income countries, 539 (60.1%) from upper middle-income countries, and 151 (16.8%) from high-income countries. Most participants were from China (n = 199), the United States (n = 102), India (n = 76), and Iran (n = 70).
Demographic and clinical variables.
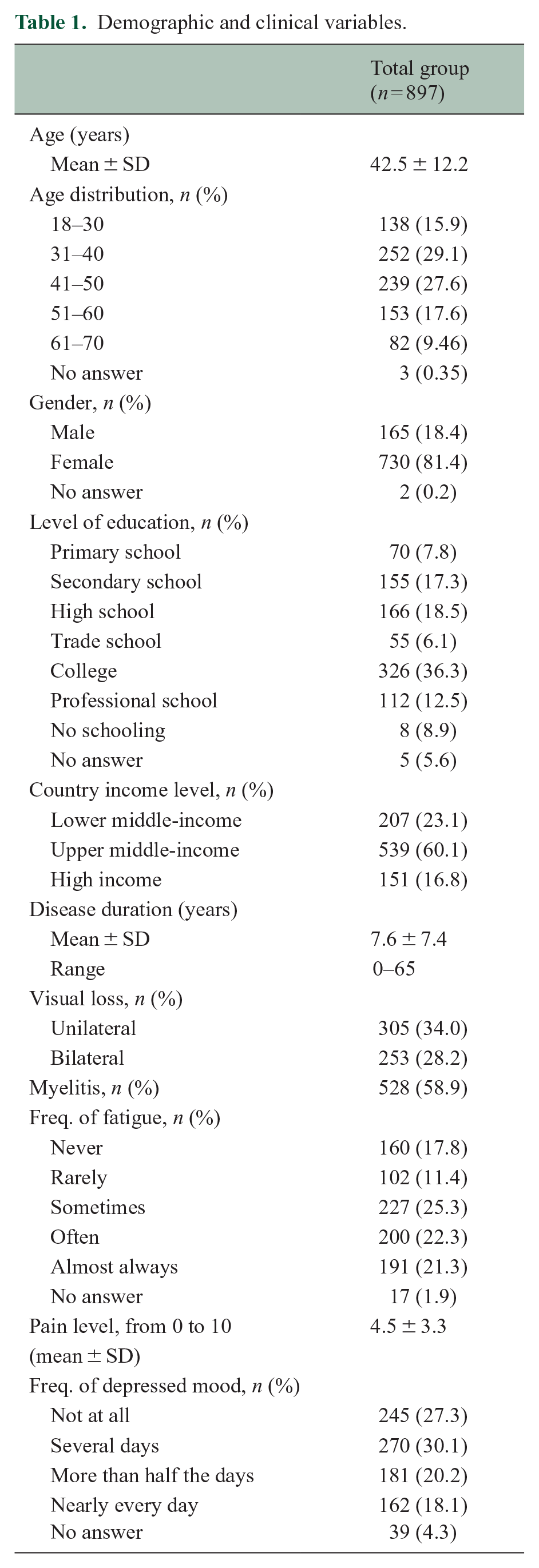
A total of 542 participants (60.4%) were married, 263 (29.3%) were single, and 83 (9.3%) were widowed, separated, or divorced. The mean household size was 3.7 ± 1.8 people, which constituted an average number of 2.8 ± 1.7 adults and 1.8 ± 1.2 income earners. Of the 886 participants who answered questions on caregiving, 636 (71.8%) reported receiving unpaid care, most commonly from spouses/partners (46.6%), parents (29.3%), children (11.0%), and siblings (8.0%).
Clinical picture
Participants were diagnosed with NMOSD at a mean age of 35.5 ± 12.0 years, with a mean age at onset of 34.1 ± 18.1. Since diagnosis, participants reported a median of two attacks (25th, 75th percentile: 1, 5).
In total, 635 (72.2%) participants were AQP-4 antibody positive, while the remainder were double-seronegative or untested. In total, 65.0% of participants from lower middle-income countries were AQP-4 positive, compared to 75.5% of upper middle-income and 70.7% of high-income participants.
In total, 305 participants (34.0%) suffered unilateral visual loss, while 253 (28.2%) lost vision in both eyes. A majority (58.9%) indicated living with myelitis, and 34.5% of them were actively using walking aids.
When asked to rate their average level of pain from 0 to 10 (with a score of 5 indicating moderate pain), participants reported a mean score of 4.5 ± 3.3. Most (57.0%) reported that pain impacted their ability to work and complete job duties, and 457 (50.9%) stated that pain impacted their decision to work. In total, 391 (43.6%) participants suffered from fatigue “often” or “almost always.” In total, 343 (38.3%) also underwent periods of depressed mood “more than half the days of the week” or “nearly every day.”
