
Abstract
Background:
Progressive forms of multiple sclerosis (MS) affect more than 1 million individuals globally. Recent approvals of ocrelizumab for primary progressive MS and siponimod for active secondary progressive MS have opened the therapeutic door, though results from early trials of neuroprotective agents have been mixed. The recent introduction of the term ‘active’ secondary progressive MS into the therapeutic lexicon has introduced potential confusion to disease description and thereby clinical management.
Objective:
This paper reviews recent progress, highlights continued knowledge and proposes, on behalf of the International Progressive MS Alliance, a global research strategy for progressive MS.
Methods:
Literature searches of PubMed between 2015 and May, 2021 were conducted using the search terms “progressive multiple sclerosis”, “primary progressive multiple sclerosis”, “secondary progressive MS”. Proposed strategies were developed through a series of in-person and virtual meetings of the International Progressive MS Alliance Scientific Steering Committee.
Results:
Sustaining and accelerating progress will require greater understanding of underlying mechanisms, identification of potential therapeutic targets, biomarker discovery and validation, and conduct of clinical trials with improved trial design. Encouraging developments in symptomatic and rehabilitative interventions are starting to address ongoing challenges experienced by people with progressive MS.
Conclusion:
We need to manage these challenges and realise the opportunities in the context of a global research strategy, which will improve quality of life for people with progressive MS.
Introduction
Multiple Sclerosis (MS) is a growing global neurological challenge affecting 2.8 million individuals worldwide. 1 A large proportion of these individuals either live with a relapsing form (RMS) and/or a progressive form of MS—the latter either Primary Progressive MS (PPMS) which is progressive from the outset, or Secondary Progressive MS (SPMS). Arriving at a precise global estimate of the prevalence of progressive forms of MS remains difficult. Prior to the availability of disease-modifying treatments, natural history studies of MS estimated that 50% of individuals diagnosed with RMS would transition to SPMS within 10 years of initial diagnosis and 90% would transition to SPMS within 25 years of initial diagnosis.2–5 In addition, it is estimated that 15% of individuals are diagnosed with PPMS. 6 Taken together it is reasonable to conclude that in excess of one million individuals globally currently live with one of the progressive forms of the disease.
Since publication of the International Progressive MS Alliance’s initial scientific strategy statement in 2012, we have seen the achievement of a significant milestone—approval of the first MS treatments for progressive disease, ocrelizumab (for PPMS) and siponimod (for active SPMS).7–9 While these agents demonstrated modest efficacy with respect to confirmed time to disability progression, their addition to the clinician’s toolbox nonetheless signals a hopeful start to a potential new therapeutic era—similar to that previously seen in relapsing MS. In addition, observational studies support the possibility that intervention with disease-modifying treatments can reduce the risk of transition from RMS to SPMS and improve disability outcomes in patients with active SPMS.10,11 Together, these developments point to the prospect that therapeutic interventions can alter the natural history of the disease and improve outcomes for those individuals concerned about developing or living with SPMS.
Despite positive developments in the field, major gaps persist in both the treatment and management of progressive disease. 12 Over the past 5 years, the emergence of global engagement and collaboration of many stakeholders to address these challenges has been a welcome development. Collective efforts by the International Progressive MS Alliance, national patient organizations, government, and industry together with researchers and clinicians have drawn much needed attention to the challenges of progressive MS. Although this effort has catalyzed scientific progress, much work remains to address the remaining scientific gaps so that people with progressive MS can have access to a robust therapeutic toolbox of pharmacological and non-pharmacological interventions.7,13
