
Abstract
Background:
The use of interactive video games is expanding within rehabilitation. The evidence base is, however, limited.
Objective:
Our aim was to evaluate the effects of a Nintendo Wii Fit® balance exercise programme on balance function and walking ability in people with multiple sclerosis (MS).
Methods:
A multi-centre, randomised, controlled single-blinded trial with random allocation to exercise or no exercise. The exercise group participated in a programme of 12 supervised 30-min sessions of balance exercises using Wii games, twice a week for 6–7 weeks. Primary outcome was the Timed Up and Go test (TUG). In total, 84 participants were enrolled; four were lost to follow-up.
Results:
After the intervention, there were no statistically significant differences between groups but effect sizes for the TUG, TUGcognitive and, the Dynamic Gait Index (DGI) were moderate and small for all other measures. Statistically significant improvements within the exercise group were present for all measures (large to moderate effect sizes) except in walking speed and balance confidence. The non-exercise group showed statistically significant improvements for the Four Square Step Test and the DGI.
Conclusion:
In comparison with no intervention, a programme of supervised balance exercise using Nintendo Wii Fit® did not render statistically significant differences, but presented moderate effect sizes for several measures of balance performance.
Keywords
Introduction
It is widely recognised that many people with multiple sclerosis (MS) have impaired balance that may lead to falls. Impaired balance may be present even if the person performs well on commonly used clinical balance tests. 1 An incidence of accidental falls ranging from 48–63% has been reported, 2 -5 and fall tendency may also be present early after onset of MS. 6 It has been suggested that several factors may be involved in reasons why a person loses his or her balance, for example dual-task conditions that stress the ability to divide attention, 7 -9 spasticity, 4,10 sensory impairments, 11,4 and the need to use an assistive device when walking. 4,12 Slowed somatosensory conduction and impaired central integration lead to changes in postural control, which may also induce falls. 5,13 . In addition, fatigue and heat-sensitivity, which aggravate other symptoms, have been identified as being related to accidental falls. 7 Balance and walking abilities are intimately related, and most falls occur during walking activities 4 and are due to tripping or slipping. 14 Thus, considering the number of people with MS who, for a large part of their lives, have balance problems and risk incurring injurious falls, there is a need to develop interventions that maintain and/or improve balance and reduce injurious falls.
The number of studies of the effects of interventions aiming to improve the balance of people with MS is limited. Tailored programmes with focus on vestibular rehabilitation including both motor and sensory strategies were found to improve balance performance, reduce the incidence of falls and disability. 15,16 However, such programmes require feedback from a therapist, and it is likely that the programmes should be implemented on a regular basis in order to maintain gains achieved. The latter adds the challenge of implementing balance programmes that are likely to keep people with MS involved in performing the programme on a regular basis. In response to this need, new ways of promoting exercise are evolving. One way might be to use interactive video games, which are becoming increasingly popular for different target groups. The scientific base regarding the use of new and perhaps fun ways to exercise using interactive video games is growing. Improvements in balance have been reported for elderly people 17 and for persons with acquired brain injury, when comparing the Nintendo Wii Fit® Balance board with traditional rehabilitation therapy. 18 Increased postural stability was found in a case study including three patients with cerebral injuries. 19 A systematic review found limited evidence for interactive video games compared with conventional rehabilitation for stroke survivors. 20 To our knowledge, only one study has investigated the use of a Nintendo Wii Fit® Balance Board among people with MS. Plow and colleagues investigated whether exercising at home using Nintendo Wii Fit® would change behaviour and increase physical activity and health. 21 The midway assessment after 7 weeks showed improvements of balance and strength but the overall physical activity behaviour had returned to baseline after the 14-week intervention was completed.
There is thus limited evidence regarding the effects of intervention using the Nintendo Wii Fit® balance exercise programme on balance and walking in people with MS. Furthermore, improved balance performance should have an effect outside training, for example, on gait, walking, and reducing falls, in order to be worth the investment in time and effort. Given the large number of people with MS with imbalance, we intended to investigate whether an exercise programme using the specific balance section of the Nintendo Wii Fit® would improve balance performance and walking.