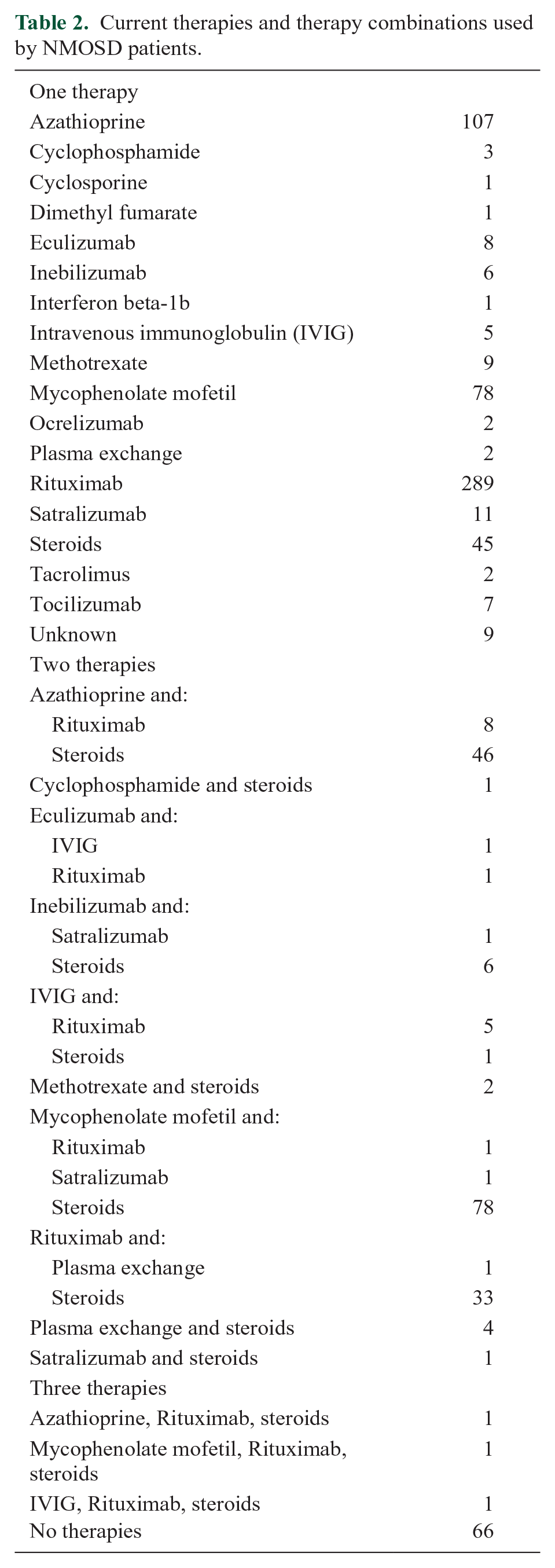
Most (92.6%) were treated for their NMOSD through immunosuppressive agents, steroids, and/or immunoglobulins (Table 2).
Current therapies and therapy combinations used by NMOSD patients.
Socioeconomic
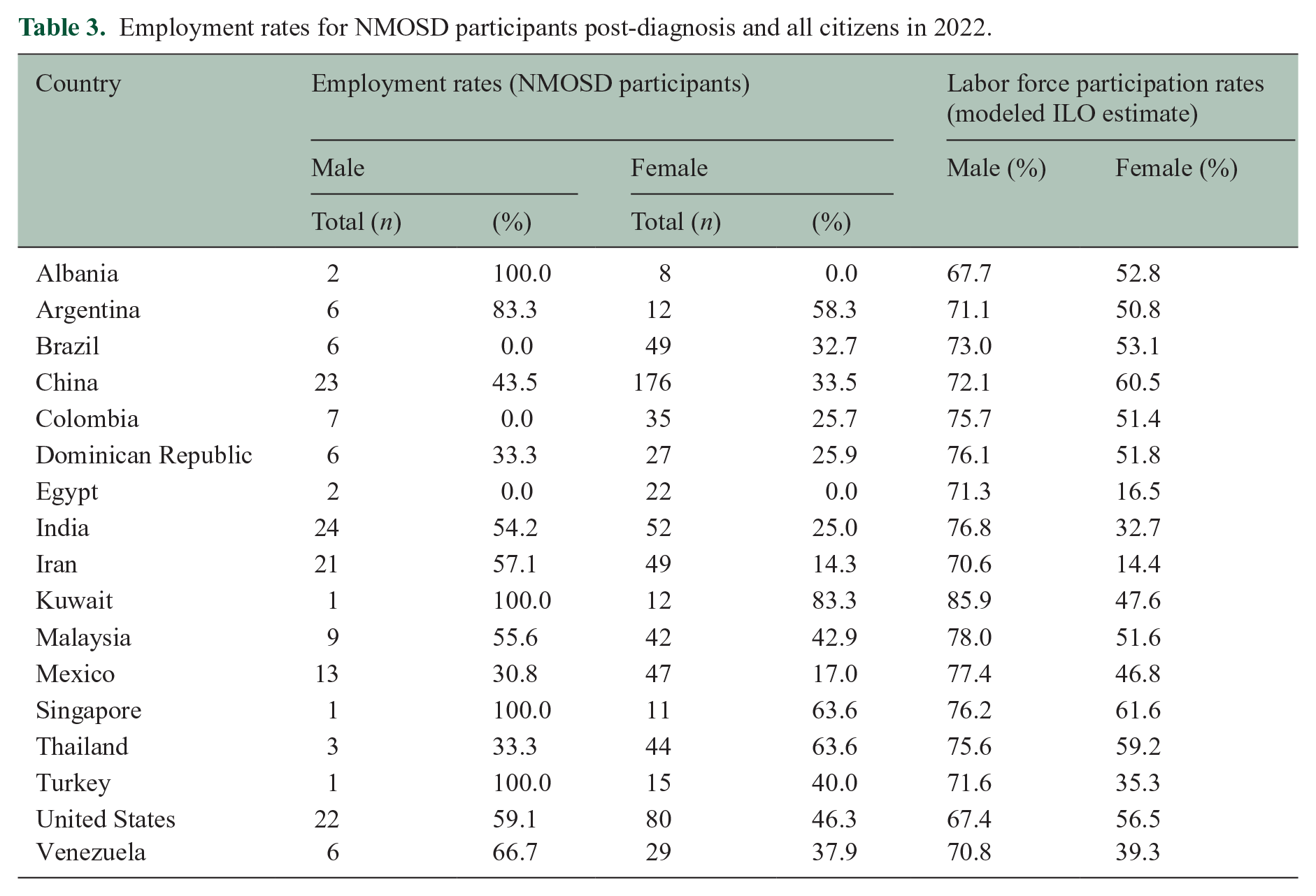
In total, 562 participants (62.7%) were employed to some capacity (full-time work, part-time work, self-employment) before their NMOSD diagnosis (73.5% full-time, 9.8% part-time, 16.7% self-employed). This decreased to 326 (36.3%) post-diagnosis (74.8% full-time, 20.6% part-time). This trend persisted across genders: any employment was 75.6% for men and 60.2% for women pre-diagnosis and 46.7% for men and 34.2% for women post-diagnosis (Table 3). Across country income categorizations, employment was 29.0% in lower middle-income countries, 35.1% in upper middle-income countries, and 52.0% in high-income countries. Fifty-five (6.1%) participants engaged in paid part-time work pre-diagnosis and 67 did part-time work post-diagnosis.