In this paper, we review recent progress, highlight continued knowledge, and propose, on behalf of the International Progressive MS Alliance, a global research strategy for progressive MS.
Progressive MS—a persistent clinical challenge
Identifying the onset of progressive MS in the individual patient remains a clinical challenge. Currently, this determination is made retrospectively using a combination of assessments by a skilled clinician.14,15 Currently, we lack effective tools to prospectively assess if and when an individual transitions from relapsing to progressive MS but there are emerging efforts to leverage large patient databases to develop algorithmic tools to aid clinicians.16,17 Moreover, advances in our understanding of the pathophysiological mechanisms of the disease suggest that multiple pathogenic mechanisms are present in an individual patient at any given time and that these mechanisms are expressed clinically with some variability. Thus, in an individual patient, the onset of progressive MS most likely begins close to a confluence of two major factors: (1) the accumulation of CNS damage, due to inflammatory disease mechanisms, combined with (2) an accumulation of neuroaxonal damage that overwhelms extant CNS compensatory mechanisms (Figure 1). The precise point at which an individual patient enters clinically apparent progressive disease and the rate of progression will vary, depending on a number of moderating factors. These include biological sex, gender, race, comorbidities, possibly genetic factors, and utilization of disease modifying treatments (DMTs) along with the aging process.18,19 There is also some evidence that the onset of progression does not take place at the same time in different central nervous system pathways and areas, nor do we fully appreciate how sustained immunotherapy influences this process.10,20,21
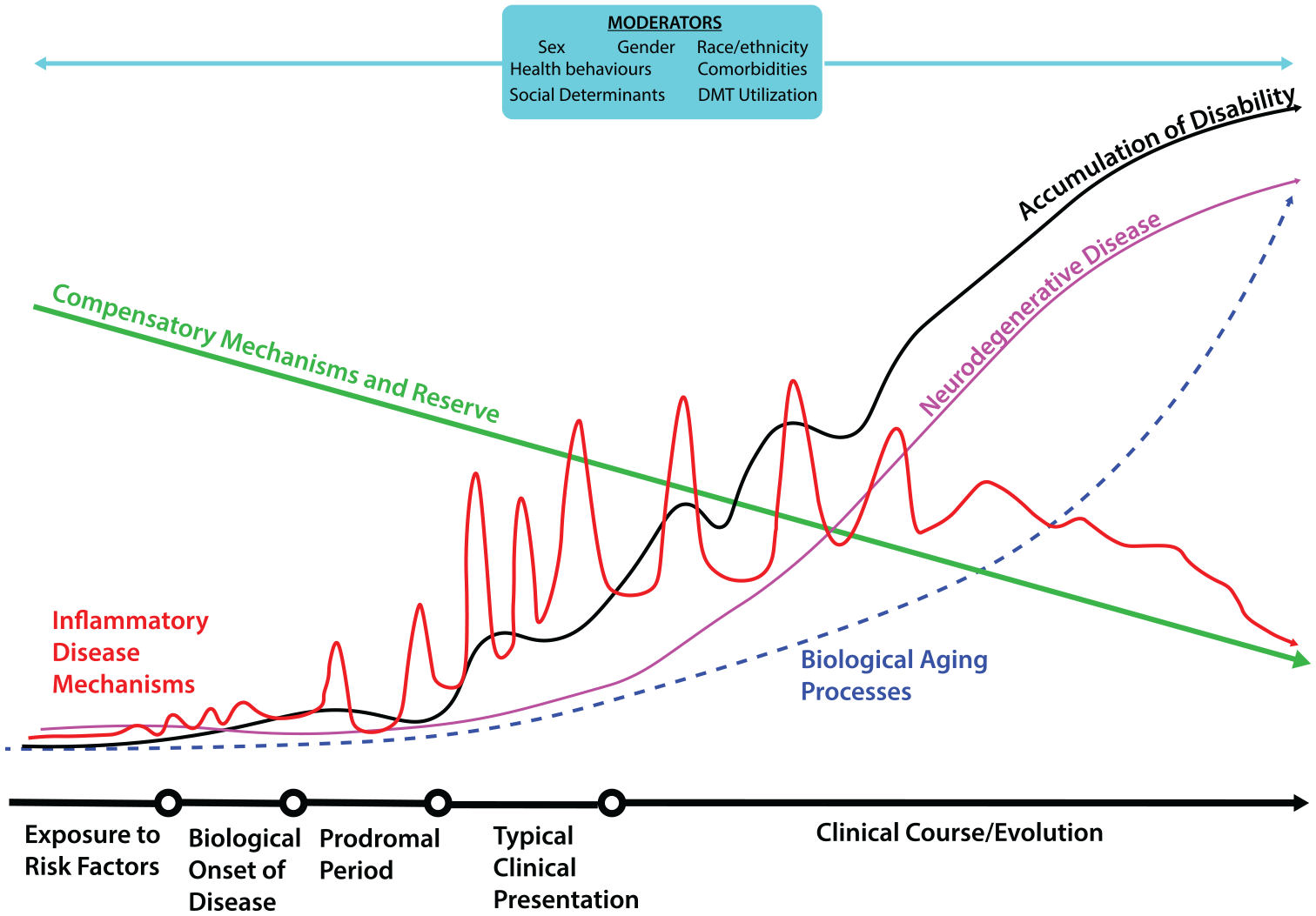
Pathways influencing development of progressive MS: The accumulation of disability and development of progressive MS likely reflects a combination of factors including damage arising from inflammatory disease mechanisms, neurodegenerative mechanisms, and biological aging. These processes are likely attenuated by compensatory mechanisms and reserve during the early- to mid-stages of the disease, but over time these compensatory processes are depleted. Moderators such as sex, gender, socioeconomic status, and DMT utilization likely exert positive and negative influences on progression and the development of progressive MS.
Recent progress
Pathophysiological mechanisms
A better understanding of the mechanisms underpinning or moderating progression is fundamental to expanding the therapeutic repertoire. Recent efforts have revealed important new insights in aspects of immune-mediated inflammation and neurodegeneration. It is thought that in MS there are two types of inflammation. 22 One is characterized by acute focal invasion of immune cells giving rise to active demyelinated plaques in the white matter, and the other by slow formation of immune cell aggregates in connective tissues spaces such as the meninges and perivascular spaces. The latter type of inflammation gradually increases with disease duration and patient age. It is associated with subpial demyelinated lesions in the cortex, slowly expanding lesions in the white matter, and diffuse neurodegeneration in the white and gray matter.22–25
The role of the innate immune system is of interest with a particular focus on the control of pathological astrocytes by microglia.26–32 Recently, NOD-leucine rich repeat and pyrin containing protein 3 (NLRP3) inflammasome has been shown to be overactive in monocytes in PPMS, and canonical NLRP3 inflammasome activation with a combination of ATP plus lipopolysaccharide was associated with increased IL1-Beta production.31,33 The mechanisms underpinning progression, however, go far beyond inflammation and likely involve failure of normal maintenance and repair mechanisms, including remyelination. Mechanisms driving neurodegeneration include axonal loss and involve the interrelationship between demyelination, astrocyte pathology mitochondrial dysfunction, and neuronal vulnerability.30,34,35 Other factors such as the role of complement genes, biological aging as reflected in telomere shortening, and microstructural changes in the spinal cord are also being considered.18,36,37 Gray matter damage has also been implicated to the onset of the progressive phase and the development of disability.21,38–41
