
Abstract
Background:
Multiple sclerosis (MS) exercise terminology lacks consistency across disciplines, hindering research synthesis.
Objective:
The ‘Moving exercise research in MS forward initiative’ (MoXFo) aims to establish agreed definitions for key MS exercise terms.
Methods:
The Lexicon development methodology was employed. A three-step process identified key exercise terminology for people with multiple sclerosis (pwMS): (1) consensus and systematic review, (2) Delphi round 1 and consideration of existing definitions and (3) Delphi round 2 for consensus among MoXFo steering group and exercise experts. Final definitions and style harmonisation were agreed upon.
Results:
The two-stage Delphi process resulted in the selection and scoring of 30 terminology definitions. The agreement was 100% for resistance exercise, balance and physical activity. Most terms had agreement >75%, but ‘posture’ (60%) and ‘exercise’ (65%) had a lower agreement.
Conclusion:
This study identified key terms and obtained agreement on definitions for 30 terms. The variability in agreement for some terms supports the need for clearly referencing or defining terminology within publications to enable clear communication across disciplines and to support precise synthesis and accurate interpretation of research.
Introduction
The volume and quality of research on exercise interventions among people with multiple sclerosis (pwMS) have grown substantially in the last two decades. 1 There is now strong evidence for the benefits of exercise in multiple sclerosis (MS). 2 For people living with MS, exercise has the potential to improve physical fitness,3,4 walking mobility, 5 - 7 strength,7,8 balance, 9 cognition, 10 fatigue,4,11- 13 mood 14 and quality of life.15,16 Evidence from interventions in pwMS further indicates that exercise improves outcomes measured by magnetic resonance imaging and modulates peripheral biomarkers associated with neural health. 17 Exercise may benefit overall brain preservation, 18 - 20 reduce relapse rate 21 and might slow disability progression. 22 - 24 However, exercise research studies in pwMS typically involve small sample sizes with a high diversity of outcome measures used, which limits research efficacy and the ability to pool data. A further issue, compounded by the interdisciplinary nature of exercise research in pwMS, is a lack of consensus on the vocabulary and definitions of these terms used in reporting the research. Terminology is used with varying meanings across disciplines. For example, the word intensity may be used to reflect the number of sessions or the metabolic equivalent of activities. Together, this limits the potency of reporting and comparison of intervention methodology, affecting the accuracy of interpretation and limiting the efficacy of subsequent systematic reviews and network meta-analyses. 25
Recently, the ‘Moving exercise research in MS forward’ (MoXFo) initiative was established to address barriers to rapid progress in the field. 26 The initial work of the MoXFo initiative identified five areas that needed attention including consensus work on definitions and terminology within the MS exercise field. Moreover, creating a consensus on vocabulary for use in future research studies is an initial step to supporting better methodological consistency and more precise interpretation across research studies and disciplines. Achieving consistency in the language used within and across scientific disciplines is challenging but a critical step in achieving research excellence and good practice. Importantly, consistency in health terminology has been shown to influence clinical studies positively and to create clarity in healthcare provider education, 27 in translation to industry, and for pwMS. 28
The scientific convention often calls for developing a standard lexicon across disciplines and geographical borders that underpins clear communication. 29 This study followed a lexicon-development methodology, 29 which has been successfully used to elevate clear communication both within and across professionals involved in interdisciplinary research in quality of life and health outcomes measurement literature in MS research. 25 This project aimed to generate a vocabulary for MS exercise terminology for audiences with a specific set of needs (vertical audience), including people from the novice to the expert and from different disciplines, who all have a common interest in exercise prescription. We set out to develop a vocabulary to enable clear communication among MS researchers, MS healthcare and fitness professionals and pwMS and their families. 30 - 32
Method
The following approach was adopted. Initially, a group of researchers from the MoXFo initiative formed a steering group (the MoXFo steering group). The MoXFo initiative was initiated by U. Dalgas and C. Heesen, who gathered experts from five crucial areas of the field in a steering group. An author group for the actual terminology work was selected as having expertise in exercise and movement science, public health, rehabilitation, measurement methodology, Lexicography, neuroscience and physiology and representing North America, Australasia, West Asia and Europe.