Employment rates for NMOSD participants post-diagnosis and all citizens in 2022.
Average work hours for paid full-time and part-time workers decreased from 32.8 hours/week to 16.3 hours/week after NMOSD diagnosis. For full-time workers specifically, 379 (42.3%) reported losing work, and 521 (58.1%) reported having to reduce their work hours or having their work hours reduced as a consequence of their diagnosis. In total, 48.9% of respondents stated that their employers were aware of their diagnosis. In total, 321 (35.8%) received health insurance from work, and of those, 264 (82.2%) indicated keeping this insurance as the reason for continuing to work.
While nearly half (48.3%) of participants reported losing wages after the NMOSD diagnosis, the median yearly income increased from 4878.10 to 7022.18 international dollars. These incomes were standardized using the international dollars system but did not account for trends such as inflation.
Model building and regression analyses
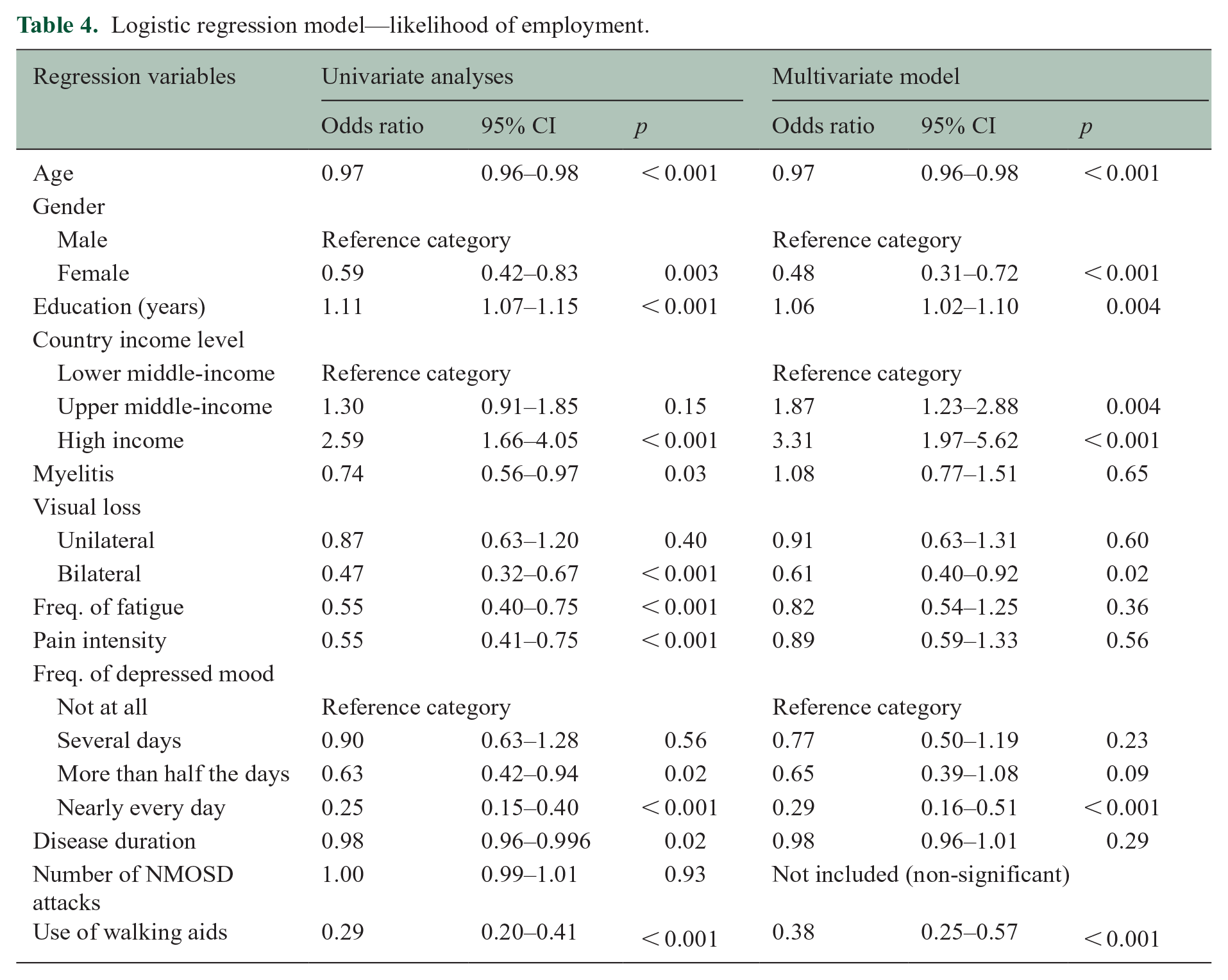
Univariate analyses looking at a multitude of relevant demographic and clinical variables selected a priori found significant associations between increased employment and younger age, more years of education, residence in a high-income country, not having myelitis, not having bilateral visual loss, lower frequency of fatigue and depression, lower pain intensity, not using walking aids, and lower disease duration. A multiple logistic regression model constructed from these variables found that younger age, being male, more years of education, residence in upper middle-income and high-income countries, not having bilateral visual loss, not having frequent episodes of depressed mood, and non-use of walking aids were predictors of employment (Table 4).