The aim of the present study was to evaluate the effects of a 6–7-week Nintendo Wii Fit® balance exercise programme on balance performance and walking ability in people with MS compared with no exercise. The hypothesis was that, after completion of the programme, balance performance and walking ability would have improved and be significantly better in comparison with no exercise.
Patients and methods
Those eligible for the study were people with MS in accordance with the revised McDonald criteria. 22 The inclusion criteria were: (a) reported, subjectively perceived impaired balance function in standing or walking activities; and (b) the ability to walk 100 m without resting. The exclusion criteria were: (a) cognitive or linguistic problems with understanding instructions or filling in self-administered outcome measures; (b) ongoing exacerbation of MS; or (c) other disease interfering with either intervention or testing procedures. The participants were not to receive physiotherapy targeting imbalance prior to or during the study, but were otherwise not restricted in their activities. A weight limit of 140 kg was used due to restrictions stated by the producer of the Nintendo Wii Fit® balance platform. The study followed the Helsinki Declaration and was approved by the Regional Ethical Committee in Uppsala-Örebro (Dnr 2010/263).
A multi-centre randomised controlled trial with random (1:1) allocation to exercise group or non-exercise group was conducted. The study was registered in FoU i Sverige, the Swedish clinical trials database (ID 48641) and Clinical Trials.Gov (ID NCT 01299025).
Participants were identified from those registered with the Swedish MS Registry or from being known at one of the participating centres, which were located in four county council areas, both rural and urban. Potential participants received a letter informing them about the study and inviting them to participate, along with a consent form. Within 2 weeks, they were also contacted by phone. Those fulfilling the inclusion criteria were enrolled by a physio therapist (PT), who also performed the tests prior to group allocation. A statistician not connected with the study conducted a computerised random allocation sequence with varied block sizes. Concealment was achieved by using sealed envelopes that were opened by another PT, who directly set up a Wii profile for those randomised to the balance exercise group. The participants were then allowed to familiarise themselves with how to use weight shifting to play the games. An appointment was then scheduled for the next visit, when the actual intervention period started. The second data collection was conducted about 1 week after completion of the intervention; that is, approximately 7–8 weeks after the first data collection. PTs collecting the data were blinded to allocation.
Intervention
The intervention consisted of individual PT-supervised sessions of 30 min of balance exercise using Nintendo Wii Fit Plus® twice a week for 6–7 weeks, with a total of 12 sessions. The Wii Fit Plus® is a video exercise game containing balance games, yoga poses, strength training and aerobics. Games in the Wii Fit Plus® that targeted balance were selected by the authors and ranked, in order to standardise the progression of exercises. The player stands on a Wii Balance Board that detects centre of balance. The exercises focus on controlling the games using the player’s centre of balance. The first session started with the games categorised as easier (Penguin Slide, Ski Slalom, Perfect 10, Heading, Table Tilt). During all sessions, the PTs encouraged the participants to progress to more difficult games (Tightrope Tension, Balance Bubble, Snowboard Slalom, Skateboard Arena, Table Tilt+, Balance Bubble+). The participants had the opportunity, however, to choose the games that they enjoyed the most. In the games, a player starts at basic level and, when a certain score is reached, the player is transferred to a more advanced level. The intervention was, therefore, tailored to suit each participant’s ability and preferences. The PTs were in charge of the remote control in order to maximise intensity. They also registered the games played, time (in minutes) needed to rest during sessions and made notes of the spontaneous comments regarding the progression. Participants in the non-exercise group were invited to start exercising using Nintendo Wii Fit Plus® after the second data collection.