Tools—biomarkers, imaging modalities, functional measures
Another challenge is the absence of biomarkers signaling progression that are scientifically sensitive and specific enough to justify their use in phase II and phase III clinical trials. A major difficulty is disentangling how much of a change of a given biomarker is due to neurodegenerative mechanisms underlying progression or to acute inflammation driven by peripheral immune mechanisms. Several imaging markers have been explored to good effect in the Phase II trial of ibudilast, which evaluated gray matter atrophy and whole brain atrophy, along with advanced MRI measures including magnetization transfer imaging and diffusion tensor imaging.42,43 Recent studies have identified some potential biomarkers of progression: imaging biomarkers include slowly expanding lesions on brain MRI (which could be a correlate of smoldering demyelination and axonal loss in chronic active lesions) and changes in N-acetyl aspartate concentration, which indicates neuroaxonal integrity and mitochondrial function.39,44 Other approaches, including OCT and a revisiting of visual evoked potentials, are also being explored.45,46
The measurement of serum neurofilament light (NfL) has been assessed in a number of recent studies looking at both acute and chronic changes in MS.47–50 An association with the development of disability has been described. The growing body of evidence associated with NfL has also stimulated global efforts to determine its utility as a tool for drug discovery and clinical management of the disease.51,52 A critical aspect of this work is the need for longitudinal examination of patient cohorts to examine the utility of NfL in measuring progression independent of relapse activity. Recent work in natalizumab-treated patients illustrates this complexity and the need for careful consideration of NfL as a tool in clinical management of progressive MS. 53
Clinical trials of investigational drugs
Recent Phase III trials in progressive MS demonstrated that ocrelizumab in PPMS and siponimod in SPMS modestly reduced the risk of confirmed disability progression, while trials of the water soluble B vitamin, biotin, in PPMS and SPMS, and natalizumab in SPMS and fingolimod in PPMS, were unequivocally negative.54–58 However, if we are to have a major impact on progression we need to develop agents that provide neuroprotection and/or encourage repair, and here the picture is less clear. There have been a number of phase II trials of putative neuroprotective agents. The innovative multi-arm MS-SMART trial evaluated three agents, amiloride, fluoxetine, and riluzole, but showed no benefit of any of the therapies. An earlier study of fluoxetine was also negative.59,60 However, a recent study of ibudilast showed positive results on several imaging outcomes (see earlier section).42,43 Very recently, masitinib, an oral tyrosine kinase inhibitor that selectively targets mast cell activity and microglia activity, was reported to significantly reduce the risk of disability progression in a double-blind placebo controlled phase III study. 61 In addition to these advances, a review of ClinicalTrials.gov and World Health Organization International Clinical Trials Registry Platform (as of April 2021) found a number of ongoing clinical trials (Phase 0/I to Phase III) of agents and interventions in progressive MS. Given the considerable attrition associated with drug development, more trials would be desirable, but, nonetheless, this augurs well for the future (Figure 2).
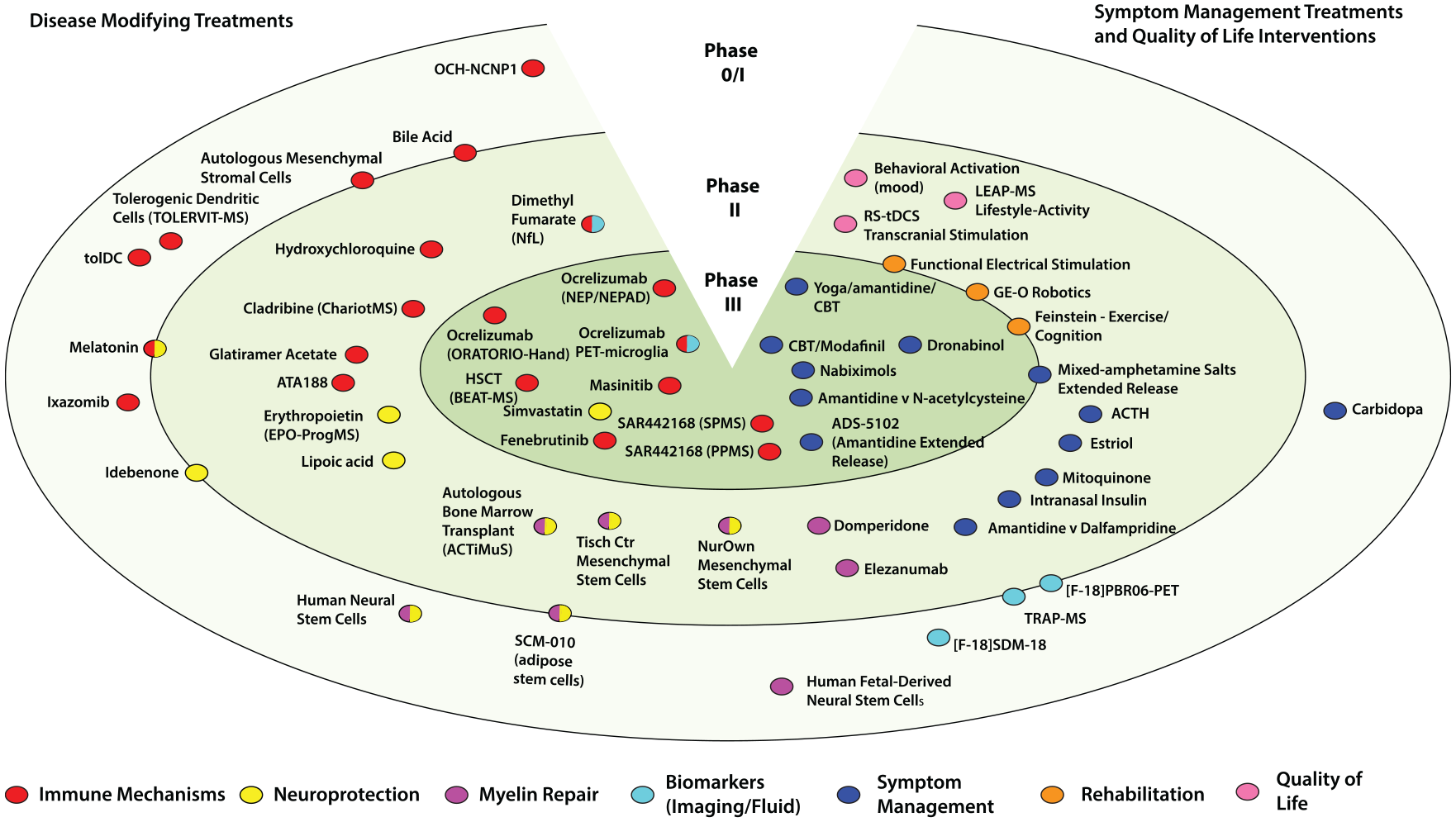
Progressive MS treatments in clinical development. Active clinical trials evaluating agents in progressive MS and registered with ClinicalTrials.gov or World Health Organization International Clinical Trials Registry Platform as of April 2021 are illustrated. Trials are positioned based on their stage of development and agent or intervention profile (disease modification or symptom management/quality of life). Phase 0/I studies are in the outermost ring, with Phase II and III studies reflected in the inner rings. Phase I/II and II/III studies are placed on the borders of the respective rings.