Logistic regression model—likelihood of employment.
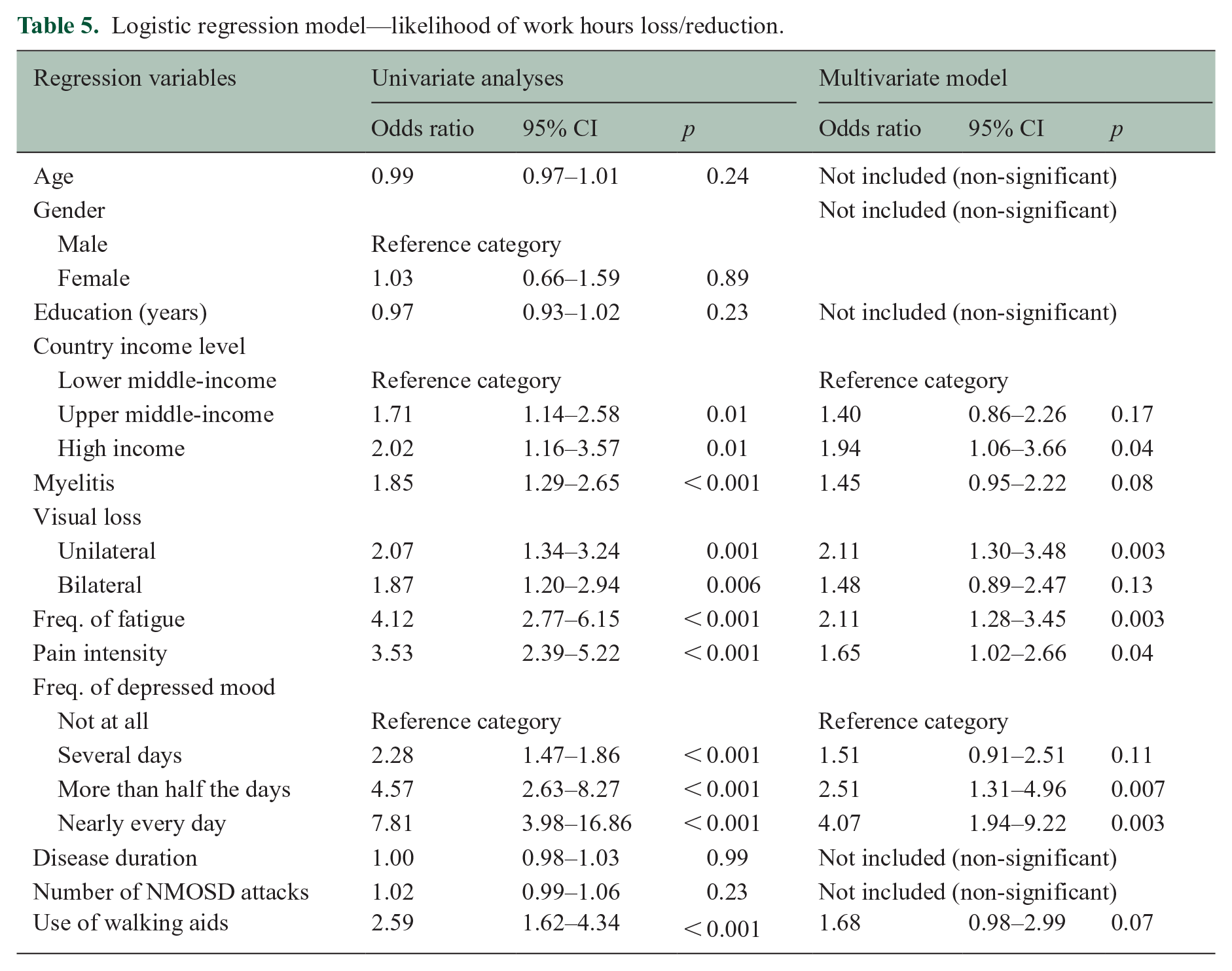
Similar processes were replicated for regression models of lost and reduced work hours and wages. In a multiple logistic regression model of lost or reduced work hours constructed from univariate analyses, clinical features including higher levels of pain, unilateral visual loss, and higher frequencies of fatigue and depressed mood were all significant predictors of a participant having lost or reduced work hours (Table 5). Residence in a high-income country was also a predictor of lost or reduced work hours.