Outcomes
The outcome measures were chosen to cover both self-reported and more objectively measured changes. The balance tests were thought to reflect daily activities such as transfers, stepping in different directions and walking. Both clinically administered and self-administered outcome measures were used in a standardised order (as listed below) using a protocol. The data collectors were trained prior to the start of the study, in order to ensure consensus in measuring and judging the participants’ performance. Potential visits (not focusing on balance) to PTs before and during the study period and self-reported physical activity were registered. The participants reported the impact of MS using the MS Impact Scale (MSIS-29) 23 since, in some cases, updated Expanded Disability Status Scores were not available. The MSIS-29 contains 29 items divided into MS-related physical and psychosocial problems, and gives subscale scores as well as a total score (0–100). The scale is valid and reliable. 24 Demographic data and information on MS type were verified from medical charts.
The primary outcome was the Timed Up and Go test (TUG), which registers the time taken to rise from a chair, walk 3 m, turn, walk back, and sit down again. 25 One practice attempt is permitted before performing the test. The test–retest reliability is very good at 0.91, and a single test attempt is sufficient. 26
Secondary outcomes were the Timed Up and Go cognitive test (TUGcognitive), the Four Square Step Test (FSST), the 25-Foot Walk Test (25TW), the Dynamic Gait Index (DGI), the 12-item MS Walking Scale (MSWS-12), the Activities-Specific Balance Confidence Scale (ABC) and the Timed Chair Stand test (TCS).
TUGcognitive is a dual-task measure, in which the person repeatedly subtracts 3 from a randomly chosen number while performing the TUG. 27
The FSST measures the ability to step over 2.5 cm-high sticks. 28 The sticks are placed as a cross on the floor and the person steps forwards, sideways and backwards in a pre-determined sequence, while time needed is recorded. Although initially created for predicting falls in older adults, it has also been used for people with MS, with a cut-off of 16.9 s giving a positive predictive value of 81% for falls. 4
The 25TW, which is known to be a valid and reliable measure for people with MS, 29,30 was used to measure walking velocity. A stationary start was used, and the participants were asked to walk quickly but safely.
The DGI was used to measure dynamic balance while walking, using eight items, where the PT grades the quality of performance from 0–3. 31 A high score indicates better performance. Inter-rater reliability is good when used on people with MS. 32
The MSWS-12 is a self-administered scale for rating MS-related limitations in walking ability during the previous 2 weeks. 33 A score is calculated ranging from 0 (not at all limited) to 100 (extremely limited). It is a valid and responsive scale. 34
The ABC measures how confident a person is in performing 16 different activities without falling, with scores ranging from 0 (not at all confident) to 100 (confident). 31 Both inter-rater (ICC = 0.92) and test–retest (0.80) reliability are good for people with MS. 35
Functional strength and balance were measured using the TCS. Time is registered for a sequence of 10 sit-to-stands from a chair, with the use of armrests being allowed. 36 Validity has not been established for people with MS.
Sample size was calculated based on the TUG, alpha-level at p = 0.05, an 80% power to detect clinically significant difference between groups (3 s) and a standard deviation of 4 s, suggesting a sample size of at least 70 participants. A difference of 3 s was based on the assumption that it would reflect an approximate 20% decrease in time to perform the TUG. 26 To account for possible dropouts, we aimed to enrol at least 80 individuals.
Statistical methods
Non-parametric statistics were used due to data not-normally distributed and per protocol analyses were conducted. Fisher’s exact test was used for dichotomous variables, a chi square exact test for non-ordered categorical variables and the Mann–Whitney U test for continuous variables. The Wilcoxon signed-rank test was used for comparison within groups and the Mann–Whitney U test for comparison between groups. Effect sizes were calculated. The significance level was set to p ≤ 0.01 not to overrate the importance of changes over time.
Results
The study sample consisted of 84 people with MS (Figure 1). Data collection started on 13 September 2010 and ended on 20 July 2011. Some 40 persons were enrolled in Örebro, 20 in Västerås, 14 in Eskilstuna and 10 in Karlstad. Four participants were lost to follow-up: one started a rehabilitation period elsewhere; one perceived worsening of symptoms; one declined follow-up; and one was lost for administrative reasons.