All stages of the process were underpinned by Lexicography, a field methodology to create a vocabulary list of selected terms from the general language or a particular field of knowledge with brief definitions suitable for a vertical audience, which is one that includes those across disciplines, and from the novice to the expert. 29 To achieve this, the following methodologies were used: a literature review, a consultation with professional bodies, an informal consensus development panel, a two-stage Delphi process and a final definitions and style harmonisation consensus development panel. The project plan and timeline outlining the aims, methods and analysis were developed by M.M. and H.D. with oversight of all authors (M.M., J.C., Y.C.L., H.D. and N.M.). The lexicon methodology 25 employed in this study involved a series of steps to determine and provide clear definitions for key terminology related to exercise in MS.
In this study, a group of 30 professionals in the field, along with a systematic review of exercise in pwMS, were used to identify appropriate terminology related to exercise in PWMS. The selected terminology then underwent a process of finding definitions, which involved 24 experts and consideration of available definitions from professional bodies (Delphi 1). Finally, a consensus methodology approach was used, which involved the MoXFo steering group and 24 exercise experts, to agree on the definitions of each term. This was achieved through a Delphi 2 round, where the experts provided their feedback and opinions on the proposed definitions, leading to a consensus on the terminology and its definition for use in future studies related to exercise in PWMS. The authors and the MoXFo steering group carried out a final harmonisation of term definitions. A flow diagram showing the different stages of the process is depicted in Figure 1.
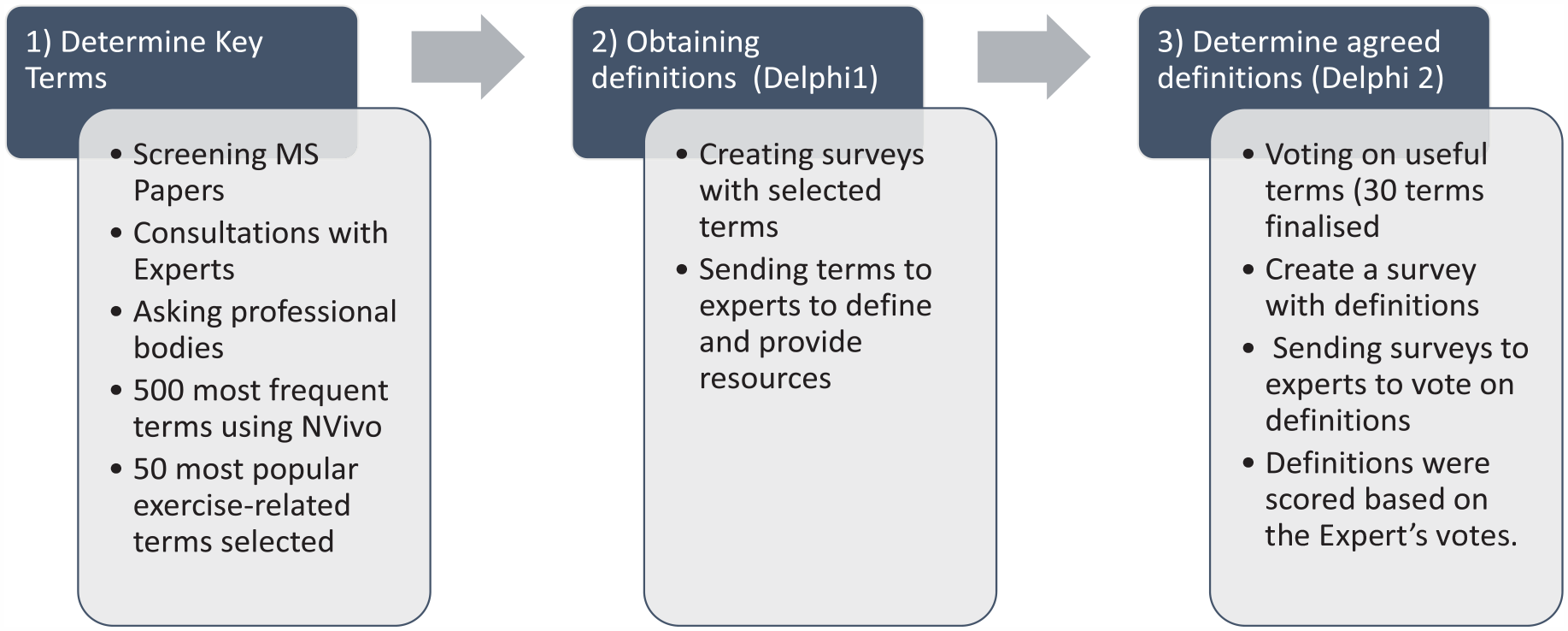
Flow diagram showing the different stages of the project.