Logistic regression model—likelihood of work hours loss/reduction.
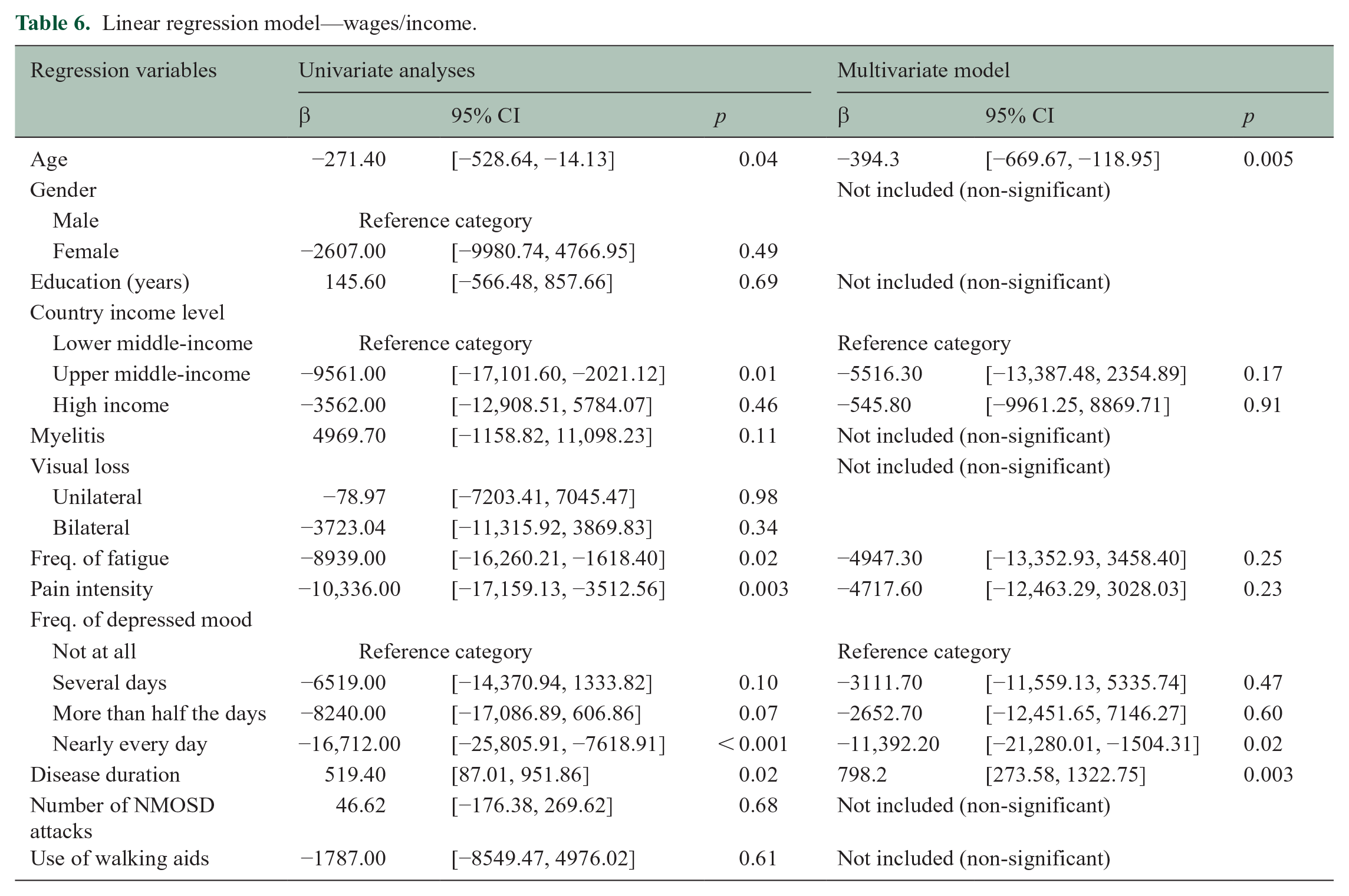
A multiple linear regression model of wages found that disease duration was positively associated with increased income between pre- and post-NMOSD diagnosis, suggesting that having more time to build a career was beneficial for wages (Table 6). On the contrary, older age and the highest frequency of depressed mood were predictive of wage decrease.
Linear regression model—wages/income.
All three regressions were repeated for the subcohorts who were known to be AQP-4 seropositive, that is, excluding those who were double-seronegative or did not receive antibody testing (Supplemental Appendix B). In total, 390 participants (61.7%) were employed before NMOSD diagnosis, and 237 (37.3%) were post-diagnosis. Average work hours for full-time and part-time workers decreased from 32.7 hours/week to 16.5 hours/week after diagnosis. In total, 237 (60.8%) previously working participants reported losing income post-diagnosis, although standardized income values increased from 5697.96 to 8203.13 international dollars over that time. This subcohort is disproportionately derived from higher-income countries.
Another sensitivity analysis was performed for the subcohort aged 18–60 years old, since the retirement age is not standardized across countries (Supplemental Appendix C).