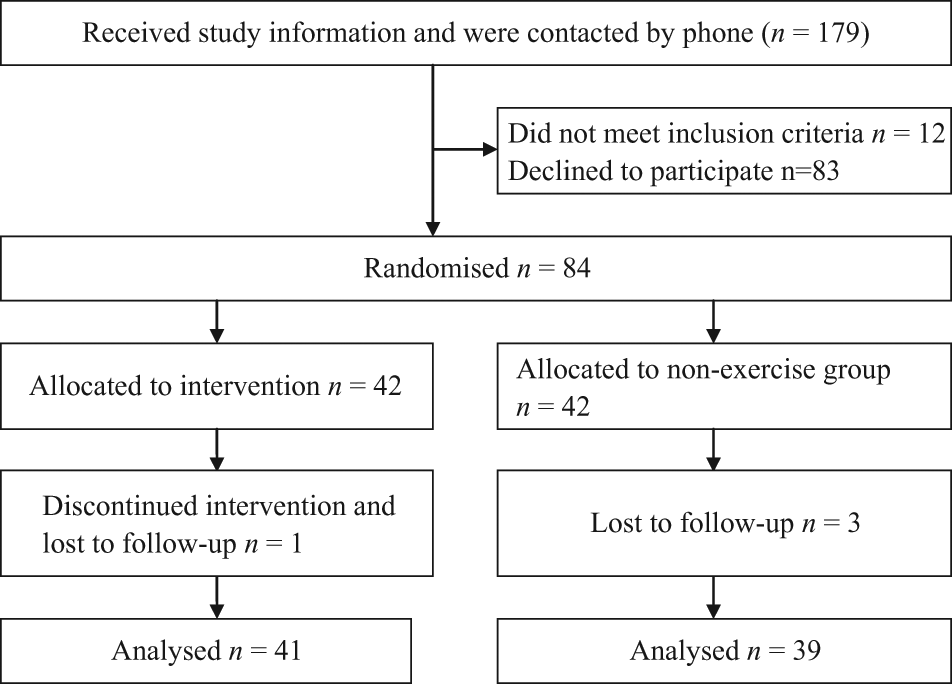
Flow chart.
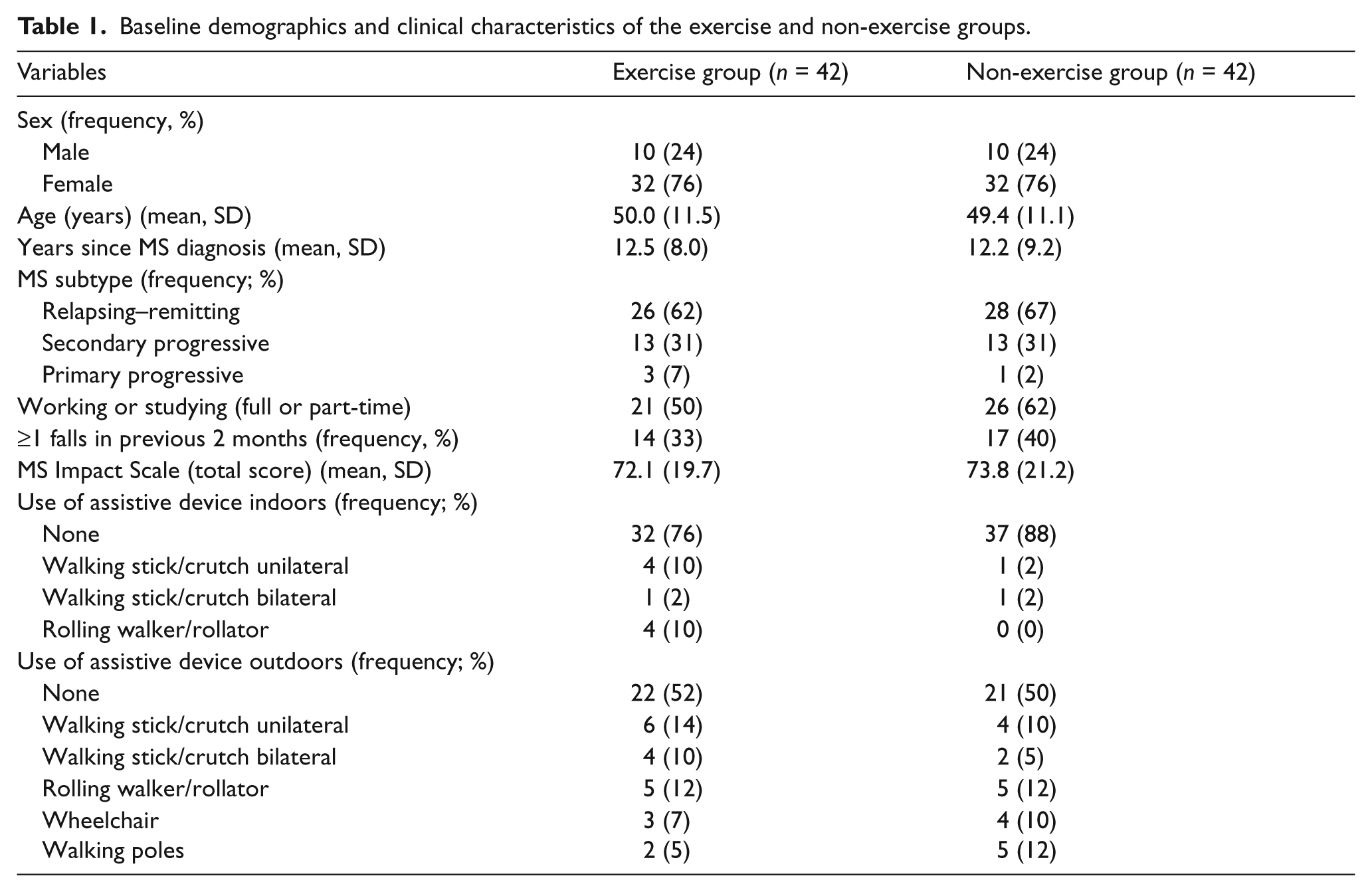
The groups were similar at baseline (Table 1).
Baseline demographics and clinical characteristics of the exercise and non-exercise groups.