Rehabilitation and symptom management
Evaluating interventions in the fields of symptomatic management and rehabilitation in progressive MS remains a major challenge—as noted recently in a call for action by a work group convened by the International Progressive MS Alliance. 62 People with progressive MS are looking for rapidly translatable approaches that treat their disease now, while the longer term disease-modifying treatments are developed. Fortunately, there have been well constructed studies demonstrating for example the benefits to motor function from a very practical standing frame program; along with careful studies examining the benefits of exercise on fatigue as well as cognition.63–66 The last of these areas is currently being evaluated in an innovative multi-center international clinical trial. 67
Three areas requiring renewed focus and effort
Understand progression
A fundamental challenge in progressive MS is the continued poor understanding of the mechanisms initiating and perpetuating disease progression. This limitation hampers efforts to identify biologically plausible treatment targets that are essential for efficient drug discovery. Continued exploration of the fundamental mechanisms of disease, using both computational systems, animal models and human studies, will be required. This work would be stimulated by the establishment of robust data sharing platforms that leverage machine learning and related artificial intelligence tools to develop new insights into biological pathways contributing to progressive disease. Drug discovery networks—whether existing or new efforts—can build on these insights to identify new or repurposed agents with potential to treat progressive MS. Furthermore, the pipeline of new therapeutic agents may be expanded by careful, innovative design of short, efficient exploratory human clinical trials to provide insights into disease progression. They may also serve as an initial proving ground for agents suitable for later stage clinical trial strategies which can further expand the pipeline of agents to be tested in larger clinical trials. 68 An additional consideration would be the development of more biologically based descriptors of the clinical course of the disease. Efforts in this area are under way under the auspices of the International Advisory Committee on Clinical Trials in MS. 15
Accelerate clinical trials
Study design is a critical consideration for accelerating clinical trials of progressive MS treatments. The current two-arm clinical trial paradigm—while largely reasonable for relapsing MS agents—poses significant challenges for progressive MS trials, given the large numbers of patients that must be enrolled and the long duration required to ascertain a clinical effect, using conventional clinical outcome measures (e.g. Expanded Disability Status Scale). 69 One solution may be the use of adaptive, multi-arm, and multi-stage trial designs to evaluate multiple agents simultaneously and in a potentially more cost effective manner. 68 Encouraging examples of this are the MS-SMART trial of three agents in progressive MS and the recently launched OCTOPUS trial.59,70,71 A very recent innovation is the use of Simon (2 stage) trial designs to screen compounds for non-futility.72,73 This approach, while far from a definitive demonstration of effect, can act as an efficient screen to identify promising therapeutic candidates relatively quickly. Such efforts are welcome, perhaps even overdue, and should inspire similar efforts globally.
Another critical barrier is the lack of a validated biomarker or outcome measure to enable shorter phase 2 clinical trials. The development of treatments for relapsing forms of MS was revolutionized by the adoption of reduction in gadolinium enhancing lesions as a proof-of-concept measure in Phase 2 trials. A similarly powerful tool(s) is needed in progressive MS. Volumetric imaging measures such as whole brain atrophy or volumetric MRI percentage brain volume change are being used in clinical trials but these require long studies, typically 96 weeks, to detect measurable changes. Such lengthy timelines when compared to the shorter intervals required in relapsing trials (typically 24 weeks for a trial measuring reduction in gadolinium enhancing lesions) pose a significant challenge for investigators and companies seeking to move agents into Phase 3 trials in progressive MS.43,59,74
The development and validation of fluid biomarkers such as NfL as well as other imaging modalities should lead to shorter studies which accelerate and enable progress.49,52,75,76 Moreover, efforts such as the Multiple Sclerosis Outcomes Assessment Consortium (MSOAC), the global Patient Reported Outcomes Initiative for MS (PROMS), and the proposed EDSS plus will contribute to development of new or modified outcome measures, but additional efforts are needed.77–81 An intriguing possibility is the use of smartphone sensor-based digital outcome assessments. While still in the early stages, recent work demonstrated that an app-based tool—Floodlight PoC—along with a smartwatch accurately captured reliable and clinically relevant measures of functional impairment in MS, in this area points to a future where ubiquitous digital tools could be leveraged to enhance research and clinical care.82,83
Finally, the ongoing challenge of phenotypic classification of the disease continues to impact clinical trials of progressive MS agents. This challenge introduced a measure of confusion due to the differing applications of the 2013 clinical course descriptors used in the review and approval of ocrelizumab and siponimod by both the US Food and Drug Administration (FDA) and the European Medicines Agency and compounded by the FDA’s retroactively expanding approval of agents for RMS to include active SPMS.9,15,84 Coordination among regulatory authorities and the MS patient and clinician community, in relation to disease phenotypes, is essential if we are to avoid undue complexity and confusion in patient recruitment, trial design, and subsequent treatment approvals.