Discussion
We investigated 897 patients living with NMOSD from 23 countries for the disease’s impact on employment and wages. Overall, patients often lost employment, reduced work hours, and lost income (although median income increased over the disease period), both due to individual-level symptoms and reflective of broader societal trends.
Employment and work hours for NMOSD patients
Employment was associated with various demographic (age, gender, years of education, country income level) and clinical (bilateral visual loss, depressed mood frequency) variables, while the loss and reduction of work hours were associated primarily with clinical factors (pain level, fatigue, and depressed mood frequency).
In interpreting these results, we propose the possibility that the symptoms of NMOSD, including blindness and paralysis, significantly impede an individual’s ability to work and often force him or her to take on reduced hours. However, when it comes to employment as a whole, well-known societal trends—including gender disparities in employment and higher employment rates in higher-income countries—also contribute.
Considering that NMOSD is a highly female-predominant disease, gender disparities in employment are particularly relevant for our study. Globally, the labor participation rate for men was 73.1% and 48.7% for women in 2023, and stratifying by country income stratum, labor participation rates were 75% for men and 38% for women in lower middle-income countries, 73% for men and 56% for women in upper middle-income countries, and 68% for men and 54% for women in high-income countries. 5 A “job gap” measure introduced by the International Labor Organization, which counts all individuals who are unemployed but desire employment, also found a significant gap between genders (15% to 10.3%) worldwide. 6
Moreover, gender disparities vary widely by country. For example, the female labor participation in 2023 was 14% in Iran and 33% in India, compared to 57% for the United States and 61% for China (four of the highest-represented countries in our data set). 5 According to the Global Gender Gap Report in 2023, additional nuance arises from the fact that even among those who are employed, women will more often face substandard working conditions, as 80% of jobs created for women are in the informal economy, which lacks standard protections and working conditions. Understanding how pervasive and significant gender disparities in employment are can help elucidate, in part, why it emerges as such a strong predictor in our (and any) employment model.
Moreover, jobs within the informal economy are also more common in lower-income countries, suggesting that while the employment rates reported above may seem relatively similar across country income strata, types of work may differ. 7 For patients with NMOSD, it is possible that certain categories of work, particularly those that do not require physical labor or have less emphasis on visual capabilities, are easier to continue after symptom onset.
Previous studies of work motivation in patients with immune-mediated inflammatory diseases have identified depression, in addition to pain, fatigue, and anxiety, as significant predictors of work absenteeism and activity impairment in univariate analyses. 8 We find similar patterns in the NMOSD context, as increased pain levels, fatigue, and depression each show varying significant associations with the likelihood of employment, work hours, and wages. Better treatment of pain and depression could potentially alleviate negative employment outcomes, as compared to some of the physical limitations of NMOSD, such as vision loss, that are more irreversible and lack effective treatments.
Interpretation of wage results
The impact of NMOSD on individual incomes will require further and more nuanced analysis beyond this study, as wages often increase over time (attributable to career progression, promotions, inflation, and other factors). We found that increases in income were positively associated with disease duration, for example, as people living with their diagnosis for 30 years (and able to maintain employment) experienced income increases.
Our finding that older age is associated with a decrease in wages suggests that while longer disease duration is associated with increased income, it is opposed by corresponding age-related losses in income. Potential explanations include decreased bargaining power for older employees (due to a lack of alternative career options later in life), age discrimination in the labor market, and the fact that older employees may not be able to work as many hours as their younger counterparts. 9 We also provide a relatively high upper age limit to be considered employable. There is no universal retirement age; the age of retirement differs widely by gender, birth year, and country of employment. 10
Finally, we find that participants who reported experiencing feelings of depression “nearly every day” were strongly associated with earning less income. We also find that pain and fatigue individually show significant associations with decreased income, corroborating some of our previous findings with reduced work hours.
Limitations and strengths of the study
Our study was primarily limited by using non-population-based sampling. All data were self-reported, and only participants with access to neurological care were able to be introduced to the study. Most participants were taking immunosuppressants; by virtue of having access to neurological care, being treated, and able to complete our survey, our participants were likely better off than the general NMOSD population. In this sense, our employment, work hours, and wages data may reflect a better result than the global situation for people living with NMOSD. We did not exclude any patients based on time since last relapse. A major limitation of this survey sampling is that it was difficult to coordinate the collection of response rates given the complex, international nature of the study. The survey could be biased toward patients who are either employed and are able to complete a survey, or rather to those with extra time to complete an unpaid survey; the direction of a potential response bias is not known.
There are variabilities in employment expectations, cultural norms, and social influences among countries. Countries have different laws, gender roles, accommodations for employees with physical disabilities, and other factors that affect trends in employment, work hours, and wages post-diagnosis. Moreover, because NMOSD mostly affects the female population, there was a natural gender imbalance in our sample. Our analysis of wages and income was limited by the omission of potential influencers, including inflation and career progression. Nonetheless, we aimed to provide an inclusive, global perspective on employment, highlighting common themes across income levels and the influence of macro-development at the country level on individual outcomes at the patient level.
Useful future additions to our survey tool could include questions inquiring about job accommodations and the work environment. In particular, understanding the availability of accessibility features is critical, as an impairment in one context can become disability in another (e.g. in a higher floor area workplace without an elevator, a weak leg may become a disability instead of an impairment).