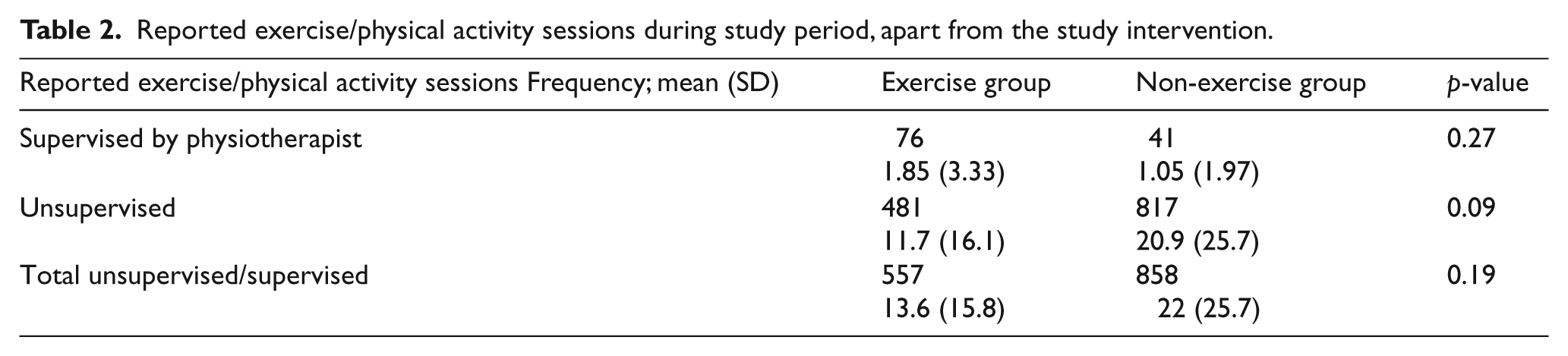
The groups differed in terms of frequency of self-reported exercise/physical activity (apart from the intervention) during the study period, though this was not statistically significant (Table 2).