Improving wellbeing
The final area for global prioritization is improving the wellbeing of persons with progressive MS. Unfortunately, this area remains poorly addressed with considerable gaps in the development of novel rehabilitative and symptomatic interventions that can meaningfully enhance quality of life for persons with progressive MS. There are, nevertheless, an abundance of potential interventional targets in the domains of physical and cognitive health, emotional wellbeing, social support, and comorbidities (Figure 3). A welcome development is the recently launched CogEx clinical trial—the first multi-country, multi-arm, randomized, blinded, sham-controlled trial of cognitive rehabilitation and aerobic exercise. 67 Continued progress in these areas will require development of a coordinated global rehabilitation and symptom management research strategy with targeted initiatives in areas that have appropriate scientific readiness. Foundational efforts will also be needed to address areas requiring further development (e.g. methodological or workforce gaps). 62
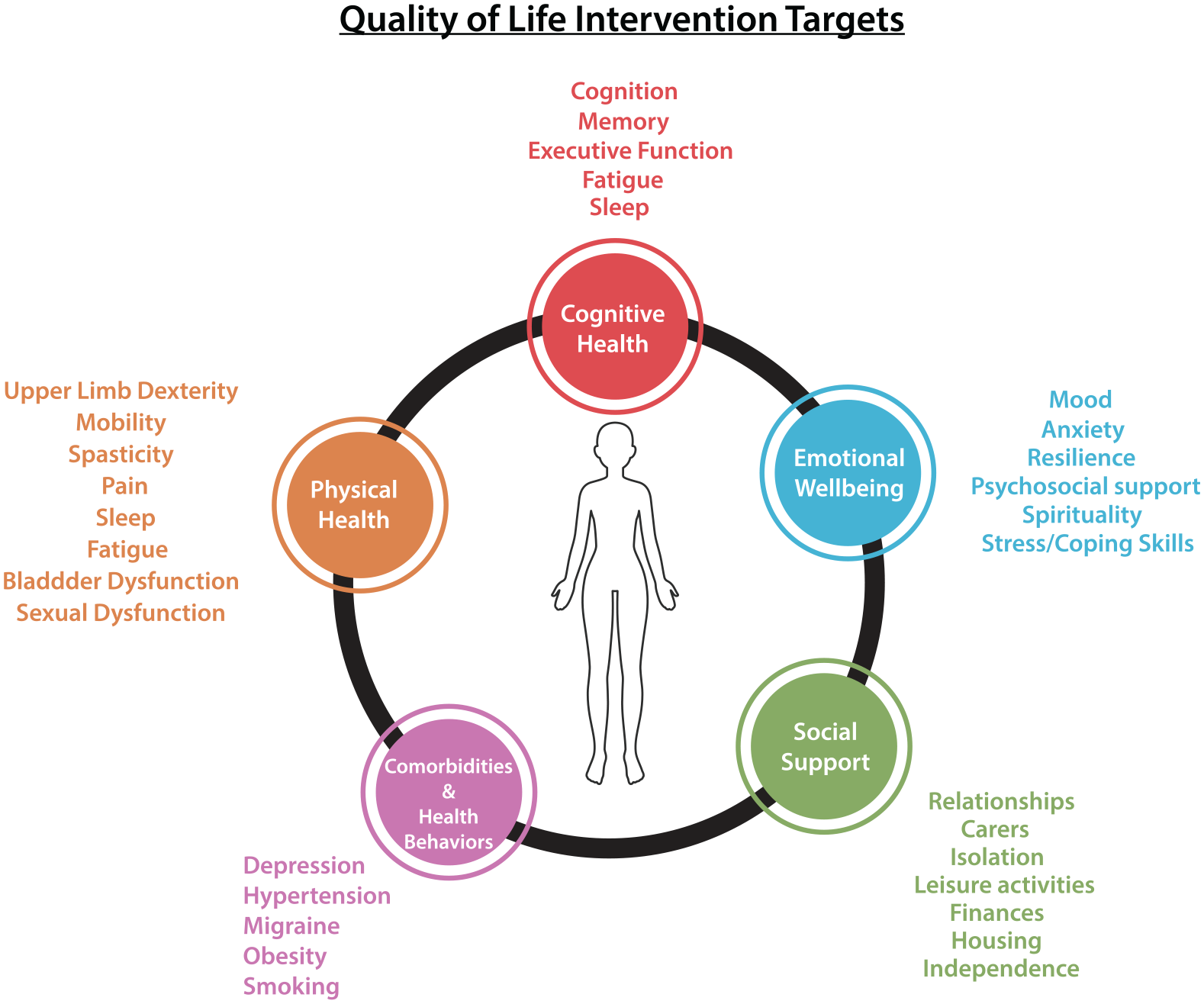
Quality-of-life intervention targets. Potential targets for quality-of-life interventions in progressive MS span several inter-related domains. While some are directly associated with disease mechanisms (e.g. cognition, pain) others are associated with other disease indications (e.g. hypertension) or social support mechanisms (e.g. care providers, housing) that affect quality of life.