For any comparisons between AQP-4 positive and double-seronegative participants in this article, it is important to note that the AQP-4 antibody is available differentially worldwide. 11 In countries with no antibody testing, participants were deemed “double-seronegative,” but this may actually be best considered as “antibody status unknown.” 12 Moreover, we did not explicitly require the NMOSD diagnostic criteria to be applied for participants’ inclusion. Given the disease severity reported by participants, we deduced that these participants would meet the most recent 2015 NMOSD diagnostic criteria (given history of visual loss, spinal cord dysfunction, number of attacks), but we did not specifically mandate that the NMOSD diagnostic criteria be applied before a participant was invited for every center. 13
Despite these limitations, issues of employment and income in NMOSD have not previously been studied in depth. NMOSD is a relatively rare disease, and we present a large international cohort of patients, which can lend insights into lived experiences and collective outcomes of people with NMOSD. Others have found that NMOSD can be an expensive disease for patients and their families. 14 Our results highlight areas of consideration to better serve patients, ranging from micro-level clinical features such as pain and fatigue management to macro-level socioeconomic variables.
Although there are country-level differences, our findings identify significant impacts from the debilitating symptoms of NMOSD, regardless of country of residence. “Invisible symptoms” such as fatigue and depression are universal. Earlier interventions to help patients maintain employment, considering the demonstrable impact of disease diagnosis on working ability, should be pursued. Developing a robust set of disability guidelines to protect patients against workplace discrimination, in line with the UN Declaration on the Rights of the Disabled Persons, along with producing new treatments for major disease symptoms, could help alleviate some of the issues highlighted in this study. 15
Advocacy organizations can educate employers about the persistent disabilities of NMOSD despite treatment. Physicians should also inquire about workplace barriers in addition to clinical symptoms, serving in an advocacy role when required. Despite being a relatively well-treated and monitored sample of NMOSD participants, we find that the disease significantly and negatively impacts patients’ likelihood of maintaining employment, work hours, and wages. Such findings shed light on the less visible but generally global socioeconomic consequences of NMOSD.
Supplemental Material
sj-docx-1-msj-10.1177_13524585251349139 – Supplemental material for Unemployment, work hour reduction, and income loss: An international, multicentered, cross-sectional study of neuromyelitis optica spectrum disorder
Supplemental material, sj-docx-1-msj-10.1177_13524585251349139 for Unemployment, work hour reduction, and income loss: An international, multicentered, cross-sectional study of neuromyelitis optica spectrum disorder by Andrew Siyoon Ham, Isabella Gomez Hjerthen, De-Cai Tian, Hongfei Gu, Wen Gao, Akshatha Sudhir, Lekha Pandit, Y Muralidhar Reddy, Jagarlapudi Muralikrishna Murthy, Sharareh Eskandarieh, Mohammad Ali Sahraian, Saeideh Ayoubi, Roberto Rodríguez-Rivas, Francisco González-González, José de Jesús Flores Rivera, Enedina Maria Lobato Oliveira, Raquel Paiva Portugal, Paloma Peter Travassos Zaidan, Shanthi Viswanathan, Karina Koh, Su-Yin Lim, Punchika Kosiyakul, Jiraporn Jitprapaikulsan, Sasitorn Siritho, Saúl Reyes, Jaime Toro, Jairo Gaitán, Deyanira Ramirez Navarro, Raúl Comme-Debroth, Josmarlin Patricia Medina Báez, Maria Castillo, Soto de Castillo Ibis, Sandra Mendoza de Salazar, Omaira Molina, Amany Hussein Ragab, Amr Mohamed Fouad, Nirmeen Adel Kishk, Juan Ignacio Rojas, Edgardo Cristiano, Liliana Patrucco, Bade Gülec, Ugur Uygunoglu, Melih Tutuncu, Aksel Siva, Amelia Yun Yi Aw, Kevin Tan, Tianrong Yeo, Raed Alroughani, Samar Farouk Ahmed, Malak Almojel, Jera Kruja, Ariola Verlaku, Olga Qirjako, Riwanti Estiasari, Kartika Maharani, Saif Huda, Patricia Kelly, Raffaele Iorio, Eleonora Sabatelli, Álvaro Cobo-Calvo, Georgina Arrambide, Javier Villacieros Álvarez, Simon Broadley, Unnah Leitner, Fodé Abass Cissé, Mohamed Lamine Touré, Kab Conde and Farrah J Mateen in Multiple Sclerosis Journal
Supplemental Material
sj-docx-2-msj-10.1177_13524585251349139 – Supplemental material for Unemployment, work hour reduction, and income loss: An international, multicentered, cross-sectional study of neuromyelitis optica spectrum disorder