Reported exercise/physical activity sessions during study period, apart from the study intervention.
Compliance with the balance exercise was excellent. One person completed 11 sessions of exercise, and the others all 12 sessions. Two persons were unable to perform the FSST and one could not perform the TUGcognitive. At the final data collection, the balance exercise group reported 10 falls during the study period compared with 14 in the non-exercise group. No falls occurred during balance exercise, data collection or travelling to or from the appointments. No other adverse events were reported. The participants expressed that they felt successively better at performing the games, and this was confirmed by the PTs. The need to sit down and rest during balance exercise decreased during the study period from mean 2.3 (SD 3.9) min to mean 1.6 (SD 3.6) min (p < 0.08) and the participants managed to play at more difficult levels. There were no statistically significant differences between groups after the intervention period in the primary outcome TUG or in any of the secondary outcomes (Table 3).
Mean (SD), median (min; max) reported for baseline and follow-up and within and between groups comparisons using p-values and effect sizes.
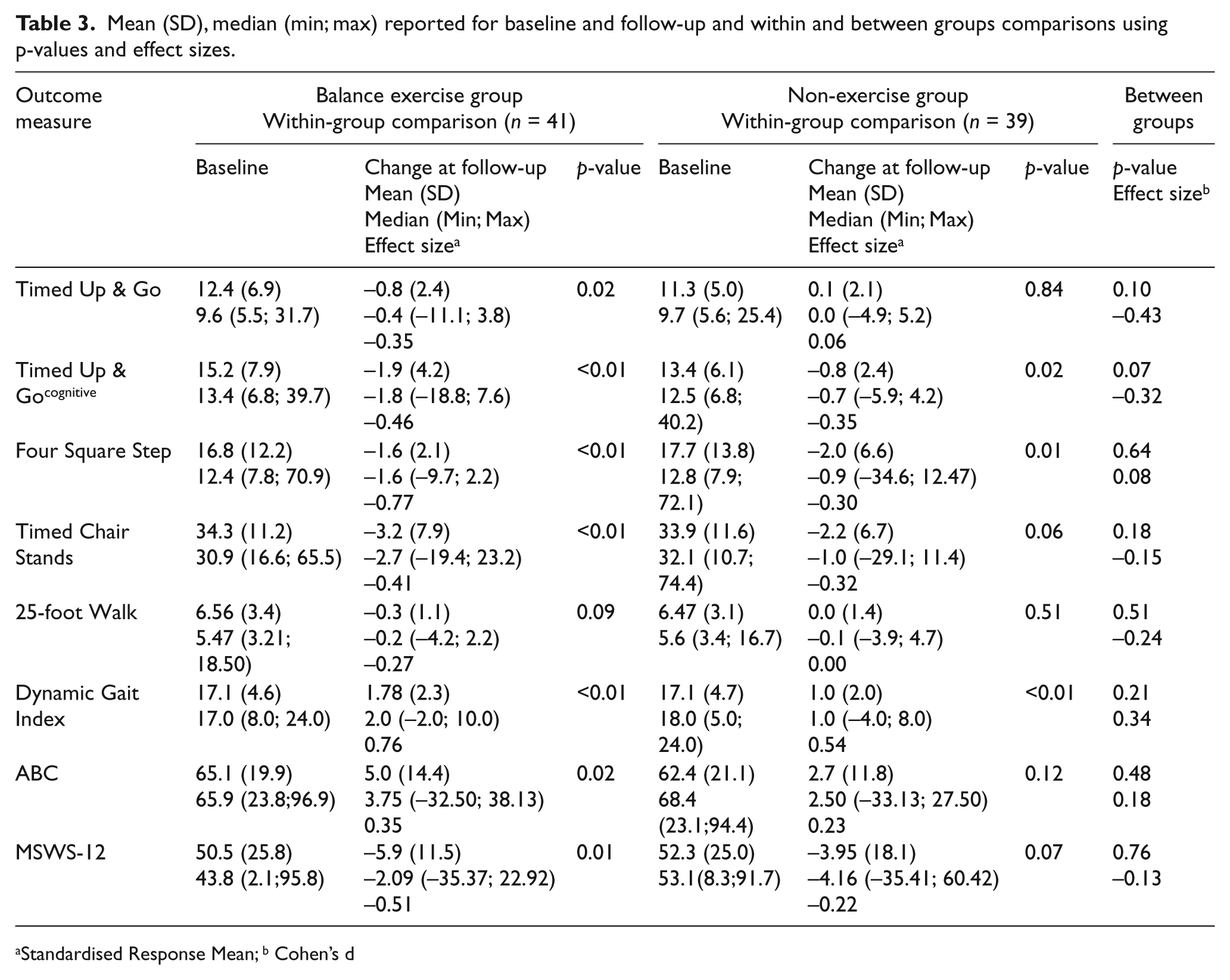
Standardised Response Mean; b Cohen’s d
In Table 3, the within-group analyses and effect sizes of the changes are presented. In the exercise group, there were significant improvements in the TUGcognitive, the FSST, the TCS, the DGI and the MSWS-12 (all p ≤ 0.01). The non-exercise group had significant improvements in the FSST and the DGI (both p ≤ 0.01). The effect sizes were large for the FSST, the DGI and, the MSWS-12 in the exercise group and moderate for all the other tests except for 25TW.
Discussion
To our knowledge, this is the first randomised controlled multi-centre trial of the effect of a 6–7-week Nintendo Wii Fit® balance exercise programme on balance performance and walking ability in people with MS. Compliance with the balance exercise was excellent and both participants and PTs found the exercise stimulating, easy to conduct, and easy to persist with. Playing the games functioned as a self-trigger to continue the exercise.