The detailed process of the three stages of the project is comprehensively explained below.
Determine key terms
(1) To determine common usage in clinical trials, we used all the full text of 81 articles from a systematic literature review produced by the MoXFo exercise trials reporting and outcomes group. 33 NVivo AI software (QRS) identified the 500 most frequently used terms from the full text of all 81 manuscripts. NVivo is a computer-assisted qualitative data analysis software (CAQDAS) that aids researchers in organising, analysing and visualising unstructured or semi-structured data. One of the key features of NVivo is its ability to identify and extract the most common terms in a document or a set of documents. This process, called text mining, enables researchers to identify patterns and trends in large data sets that may be difficult to detect through manual analysis.
After the data mining process of all the articles using NVivo, the list included terms not related to exercise and physical activity. M.M. and H.D. searched the list by hand and identified the 50 most frequently used terms related to exercise and physical activity (stage a). 33
(2) Simultaneously, an expert panel that included the authors, the MoXFo steering group, and 30 International experts, representing disciplines of physical activity, physiotherapy and exercise science/physiology and different geographical regions were invited to identify key terms. Each expert was asked to identify 10 key terms that required definition clarity (Supplemental Appendix 2). Criteria for the inclusion of experts were that members must be researchers or professionals working in physical activity or clinical exercise science or with expertise in exercise science and MS. Identification of appropriate panellists were performed through the manual review of relevant peer-reviewed literature, personal networks and special interest groups for physiotherapy, physical activity and exercise science/physiology. Twenty-four experts agreed to participate. Participating experts were asked to identify 10 key terms from the 50 most frequently used terms. Each in relation to exercise and MS, requiring definition clarity.
(3) Duplicates were removed, and terms from the review (42 terms) and experts (8 additional terms) were merged. A total number of 50 terms were left.
Obtaining definitions from the selected key terminology (Delphi 1)
(1) Two researchers (H.D. and Y.C.L.) approached professional bodies (physical activity/public health, exercise science/physiology, physiotherapy) from English-speaking nations to collect already available definitions and vocabulary (Supplemental Appendix 2). Utilising Delphi methodology to determine consensus, initially, a questionnaire (Delphi 1) was simultaneously sent out to the 24 experts to determine definitions for all 50 terms. The literature makes no formal recommendation regarding the number of survey voting (Delphi) members; above 8 is considered acceptable, but 20 is common. 34 The questionnaire was piloted on five individuals to test functionality and clarity, which was then confirmed through the study panel. Each expert was requested to define five terms independently. Each term was sent to at least two experts, so there was cross-over. Terms were matched to experts considering their expertise (used references and resources are listed in Supplemental Appendix 1). A resulting long list of vocabulary and definitions from experts and professional bodies was progressed to the next stage.34,35 Terms were considered out of scope and not included in the survey if they were biomarkers, adherence or other non-exercise focus terms and reduced down to 30 terms. 36
Determine agreed definitions for selected terms (Delphi 2)
Two definitions were allocated for each term in order to reduce burden or ranking. Where there were more than two definitions, for example, when both experts and an expert body definition were available, the authors (M.M., J.C., Y.C.L., H.D. and N.M.) met as an informal consensus development panel to select two definitions. For the second round of Delphi (Delphi 2), each term with two associated definitions were then sent to at least two people from the 24 experts for voting. Where there was a strong authority definition from a professional body and agreed upon by the authors, this was selected. In this instance, the one definition was sent out with a yes/no question.
All highest-ranked definitions based on the expert’s votes were then editorially harmonised for style by the authors (M.M., J.C., Y.C.L., H.D. and N.M.) in a consensus meeting and later by final editorial by the senior author in exchange with the MoXFo steering group. Final editorial harmonisation was carried out for consistency in the structuring of terminology definitions.
Data analysis
Frequency and descriptive analysis were completed on the responses in the Delphi 2. The agreement was carried out by the non-parametric assessment; Kendall’s W coefficient of concordance was used to quantify the extent of agreement between raters. 37 Data were analysed in SPSS version 28. An a priori arbitrary cut point was set so that all terms with >50% agreement were included. All terms are listed with agreed and non-agreed terminology in Supplementary Material.