Critical steps going forward
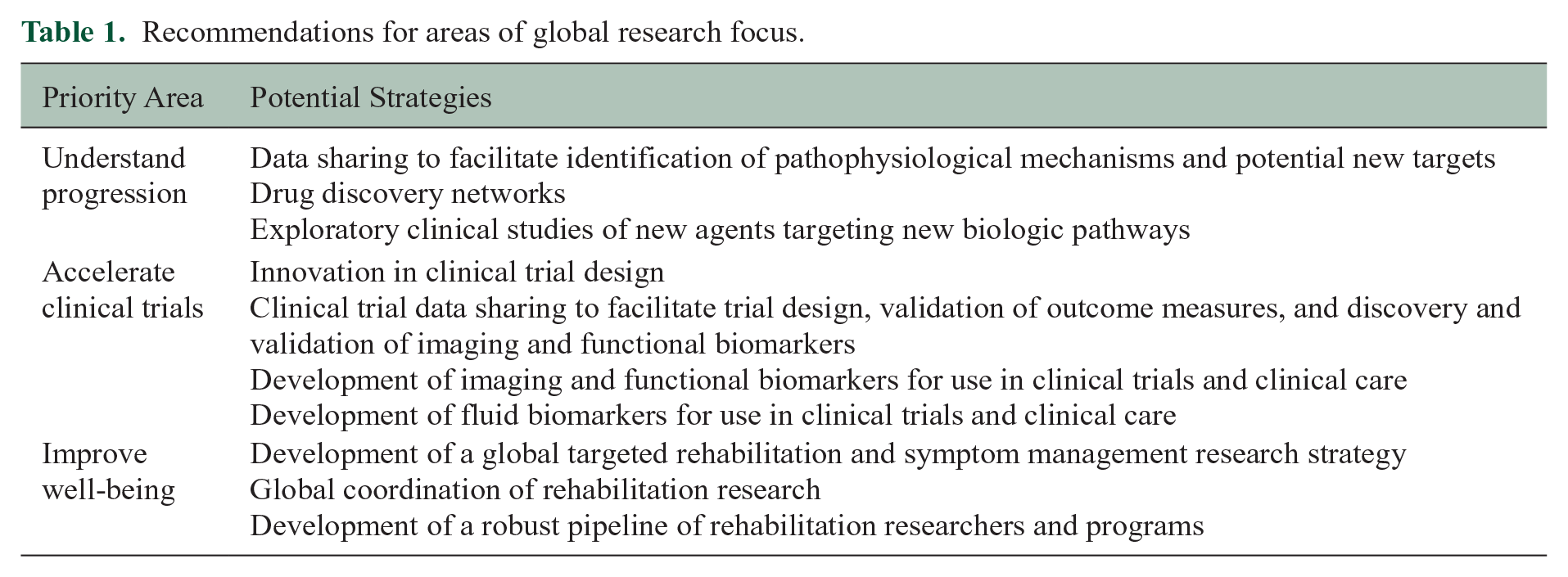
The research and clinical progress, together with the raised profile of progressive MS, over the last 5 years is a cause for hope. Clinical trials of approved treatments for progressive MS as well as those with negative outcomes are providing valuable insights and experience for the design and conduct of future trials. Moreover, there is growing appreciation of the importance of quality-of-life interventions in enabling patients with progressive MS to participate fully in society leading full and productive lives. While significant challenges remain, there are opportunities for impact provided the community prioritizes efforts to understand progression, accelerate clinical trials, and to enhance well-being of those with progressive MS (Table 1).
Recommendations for areas of global research focus.
All parties—people affected by progressive MS, patient groups, funders, academia, industry, regulatory authorities—have a role to play and ideally should be engaged, coordinated, and encouraged to work together (Figure 4). 85 Perspectives of people affected by Progressive MS must be incorporated across the research continuum to ensure proper focus on what matters to them. Engaging people with Progressive MS, as a key stakeholder, in research and measuring impact on outcome that matter most to them, will give research the direction to make all the relevant stakeholders co-accountable for social and wellbeing needs related to progressive MS. 79 This involvement can take many forms, such as inclusion of people with MS in establishing research agendas, contributing to design of clinical trials, planning for and communicating research results, and informing funding decisions and/or other parts of the research continuum. A recent example of such inclusion is the EU-funded MULTI-ACT initiative that has developed a framework to incorporate the perspectives of people with brain diseases in setting research agendas and in evaluating research impact. 86 These endeavors and others point to a future where patients contribute distinctively and meaningfully to the development transformational treatments.