There is no consensus on how often or for how long balance exercise should be given in order to achieve a substantial change. In the present study, the following factors were considered: previous recommendations for strength or endurance exercise for people with MS, 37 the possibility to participate from the patient’s perspective, and matching the clinical reality of resources if this intervention were to be given outside a study protocol. It is likely that a more intense exercise regime would result in more improvements.
After completion of the programme, there were no statistically significant differences between the balance exercise group and the non-exercise group in the primary or secondary outcomes. The lack of difference in the primary outcome between the groups may be explained by the fact that the participants in the non-exercise group appear to have been more frequently physically active than the balance exercise group. It is noteworthy that only the balance exercise group reported significantly fewer perceived limitations in walking.
The fact that there were improvements in the balance exercise group that were not present in the non-exercise group might indicate achievements specific to the exercise programme. The two outcomes that did not improve after the completion of the Nintendo Wii Fit® Balance exercise programme were the TUG and the Timed 25-Foot Walk. On the other hand, there were improvements in the TUGcognitive, which is basically the same test but plausibly more sensitive and less likely to have a ceiling effect, which is an advantage when applied to a group of people with MS with good walking capacity, as in the present study. In agreement with other studies of the effect of exercise programmes using Wii games for people with MS or the elderly, there were improvements in balance performance. 17,18,21 In the present study, however, improvements were also noted in self-reported outcomes such as the MSWS-12 that is the self-perceived limitation of walking ability in MS. The MSWS-12 might possibly be considered an indicator of walking ability in everyday life, which suggests that a transfer of gains to the participants’ everyday life had occurred.