Supplemental material, sj-docx-2-msj-10.1177_13524585251349139 for Unemployment, work hour reduction, and income loss: An international, multicentered, cross-sectional study of neuromyelitis optica spectrum disorder by Andrew Siyoon Ham, Isabella Gomez Hjerthen, De-Cai Tian, Hongfei Gu, Wen Gao, Akshatha Sudhir, Lekha Pandit, Y Muralidhar Reddy, Jagarlapudi Muralikrishna Murthy, Sharareh Eskandarieh, Mohammad Ali Sahraian, Saeideh Ayoubi, Roberto Rodríguez-Rivas, Francisco González-González, José de Jesús Flores Rivera, Enedina Maria Lobato Oliveira, Raquel Paiva Portugal, Paloma Peter Travassos Zaidan, Shanthi Viswanathan, Karina Koh, Su-Yin Lim, Punchika Kosiyakul, Jiraporn Jitprapaikulsan, Sasitorn Siritho, Saúl Reyes, Jaime Toro, Jairo Gaitán, Deyanira Ramirez Navarro, Raúl Comme-Debroth, Josmarlin Patricia Medina Báez, Maria Castillo, Soto de Castillo Ibis, Sandra Mendoza de Salazar, Omaira Molina, Amany Hussein Ragab, Amr Mohamed Fouad, Nirmeen Adel Kishk, Juan Ignacio Rojas, Edgardo Cristiano, Liliana Patrucco, Bade Gülec, Ugur Uygunoglu, Melih Tutuncu, Aksel Siva, Amelia Yun Yi Aw, Kevin Tan, Tianrong Yeo, Raed Alroughani, Samar Farouk Ahmed, Malak Almojel, Jera Kruja, Ariola Verlaku, Olga Qirjako, Riwanti Estiasari, Kartika Maharani, Saif Huda, Patricia Kelly, Raffaele Iorio, Eleonora Sabatelli, Álvaro Cobo-Calvo, Georgina Arrambide, Javier Villacieros Álvarez, Simon Broadley, Unnah Leitner, Fodé Abass Cissé, Mohamed Lamine Touré, Kab Conde and Farrah J Mateen in Multiple Sclerosis Journal
Supplemental Material
sj-docx-3-msj-10.1177_13524585251349139 – Supplemental material for Unemployment, work hour reduction, and income loss: An international, multicentered, cross-sectional study of neuromyelitis optica spectrum disorder
Supplemental material, sj-docx-3-msj-10.1177_13524585251349139 for Unemployment, work hour reduction, and income loss: An international, multicentered, cross-sectional study of neuromyelitis optica spectrum disorder by Andrew Siyoon Ham, Isabella Gomez Hjerthen, De-Cai Tian, Hongfei Gu, Wen Gao, Akshatha Sudhir, Lekha Pandit, Y Muralidhar Reddy, Jagarlapudi Muralikrishna Murthy, Sharareh Eskandarieh, Mohammad Ali Sahraian, Saeideh Ayoubi, Roberto Rodríguez-Rivas, Francisco González-González, José de Jesús Flores Rivera, Enedina Maria Lobato Oliveira, Raquel Paiva Portugal, Paloma Peter Travassos Zaidan, Shanthi Viswanathan, Karina Koh, Su-Yin Lim, Punchika Kosiyakul, Jiraporn Jitprapaikulsan, Sasitorn Siritho, Saúl Reyes, Jaime Toro, Jairo Gaitán, Deyanira Ramirez Navarro, Raúl Comme-Debroth, Josmarlin Patricia Medina Báez, Maria Castillo, Soto de Castillo Ibis, Sandra Mendoza de Salazar, Omaira Molina, Amany Hussein Ragab, Amr Mohamed Fouad, Nirmeen Adel Kishk, Juan Ignacio Rojas, Edgardo Cristiano, Liliana Patrucco, Bade Gülec, Ugur Uygunoglu, Melih Tutuncu, Aksel Siva, Amelia Yun Yi Aw, Kevin Tan, Tianrong Yeo, Raed Alroughani, Samar Farouk Ahmed, Malak Almojel, Jera Kruja, Ariola Verlaku, Olga Qirjako, Riwanti Estiasari, Kartika Maharani, Saif Huda, Patricia Kelly, Raffaele Iorio, Eleonora Sabatelli, Álvaro Cobo-Calvo, Georgina Arrambide, Javier Villacieros Álvarez, Simon Broadley, Unnah Leitner, Fodé Abass Cissé, Mohamed Lamine Touré, Kab Conde and Farrah J Mateen in Multiple Sclerosis Journal
Footnotes
Author Contributions
F.J.M. contributed to the conception and design of the study; all co-authors contributed to the acquisition and analysis of data; A.S.H. and F.J.M. contributed to drafting the text or preparing the figures. I.G.H. also contributed to the study concept and data interpretation.
Data Availability Statement
Anonymized data will be made available to qualified investigators upon request, subject to ethics board approvals.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr F.J.M. has received research funding for her institution from Alexion, Amgen, EMD Serono, Genentech, Novartis, and TG Therapeutics and consulting fees from Alexion, EMD Serono, Genentech, and Roche. Dr T.Y. has received honoraria from ASNA, Edanz Pharma, Euroimmun AG, Merck, Novartis, Roche, Terumo BCT for consulting services and speaker’s fees, and research grants from the National Medical Research Council (NMRC Singapore) and Roche. Dr A.S. has received research grants from The Turkish Multiple Sclerosis Society and research grants from The Scientific and Technological Research Council of Turkey & Istanbul University-Cerrahpasa Research Support Funds. Dr A.C.-C. has received a grant from the Instituto de Salud Carlos III, Spain; JR19/00007.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding sources for this project include the Sumaira Foundation and an investigator-initiated grant from Amgen. Both sponsors had no role in the study concept, design, analysis, or decision to submit the work for publication. The authors are grateful to the American Academy of Neurology’s Neuroscience is Rewarding program for an internship scholarship to I.G.H.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.