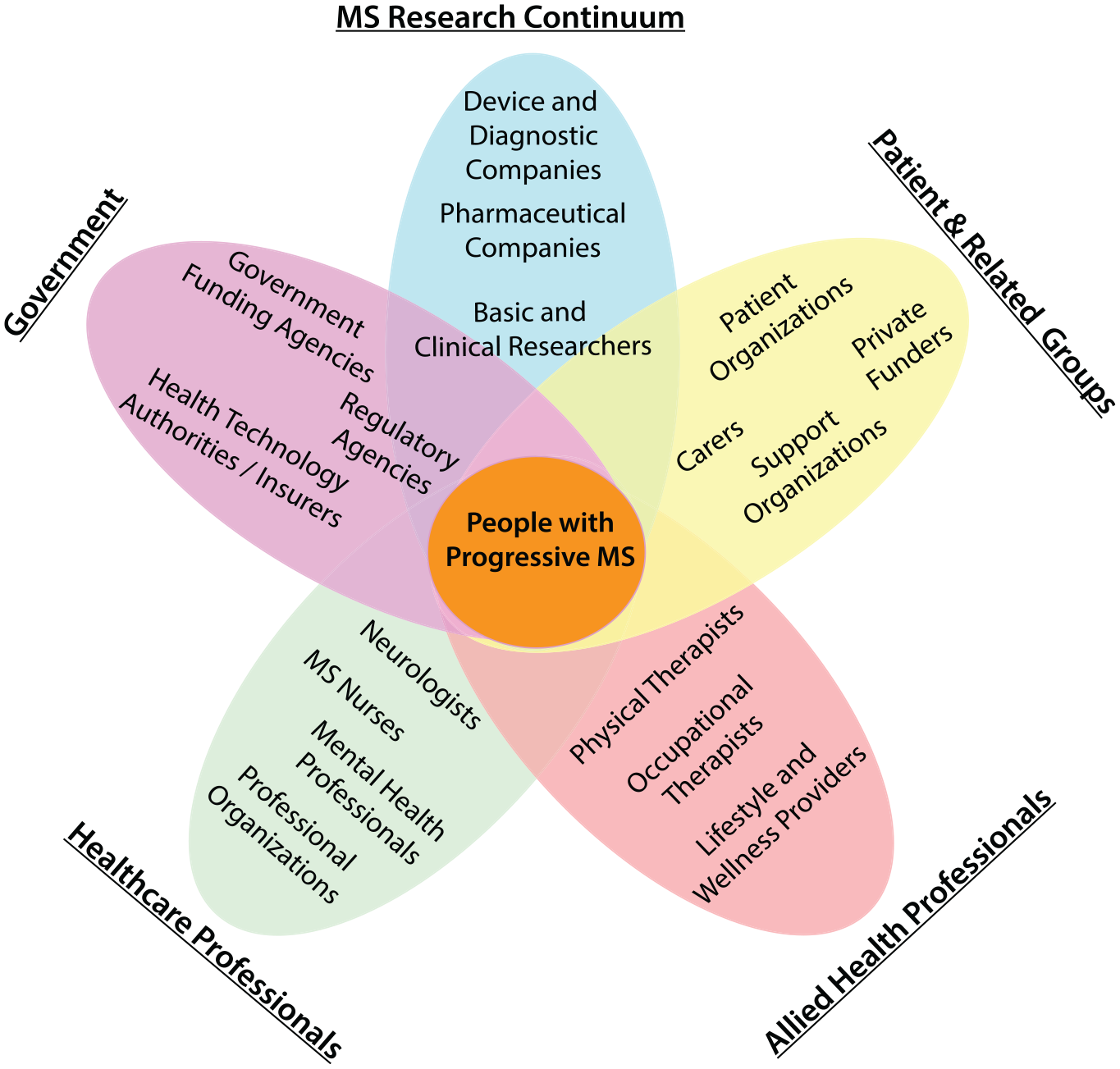
Stakeholders in the progressive MS agenda. Addressing the challenges of MS is a multi-stakeholder effort spanning patient organizations, clinical professionals, government, and industry.
Funders will need to sustain investments in ongoing programs and consider new ways of catalyzing progress. The impact of these investments will be further enhanced by meaningful coordination of research agendas at the national and international levels. Global multi-disciplinary and multi-stakeholder collaborative efforts like the International Progressive MS Alliance and a number of related strategic alliances (e.g. International Advisory Committee on Clinical Trials in MS, imaging networks in Europe and North America—MAGNIMS and NAIMS, respectively—and the UK MS Society multi-arm clinical trial platform—OCTOPUS—among others) will be critically important in directing efforts to refine our descriptions of progressive MS, accelerating drug discovery, and ensuring efficient conduct of clinical trials. Finally, robust efforts must be undertaken to ensure knowledge translation and implementation of interventions by health systems and clinicians. Fortunately, the field of implementation science points the way to success in such endeavors. 87 The well-established Quality Enhancement Research Initiative (QUERI) led by the US Veterans Administration is one pertinent illustration of how quality of care can be improved with a sustained focus on measuring the health, economic, and cultural impacts of scientific investments.88,89 Without similar efforts, we risk advancing knowledge without concomitant benefits being realized by people with progressive MS.
Conclusion
Addressing the needs of people with progressive MS remains a central challenge for the MS community. While there has been considerable progress in understanding the pathophysiological mechanisms of progressive MS, much remains to be understood. Moreover, the emergence of modestly effective treatments for progressive forms of the disease—while a source of hope—are just a beginning. Continued and coordinated efforts by the global scientific, clinical, and patient advocacy community will be critical to ensure sustained progress toward a future where fewer individuals are affected by progressive MS and where those with progressive MS have access to a suite of comprehensive and effective treatments. The International Progressive MS Alliance and its member organizations and many supporters affirm their commitment to invest in the proposed research strategy and call on the global research community to join in these collective efforts to find solutions and deliver hope to those affected by progressive MS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Thompson et al Conflict of Interest Disclosures.
AJ Thompson reports personal fees paid to his institution from Eisai Ltd; is an editorial board member for The Lancet Neurology receiving a free subscription; is Editor-in-Chief for Multiple Sclerosis Journal receiving an honorarium from SAGE Publications; receives support for travel as Chair, Scientific Advisory Committee, International Progressive MS Alliance, and from the National MS Society (USA) as member, NMSS Research Programs Advisory Committee.