It is important that statistically non-significant results are also reported, in order to be able to draw systematic conclusions concerning treatment effects. The strength of this study is the design, levelling out differences at baseline. There were no deviations from the random allocation, and all participants allocated to the experimental group started the intervention. Follow-up data were collected for 95% of those enrolled, and data were only incomplete for a few participants that were not able to perform one or two tests. Blinding of the participants or of the PTs performing the intervention was not possible, but those collecting data were blinded to group allocation and pre- and post-measurements for each participant were taken by the same person. If a treatment effect is shown in a multi-centre study, the generalisability increases. It has, nevertheless, been reported that multi-centre trials show fewer treatment effects compared with single-centre trials. 38 To ensure that the intervention was equally distributed, protocols were printed and all PTs met for training and discussion of how to administer the intervention. The research leaders were available for questions throughout the study. It is possible that a single-centre study design would have included a more homogenous study sample with less variation in delivering the treatment, although a sufficiently large sample would not have been possible with a single-centre approach in this case. The positive changes within the balance exercise group are difficult to ignore and subgroup analyses are tempting, although the a priori power calculation would be ignored.
Study limitations
Approximately 50% of those eligible for the study agreed to participate. Reasons for declining participation included comments about the difficulty of combining exercise with work. The external validity of the study is thus limited to those both meeting the inclusion criteria and with an interest in and practical possibilities to take part in an exercise programme. There was a lack of control over activities performed outside the protocol. The physical activity levels were not comprehensively measured but relied on self-report. Several participants in the non-exercise group expressed disappointment when not randomised to the balance exercise group, and spontaneously commented on how they had now found motivation to exercise on their own, which was possibly emphasised by the fact that they were to be followed-up 2 months later. The non-exercise group reported twice the frequency of unsupervised exercise during the study period compared with the balance exercise group. This difference between the groups in level of unsupervised activities during the study had not been anticipated, and was not adjusted for when calculating the sample size. From a clinical perspective, it is interesting to note that a planned follow-up without intervention might motivate people to start exercising.
The sample size estimation was based on TUG, with a potential standard deviation of 4 s. The sample was more heterogeneous than expected in this perspective, with a standard deviation of 6 s. This resulted in reduced power to detect a true difference, which may have caused a type-II error. In fact, a post-study calculation revealed that a sample with 100 people in each group would have been needed to detect a true difference. It is quite possible that the TUG was not appropriate, since approximately 14% of the sample performed TUG ≤ 7 s. Using measures for postural control, such as lateral or forward reach test or postural sway in different conditions, might have revealed more differences in favour of the balance exercise group.
The PTs providing the balance exercise agreed that the participants appeared highly motivated during exercise. Interactive video games seem to provide an enjoyable way to exercise, which is in line with the aim of increasing physical activity level in general and for people with MS in particular. Interactive video games may be used to stimulate physical activity. We suggest that different interactive video game interventions should be further investigated, since they may provide an easily accessible way to exercise and remain physically active and improve balance function. Interventions that combine the balance board with exercises that require stepping and walking may be more effective than using the balance board alone. Interactive video games can be used to target several areas of interest in MS care apart from balance performance, such as endurance, body awareness, strength, etc.
Conclusion
In comparison with no intervention, a programme of supervised balance exercise using Nintendo Wii Fit® presented moderate effect sizes for several measures of balance performance. A combination of the Nintendo Wii Fit® Balance board as home exercise and supervised physiotherapy may be a future approach to consider.
Footnotes
Acknowledgements
Thanks are due to the assisting PTs: Anna Carling, Department of Physiotherapy at University Hospital, Örebro; Steven Allen, Brickegårdens Primary Health Care Centre; Anna Lövgren and Kerstin Eriksson, Nora Primary Health Care Centre; Malin Andreasson and Helena Vesterlin, NeuroRehab at Mälarhospital in Eskilstuna; Ingmarie Westlund and Ingrid Lundström, Rehabclinic at Västerås hospital; and Lena Sanner and Malin Nilsson, Rehabunit at the Central Hospital in Karlstad.
Funding
This work was funded by the Uppsala-Örebro Regional Research Council, the Research Committee of Örebro County Council, and the Norrbacka-Eugenia Foundation.
Conflict of interest
The authors declare that there are no conflicts of interest.