Reducing bias
To address issues of both implicit and explicit bias, we recruited experts across disciplines and geography, and across both the MS scientific community and with wider clinical reach. We found the most cited authors and approached them, and then used a snowball technique to other experts. We also followed personal contacts through the MoXFo steering group. At all stages, teams worked together with different backgrounds and disciplines. Experts were paired to maximise diversity in geography and background. Critical stages were carried out by a consensus development panel (M.M., J.C., Y.C.L., H.D. and N.M.), and the final consensus was taken to the MoXFo steering group for agreement.
Results
Data on key terms were gathered between 15 August and 15 September 2021.
Key terminology selection: the review included 81 full papers from which the initial top 500 most frequently used terms were ranked, of which the top 50 exercise terms were taken forward to the next stage. Experts independently highlighted 15 terms for inclusion; all these terms were in the top 50 set of terms from the review.
Definition determination: 50 terms were sent out for definitions. The terms, frequency and relevance data are available from the authors on request. If the terms were biomarkers, adherence or other non-exercise-related terms, they were excluded from the survey as they were considered out of scope. The number of terms was then reduced to 30. The authors were able to use 30 terms in Delphi 2, considering the described criteria, with associated definitions that were then sent out for consensus (Tables 1 and 2). Table 1 summarises the terms and definitions.
Consensus methods: 28 term definitions achieved over 75% agreement. Definitions with scoring are presented in (Table 1). The final agreed definitions from the consensus process and following subsequent harmonisation process are listed in Tables 1 and 2 and Figure 1.
Terms definitions scores, based on the experts’ votes.
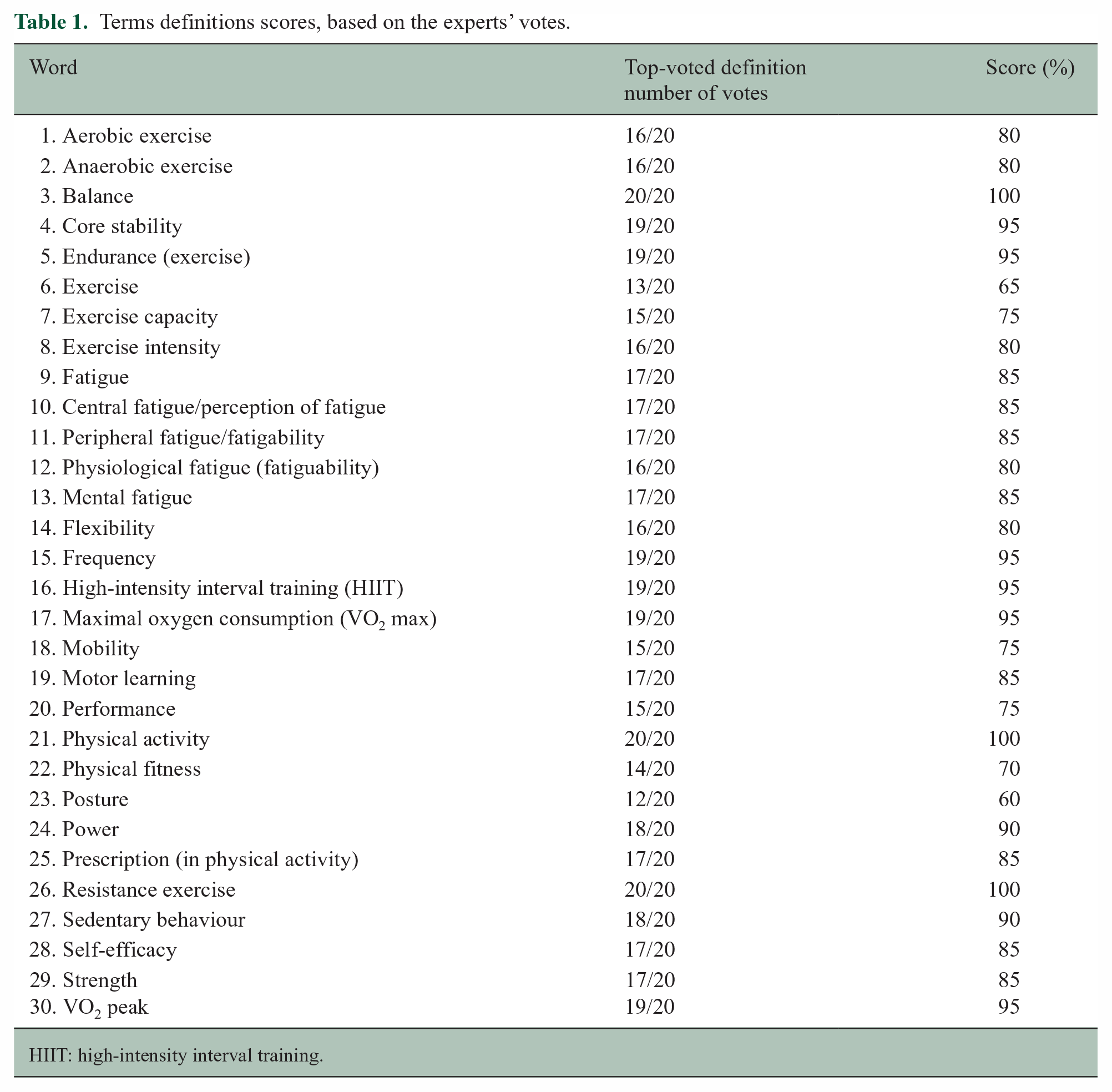
HIIT: high-intensity interval training.
Final definitions (see the Supplemental Appendix 1 for references and resources that have been used for providing the definitions).
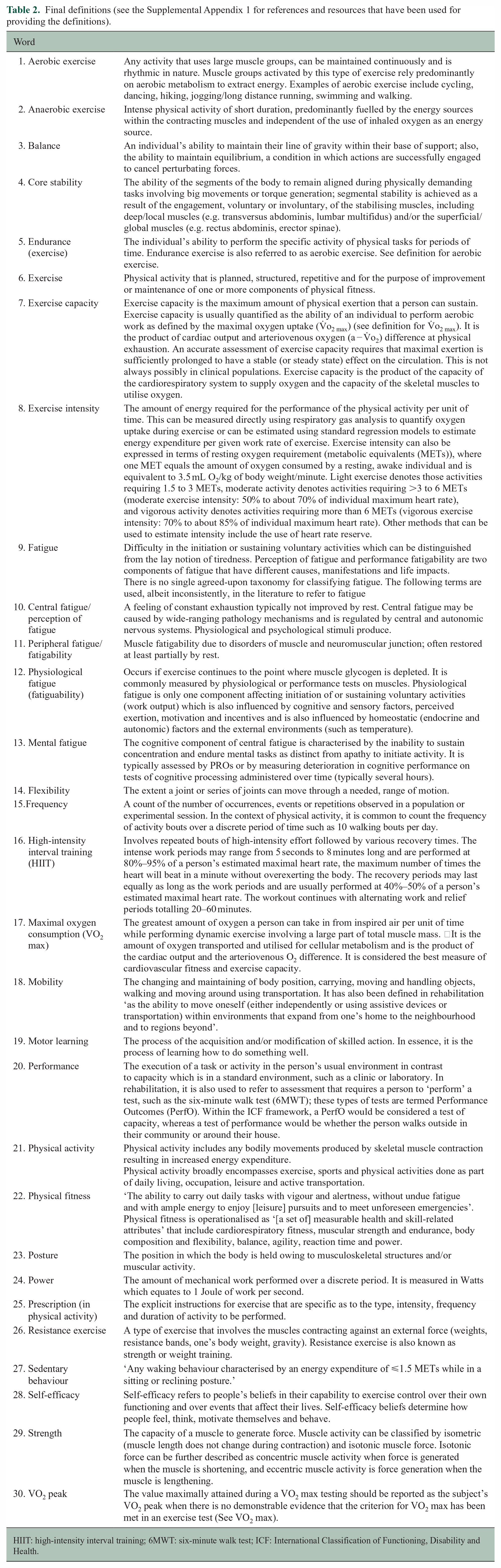
HIIT: high-intensity interval training; 6MWT: six-minute walk test; ICF: International Classification of Functioning, Disability and Health.