WM Carroll reports honoraria and travel assistance for participation in industry sponsored meetings from and has provided advice to Biogen, Novartis, Genzyme, Sanofi, Aventis, Merck, and Celgene and has received travel support from the International Progressive MS Alliance, PACTRIMS and the World Federation of Neurology.
O Ciccarelli is Deputy Editor for Neurology and has acted as a Consultant for Merck and Biogen.
RAM receives research funding from CIHR, the MS Society of Canada, Research Manitoba, the CMSC, National MS Society, US Department of Defense, and Crohn’s and Colitis Canada. She is supported by the Waugh Family Chair in Multiple Sclerosis. She is a co-investigator on studies funded by Biogen Idec and Roche.
G. Comi has received compensation for consulting services for Bristol Myers Squibb, Janssen, Novartis, Teva, Sanofi, Genzyme, Merck, Biogen, Excemed, Roche, Almirall, Chugai, Receptos, and Forward Pharma and compensation for speaking activities for Novartis, Teva, Sanofi, Genzyme, Merck, Biogen, Excemed, and Roche.
A. Cross has done paid consulting for Biogen, Bristol Myers Squibb (Celgene), EMD Serono, Genentech/Roche, Greenwich Biosciences, Horizon Therapeutics, Janssen, Novartis, and TG Therapeutics and has contracted research funded by EMD Serono and Genentech.
A. Feinstein is on an Advisory Board for Akili Interactive and reports grants from the MS Society of Canada, book royalties from Johns Hopkins University Press, Cambridge University Press and Amadeus Press and speaker’s honoraria from Novartis, Biogen, Roche, and Sanofi-Genzyme.
C. Lubetzki reports grants from Biogen and personal fees for participation to advisory boards and/or symposia from Biogen, Merck Serono, Roche, Rewind, and Ipsen.
A Donnelly receives support for travel and subsistence as a member, Scientific Advisory Committee, International Progressive MS Alliance.
RJ Fox reports personal consulting fees from AB Science, Biogen, Celgene, EMD Serono, Genentech, Genzyme, Greenwich Biosciences, Immunic, Janssen, Novartis, Sanofi, and TG Therapeutics; has served on advisory committees for AB Science, Biogen, Genzyme, Immunic, Janssen, Novartis, Sanofi, and TG Therapeutics; and receives clinical trial contract and research grant funding from Biogen, Novartis, and Sanofi.
Anne Helme has no personal pecuniary interests to disclose, other than being an employee of the MS International Federation (MSIF), which receives income from a range of corporate sponsors, recently including: Biogen, Bristol Myers Squibb (formerly Celgene), Genzyme, Med-Day, Merck, Mylan, Novartis, Roche. MSIF is a managing member of the International Progressive MS Alliance.
P Kanellis is an employee of the Multiple Sclerosis Society of Canada, a member of the International Progressive MS Alliance
R Hohlfeld received consultancy fees from Novartis, Sanofi, Biogen, Merck, Janssen/Johnson&Johnson, and Roche.
R. Hyde is an employee of Biogen and co-chair of the International Progressive MS Alliance Industry Forum.
D Landsman is an employee of the National Multiple Sclerosis Society, a managing member of the International Progressive MS Alliance and has no conflict of interest.
X Montalban received speaking honoraria and travel expenses for participation in scientific meetings, has been a steering committee member of clinical trials or participated in advisory boards of clinical trials in the past years with Abbvie, Actelion, Alexion, Bayer, Biogen, Bristol-Myers Squibb/Celgene, EMD Serono, Genzyme, Hoffmann-La Roche, Immunic, Janssen Pharmaceuticals, Medday, Merck, Mylan, Nervgen, Novartis, Sanofi-Genzyme, Teva Pharmaceutical, TG Therapeutics, Excemed, MSIF, and NMSS.
JM Morahan is an employee of Multiple Sclerosis Australia, a managing member of the International Progressive MS Alliance.
B. Musch is an employee of Genentech, a subsidiary of Roche AG.
M. Salvetti reports speaking honoraria and research support from Merck, Sanofi, Novartis, Biogen, Roche, Bristol Myers Squibb.
S Rawlings is an employee of the MS Society UK, a managing member of the International Progressive MS Alliance.
C Sincock receives support for travel and subsistence as a member of the Scientific Advisory Committee, International Progressive MS Alliance.
K Smith receives consulting fees for project work from the International Progressive MS Alliance, and travel support from the Alliance as a member of the Scientific Steering Committee and the National MS Society as a member of their Scientific Advisory Committee.
F Sellebjerg has served on scientific advisory boards for, served as consultant for, received support for congress participation or received speaker honoraria from Alexion, Biogen, Bristol Myers Squibb, Merck, Novartis, Roche, and Sanofi Genzyme. His laboratory has received research support from Biogen, Merck, Novartis, Roche, and Sanofi Genzyme.
J Strum is the host of the RealTalk MS podcast. He has received podcast sponsorship fees from the National MS Society, EMD Serono, and Janssen Pharmaceuticals. As a speaker, he has received honoraria from Novartis, Auburn University, European MS Platform, and Can-Do MS. As co-lead investigator for caregiver research projects, he has received compensation from the Accelerated Cure Project for MS. He has also received support for travel to conferences and meetings from the National MS Society, the International Progressive MS Alliance, and the Accelerated Cure Project for MS.
P Zaratin is an employee of the Italian Multiple Sclerosis Society, a managing member of the International Progressive MS Alliance and has no conflict of interest.
T Coetzee is an employee of the National Multiple Sclerosis Society, a managing member of the International Progressive MS Alliance and has no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the International Progressive MS Alliance. The funder provided financial support for convening activities of the authors to inform development of research strategies discussed in this paper.