Discussion
Here, we set out to consider the terminology and definitions for core exercise terms and move towards internationally shared vocabulary in MS exercise research for exercise scientists, clinicians and pwMS and those involved in their care. In this study, we established majority agreement in vocabulary for 30 terms. There was complete (100%) agreement from the expert reviewers in the three terms’: resistance exercise, balance and physical activity. There was good agreement (>75%) in the majority of terms, with the lowest agreement for the terms ‘posture’ (60%) and ‘exercise’ (65%). However, there was still extensive discussion at the consensus development and the MoXFo steering group panels on the final agreed terminologies. These discussions included debates about the nuances of specific terms, such as their definitions and appropriate usage, as well as considerations of the cultural and linguistic differences that might affect their interpretation. In addition, there were also discussions around the inclusion or exclusion of certain terms, with some experts arguing for the inclusion of additional terms to provide a more comprehensive vocabulary for MS exercise research. Ultimately, after careful consideration of all viewpoints and extensive deliberation, we propose that this paper provides initial information about definitions to be used, but that further systematic methodology is needed to identify comprehensive definitions for the field.
MS is a complex neurological disorder affecting millions worldwide and involving multidisciplinary teams. Unfortunately, this has resulted in a lack of unified terminology and underlying definitions, leading to confusion, miscommunication and misunderstandings. Having clear definitions for terms makes it easier for healthcare professionals to communicate with each other and patients. It also ensures that pwMS receive accurate information about their condition. Without a unified terminology, healthcare professionals may use different terms to describe the same concept, leading to imprecise treatment and communication. Hence, we recommend that researchers clearly reference or state definitions of their terms so that data can be appropriately combined in meta-analyses. There were some notable important gaps, where we were unable to recommend terminology, such as anaerobic capacity and intensity, where further work is needed. It was also hard to agree when fundamental differences existed, such as the observed difference in understanding of the word ‘intensity’ across clinical and research teams. We propose that this important fundamental work still needs to be performed.
Our approach has limitations, whereby we set out to harmonise terminology across a range of disciplines, with completely different training backgrounds, which led to some disagreement in the level of detail required, or definitions that should be used. There is inevitable bias in the inclusion of experts, although we attempted to invite experts across a wide geography and expertise. We used a final harmonisation process, which inevitably led to some bias in decision-making, although a consensus panel, including the MoXFo steering group, was used for the final agreement.
While considering the limitations in our approach, we do propose that there is an urgent need for researchers to include literature in systematic reviews and meta-analyses with confidence that they are synthesising appropriate interventions and measures. This is hard to do when fundamental differences exist, such as the observed difference in understanding of the word ‘intensity’ across clinical and research teams. There will be a number of terms that are not currently in common usage and new terms that will appear as the area evolves, and we propose that researchers proactively define these terms in research papers. We request that editors encourage that terminology is either clearly defined or referenced in order to increase confidence in the interpretation of research findings and research efficacy in this area.
Supplemental Material
sj-docx-1-msj-10.1177_13524585231204460 – Supplemental material for The MoXFo Initiative: Using consensus methodology to move forward towards internationally shared vocabulary in multiple sclerosis exercise research
Supplemental material, sj-docx-1-msj-10.1177_13524585231204460 for The MoXFo Initiative: Using consensus methodology to move forward towards internationally shared vocabulary in multiple sclerosis exercise research by Maedeh Mansoubi, Yvonne Charlotte Learmonth, Nancy Mayo, Johnny Collet and Helen Dawes in Multiple Sclerosis Journal
Supplemental Material
sj-docx-2-msj-10.1177_13524585231204460 – Supplemental material for The MoXFo Initiative: Using consensus methodology to move forward towards internationally shared vocabulary in multiple sclerosis exercise research
Supplemental material, sj-docx-2-msj-10.1177_13524585231204460 for The MoXFo Initiative: Using consensus methodology to move forward towards internationally shared vocabulary in multiple sclerosis exercise research by Maedeh Mansoubi, Yvonne Charlotte Learmonth, Nancy Mayo, Johnny Collet and Helen Dawes in Multiple Sclerosis Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by the National Institute for Health and Care Research Exeter Biomedical Research Centre. Professor Helen Dawes and Dr Maedeh Mansoubi’s work is supported by the National Institute for Health and Care Research Exeter Biomedical Research Centre. Dr Johnny Collett is funded by the NIHR Oxford Health Biomedical Research Centre. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.